
Novel COVID-19 Diagnosis Delivery App Using Computed Tomography Images Analyzed with Saliency-Preprocessing and Deep Learning


Abstract
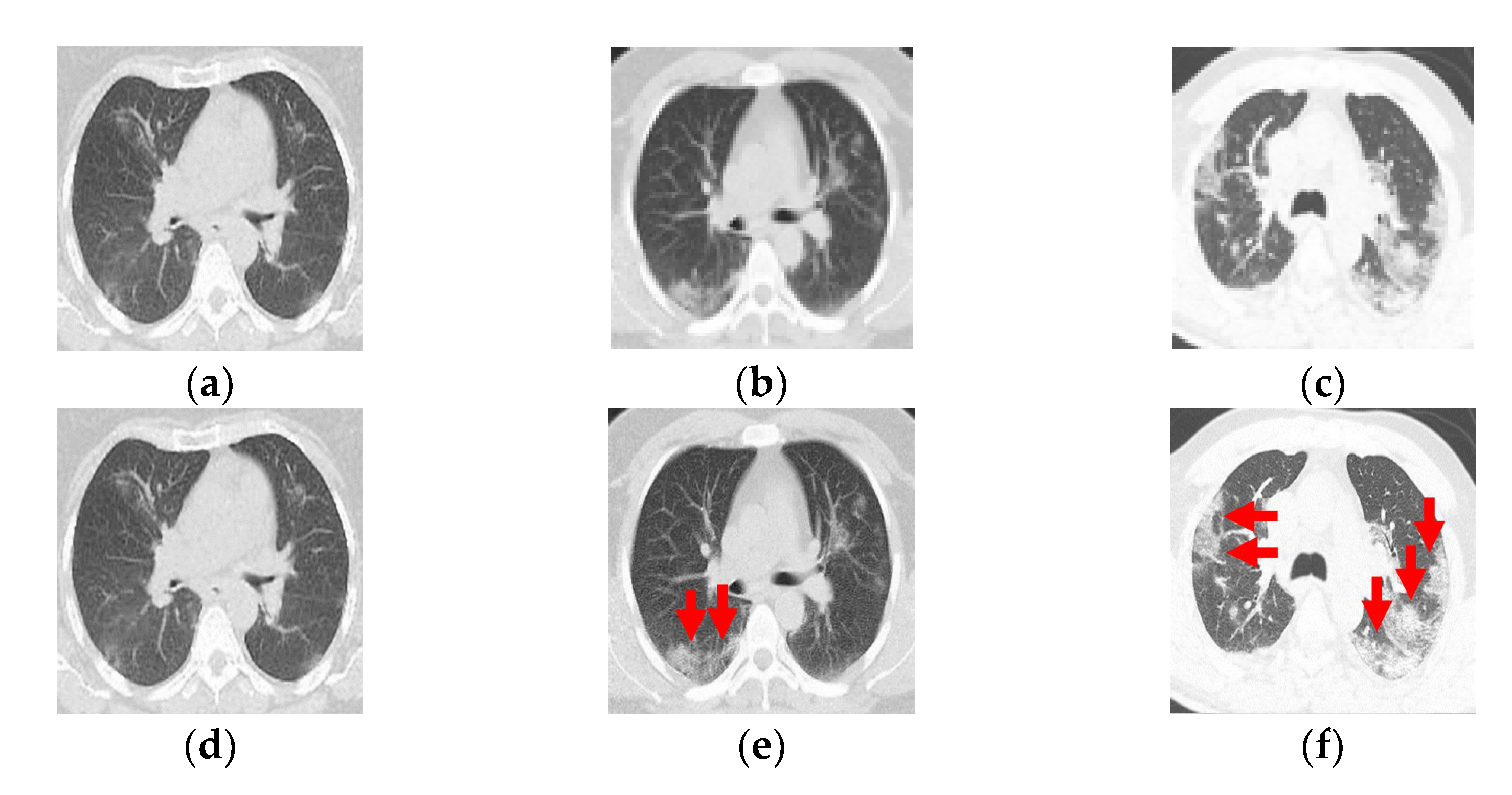
:1. Introduction
2. Materials and Methods
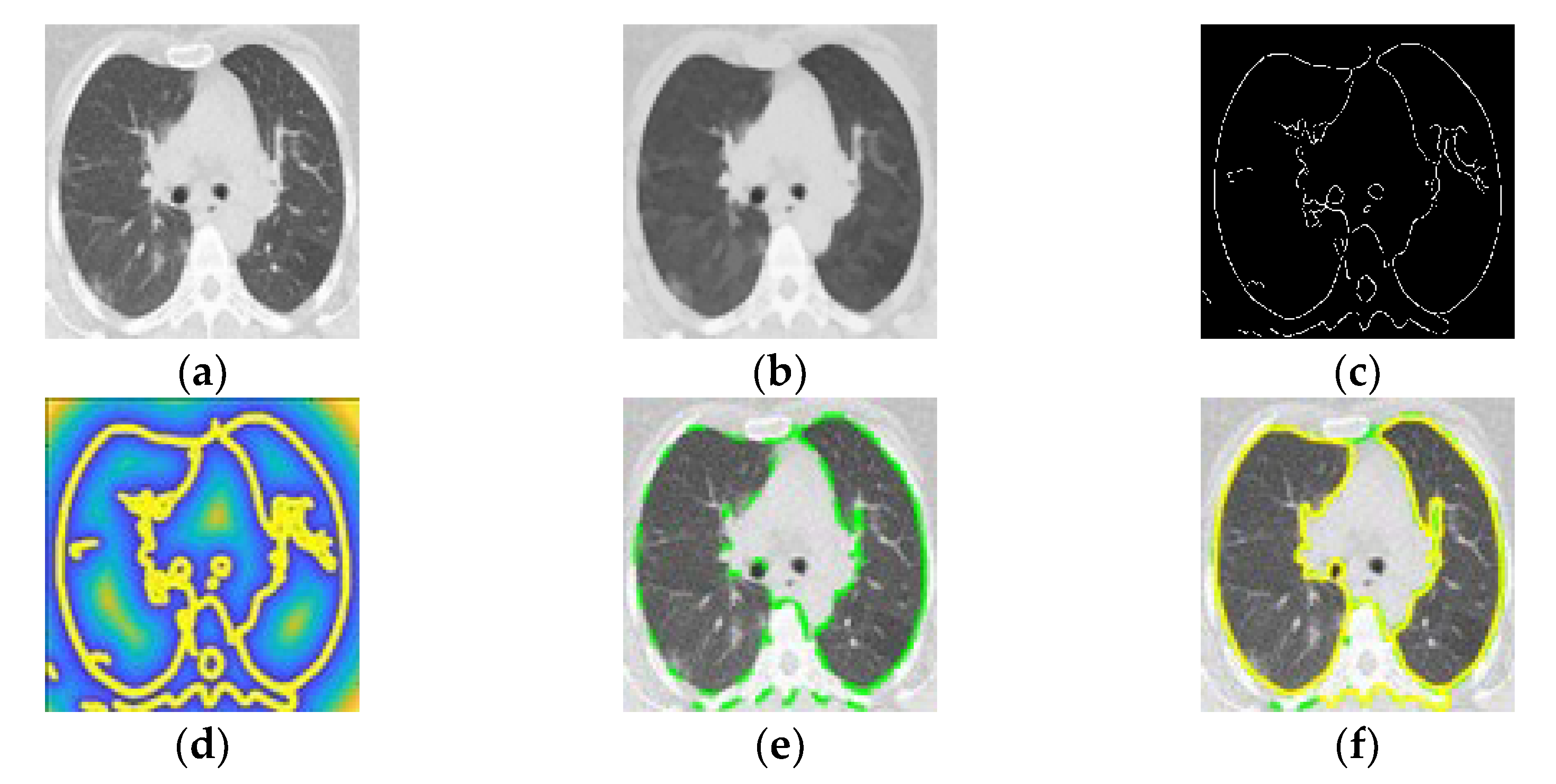
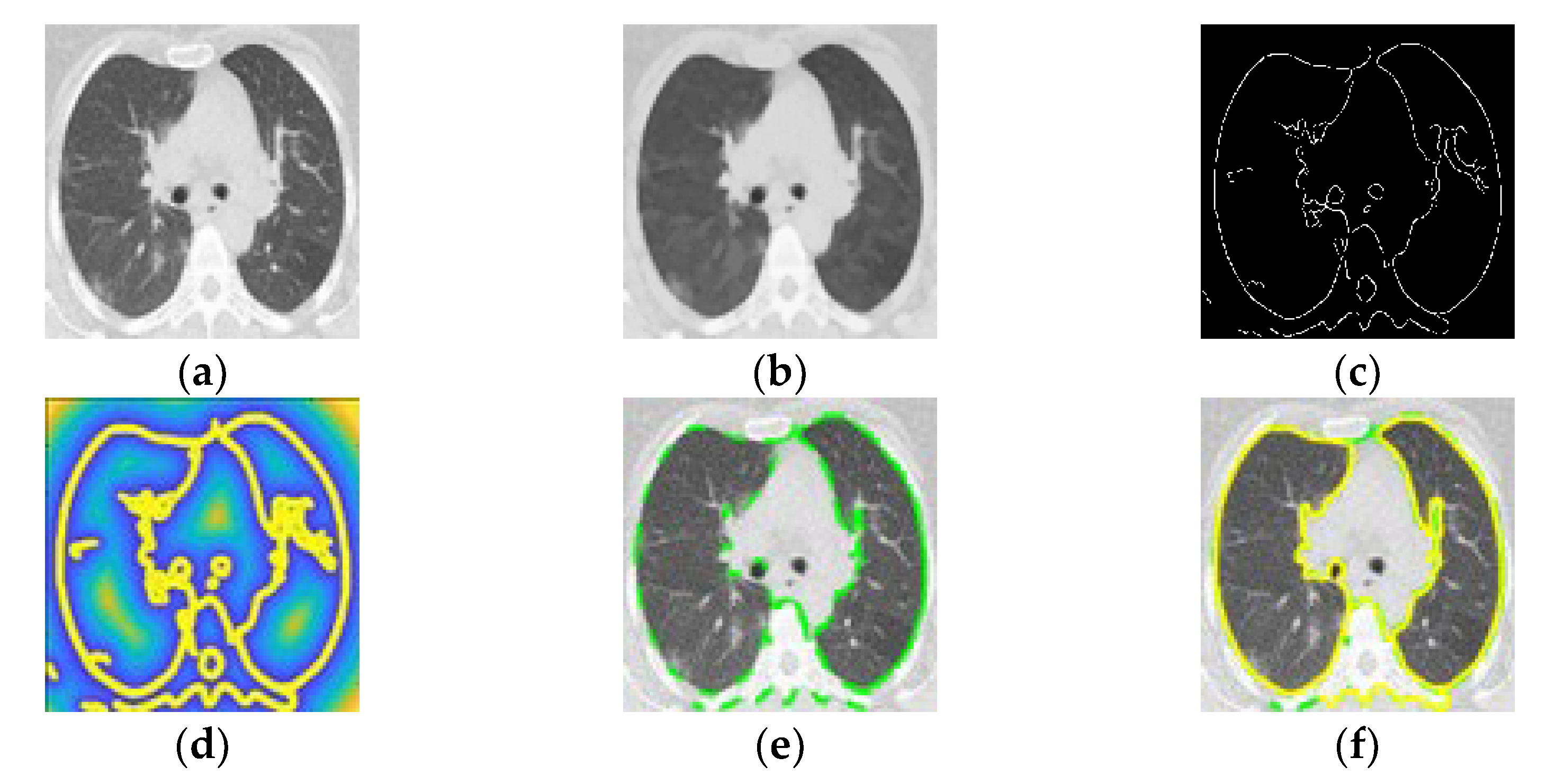
2.1. Pulmonary Parenchymal Identification by Poisson Inverse Gradient
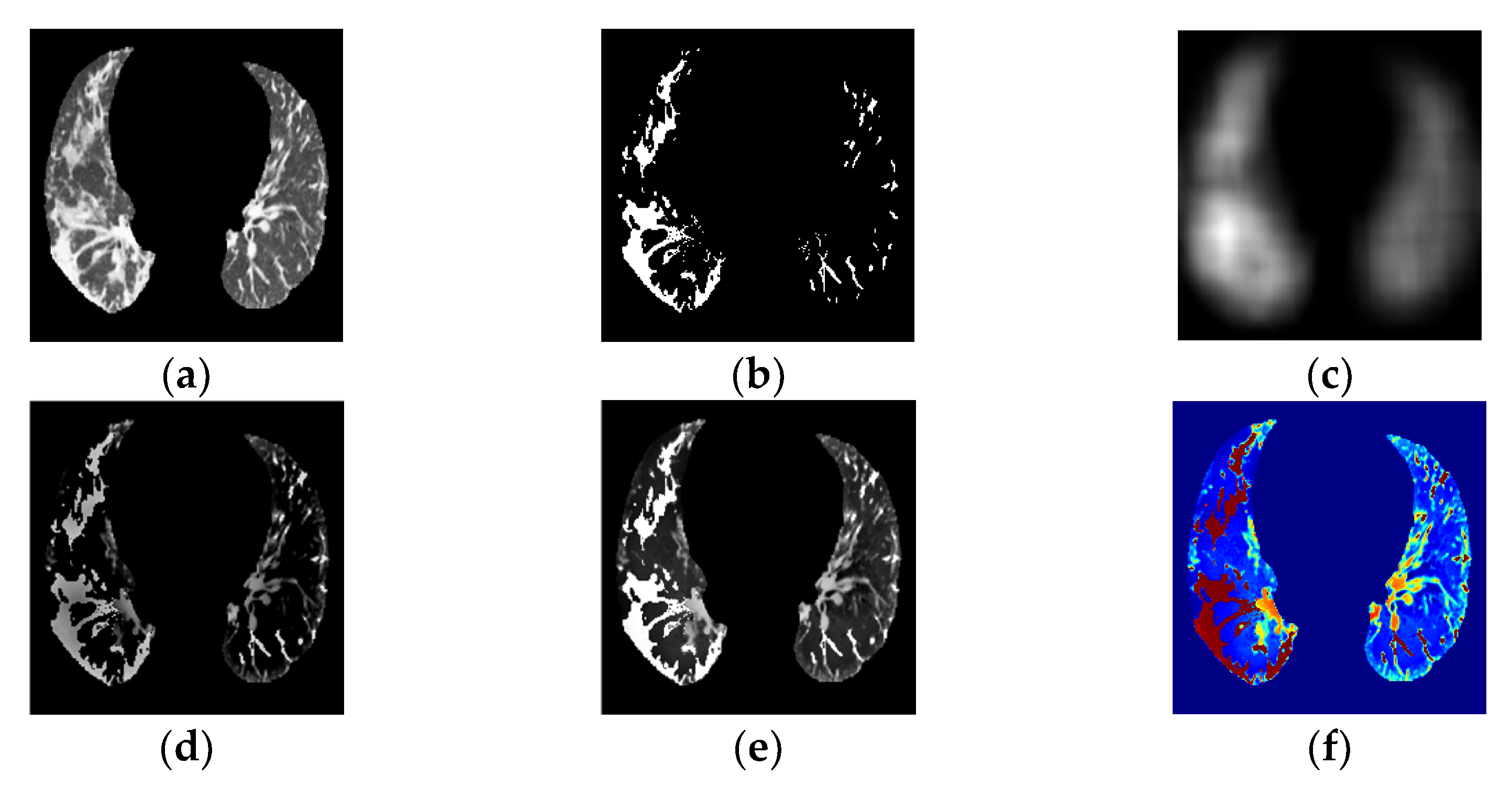
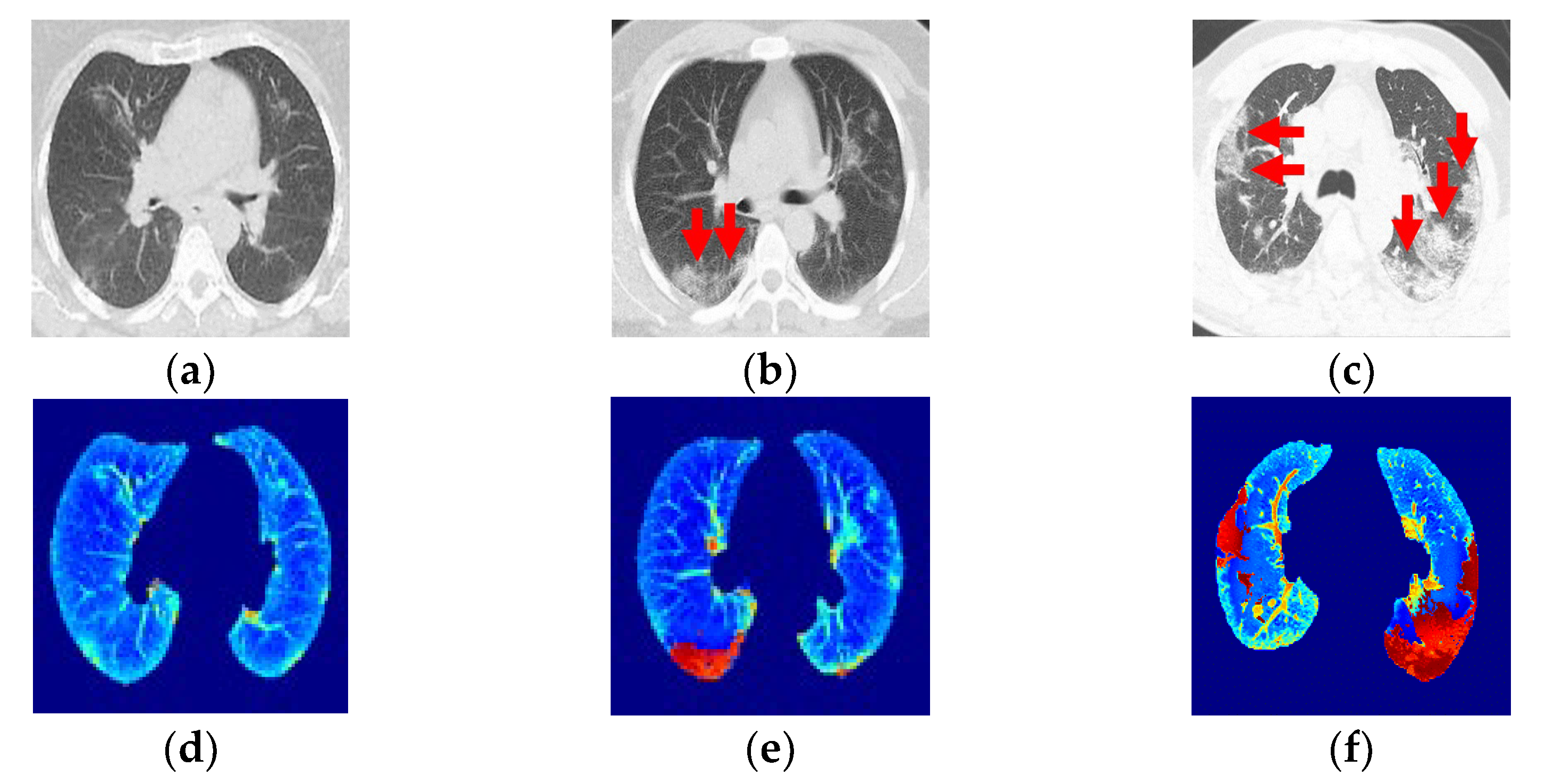
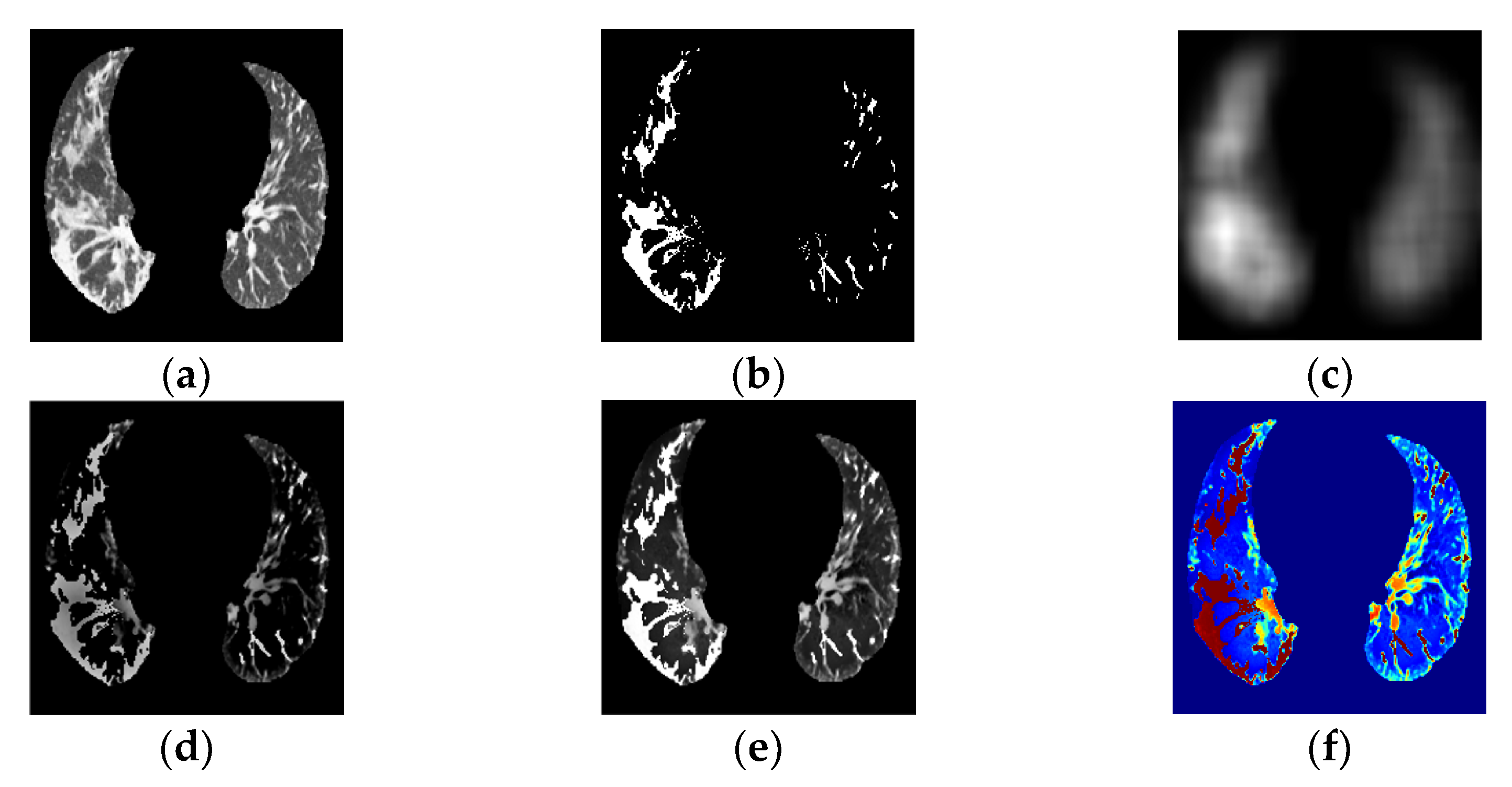
2.2. Ground-Glass Opacity and Pulmonary Infiltrates Highlighted by Saliency Fusion
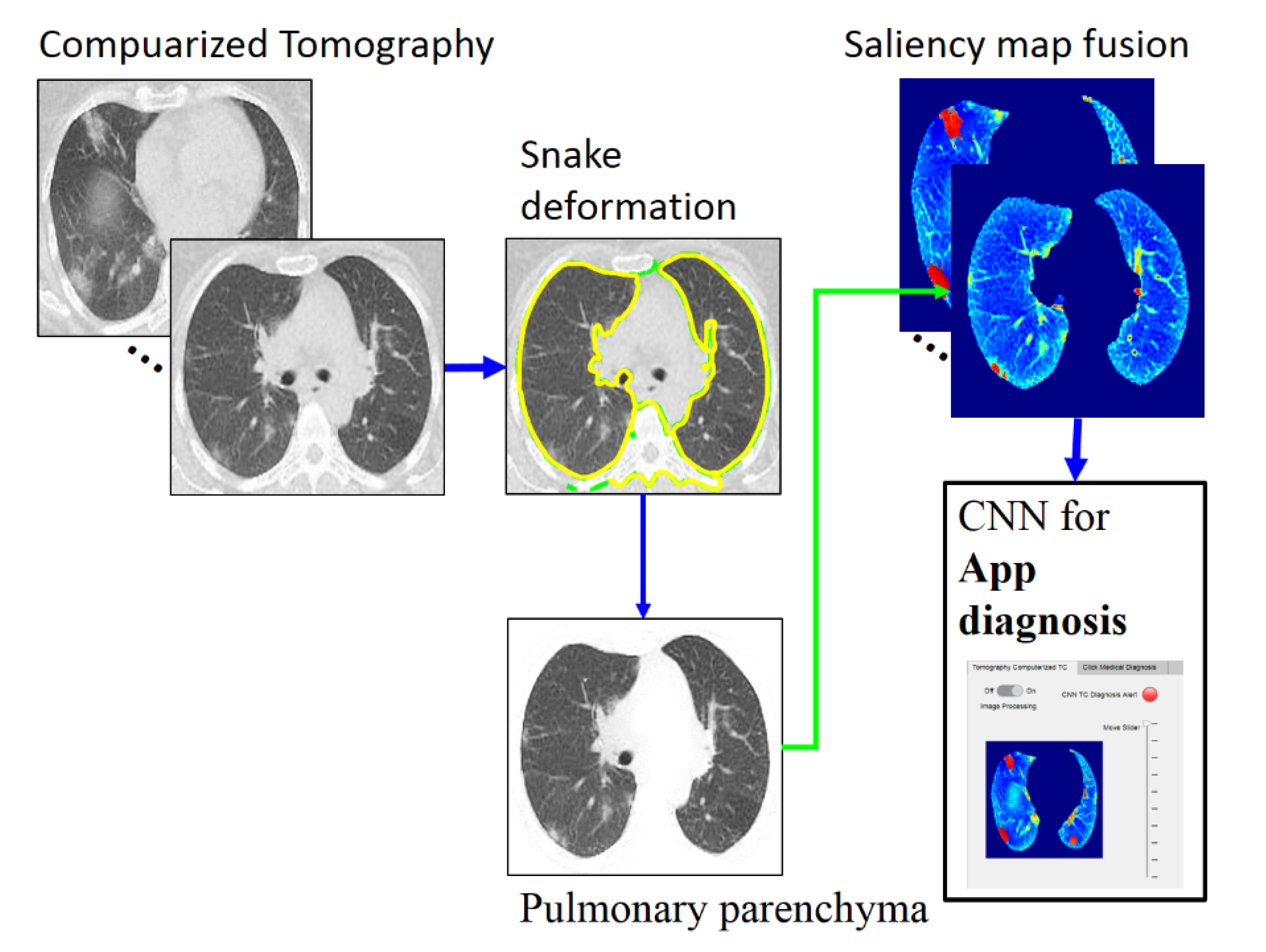
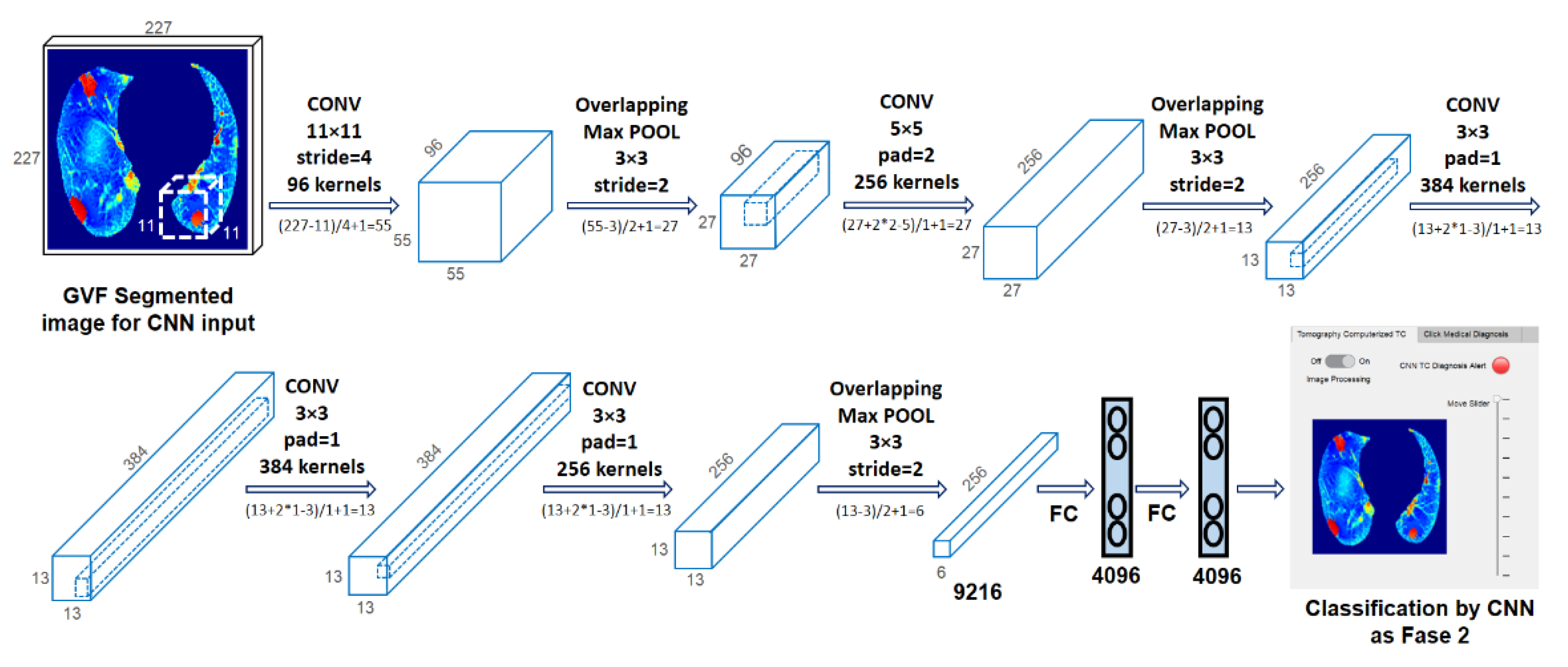
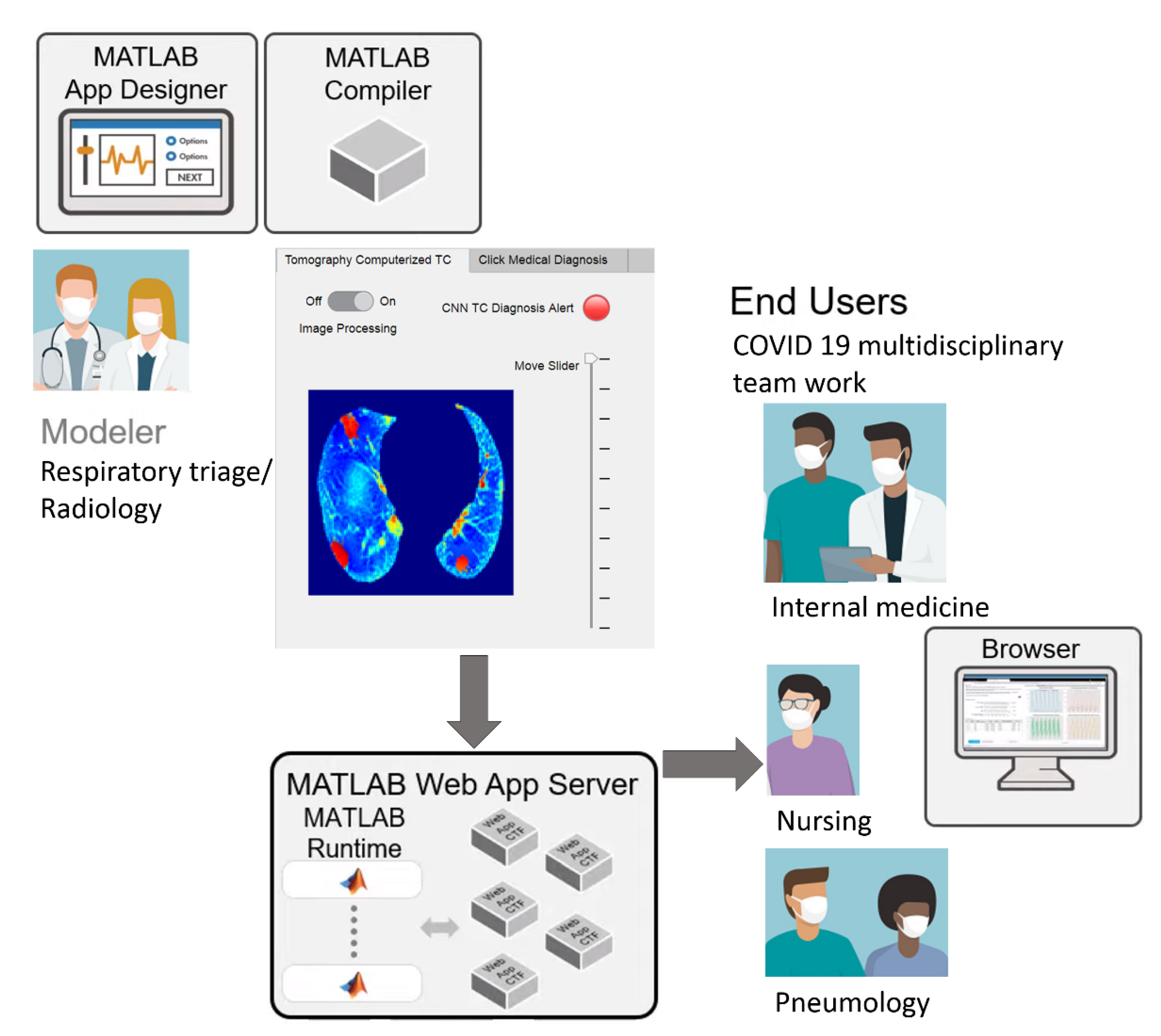
2.3. Convolutional Neural Network Classification for Telemedicine App
3. Experimental Results
3.1. Dataset
3.2. Quantitative and Qualitative Evaluation of PP and GGO–PI Identification
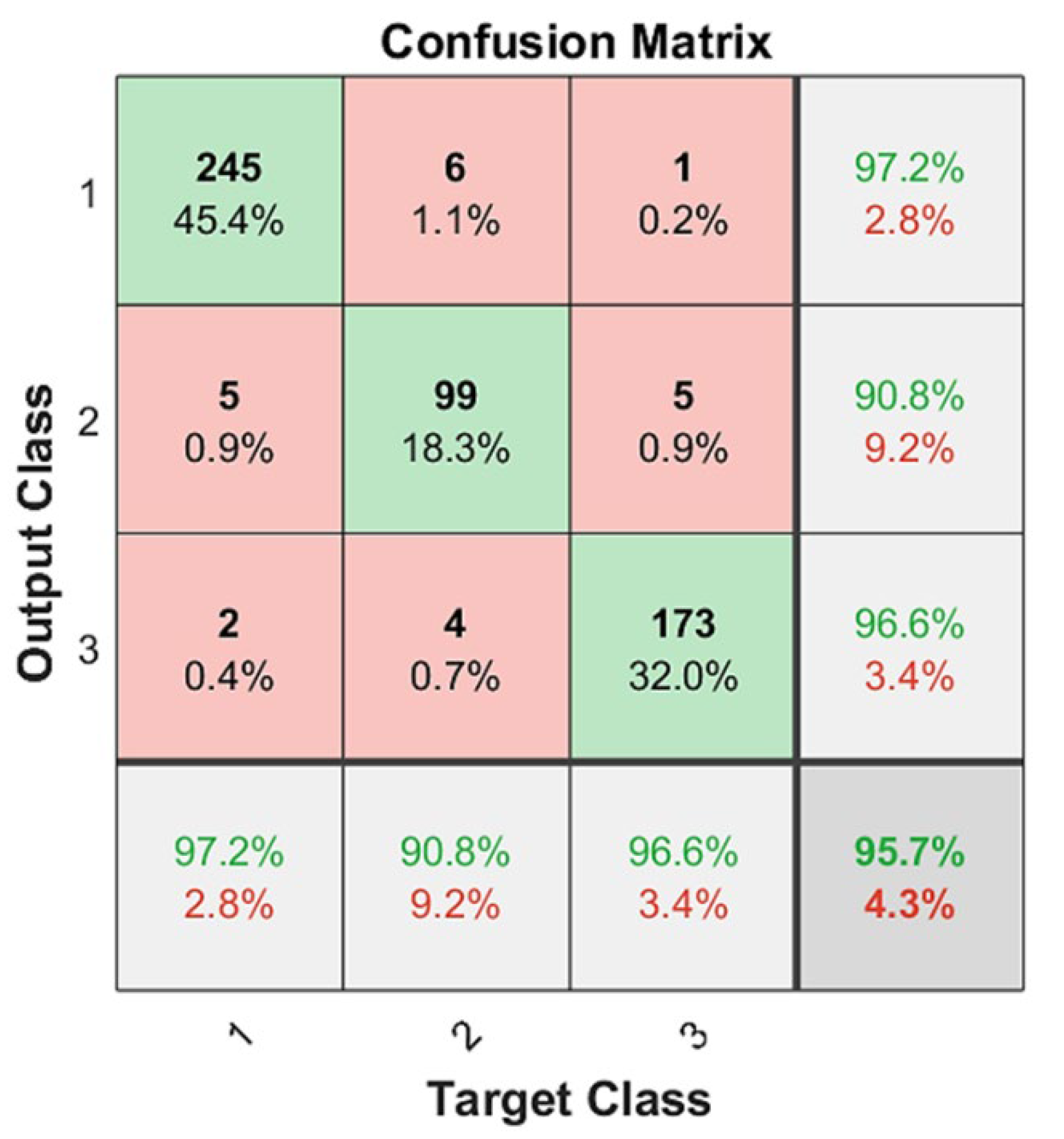
3.3. Quantitative Indicators for CNN Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 30 January 2020).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020 (accessed on 11 March 2020).
- Stogiannos, N.; Fotopoulos, D.; Woznitza, N.; Malamateniou, C. COVID-19 in the radiology department: What radiographers need to know. Radiography 2020, 26, 254–263. [Google Scholar] [CrossRef]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.-T.; Leung, S.T.; Chin, T.W.-Y.; Lo, C.S.Y. Frequency and Distribution of Chest Ra-diographic Findings in COVID-19 Positive Patients. Radiology 2020, 296, E72–E78. [Google Scholar] [CrossRef] [Green Version]
- Zhang, N.; Xu, X.; Zhou, L.-Y.; Chen, G.; Li, Y.; Yin, H. Clinical characteristics and chest CT imaging features of critically ill COVID-19 patients. Eur. Radiol. 2020, 30, 6151–6160. [Google Scholar] [CrossRef]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for Typical Coronavirus Disease 2019 (COVID-19) Pneumonia: Relationship to Negative RT-PCR Testing. Radiology 2020, 296, E41–E45. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. AJR Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef]
- Hani, C.; Trieu, N.H.; Saab, I.; Dangeard, S.; Bennani, S.; Chassagnon, G. COVID-19 pneumonia: A review of typical CT findings and differential diagnosis. Diagn. Interv. Imaging 2020, 101, 263–268. [Google Scholar] [CrossRef]
- Liu, K.-C.; Xu, P.; Lv, W.-F.; Qiu, X.-H.; Yao, J.-L.; Gu, J.-F. CT manifestations of coronavirus disease-2019: A retrospective analysis of 73 cases by disease severity. Eur. J. Radiol. 2020, 126, 108941. [Google Scholar] [CrossRef]
- Luo, N.; Zhang, H.; Zhou, Y.; Kong, Z.; Sun, W.; Huang, N. Utility of chest CT in diagnosis of COVID-19 pneumonia. Diagn. Interv. Radiol. 2020, 26, 437–442. [Google Scholar] [CrossRef]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.-C.; Luo, H.; Liu, S.; Huang, S.; Zhou, Z.; Yu, Q. Dynamic evolution of COVID-19 on chest computed tomography: Experience from Jiangsu Province of China. Eur. Radiol. 2020, 30, 6194–6203. [Google Scholar] [CrossRef]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Farina, D.; Rondi, P.; Botturi, E.; Renzulli, M.; Borghesi, A.; Guelfi, D.; Ravanelli, M. Gastrointestinal: Bowel ischemia in a suspected coronavirus disease (COVID-19) patient. J. Gastroenterol. Hepatol. 2021, 36, 41. [Google Scholar] [CrossRef] [PubMed]
- Brandi, N.; Ciccarese, F.; Rimondi, M.R.; Balacchi, C.; Modolon, C.; Sportoletti, C.; Golfieri, R. An Imaging Overview of COVID-19 ARDS in ICU Patients and Its Complications: A Pictorial Review. Diagnostics 2022, 12, 846. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Liu, Q.; Xu, H.; Lu, H.; Liu, S.; Li, H. Imaging of coronavirus disease 2019: A Chinese expert consensus statement. Eur. J. Radiol. 2020, 127, 109008. [Google Scholar] [CrossRef]
- Li, M. Chest CT features and their role in COVID-19. Radiol. Infect. Dis. 2020, 7, 51–54. [Google Scholar] [CrossRef]
- Greff, K.; Srivastava, R.; Jan, K.; Steunebrink, B. LSTM: A search space odyssey. IEEE Trans. Neural Netw. Learn. Syst. 2017, 28, 2222–2232. [Google Scholar] [CrossRef] [Green Version]
- Skalic, M.; Jiménez, J.; Sabbadin, D.; De, G. Shape-based generative modeling for de novo drug design. J. Chem. Info. Model. 2019, 59, 1205–1214. [Google Scholar] [CrossRef]
- Pham, Q.V.; Nguyen, D.C.; Huynh-The, T.; Hwang, W.J.; Pathirana, P.N. Artificial intelligence (AI) and big data for coro-navirus (COVID-19) pandemic: A survey on the state-of-the-arts. IEEE Access 2020, 8, 130820–130839. [Google Scholar] [CrossRef]
- Mobiny, A.; Cicalese, P.A.; Zare, S.; Yuan, P.; Abavisani, M.; Wu, C.C.; Van Nguyen, H. Radiologist-level COVID-19 detection using CT scans with detail-oriented capsule networks. arXiv 2020, arXiv:2004.07407. [Google Scholar] [CrossRef]
- Amyar, A.; Modzelewski, R.; Li, H.; Ruan, S. Multi-task deep learning based CT imaging analysis for COVID-19 pneumonia: Classification and segmentation. Comput. Biol. Med. 2020, 126, 104037. [Google Scholar] [CrossRef]
- Polsinelli, M.; Cinque, L.; Placidi, G. A light CNN for detecting COVID-19 from CT scans of the chest. Pattern Recognit. Lett. 2020, 140, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Xia, J. Using artificial intelligence to detect COVID-19 and community-acquired pneumonia based on pulmonary CT: Evaluation of the diagnostic accuracy. Radiology 2020, 296, E65–E71. [Google Scholar] [CrossRef] [PubMed]
- Konar, D.; Panigrahi, B.K.; Bhattacharyya, S.; Dey, N.; Jiang, R. Auto-diagnosis of COVID-19 using lung CT images with semi-supervised shallow learning network. IEEE Access 2021, 9, 28716–28728. [Google Scholar] [CrossRef]
- Wu, Y.H.; Gao, S.H.; Mei, J.; Xu, J.; Fan, D.P.; Zhang, R.G.; Cheng, M.M. Jcs: An explainable Covid-19 diagnosis system by joint classification and segmentation. IEEE Trans. Image Process. 2021, 30, 3113–3126. [Google Scholar] [CrossRef] [PubMed]
- Kass, M.; Witkin, A.; Terzopoulos, D. Snake: Snake energy models. Int. J. Comput. Vis. 1988, 1, 321–331. [Google Scholar] [CrossRef]
- Li, B.; Acton, S.T. Automatic active model initialization via Poisson inverse gradient. IEEE Trans. Image Process. 2008, 17, 1406–1420. [Google Scholar] [CrossRef]
- Tello-Mijares, S.; Woo, L. Computed tomography image processing analysis in COVID-19 patient follow-up assessment. J. Healthc. Eng. 2021, 2021, 8869372. [Google Scholar] [CrossRef]
- Balacchi, C.; Brandi, N.; Ciccarese, F.; Coppola, F.; Lucidi, V.; Bartalena, L.; Golfieri, R. Comparing the first and the second waves of COVID-19 in Italy: Differences in epidemiological features and CT findings using a semi-quantitative score. Emerg. Radiol. 2021, 28, 1055–1061. [Google Scholar] [CrossRef]
- Canny, J.F. A computation approach to edge detection. IEEE Trans. Pattern Anal. Mach. Intell. 1986, 8, 670–700. [Google Scholar] [CrossRef]
- Tello-Mijares, S.; Bescós, J. Region-based multifocus image fusion for the precise acquisition of Pap smear images. J. Biomed. Opt. 2018, 23, 056005. [Google Scholar] [CrossRef] [Green Version]
- De Jaegere, T.M.; Krdzalic, J.; Fasen, B.A.; Kwee, R.M. COVID-19 CT Investigators South-East Netherlands (CISEN) study group. Radiological Society of North America chest CT classification system for reporting COVID-19 pneumonia: Interobserver variability and correlation with RT-PCR. Radiol. Cardiothorac. Imaging 2020, 2, e200213. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L. Chest CT. Findings in Patients with Coronavirus Disease 2019 and Its Relationship with Clinical Features. Invest Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneu-monia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prokop, M.; Van Everdingen, W.; Van Rees Vellinga, T.; Quarles Van Ufford, J.; Stöger, L.; Beenen, L. CO-RADS—A categorical CT assessment scheme for patients with suspected COVID-19: Definition and evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bottou, L.; Bengio, Y.; Haffner, P. Gradient-based learning applied to document recognition. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky, A.; Ilya, S.; Geoffrey, E.H. ImageNet Classification with Deep Convolutional Neural Networks. Adv. Neural Inf. Proc. Syst. 2012, 25, 1097–1105. [Google Scholar] [CrossRef]
- Ajit, A.; Acharya, K.; Samanta, A. A review of convolutional neural networks. In Proceedings of the 2020 International Conference on Emerging Trends in Information Technology and Engineering (ic-ETITE), Vellore, India, 24–25 February 2020; pp. 1–5. [Google Scholar] [CrossRef]
- Vargas-Hákim, G.A.; Mezura-Montes, E.; Acosta-Mesa, H.G. A Review on Convolutional Neural Networks Encodings for Neuroevolution. IEEE Trans. Evol. Comput. 2022, 26, 12–27. [Google Scholar] [CrossRef]
- Heravi, E.J.; Aghdam, H.H.; Puig, D. Classification of Foods Using Spatial Pyramid Convolutional Neural Network. In Frontiers in Artificial Intelligence and Applications; IOS Press: Amsterdam, The Netherlands, 2016; pp. 163–168. [Google Scholar]
- Greenhalgh, T.; Wherton, J.; Shaw, S.; Morrison, C. Video consultations for COVID-19. BMJ 2020, 368, m998. [Google Scholar] [CrossRef] [Green Version]
- Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration within Health Systems toFight the COVID-19 Pandemic: A Call to Action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef]
- Zijdenbos, A.; Dawant, B.; Margolin, R.; Palmer, A. Morphometric analysis of white matter lesions in MR images: Method and validation. IEEE Trans. Med. Imag. 1994, 13, 716–724. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TP | FP | FN | P | ns | PPV | TPR | F1 | |
|---|---|---|---|---|---|---|---|---|
| Class 1 | 245 | 7 | 7 | 252 | 259 | 0.9722 | 0.9459 | 0.9589 |
| Class 2 | 99 | 10 | 10 | 109 | 119 | 0.9082 | 0.8319 | 0.8684 |
| Class 3 | 173 | 6 | 6 | 179 | 185 | 0.9664 | 0.9675 | 0.9505 |
| TOTAL | 517 | 23 | 23 | |||||
| PPV | TPR | F1 | |
|---|---|---|---|
| Macro | 0.9489 | 0.9043 | 0.9259 |
| Reference | Classes | Set Images | Training/Test | PPV | TPR | F1 |
|---|---|---|---|---|---|---|
| Proposed Vgg19 | Early, Progression, Peak | 540 (252, 09, 179) | 2-fold class validation | 0.948 | 0.904 | 0.925 |
| [21] | COVID-19, non-COVID-19 | 746 (333, 397) | 0.85/0.25 | 0.843 | 0.915 | |
| [22] | COVID-19, non-COVID-19 | 1044 (449, 595) | 944/100 | 0.81 | 0.83 | |
| [26] | COVID-19, non-COVID-19 | 757 (360, 397) | 0.6 train/0.2 validation/0.2 test | 0.8173 | 0.85 | 0. 83 |
| [24] | COVID-19, community-acquired pneumonia, non-pneumonia | 4352 (1292, 1735, 1325) | 0.9/0.1 | 0.9 | ||
| [25] | COVID-19, non-COVID-19 | 2482 (1252, 1230) | 1764/718 | 0.965 | 0.935 | 0.948 |
| [26] | COVID-19, non-COVID-19 | 144,167 (64,711, 68,041) | 2794–7500/64,711–68,041 | 0.95 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tello-Mijares, S.; Woo, F. Novel COVID-19 Diagnosis Delivery App Using Computed Tomography Images Analyzed with Saliency-Preprocessing and Deep Learning. Tomography 2022, 8, 1618-1630. https://doi.org/10.3390/tomography8030134
Tello-Mijares S, Woo F. Novel COVID-19 Diagnosis Delivery App Using Computed Tomography Images Analyzed with Saliency-Preprocessing and Deep Learning. Tomography. 2022; 8(3):1618-1630. https://doi.org/10.3390/tomography8030134
Chicago/Turabian StyleTello-Mijares, Santiago, and Fomuy Woo. 2022. "Novel COVID-19 Diagnosis Delivery App Using Computed Tomography Images Analyzed with Saliency-Preprocessing and Deep Learning" Tomography 8, no. 3: 1618-1630. https://doi.org/10.3390/tomography8030134
APA StyleTello-Mijares, S., & Woo, F. (2022). Novel COVID-19 Diagnosis Delivery App Using Computed Tomography Images Analyzed with Saliency-Preprocessing and Deep Learning. Tomography, 8(3), 1618-1630. https://doi.org/10.3390/tomography8030134