

Evaluation of Radiation Exposure and Influential Factors in Cone-Beam Computed Tomography (CBCT) of the Head and Abdomen during Interventional Procedures

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
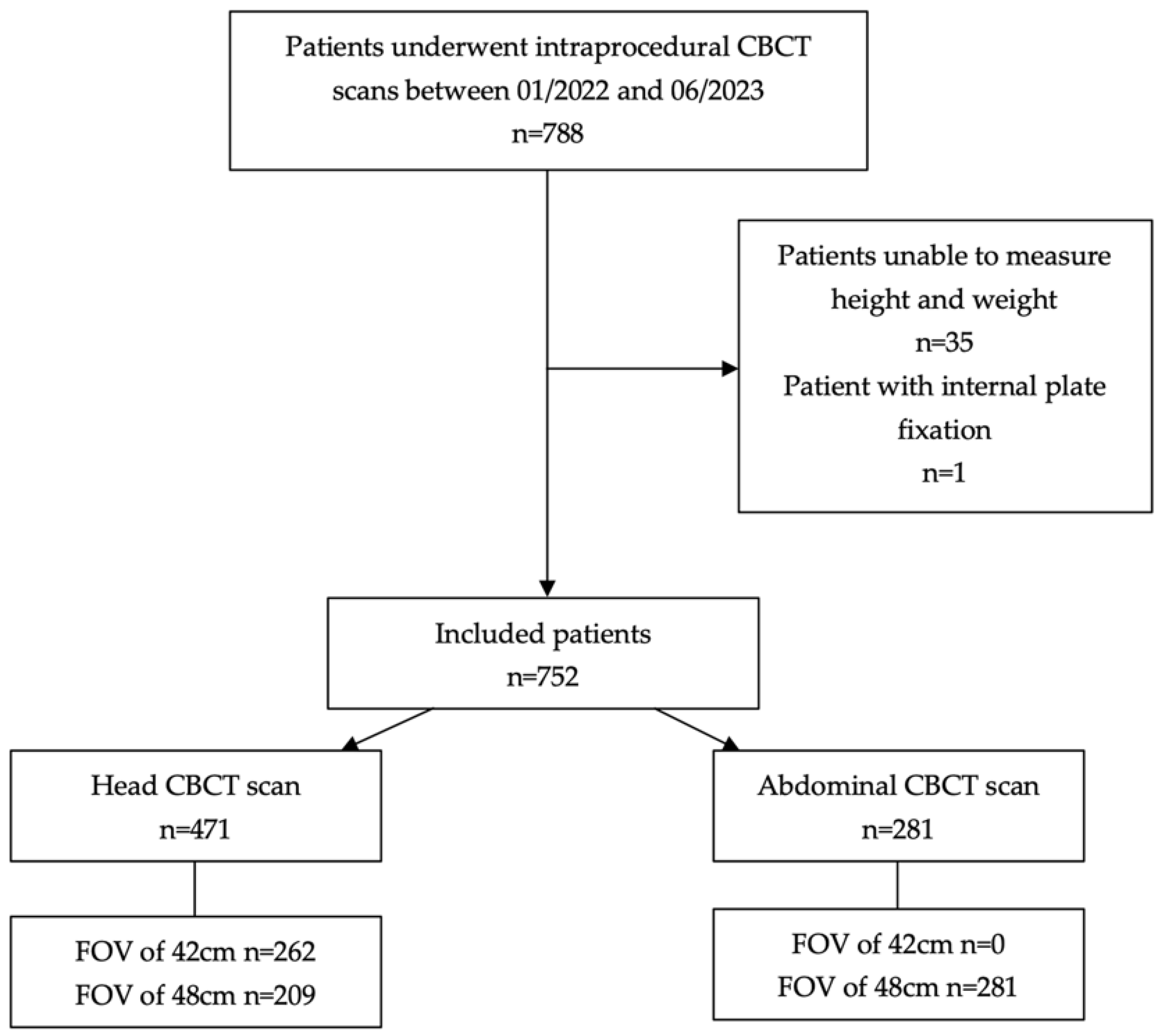
2.1. Study Population
2.2. CBCT System and Protocols
2.3. Patient Radiation Exposure Measurement
2.4. Data Collection and Outcomes
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Assessment of Patient Radiation Dose and Affecting Factors
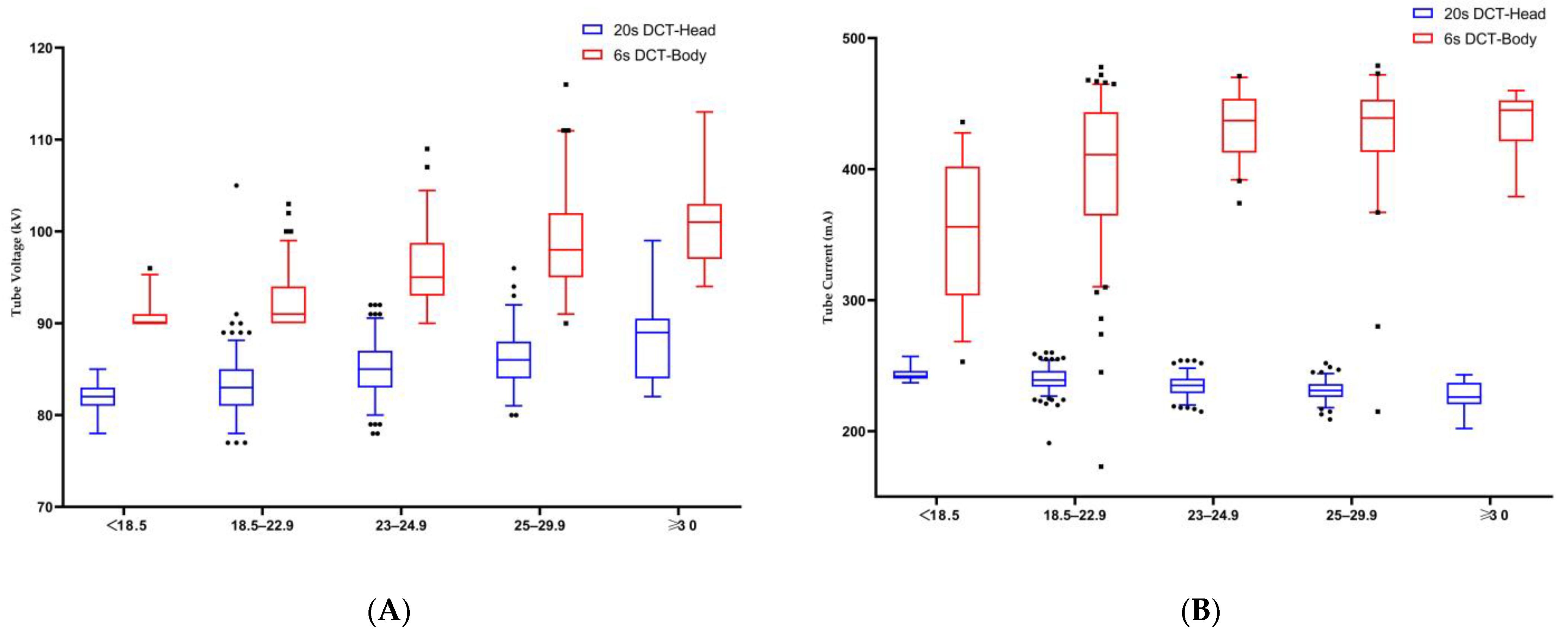
3.3. Modulation of Exposure Parameters under AEC
3.4. Multiple Regression Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Floridi, C.; Radaelli, A.; Abi-Jaoudeh, N.; Grass, M.; Lin, M.; Chiaradia, M.; Geschwind, J.F.; Kobeiter, H.; Squillaci, E.; Maleux, G.; et al. C-arm cone-beam computed tomography in interventional oncology: Technical aspects and clinical applications. Radiol. Med. 2014, 119, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Raz, E.; Nossek, E.; Sahlein, D.H.; Sharashidze, V.; Narayan, V.; Ali, A.; Esparza, R.; Peschillo, S.; Chung, C.; Diana, F.; et al. Principles, techniques and applications of high resolution cone beam CT angiography in the neuroangio suite. J. Neurointerv. Surg. 2023, 15, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Berczeli, M.; Chinnadurai, P.; Veress, D.S.; Diaz, O.; Bavare, C.S.; Lumsden, A.B. Added Value of Selective Intra-arterial Cone-Beam CT Angiography in the Management of Visceral Artery Aneurysms. J. Endovasc. Ther. 2022, 15266028221118510. [Google Scholar] [CrossRef] [PubMed]
- Mezzetto, L.; Mastrorilli, D.; Abatucci, G.; Scorsone, L.; Macri, M.; Criscenti, P.; Onorati, F.; Gennai, S.; Veraldi, E.; Veraldi, G.F. Impact of Cone Beam Computed Tomography in Advanced Endovascular Aortic Aneurysm Repair Using Last Generation 3D C-arm. Ann. Vasc. Surg. 2022, 78, 132–140. [Google Scholar] [CrossRef]
- Fronda, M.; Mistretta, F.; Calandri, M.; Ciferri, F.; Nardelli, F.; Bergamasco, L.; Fonio, P.; Doriguzzi Breatta, A. The Role of Immediate Post-Procedural Cone-Beam Computed Tomography (CBCT) in Predicting the Early Radiologic Response of Hepatocellular Carcinoma (HCC) Nodules to Drug-Eluting Bead Transarterial Chemoembolization (DEB-TACE). J. Clin. Med. 2022, 11, 7089. [Google Scholar] [CrossRef] [PubMed]
- Fior, D.; Vacirca, F.; Leni, D.; Pagni, F.; Ippolito, D.; Riva, L.; Sironi, S.; Corso, R. Virtual Guidance of Percutaneous Transthoracic Needle Biopsy with C-Arm Cone-Beam CT: Diagnostic Accuracy, Risk Factors and Effective Radiation Dose. Cardiovasc. Intervent. Radiol. 2019, 42, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Jiao, D.; Ren, K.; Li, Z.; Shui, S.; Han, X. Clinical role of guidance by C-arm CT for (125)I brachytherapy on pulmonary tumors. Radiol. Med. 2017, 122, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, D.; Gurajala, R.K.; Kapoor, B.; Setser, R.; Karuppasamy, K. Relationship between cone-beam CT technique and diagnostic usefulness in patients undergoing embolotherapy for hepatocellular carcinoma. Clin. Radiol. 2017, 72, 993.e1–993.e6. [Google Scholar] [CrossRef]
- Kothary, N.; Abdelmaksoud, M.H.; Tognolini, A.; Fahrig, R.; Rosenberg, J.; Hovsepian, D.M.; Ganguly, A.; Louie, J.D.; Kuo, W.T.; Hwang, G.L.; et al. Imaging guidance with C-arm CT: Prospective evaluation of its impact on patient radiation exposure during transhepatic arterial chemoembolization. J. Vasc. Interv. Radiol. 2011, 22, 1535–1543. [Google Scholar] [CrossRef]
- Jonczyk, M.; Collettini, F.; Geisel, D.; Schnapauff, D.; Boning, G.; Wieners, G.; Gebauer, G. Radiation exposure during TACE procedures using additional cone-beam CT (CBCT) for guidance: Safety and precautions. Acta Radiol. 2018, 59, 1277–1284. [Google Scholar] [CrossRef]
- Abuzaid, M.M.; Elshami, W.; Jayachandran, D.; Korappil, N.; Tekin, H.O. Establishment of Diagnostic Reference Levels in Cone Beam Computed Tomography Scans in the United Arab Emirates. Tomography 2022, 8, 2939–2945. [Google Scholar] [CrossRef]
- Suzuki, S.; Yamaguchi, I.; Kidouchi, T.; Yamamoto, A.; Masumoto, T.; Ozaki, Y. Evaluation of effective dose during abdominal three-dimensional imaging for three flat-panel-detector angiography systems. Cardiovasc. Intervent. Radiol. 2011, 34, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Kwok, Y.M.; Irani, F.G.; Tay, K.H.; Yang, C.C.; Padre, C.G.; Tan, B.S. Effective dose estimates for cone beam computed tomography in interventional radiology. Eur. Radiol. 2013, 23, 3197–3204. [Google Scholar] [CrossRef] [PubMed]
- Bai, M.; Liu, B.; Mu, H.; Liu, X.; Jiang, Y. The comparison of radiation dose between C-arm flat-detector CT (DynaCT) and multi-slice CT (MSCT): A phantom study. Eur. J. Radiol. 2012, 81, 3577–3580. [Google Scholar] [CrossRef] [PubMed]
- Tyan, Y.S.; Li, Y.Y.; Ku, M.C.; Huang, H.H.; Chen, T.R. The effective dose assessment of C-arm CT in hepatic arterial embolisation therapy. Br. J. Radiol. 2013, 86, 20120551. [Google Scholar] [CrossRef]
- Kawauchi, S.; Chida, K.; Hamada, Y.; Tsuruta, W. Image Quality and Radiation Dose of Conventional and Wide-Field High-Resolution Cone-Beam Computed Tomography for Cerebral Angiography: A Phantom Study. Tomography 2023, 9, 1683–1693. [Google Scholar] [CrossRef]
- Petroulia, V.D.; Kaesmacher, J.; Piechowiak, E.I.; Dobrocky, T.; Pilgram-Pastor, S.M.; Gralla, J.; Wagner, F.; Mordasini, P. Evaluation of Sine Spin flat detector CT imaging compared with multidetector CT. J. Neurointerv. Surg. 2023, 15, 292–297. [Google Scholar] [CrossRef]
- Kim, D.J.; Park, M.K.; Jung, D.E.; Kang, J.H.; Kim, B.M. Radiation Dose Reduction without Compromise to Image Quality by Alterations of Filtration and Focal Spot Size in Cerebral Angiography. Korean J. Radiol. 2017, 18, 722–728. [Google Scholar] [CrossRef]
- Mantis, C.; Papadakis, E.; Anadiotis, A.; Kafkas, N.; Patsilinakos, S. Factors affecting radiation exposure during transradial cardiac catheterisation and percutaneous coronary intervention. Clin. Radiol. 2022, 77, e387–e393. [Google Scholar] [CrossRef]
- Klein, A.; Xi, Y.; Guild, J.; Tsai, S.; Ramanan, B.; Chamseddin, K.; Timaran, C.; Kirkwood, M. The Effects of Gender on Radiation Dose during Fenestrated Endovascular Aneurysm Repair. Ann. Vasc. Surg. 2020, 68, 305–309. [Google Scholar] [CrossRef]
- Madder, R.D.; VanOosterhout, S.; Mulder, A.; Ten Brock, T.; Clarey, A.T.; Parker, J.L.; Jacoby, M.E. Patient Body Mass Index and Physician Radiation Dose During Coronary Angiography. Circ. Cardiovasc. Interv. 2019, 12, e006823. [Google Scholar] [CrossRef] [PubMed]
- Kyriakou, Y.; Richter, G.; Dorfler, A.; Kalender, W.A. Neuroradiologic applications with routine C-arm flat panel detector CT: Evaluation of patient dose measurements. AJNR Am. J. Neuroradiol. 2008, 29, 1930–1936. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Zimmet, P.; Caterson, I.; Chunming, C.; Ikeda, Y.; Khalid, D.; Kim, Y.; Bassett, J. The Asia-Pacific perspective: Redefining obesity and its treatment; Health Communications Australia Pty Limited: Sydney, Australia, 2002; pp. 17–19. [Google Scholar]
- Vano, E.; Miller, D.L.; Martin, C.J.; Rehani, M.M.; Kang, K.; Rosenstein, M.; Ortiz-Lopez, P.; Mattsson, S.; Padovani, R.; Rogers, A.; et al. ICRP Publication 135: Diagnostic Reference Levels in Medical Imaging. Ann. ICRP 2017, 46, 1–144. [Google Scholar] [CrossRef] [PubMed]
- Piron, L.; Le Roy, J.; Cassinotto, C.; Delicque, J.; Belgour, A.; Allimant, C.; Beregi, J.P.; Greffier, J.; Molinari, N.; Guiu, B. Radiation Exposure During Transarterial Chemoembolization: Angio-CT Versus Cone-Beam CT. Cardiovasc. Intervent. Radiol. 2019, 42, 1609–1618. [Google Scholar] [CrossRef]
- Doerfler, A.; Golitz, P.; Engelhorn, T.; Kloska, S.; Struffert, T. Flat-Panel Computed Tomography (DYNA-CT) in Neuroradiology. From High-Resolution Imaging of Implants to One-Stop-Shopping for Acute Stroke. Clin. Neuroradiol. 2015, 25 Suppl. 2, 291–297. [Google Scholar] [CrossRef]
- Struffert, T.; Hauer, M.; Banckwitz, R.; Kohler, C.; Royalty, K.; Doerfler, A. Effective dose to patient measurements in flat-detector and multislice computed tomography: A comparison of applications in neuroradiology. Eur. Radiol. 2014, 24, 1257–1265. [Google Scholar] [CrossRef]
- Suzuki, S.; Furui, S.; Yamaguchi, I.; Yamagishi, M.; Watanabe, A.; Abe, T.; Kobayashi, I. Effective dose during abdominal three-dimensional imaging with a flat-panel detector angiography system. Radiology 2009, 250, 545–550. [Google Scholar] [CrossRef]
- Kawauchi, S.; Chida, K.; Moritake, T.; Hamada, Y.; Matsumaru, Y.; Tsuruta, W.; Sato, M.; Hosoo, H.; Sun, L. Treatment of Internal Carotid Aneurysms Using Pipeline Embolization Devices: Measuring the Radiation Dose of the Patient and Determining the Factors Affecting It. Radiat. Prot. Dosimetry 2020, 188, 389–396. [Google Scholar] [CrossRef]
- Suomi, V.; Jarvinen, J.; Kiviniemi, T.; Ylitalo, A.; Pietila, M. Full feature selection for estimating KAP radiation dose in coronary angiographies and percutaneous coronary interventions. Comput. Biol. Med. 2020, 120, 103725. [Google Scholar] [CrossRef]
- Inoue, Y.; Mori, M.; Itoh, H.; Mitsui, K.; Miyatake, H.; Yamane, T.; Hata, H. Age-Dependent Changes in Effective Dose in Pediatric Brain CT: Comparisons of Estimation Methods. Tomography 2023, 10, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Yel, I.; Booz, C.; Albrecht, M.H.; Gruber-Rouh, T.; Polkowski, C.; Jacobi, M.; Lenga, L.; Schulz, M.; Frank, J.; Marzi, I.; et al. Optimization of image quality and radiation dose using different cone-beam CT exposure parameters. Eur. J. Radiol. 2019, 116, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Kirisattayakul, W.; Pattum, P.; Munkong, W.; Prabsattroo, T.; Khottapat, C.; Chomkhunthod, T.; Pungkun, V. Comparing Radiation Dose of Cerebral Angiography Using Conventional and High kV Techniques: A Retrospective Study on Intracranial Aneurysm Patients and a Phantom Study. Tomography 2023, 9, 621–632. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Parameters | 20sDCT-Head | 6sDCT-Body |
|---|---|---|
| Exposure | 70 kVp | 90 kVp |
| Pulse width | 12.5 ms | 5.0 ms |
| Frame rate | 0.4°/F | 0.5°/F |
| Rotation | 200° | 200° |
| Imaging start position | 98 LAO; 0 CRA | 168 RAO; 0 CRA |
| Number of frames | 496 frames | 397 frames |
| Exposure time | 20.0 s | 6.0 s |
| Detector size | 30 × 40 cm | 30 × 40 cm |
| Field of view | 42 cm, 48 cm | 48 cm |
| Protocols | Parameters | Female | Male | p-Value |
|---|---|---|---|---|
| Number | n = 198 | n = 273 | ||
| DAP (Gy⋅cm2) | 53.1 (49.6–63.1) | 54.2 (51.2–65.6) | <0.0001 | |
| 20sDCT-Head | RAK (mGy) | 212 (206–219) | 221 (214–227) | <0.0001 |
| Tube Voltage (kV) | 83 (81–85) | 86 (84–88) | <0.0001 | |
| Tube Current (mA) | 240 (235–245) | 232 (227–237) | <0.0001 | |
| Number | n = 93 | n = 188 | ||
| DAP (Gy⋅cm2) | 41.0 (34.6–49.0) | 50.1 (43.6–55.7) | <0.0001 | |
| 6sDCT-Body | RAK (mGy) | 135 (114.5–161.5) | 165 (144–184) | <0.0001 |
| Tube Voltage (kV) | 92 (90–94.5) | 95 (91–98.8) | <0.0001 | |
| Tube Current (mA) | 398 (346.5–435.5) | 432 (398.3–449.5) | <0.0001 |
| Protocols | Parameters | FOV 42 cm | FOV 48 cm | p-Value |
|---|---|---|---|---|
| Number | n = 262 | n = 209 | ||
| DAP (Gy⋅cm2) | 50.8 (49.1–52.4) | 64.8 (62.8–66.9) | <0.0001 | |
| 20sDCT-Head | RAK (mGy) | 220 (213–227) | 214 (207–220) | <0.0001 |
| Tube Voltage (kV) | 85 (83–87) | 85 (82–87) | 0.671 | |
| Tube Current (mA) | 235 (230–241) | 235 (230–242) | 0.874 |
| Parameters | BMI, <18.5 | BMI, 18.5–22.9 | BMI, 23–24.9 | BMI, 25–29.9 | BMI, ≥30 | p-Value |
|---|---|---|---|---|---|---|
| Number | n = 10 | n = 176 | n = 129 | n = 139 | n = 17 | |
| DAP (Gy⋅cm2) | 50.8 (48.2–62.4) | 52.8 (49.6–63.4) | 53.7 (50.7–64.9) | 54.1 (51.5–64.5) | 63.9 (53.6–69.3) | 0.001 |
| RAK (mGy) | 211.5 (203–220.3) | 213 (207.3–220) | 219 (211.5–224) | 221 (214–228) | 228 (217–236.5) | <0.0001 |
| Tube voltage (kV) | 82 (80.5–83) | 83 (81–85) | 85 (83–87) | 86 (84–88) | 89 (84–90.5) | <0.0001 |
| Tube current (mA) | 243.5 (240.8–247.8) | 239 (234–246) | 235 (229–240) | 231 (226–236) | 226 (220.5–237) | <0.0001 |
| Parameters | BMI, <18.5 | BMI, 18.5–22.9 | BMI, 23–24.9 | BMI, 25–29.9 | BMI, ≥30 | p-Value |
|---|---|---|---|---|---|---|
| Number | n = 33 | n = 121 | n = 56 | n = 60 | n = 11 | |
| DAP (Gy⋅cm2) | 35.8 (29.9–39.9) | 43.5 (37.5–48.2) | 52.3 (47.4–55.6) | 54.7 (50.5–60.4) | 59.9 (51.2–60.9) | <0.0001 |
| RAK (mGy) | 118 (98.5–132) | 144 (123.5–159) | 172.5 (156.3–183) | 180(167–199) | 198 (169–201) | <0.0001 |
| Tube voltage (kV) | 90 (90–91) | 91 (90–94) | 95 (93–98.8) | 98 (95.3–102) | 101 (97–103) | <0.0001 |
| Tube current (mA) | 356 (303.5–402) | 411 (363–443.5) | 437 (412.5–453.8) | 439 (413–452.8) | 444 (421–453) | <0.0001 |
| Protocols | Variables | Reg Coef. | Std Coef. | (95% CI) | p-Value |
|---|---|---|---|---|---|
| 6sDCT-Body | Age | −0.001 | −0.001 | (−0.073/0.071) | 0.985 |
| R2 = 0.529 | Male sex | 7.525 | 0.35 | (5.767/9.283) | <0.0001 |
| BMI | 1.752 | 0.628 | (1.525/1.979) | <0.0001 | |
| 20sDCT-Head | Age | −0.043 | −0.066 | (−0.062/−0.023) | <0.0001 |
| R2 = 0.895 | Male sex | 2.297 | 0.151 | (1.84/2.753) | <0.0001 |
| BMI | 0.304 | 0.134 | (0.237/0.371) | <0.0001 | |
| FOV 48 cm | 13.997 | 0.926 | (13.551/14.443) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.; Qu, W.; Zhang, D.; Zhong, B.; Li, Z.; Jiang, Z.; Ni, G.; Ni, C. Evaluation of Radiation Exposure and Influential Factors in Cone-Beam Computed Tomography (CBCT) of the Head and Abdomen during Interventional Procedures. Tomography 2024, 10, 320-330. https://doi.org/10.3390/tomography10030025
Li M, Qu W, Zhang D, Zhong B, Li Z, Jiang Z, Ni G, Ni C. Evaluation of Radiation Exposure and Influential Factors in Cone-Beam Computed Tomography (CBCT) of the Head and Abdomen during Interventional Procedures. Tomography. 2024; 10(3):320-330. https://doi.org/10.3390/tomography10030025
Chicago/Turabian StyleLi, Mingming, Weiwei Qu, Dong Zhang, Binyan Zhong, Zhi Li, Zhengyu Jiang, Guanyin Ni, and Caifang Ni. 2024. "Evaluation of Radiation Exposure and Influential Factors in Cone-Beam Computed Tomography (CBCT) of the Head and Abdomen during Interventional Procedures" Tomography 10, no. 3: 320-330. https://doi.org/10.3390/tomography10030025
APA StyleLi, M., Qu, W., Zhang, D., Zhong, B., Li, Z., Jiang, Z., Ni, G., & Ni, C. (2024). Evaluation of Radiation Exposure and Influential Factors in Cone-Beam Computed Tomography (CBCT) of the Head and Abdomen during Interventional Procedures. Tomography, 10(3), 320-330. https://doi.org/10.3390/tomography10030025