
Myocardial Strain for the Differentiation of Myocardial Involvement in the Post-Acute Sequelae of COVID-19—A Multiparametric Cardiac MRI Study

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
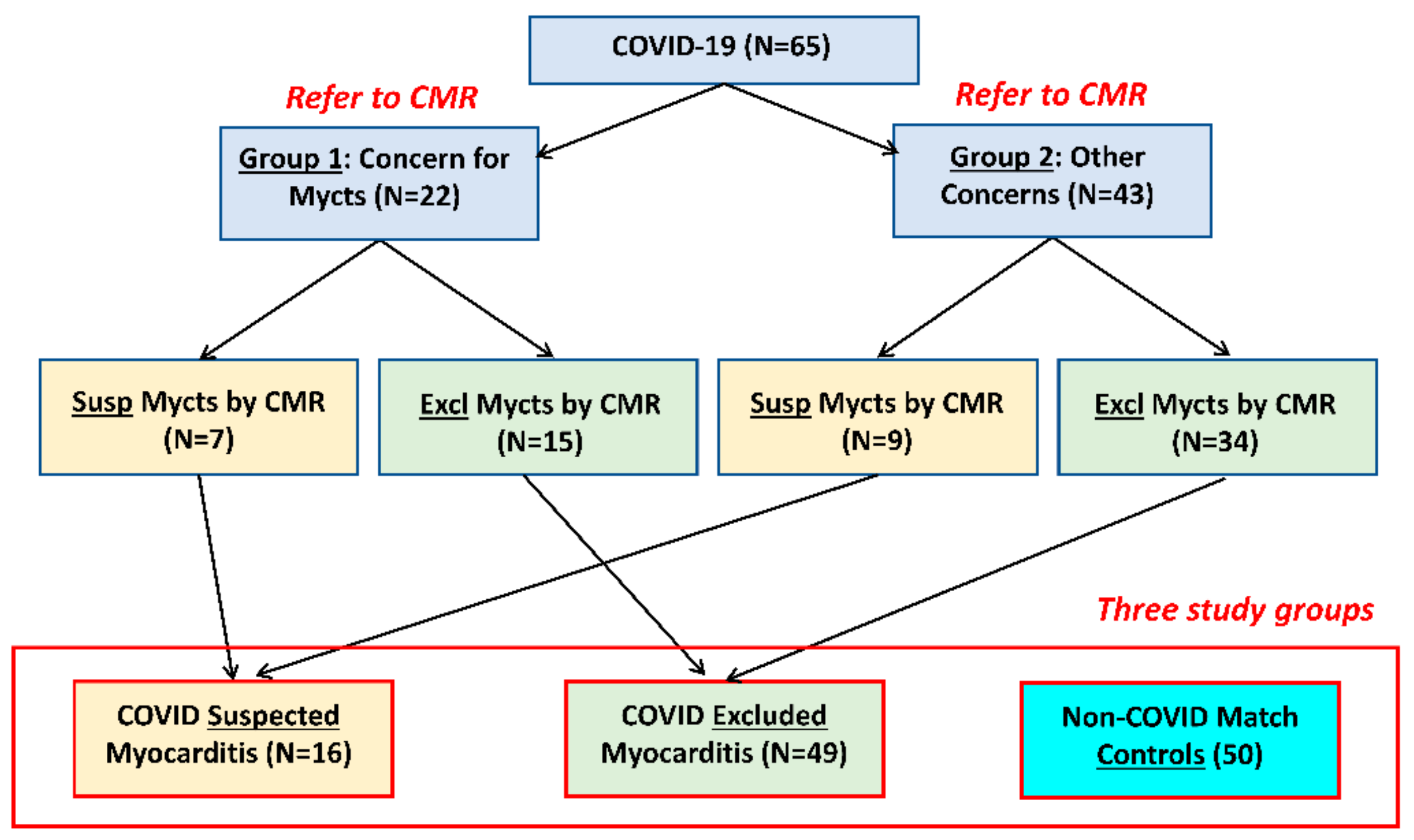
2.1. Study Design
2.2. Clinical Presentation
2.3. Image Acquisition
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Global Cardiac Function Reflects Ventricular Remodeling Post-COVID-19 Infection
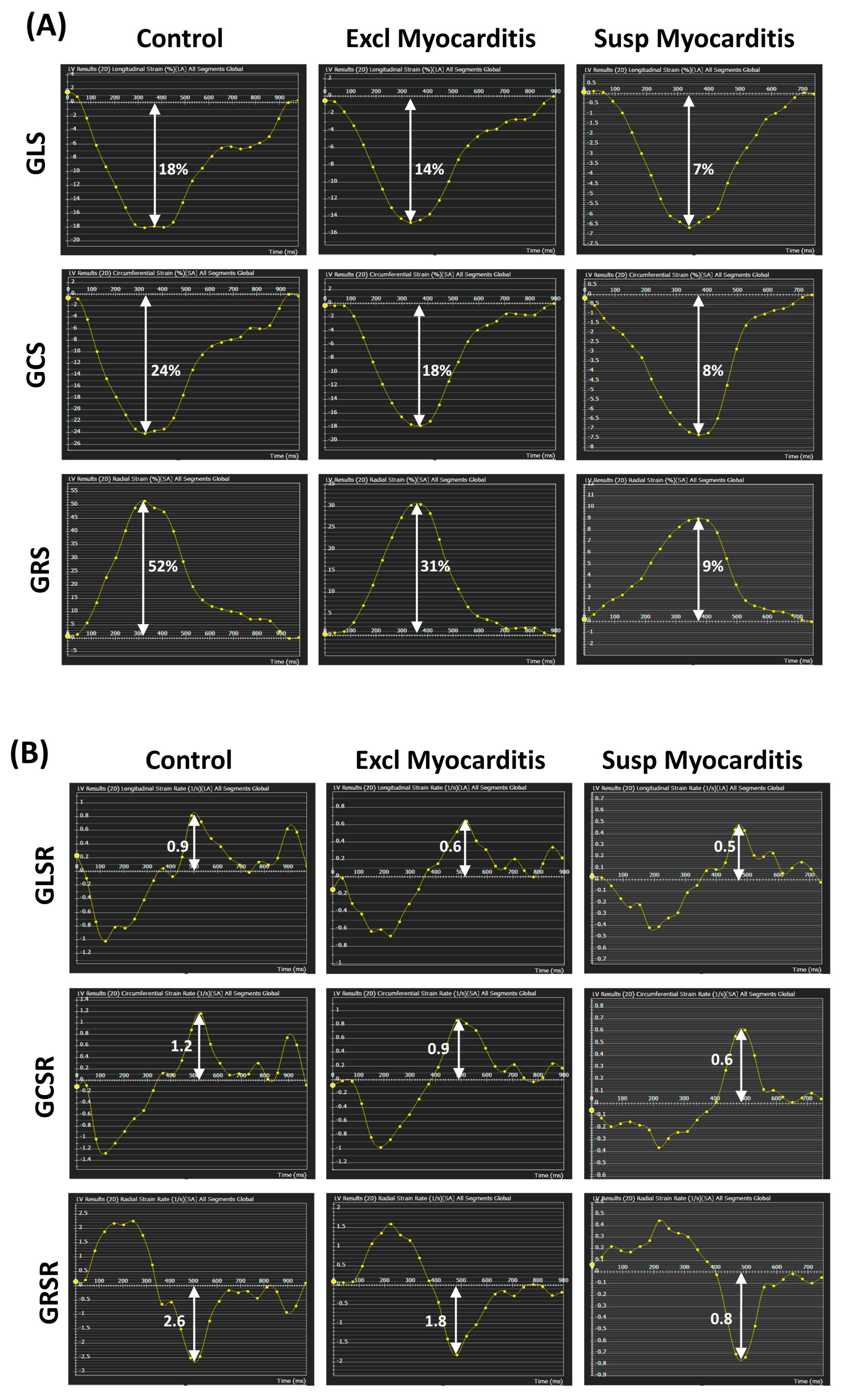
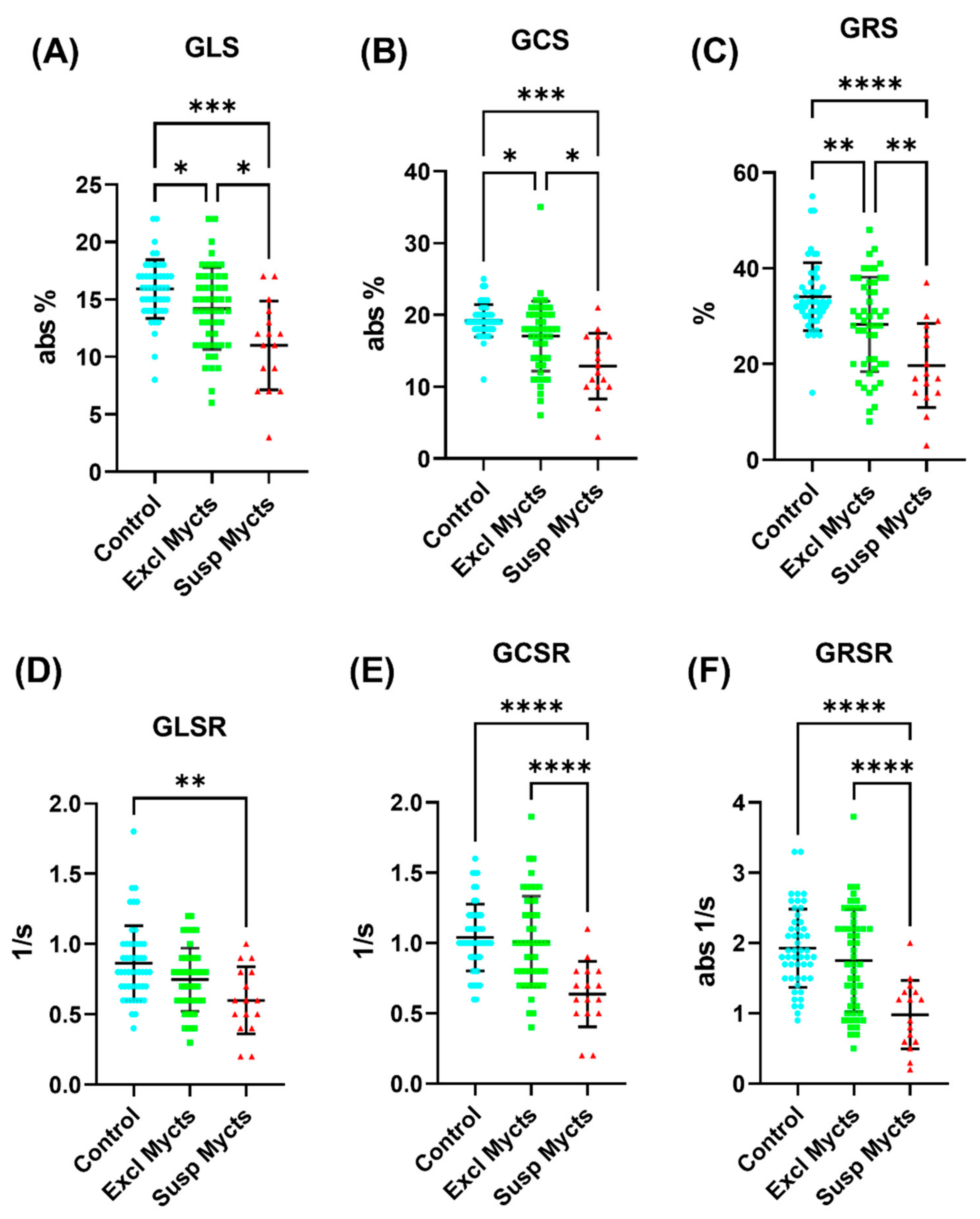
3.3. Strain and Strain Rate Are Sensitive Markers for Identifying COVID-19 Patients with Myocarditis
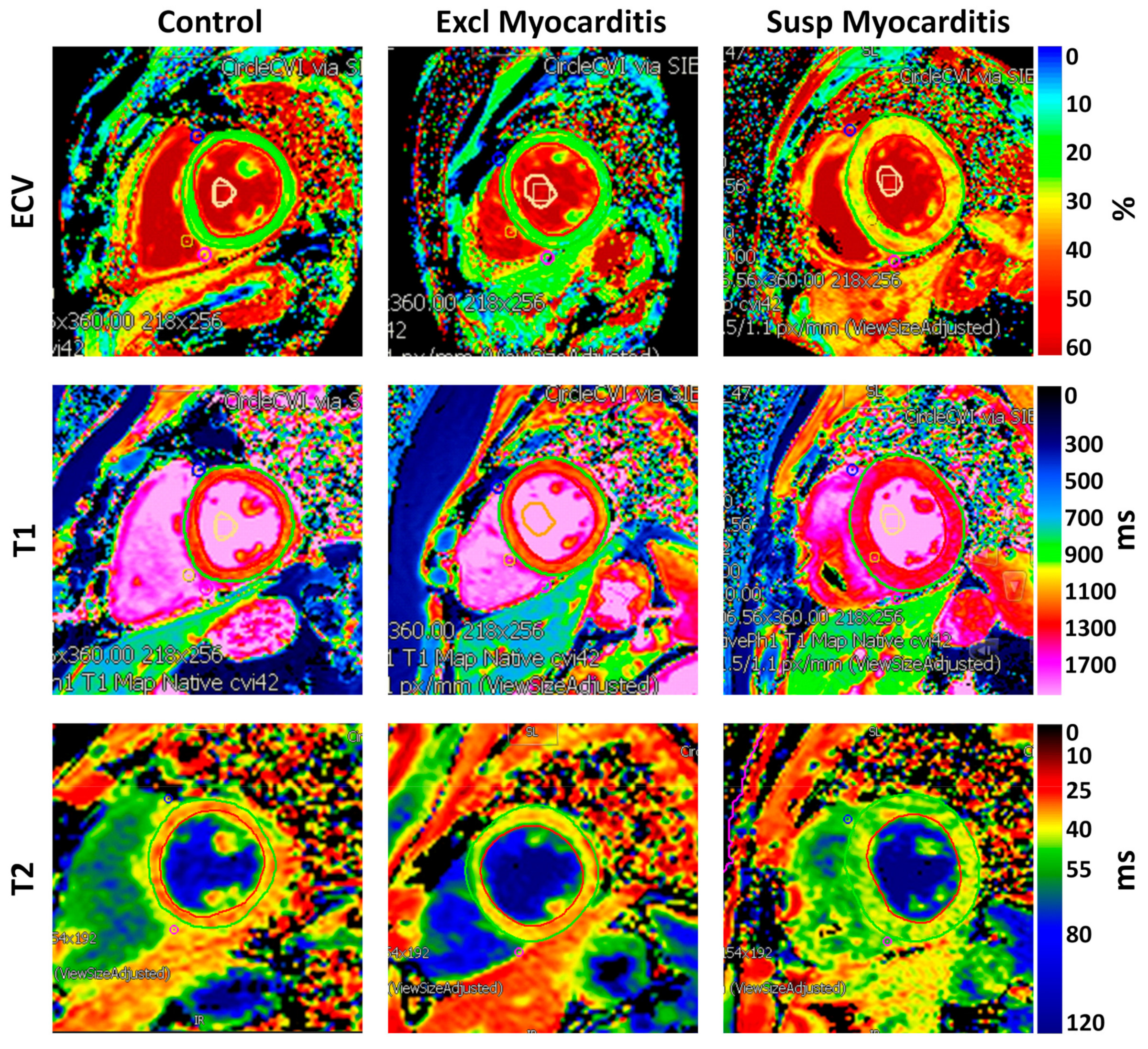
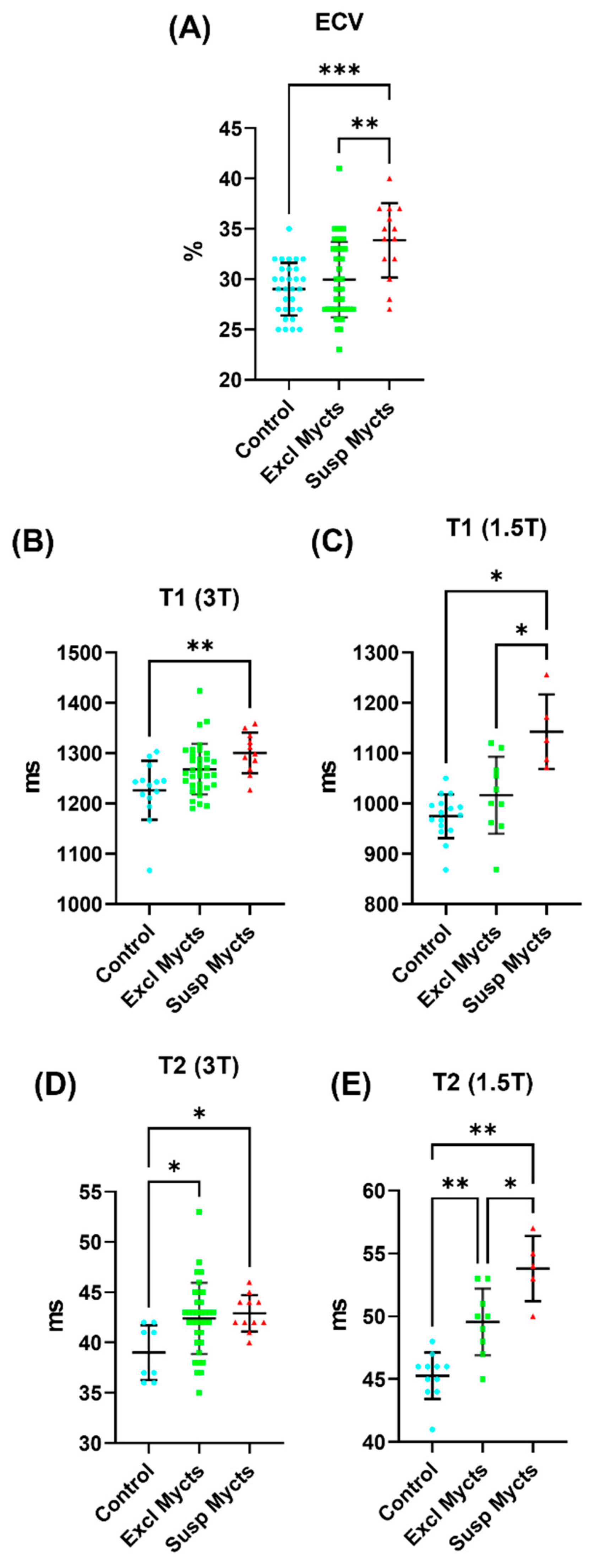
3.4. COVID-19 Affects Myocardial Tissue Structure
3.4.1. LGE Findings
3.4.2. ECV Measurements
3.4.3. T1 Measurements
3.4.4. T2 Measurements
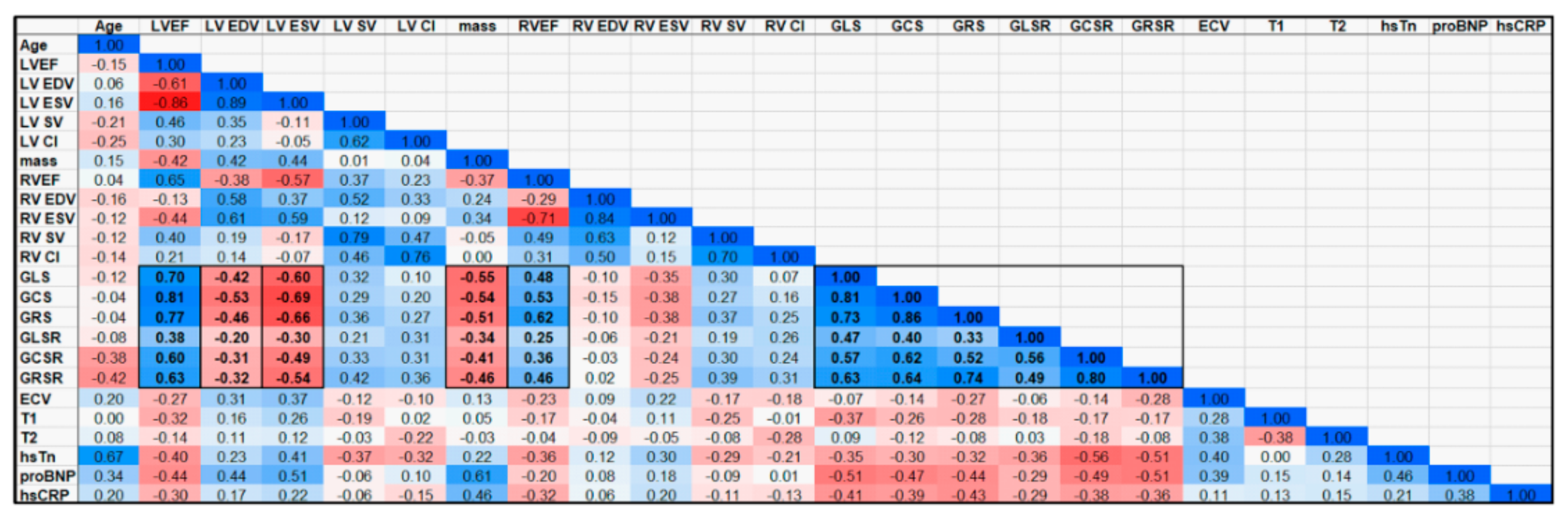
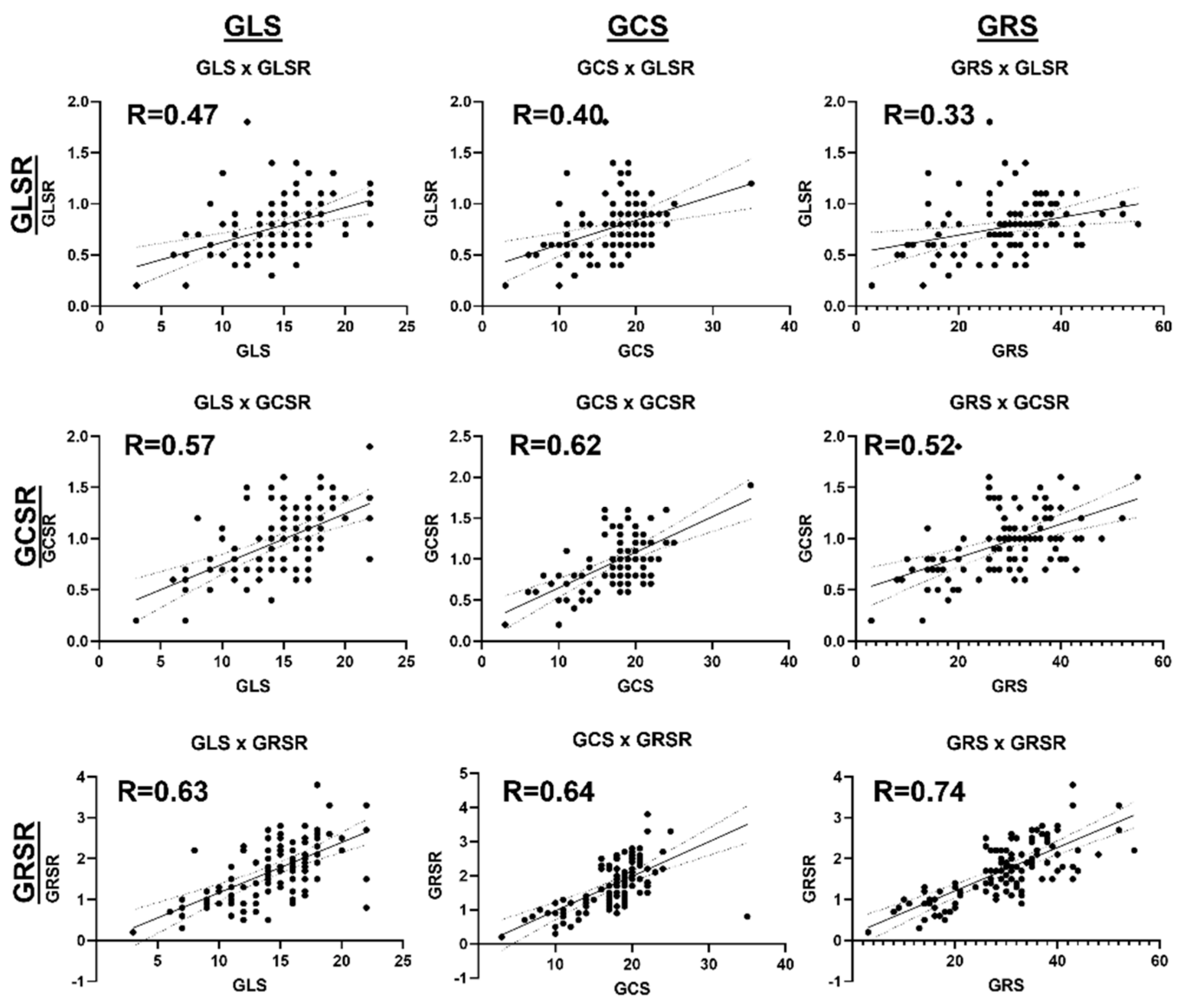
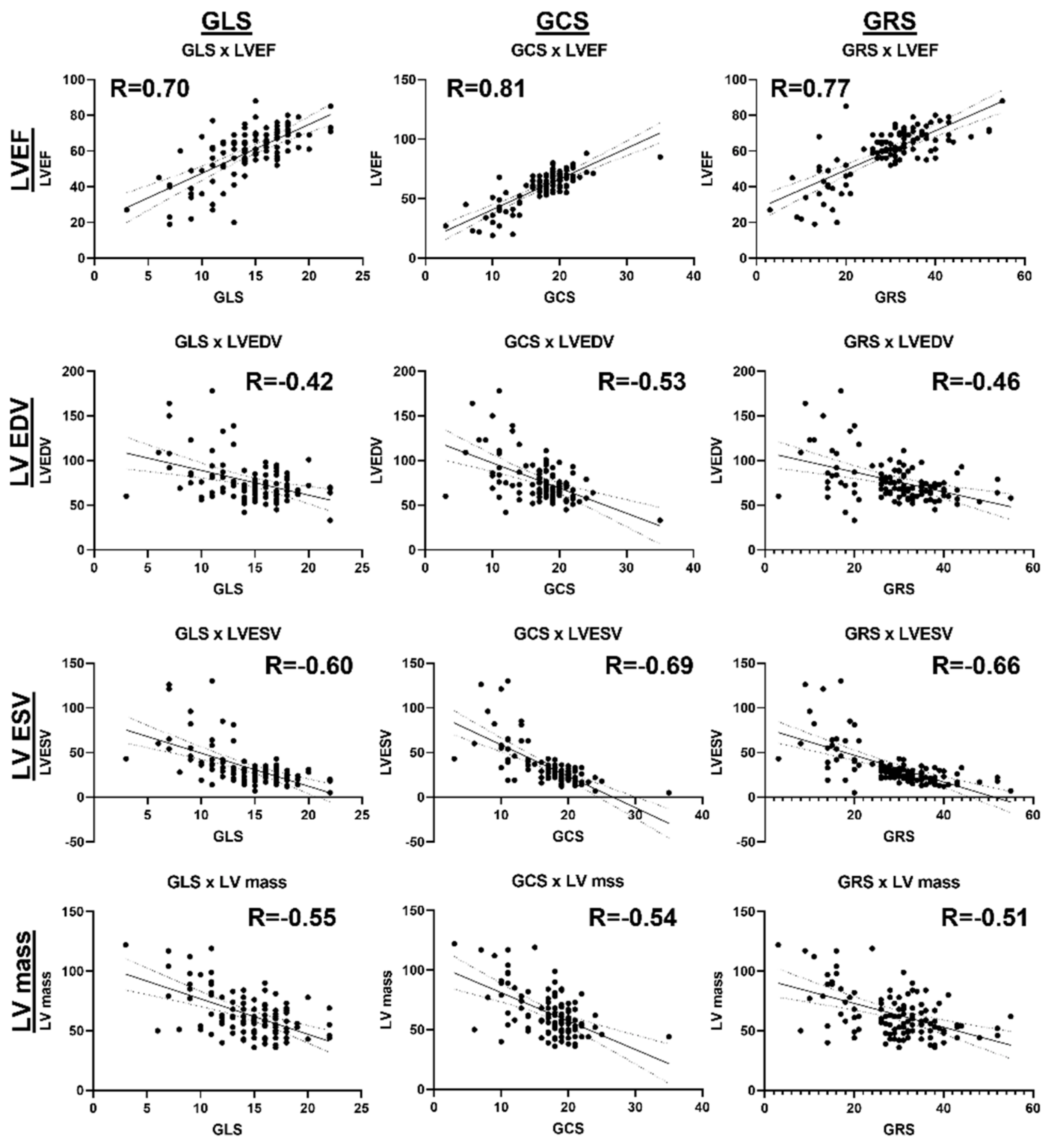
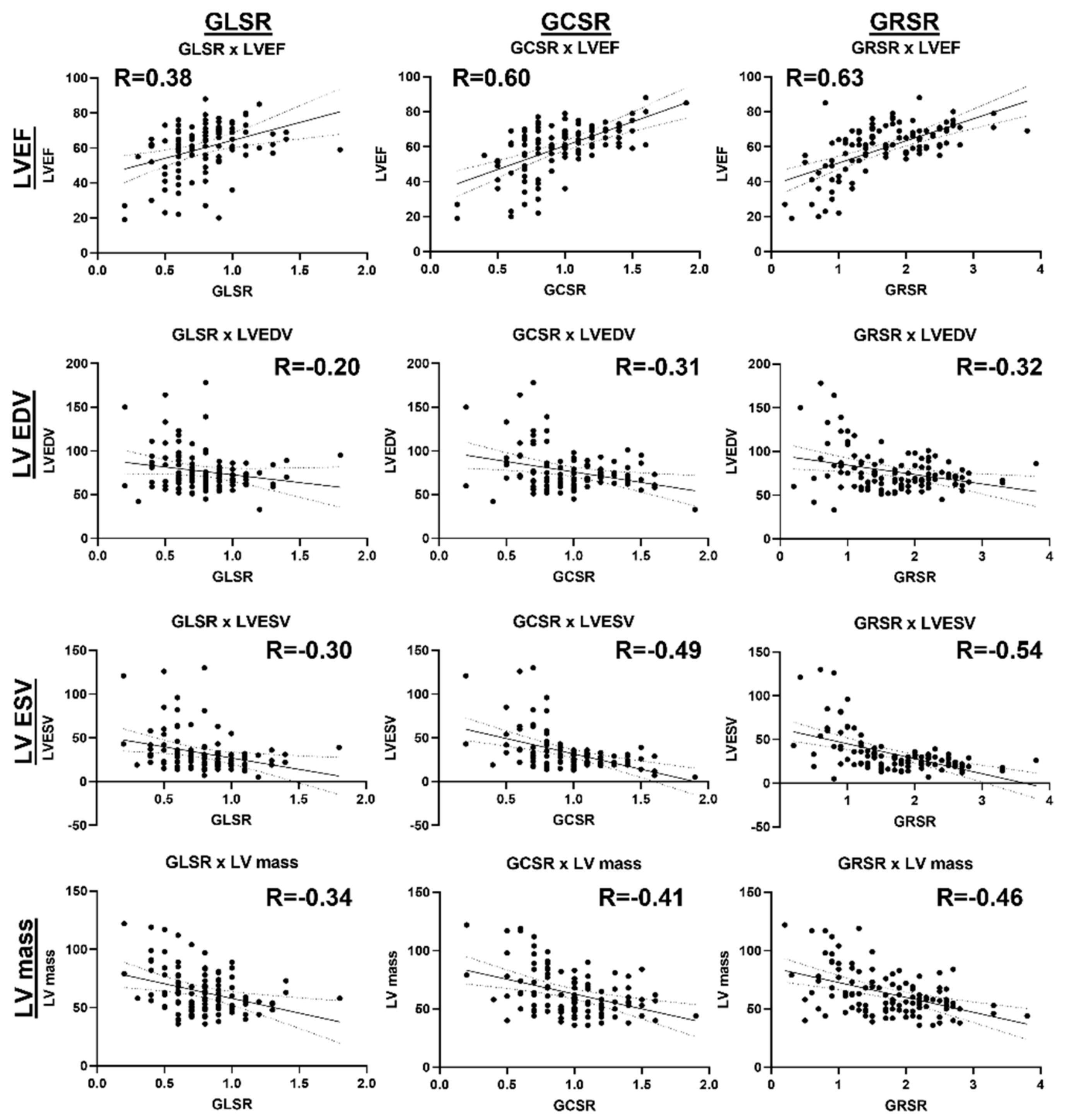
3.5. Associations between Cardiac Functional Parameters
4. Discussion
4.1. Study Findings and Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kravchenko, D.; Isaak, A.; Zimmer, S.; Mesropyan, N.; Reinert, M.; Faron, A.; Pieper, C.C.; Heine, A.; Velten, M.; Nattermann, J.; et al. Cardiac MRI in Patients with Prolonged Cardiorespiratory Symptoms after Mild to Moderate COVID-19. Radiology 2021, 301, E419–E425. [Google Scholar] [CrossRef]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef]
- Tan, Z.; Huang, S.; Mei, K.; Liu, M.; Ma, J.; Jiang, Y.; Zhu, W.; Yu, P.; Liu, X. The Prevalence and Associated Death of Ventricular Arrhythmia and Sudden Cardiac Death in Hospitalized Patients With COVID-19: A Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 8, 795750. [Google Scholar] [CrossRef]
- Writing, C.; Gluckman, T.J.; Bhave, N.M.; Allen, L.A.; Chung, E.H.; Spatz, E.S.; Ammirati, E.; Baggish, A.L.; Bozkurt, B.; Cornwell, W.K., 3rd; et al. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 79, 1717–1756. [Google Scholar]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Brito, D.; Meester, S.; Yanamala, N.; Patel, H.B.; Balcik, B.J.; Casaclang-Verzosa, G.; Seetharam, K.; Riveros, D.; Beto, R.J., 2nd; Balla, S.; et al. High Prevalence of Pericardial Involvement in College Student Athletes Recovering From COVID-19. JACC Cardiovasc. Imaging 2021, 14, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Salerno, M.; Kwong, R.Y. CMR in the Era of COVID-19: Evaluation of Myocarditis in the Subacute Phase. JACC Cardiovasc. Imaging 2020, 13, 2340–2342. [Google Scholar] [CrossRef] [PubMed]
- Ojha, V.; Verma, M.; Pandey, N.N.; Mani, A.; Malhi, A.S.; Kumar, S.; Jagia, P.; Roy, A.; Sharma, S. Cardiac Magnetic Resonance Imaging in Coronavirus Disease 2019 (COVID-19): A Systematic Review of Cardiac Magnetic Resonance Imaging Findings in 199 Patients. J. Thorac. Imaging 2021, 36, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zhao, P.; Tang, D.; Zhu, T.; Han, R.; Zhan, C.; Liu, W.; Zeng, H.; Tao, Q.; Xia, L. Cardiac Involvement in Patients Recovered From COVID-2019 Identified Using Magnetic Resonance Imaging. JACC Cardiovasc. Imaging 2020, 13, 2330–2339. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Tanacli, R.; Doeblin, P.; Gotze, C.; Zieschang, V.; Faragli, A.; Stehning, C.; Korosoglou, G.; Erley, J.; Weiss, J.; Berger, A.; et al. COVID-19 vs. Classical Myocarditis Associated Myocardial Injury Evaluated by Cardiac Magnetic Resonance and Endomyocardial Biopsy. Front. Cardiovasc. Med. 2021, 8, 737257. [Google Scholar] [CrossRef]
- Mustroph, J.; Hupf, J.; Baier, M.J.; Evert, K.; Brochhausen, C.; Broeker, K.; Meindl, C.; Seither, B.; Jungbauer, C.; Evert, M.; et al. Cardiac Fibrosis Is a Risk Factor for Severe COVID-19. Front. Immunol. 2021, 12, 740260. [Google Scholar] [CrossRef] [PubMed]
- Buckley, B.J.R.; Harrison, S.L.; Fazio-Eynullayeva, E.; Underhill, P.; Lane, D.A.; Lip, G.Y.H. Prevalence and clinical outcomes of myocarditis and pericarditis in 718,365 COVID-19 patients. Eur. J. Clin. Investig. 2021, 51, e13679. [Google Scholar] [CrossRef] [PubMed]
- Greulich, S.; Klingel, K. COVID-19 and Myocarditis: Findings from Cardiac Magnetic Resonance Imaging and Endomyocardial Biopsies. Hamostaseologie 2021, 41, 366–370. [Google Scholar] [CrossRef]
- Szarpak, L.; Pruc, M.; Filipiak, K.J.; Popieluch, J.; Bielski, A.; Jaguszewski, M.J.; Gilis-Malinowska, N.; Chirico, F.; Rafique, Z.; Peacock, F.W. Myocarditis: A complication of COVID-19 and long-COVID-19 syndrome as a serious threat in modern cardiology. Cardiol. J. 2022, 29, 178–179. [Google Scholar] [CrossRef] [PubMed]
- Peretto, G.; Sala, S.; Rizzo, S.; De Luca, G.; Campochiaro, C.; Sartorelli, S.; Benedetti, G.; Palmisano, A.; Esposito, A.; Tresoldi, M.; et al. Arrhythmias in myocarditis: State of the art. Heart Rhythm. 2019, 16, 793–801. [Google Scholar] [CrossRef]
- Tseng, Z.H.; Moffatt, E.; Kim, A.; Vittinghoff, E.; Ursell, P.; Connolly, A.; Olgin, J.E.; Wong, J.K.; Hsue, P.Y. Sudden Cardiac Death and Myocardial Fibrosis, Determined by Autopsy, in Persons with HIV. N. Engl. J. Med. 2021, 384, 2306–2316. [Google Scholar] [CrossRef] [PubMed]
- Aretz, H.T. Myocarditis: The Dallas criteria. Hum. Pathol. 1987, 18, 619–624. [Google Scholar] [CrossRef]
- Vidusa, L.; Kalejs, O.; Maca-Kaleja, A.; Strumfa, I. Role of Endomyocardial Biopsy in Diagnostics of Myocarditis. Diagnostics 2022, 12, 2104. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef] [PubMed]
- Aus dem Siepen, F.; Buss, S.J.; Messroghli, D.; Andre, F.; Lossnitzer, D.; Seitz, S.; Keller, M.; Schnabel, P.A.; Giannitsis, E.; Korosoglou, G.; et al. T1 mapping in dilated cardiomyopathy with cardiac magnetic resonance: Quantification of diffuse myocardial fibrosis and comparison with endomyocardial biopsy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 210–216. [Google Scholar] [CrossRef]
- Galea, N.; Marchitelli, L.; Pambianchi, G.; Catapano, F.; Cundari, G.; Birtolo, L.I.; Maestrini, V.; Mancone, M.; Fedele, F.; Catalano, C.; et al. T2-mapping increase is the prevalent imaging biomarker of myocardial involvement in active COVID-19: A Cardiovascular Magnetic Resonance study. J. Cardiovasc. Magn. Reson. 2021, 23, 68. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.E.; Aggarwal, S.K.; Phillips, N.J.; Soslow, J.H.; Dendy, J.M.; Hughes, S.G. Cardiac Magnetic Resonance in the Evaluation of COVID-19. Card. Fail. Rev. 2022, 8, e09. [Google Scholar] [CrossRef] [PubMed]
- Lamy, J.; Soulat, G.; Evin, M.; Huber, A.; de Cesare, A.; Giron, A.; Diebold, B.; Redheuil, A.; Mousseaux, E.; Kachenoura, N. Scan-rescan reproducibility of ventricular and atrial MRI feature tracking strain. Comput. Biol. Med. 2018, 92, 197–203. [Google Scholar] [CrossRef]
- Puzyrenko, A.; Jacobs, E.R.; Padilla, N.; Devine, A.; Aljadah, M.; Gantner, B.N.; Pan, A.Y.; Lai, S.; Dai, Q.; Rubenstein, J.C.; et al. Collagen-Specific HSP47(+) Myofibroblasts and CD163(+) Macrophages Identify Profibrotic Phenotypes in Deceased Hearts With SARS-CoV-2 Infections. J. Am. Heart Assoc. 2023, 12, e027990. [Google Scholar] [CrossRef]
- Wagoner, L.E.; Starling, R.C.; O’Connor, C.M. Cardiac function and heart failure. J. Am. Coll. Cardiol. 2006, 47 (Suppl. S11), D18–D22. [Google Scholar] [CrossRef][Green Version]
- Javed, Z.; Haisum Maqsood, M.; Yahya, T.; Amin, Z.; Acquah, I.; Valero-Elizondo, J.; Andrieni, J.; Dubey, P.; Jackson, R.K.; Daffin, M.A.; et al. Race, Racism, and Cardiovascular Health: Applying a Social Determinants of Health Framework to Racial/Ethnic Disparities in Cardiovascular Disease. Circ. Cardiovasc. Qual. Outcomes 2022, 15, e007917. [Google Scholar] [CrossRef]
- Graham, G. Disparities in cardiovascular disease risk in the United States. Curr. Cardiol. Rev. 2015, 11, 238–245. [Google Scholar] [CrossRef]
- Das, B.B.; Akam-Venkata, J.; Abdulkarim, M.; Hussain, T. Parametric Mapping Cardiac Magnetic Resonance Imaging for the Diagnosis of Myocarditis in Children in the Era of COVID-19 and MIS-C. Children 2022, 9, 1061. [Google Scholar] [CrossRef]
- Starekova, J.; Bluemke, D.A.; Bradham, W.S.; Eckhardt, L.L.; Grist, T.M.; Kusmirek, J.E.; Purtell, C.S.; Schiebler, M.L.; Reeder, S.B. Evaluation for Myocarditis in Competitive Student Athletes Recovering From Coronavirus Disease 2019 With Cardiac Magnetic Resonance Imaging. JAMA Cardiol. 2021, 6, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Shaw, L.J.; Min, J.K.; Page, C.B.; Berman, D.S.; Chaitman, B.R.; Picard, M.H.; Kwong, R.Y.; O’Brien, S.M.; Huang, Z.; et al. Outcomes in the ISCHEMIA Trial Based on Coronary Artery Disease and Ischemia Severity. Circulation 2021, 144, 1024–1038. [Google Scholar] [CrossRef] [PubMed]
- Mileva, N.; Paolisso, P.; Gallinoro, E.; Fabbricatore, D.; Munhoz, D.; Bergamaschi, L.; Belmonte, M.; Panayotov, P.; Pizzi, C.; Barbato, E.; et al. Diagnostic and Prognostic Role of Cardiac Magnetic Resonance in MINOCA: Systematic Review and Meta-Analysis. JACC Cardiovasc. Imaging 2023, 16, 376–389. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter (Unit) | Control | Excluded Myocarditis | Suspected Myocarditis |
|---|---|---|---|
| Number of subjects | 50 | 49 | 16 |
| Sex (M/F) | 24/26 | 19/30 | 9/7 |
| Age (years; mean ± SD) | 48 ± 15 | 44 ± 17 | 54 ± 15 |
| BSA (m2; mean ± SD) | 2.06 ± 0.29 | 2.11 ± 0.32 | 2.16 ± 0.31 |
| Heart rate (bpm; mean ± SD) | 64 ± 12 | 66 ± 13 | 74 ± 15 |
| Days between COVID diagnosis and MRI (mean ± SD) | -- | 176 ± 130 | 98 ± 106 |
| COVID vaccinated | 18 (36%) | 20 (41%) | 3 (19%) |
| White persons | 45 (90%) | 37 (76%) | 10 (63%) |
| Black persons | 5 (10%) | 9 (18%) | 5 (31%) |
| Other | 0 (0%) | 3 (6%) | 1 (6%) |
| Non-Hispanic | 50 (100%) | 47 (96%) | 15 (94%) |
| Hispanic | 0 (0%) | 2 (4%) | 1 (6%) |
| Hypertension | 18 (36%) | 7 (14%) | 9 (56%) |
| Hyperlipidemia | 15 (30%) | 5 (10%) | 4 (25%) |
| Diabetes | 6 (12%) | 3 (6%) | 6 (38%) |
| Obesity | 7 (14%) | 7 (14%) | 4 (25%) |
| Arrhythmias | 17 (34%) | 7 (14%) | 4 (25%) |
| Cardiomyopathy | 3 (6%) | 2 (4%) | 5 (31%) |
| CAD | 1 (2%) | 5 (10%) | 5 (31%) |
| HF | 10 (20%) | 7 (14%) | 11 (69%) |
| Parameter (Unit) | Control | Excluded Myocarditis | P1 | Suspected Myocarditis | P2/P3 |
|---|---|---|---|---|---|
| hsTn (ng/L) | 11.4 ± 6.6 | 11.9 ± 11.2 | 0.998 | 28.2 ± 20 | 0.101/0.117 |
| NT proBNP (pg/mL) | 187 ± 208 | 384 ± 452 | 0.336 | 627 ± 583 | 0.313/0.722 |
| hsCRP (mg/L) | 8.4 ± 9.5 | 4.4 ± 5.2 | 0.744 | 9.8 ± 9.7 | 0.991/0.343 |
| LV EF (%) #*† | 67 ± 7 | 58 ± 13 | <0.001 | 44 ± 17 | <0.001/0.014 |
| LV EDV (ml/m2) | 70 ± 12 | 78 ± 24 | 0.073 | 93 ± 37 | 0.070/0.382 |
| LV ESV (ml/m2) #* | 23 ± 7 | 35 ± 21 | 0.001 | 56 ± 36 | 0.008/0.108 |
| LV CI (L/min/m2) | 2.9 ± 0.7 | 2.8 ± 0.8 | 0.672 | 2.7 ± 0.8 | 0.567/0.942 |
| LV Mass (g/m2) | 61 ± 13 | 62 ± 19 | 0.975 | 78 ± 28 | 0.079/0.124 |
| RV EF (%) * | 56 ± 7 | 53 ± 10 | 0.113 | 46 ± 14 | 0.032/0.230 |
| RV EDV (ml/m2) | 79 ± 16 | 77 ± 20 | 0.942 | 78 ± 30 | >0.999/0.998 |
| RV ESV (ml/m2) | 35 ± 10 | 37 ± 14 | 0.709 | 44 ± 29 | 0.486/0.704 |
| RV CI (L/min/m2) | 2.8 ± 0.7 | 2.6 ± 0.8 | 0.346 | 2.6 ± 1.1 | 0.810/>0.999 |
| Parameter (Unit) | Control | Excluded Myocarditis | P1 | Suspected Myocarditis | P2/P3 |
|---|---|---|---|---|---|
| GLS (abs %) #*† | 16 ± 3 | 14 ± 4 | 0.023 | 11 ± 4 | <0.001/0.021 |
| LS-B (abs %) *† | 20 ± 4 | 19 ± 5 | 0.376 | 14 ± 4 | <0.001/<0.001 |
| LS-M (abs %) #* | 14 ± 3 | 12 ± 4 | 0.013 | 11 ± 4 | 0.021/0.661 |
| LS-A (abs %) | 14 ± 4 | 13 ± 4 | 0.641 | 11 ± 6 | 0.111/0.298 |
| GCS (abs %) #*† | 19 ± 2 | 17 ± 5 | 0.019 | 13 ± 5 | <0.001/0.013 |
| CS-B (abs %) *† | 18 ± 3 | 17 ± 5 | 0.301 | 12 ± 4 | <0.001/0.007 |
| CS-M (abs %) #*† | 19 ± 3 | 16 ± 5 | 0.010 | 12 ± 5 | 0.001/0.035 |
| CS-A (abs %) *† | 24 ± 3 | 22 ± 7 | 0.120 | 17 ± 6 | <0.001/0.033 |
| GRS (%) #*† | 34 ± 7 | 28 ± 10 | 0.004 | 20 ± 9 | <0.001/0.008 |
| RS-B (%) #*† | 32 ± 7 | 28 ± 9 | 0.033 | 20 ± 9 | <0.001/0.009 |
| RS-M (%) #*† | 32 ± 8 | 26 ± 9 | 0.002 | 19 ± 10 | <0.001/0.044 |
| RS-A (%) #*† | 51 ± 13 | 42 ± 18 | 0.020 | 30 ± 14 | <0.001/0.024 |
| GLSR (1/s) * | 0.9 ± 0.27 | 0.7 ± 0.22 | 0.058 | 0.6 ± 0.24 | 0.003/0.114 |
| LSR-B (1/s) *† | 1.3 ± 0.43 | 1.2 ± 0.41 | 0.294 | 0.9 ± 0.28 | <0.001/0.017 |
| LSR-M (1/s) | 0.9 ± 0.27 | 0.8 ± 0.28 | 0.986 | 0.7 ± 0.29 | 0.074/0.117 |
| LSR-A (1/s) | 0.9 ± 0.33 | 0.9 ± 0.31 | >0.999 | 0.8 ± 0.35 | 0.165/0.171 |
| GCSR (1/s) *† | 1.0 ± 0.24 | 1.0 ± 0.32 | 0.937 | 0.6 ± 0.23 | <0.001/<0.001 |
| CSR-B (1/s) *† | 1.1 ± 0.27 | 1.0 ± 0.36 | 0.649 | 0.7 ± 0.29 | <0.001/<0.001 |
| CSR-M (1/s) *† | 1.1 ± 0.26 | 1.0 ± 0.35 | 0.629 | 0.6 ± 0.27 | <0.001/<0.001 |
| CSR-A (1/s) *† | 1.5 ± 0.41 | 1.5 ± 0.50 | 0.881 | 1.1 ± 0.43 | <0.002/0.012 |
| GRSR(abs 1/s) *† | 1.9 ± 0.56 | 1.8 ± 0.73 | 0.441 | 1.0 ± 0.49 | <0.001/<0.001 |
| RSR-B (abs 1/s) *† | 2.1 ± 0.63 | 1.8 ± 0.73 | 0.092 | 1.1 ± 0.64 | <0.001/0.002 |
| RSR-M (abs 1/s) *† | 1.8 ± 0.46 | 1.6 ± 0.64 | 0.290 | 0.9 ± 0.46 | <0.001/<0.001 |
| RSR-A (abs 1/s) *† | 3.3 ± 1.11 | 3.0 ± 1.54 | 0.607 | 1.9 ± 1.07 | <0.001/0.006 |
| Parameter (Unit) | Controls | Excluded Myocarditis | P1 | Suspected Myocarditis | P2/P3 |
|---|---|---|---|---|---|
| LGE (subjects) | 0 | 11 | -- | 15 | -- |
| ECV-G (%) *† | 29 ± 3 | 30 ± 4 | 0.486 | 34 ± 4 | <0.001/0.007 |
| ECV-B (%) *† | 29 ± 3 | 28 ± 4 | 0.934 | 34 ± 4 | <0.001/<0.001 |
| ECV-M (%) *† | 28 ± 3 | 29 ± 3 | 0.979 | 33 ± 4 | 0.003/0.005 |
| ECV-A (%) * | 30 ± 3 | 32 ± 8 | 0.247 | 35 ± 5 | 0.006/0.312 |
| T1_3T-G (ms) * | 1226 ± 59 | 1268 ± 50 | 0.081 | 1301 ± 40 | 0.003/0.118 |
| T1_3T-B (ms) * | 1228 ± 56 | 1266 ± 63 | 0.126 | 1301 ± 40 | 0.003/0.108 |
| T1_3T-M (ms) * | 1218 ± 59 | 1261 ± 53 | 0.075 | 1299 ± 50 | 0.004/0.134 |
| T1_3T-A (ms) | 1236 ± 70 | 1293 ± 80 | 0.075 | 1301 ± 53 | 0.050/0.969 |
| T1_1.5T-G (ms) *† | 975 ± 44 | 1017 ± 77 | 0.346 | 1143 ± 74 | 0.013/0.042 |
| T1_1.5T-B (ms) | 1005 ± 35 | 1039 ± 58 | 0.307 | 1199 ± 128 | 0.070/0.111 |
| T1_1.5T-M (ms) * | 983 ± 58 | 1006 ± 89 | 0.842 | 1116 ± 78 | 0.045/0.102 |
| T1_1.5T-A (ms) * | 936 ± 64 | 1011 ± 103 | 0.160 | 1079 ± 41 | <0.001/0.241 |
| T2_3T-G (ms) #* | 39 ± 3 | 42 ± 4 | 0.030 | 43 ± 2 | 0.014/0.896 |
| T2_3T-B (ms) #* | 38 ± 2 | 42 ± 4 | 0.008 | 43 ± 3 | 0.007/0.801 |
| T2_3T-M (ms) * | 39 ± 3 | 42 ± 4 | 0.078 | 43 ± 2 | 0.038/0.833 |
| T2_3T-A (ms) | 41 ± 4 | 44 ± 4 | 0.186 | 43 ± 4 | 0.402/0.970 |
| T2_1.5T-G (ms) #*† | 45 ± 2 | 50 ± 3 | 0.003 | 54 ± 3 | 0.002/0.048 |
| T2_1.5T-B (ms) #*† | 44 ± 1 | 48 ± 3 | 0.012 | 53 ± 2 | 0.001/0.015 |
| T2_1.5T-M (ms) #*† | 46 ± 1 | 50 ± 3 | 0.003 | 53 ± 2 | <0.001/0.033 |
| T2_1.5T-A (ms) #* | 47 ± 3 | 51 ± 3 | 0.025 | 55 ± 4 | 0.025/0.235 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, E.-S.H.; Rubenstein, J.; Sosa, A.; Stojanovska, J.; Pan, A.; North, P.; Rui, H.; Benjamin, I. Myocardial Strain for the Differentiation of Myocardial Involvement in the Post-Acute Sequelae of COVID-19—A Multiparametric Cardiac MRI Study. Tomography 2024, 10, 331-348. https://doi.org/10.3390/tomography10030026
Ibrahim E-SH, Rubenstein J, Sosa A, Stojanovska J, Pan A, North P, Rui H, Benjamin I. Myocardial Strain for the Differentiation of Myocardial Involvement in the Post-Acute Sequelae of COVID-19—A Multiparametric Cardiac MRI Study. Tomography. 2024; 10(3):331-348. https://doi.org/10.3390/tomography10030026
Chicago/Turabian StyleIbrahim, El-Sayed H., Jason Rubenstein, Antonio Sosa, Jadranka Stojanovska, Amy Pan, Paula North, Hallgeir Rui, and Ivor Benjamin. 2024. "Myocardial Strain for the Differentiation of Myocardial Involvement in the Post-Acute Sequelae of COVID-19—A Multiparametric Cardiac MRI Study" Tomography 10, no. 3: 331-348. https://doi.org/10.3390/tomography10030026
APA StyleIbrahim, E.-S. H., Rubenstein, J., Sosa, A., Stojanovska, J., Pan, A., North, P., Rui, H., & Benjamin, I. (2024). Myocardial Strain for the Differentiation of Myocardial Involvement in the Post-Acute Sequelae of COVID-19—A Multiparametric Cardiac MRI Study. Tomography, 10(3), 331-348. https://doi.org/10.3390/tomography10030026