Abstract
Background: Discrimination, racism, harassment, stereotyping, and bullying are a significant issue for medical students as they create a hostile environment with detrimental effect on student wellbeing and educational experience. Findings suggest that though prevalent, reporting of these experiences is rare and perceived as ineffective. Objectives: This scoping review aims to map the trends, types, and nature of discrimination, harassment, bullying, stereotyping, intimidation, and racism reports in undergraduate medical education in the UK since 2010 and to determine areas of focus for undertaking full systematic reviews in the future. Method: A search was conducted using the MEDLINE, AHMED, CINHL, and EMBASE electronic databases from 2010 up to February 2022 in English. Only primary research papers (e.g., cohort studies, cross-sectional studies, and case series) that report the words/phrases discrimination (including gender and racial), harassment (including verbal, sexual, academic, and physical), bullying, stereotype, intimidation, and racism within medical education in the UK after 2010, following the Equity Act 2010, were eligible for inclusion. Results: Five relevant articles relating to discrimination, harassment, bullying, stereotyping, intimidation, and racism in medical schools in the UK were included. Three themes were identified across these studies. Conclusions: The data suggest that there is a high prevalence rate of discrimination, harassment, and stereotyping being experienced by ethnic minority undergraduate medical students in the UK. There is underreporting due to perceived and structural barriers. The identified studies suggest that less progress has been made in these areas.
1. Introduction
More than a third of all UK medical students are from ethnically diverse backgrounds. However, all too often, individuals from ethnic minorities encounter social barriers and micro-aggressions whilst at medical school and during placements in the community (Fnais et al. 2014). One of the core duties of universities and medical schools is to protect the health and welfare of students enrolled on a medical course, and this means also during clinical placements and community activities. Although more than 24% of medical students report racial harassment (EHRC 2019), only half of the UK medical schools even collect data on this issue. A recent report calls this inaction ‘turning a blind eye on racism’ (Kmietowicz 2020).
Racial harassment and discrimination are not unique to the UK. For example, a large cross-sectional survey and retrospective cohort study by Hill et al. (2020) in the United States comprising 27,504 graduate students from 140 accredited US medical schools showed that women, racial/ethnic minorities, and sexual orientation minorities appear to experience a disproportionate burden of the mistreatment reported in medical schools. These reports of racial/ethnic discrimination included being denied opportunities for training or rewards based on race/ethnicity, being subjected to racially/ethnically offensive remarks or names, and receiving lower evaluations or grades solely because of race/ethnicity. Furthermore, these minoritised students reported a higher prevalence of experiencing two or more types of mistreatment compared with White students.
Racial harassment in medical education is often interconnected with other scoped forms of discrimination, as it can be a manifestation of broader institutional, structural, and systemic racism within medical education (Green et al. 2022; FitzGerald and Hurst 2017; Sue et al. 2007). Examples of scoped forms of discrimination can include implicit biases where faculty members, for instance may, unconsciously favour or disfavour certain students based on their race or ethnicity, leading to differential treatment or negative comments. It can also involve microaggressions, which are subtle, often unintentional acts or comments that convey negative messages or stereotypes about a person’s race or ethnicity. Another common form is institutional discrimination when it is built into the policies, practices, and systems of medical education institutions (Alexander and Arday 2015).
Clinicians and medical educators are expected to treat all medical students, staff, and patients equally according to the General Medicine Council (GMC) statement on equality, diversity, and inclusion (GMC 2022). However, this is often not the shared experience of people from affected ethnic minority groups. The GMC have joined the Medical School Council’s Equality, Diversity and Inclusion Alliance to demonstrate their support for initiatives to make learning environments and undergraduate training processes more inclusive (GMC 2022). Reported examples are underrepresentation at senior management level (UK medical schools’ executive leadership is predominately White, whereas around 41% of medical students are from ethnic minorities), an unbalanced ethnically diverse student/staff mix, and less supportive learning and development environment. Together, these factors may explain why ethnic minority students are more likely to struggle with integration into university life, are more frequently reporting negative student experiences, are less likely to access academic support services, and are more likely to experience differential attainment in assessment (Arday and Mirza 2018; Alexander and Shankley 2020; EHRC 2019; Haq et al. 2005; Woolf 2009; Woolf et al. 2011; Universities UK 2019).
The growing number of ethnic minority students enrolling on medicine courses and the need to have a diverse healthcare workforce to look after an increasingly culturally diverse patient population has fuelled the imperative need to address differential lived experiences of racism and discrimination in UK medical schools. The fact that ethnic minority doctors seem to continue to suffer bullying and harassment and poorer career progression indicates an unacceptable situation, considering the shortage of UK trained doctors and the negative impact this has on individuals’ health and well-being (BMA 2022; Nagpaul 2022a, 2022b; RCP 2019).
Supporting the development of diverse and inclusive learning environments, where students are supported to achieve their full potential, is key to tackling inequalities in educational outcomes. UK medical schools are ideally positioned to drive change by firstly actively challenging racism in medical education and healthcare, including in clinical placements, and, secondly, by teaching future physicians how to dismantle inequalities when they are still in formative stages of their careers.
While bullying, undermining behaviour, and harassment in the medical workplace in the UK have received due attention (Carter et al. 2013; General Medical Council 2014; Johnson 2016; Halim and Riding 2018), their scale within undergraduate medical education has rarely been considered. We have, therefore, set out to scope the primary literature with the following specific objectives:
- -
- To map the types and nature of primary research activities concerning the extent and experience of discrimination, harassment, stereotyping, bullying, and victimisation in undergraduate medical education since the UK Parliament passed the Equality Act (2010). This act has been designated as a crucial landmark and main source of legal protection in the UK from racial harassment for university staff and students. The 2010 Act ensures that medical education institutions must provide equal opportunities for all students, regardless of their background or protected characteristics. This means that students must be given the same access to education, training, and resources, regardless of their protected characteristics. By following up on research after the Equality Act (2010) in this review, we anticipate that researchers, policymakers, and practitioners may identify areas where discrimination and inequality persist and develop strategies to address them.
- -
- To summarise and disseminate the current state of primary research activities concerning discrimination, harassment, stereotyping, bullying, and victimisation in undergraduate medical education and areas of content focus.
- -
- To determine areas of focus for undertaking full future systematic reviews of content.
- -
- To identify gaps in the existing evidence base in the context of discrimination, harassment, stereotyping, bullying, and victimisation in undergraduate medical education, providing directions for future research for the content of primary and secondary research.
2. Methods
For this scoping review, the methodology for scoping reviews as described by Arksey and O’Malley (2005) was utilised. This scoping review complies with the PRISMA-ScR (preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews) checklist (Tricco et al. 2018). To support the use of this approach within the educational context, the STORIES (structured approach to the reporting in healthcare education of evidence synthesis) statement (Gordon and Gibbs 2014) and BEME guidance (Hammick et al. 2010) were adopted to guide this report. This approach for scoping reviews in medical health education reviews has been used previously (Daniel et al. 2021).
This scoping review followed the five stages of a scoping review (Arksey and O’Malley 2005):
Stage 1: identifying the research aims/questions (described above);
Stage 2: identifying relevant studies;
Stage 3: study selection;
Stage 4: charting the data;
Stage 5: collating, summarising, and reporting the results.
2.1. Stage 2: Identifying Relevant Studies
Four reviewers (AB, JW, NA, and CI) performed a comprehensive search of the literature in two stages. Firstly, a broad search on MEDLINE using the keywords discrimination, harassment, bullying, stereotype, intimidation, and racism was conducted to identify the appropriate databases and index terms used to develop a comprehensive search strategy. The second search was performed across the electronic databases MEDLINE (Ovid), Embase (Ovid), and Cinahl (EBSCO), using the identified keywords and index terms, on 5th February 2022. The search was limited to English primary studies conducted in the UK ranging from 2010 to February 2022, since the passing of the Equality Act (2010) in the UK.
2.2. Stage 3: Study Selection
The PEO format (population, exposure, outcome) was used to guide study eligibility criteria, as depicted in Table 1.

Table 1.
Study eligibility criteria.
Only peer-reviewed primary research papers (qualitative, quantitative, and mixed-method studies) in undergraduate medical education that report any form of discrimination (racial, gender, institutional, etc.), harassment (verbal, sexual, academic, physical), bullying, stereotyping, intimidation, or bias in UK medical schools following the Equality Act (2010) were eligible for inclusion.
Secondary research papers (guidelines, systematic reviews, literature reviews), ideas, editorials, opinion letters, and studies conducted on non-medical undergraduate students or those on postgraduate medical students were excluded from the scope.
Three reviewers independently screened the articles from each database using the above criteria. All articles that contained the search terms in their title and/or abstract were included for a full text review. After deduplication, the full texts of the eligible articles were also hand-searched to identify potentially eligible studies. Discrepancies at all stages were resolved through discussion until consensus was reached and, when needed, involved two additional authors (CI and TGH).
2.3. Stage 4: Charting the Data
The articles were independently extracted by three authors (AM, CI, and TGH) into a custom-made spreadsheet where the data were stored, organised, and coded. When complete, data were cross-checked by a second reviewer.
The data extracted for each included study are listed below:
- ▪
- Article identifiers (author(s), journal, and year of publication);
- ▪
- Geographic location;
- ▪
- Aim of the article, methods, ethics approval, and funding;
- ▪
- Number of participants;
- ▪
- Key findings in relation to the scope, conclusion, and limitations.
2.4. Stage 5: Collating, Summarising, and Reporting the Results
The data from the charting form were collated and summarised as per the sections above. Tables and diagrams we used for easy visualisation and mapping of the current evidence base related to the scope. After charting the data, articles were classified into themes developed via an inductive approach during the full text review and discussed between the three reviewers to reach agreement on the themes. A narrative synthesis approach was used to present the scope, nature, and focus of the included studies.
This enabled us to have an overview of the state of the art of research activities regarding any form of discrimination, harassment, bullying, stereotyping, intimidation, or bias in UK undergraduate medical schools over the last twenty-two years and to provide directions for future primary and secondary research in the field.
3. Results
A total of 11,312 records were identified through searching of the three databases. After deduplication and title and abstract screening, 17 records were sourced for full text review. Of these, 12 full-text articles were excluded for the following reasons: seven records were not primary studies but guidelines, commentaries, letters, editorials, and review articles, while five records did not meet the population inclusion criteria, i.e., studies were not related to undergraduate medical students.
Five studies fully met the eligibility criteria and were included in this scoping review (Morrison et al. 2019; Claridge et al. 2018; Broad et al. 2018; Yeates et al. 2017; Roberts et al. 2010). The PRISMA flow diagram (Figure 1) depicts the stages of the study selection process.
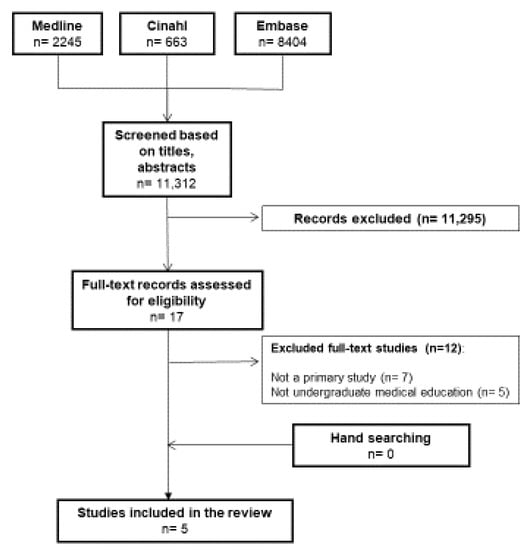
Figure 1.
PRISMA flowchart showing retrieval of articles used in the review.
The summary of included studies is presented in Table A1. Excluded studies and reasons for exclusion are provided in Table A2 (Table A1 and Table A2 can be found in Appendix A).
3.1. Descriptive Findings: Characteristics of Included Studies
Three studies (Morrison et al. 2019; Claridge et al. 2018; Roberts et al. 2010) were of a qualitative nature (focus groups and interviews), while one study (Broad et al. 2018) used a mixed method (focus groups and survey). One study was described as a randomised double-blind internet-based controlled trial (Yeates et al. 2017) in which participants analysed scripted video material and performed different cognitive tests.
Two studies were published in 2018 (Broad et al. 2018; Claridge et al. 2018) and the other three were published in 2019, 2017, and 2010, respectively (Morrison et al. 2019; Yeates et al. 2017; Roberts et al. 2010).
One study (Broad et al. 2018) was conducted in a Bristol medical school, one study in London (Claridge et al. 2018), one in Manchester (Yeates et al. 2017), one in the West Midlands (Morrison et al. 2019), and one study involved two medical schools located the North West (Roberts et al. 2010).
All five studies disclosed ethics approval, mentioned that data were anonymised and handled in compliance with the General Data Protection Regulations, and declared no competing interests.
Source of funding were mentioned in all but one study (Roberts et al. 2010). Three studies (Broad et al. 2018; Claridge et al. 2018; Yeates et al. 2017) received university funding, while one (Morrison et al. 2019) did not receive any funding.
3.2. Characteristics of Participants
The number of participants ranged from 24 (Morrison et al. 2019) to 259 that participated in a survey (Broad et al. 2018). One study (Broad et al. 2018) included students across all years of undergraduate entry, one study (Roberts et al. 2010) included undergraduate students in year one and two, and Morrison et al. (2019) explored the experiences of undergraduate training among multiple cohorts of graduate-entry medical students. Participants in one study also included staff and medical examiners along with undergraduate medical students (Claridge et al. 2018), while the study by Yeates et al. (2017) was conducted on current UK undergraduate Objective Structured Clinical Exam (OSCE) examiners and did not include students.
The demographic background of participants also differed across the studies. Participants identified as Black and Minority Ethnic (BME) only were included in two studies (Morrison et al. 2019; Roberts et al. 2010), with mixed White and BME backgrounds in three studies (Broad et al. 2018; Claridge et al. 2018; Yeates et al. 2017). One study (Claridge et al. 2018) excluded non-British and non-domestic students.
During thematic and content analysis, three themes were revealed. These comprised (1) the prevalence of discrimination and harassment and barriers to reporting, (2) differential attainment by ethnicity in medical undergraduate training, and (3) barriers to learning about culture, race, and ethnicity.
3.2.1. Prevalence of Discrimination and Harassment and Barriers to Reporting
The prevalence of discrimination and harassment in undergraduate medical school setting was assessed in only one study (Broad et al. 2018), and reporting was assessed in two studies (Broad et al. 2018; Morrison et al. 2019).
(a) Prevalence and experiences of discrimination and harassment
Survey findings suggest that of 259 survey responders, 211 (81.5%, 95% CI: 76.3 to 85.7) students had either experienced (63.3%, 95% CI: 57.3 to 69.0) or witnessed (56.4%, 95% CI: 50.3 to 62.3) at least one type of discrimination or harassment. BME, religious, and non-heterosexual students, students with disabilities, and female students were more likely to experience or witness individual types of discrimination or harassment.
Qualitative results from the focus groups showed that everyday discrimination and harassment such as invasions of personal space, the use of ethnic/racial teasing or jokes, belittlement, and derogatory language around protected characteristics (described in 56 instances) were perceived as normalised behaviour. Structural direct and indirect discrimination or harassment, in which the learning environment encouraged some and excluded other students based on protected characteristics, was reported in 16 statements. Students described 20 events concerning exceptional discrimination or harassment associated with actions or words used by educators that directly abused or excluded participants, including bullying and sexual harassment.
(b) Barriers to reporting
In the study of Broad et al. (2018), despite the high percentage of students that had either experienced or witnessed discrimination or harassment (81.5%, 95% CI: 76.3 to 85.7), only seven students had reported these (5.0%, 95% CI: 2.4 to 10, n = 140 survey respondents). The confidence of reporting discrimination or harassment to medical or university staff was very low (21.3%, 95% CI: 16.8 to 26). The lack of understanding of the challenges minority students face, inaccessible, ineffective, and burdensome reporting system, and lack of trust in institutions were highlighted in both studies (Broad et al. 2018; Morrison et al. 2019). Notably, fear of personal consequences after reporting described most as “potential victimisation, fears of impacts on their progress outcomes, assessments, education and career prospects, and fears of being labelled within a hierarchical context” was stated on 33 occasions in the study of Broad et al. (2018).
3.2.2. Differential Attainment by Ethnicity in Medical Undergraduate Training
Attainment gap and lower academic performance among BME students was investigated in three studies. Two studies (Morrison et al. 2019; Claridge et al. 2018) assessed the reasons for lower attainment among students, and two studies (Yeates et al. 2017; Claridge et al. 2018) investigated reasons for lower attainment from the perspective of the staff involved as educators and examiners.
Student interviews raised multiple issues as possible barriers to performance, which we grouped as social factors (social integration, social networking, and family) and stereotyping. Social networking is defined as social relationships students build with peers and senior colleagues. These relationships are often a source of support and resource mining. Peers often share multiple common interests. This can also encompass social interactions (Claridge et al. 2018). Social integration is a type of cultural incorporation, whereby students sharing particular characteristics/interests are invited into an established social network to become part of a micro-community. This community, in turn, provides each member with support, resources, and a feeling of belonging. Those deemed to be outsiders will be refused access to these benefits (Vaughan 2013).
Social integration and social networking are essential to learning and increasing performance, and were the most common social factor reported across the studies. BME students felt actively excluded or assumed they could not be part of the group due to perceived differences (Morrison et al. 2019; Claridge et al. 2018). This resulted in students feeling invisible, excluded, and biased against, made integration difficult to apparent ethnic divisions (Claridge et al. 2018), and reduced access to peer resources (Morrison et al. 2019). Some students felt uncomfortable attending events (lecturers or revision groups) organised by student societies (Claridge et al. 2018) and felt more comfortable among other ethnic minorities, especially because of the small number of BME students in each cohort (Morrison et al. 2019).
The role of the family as another social factor that was perceived as a possible barrier to performance was investigated by Claridge et al. (2018). Family responsibilities such as caring, chores, or curfews seemed to have an impact on students’ social and academic lives.
In both studies, students highlighted experiencing and/or witnessing prejudice and stereotyping by other students and teaching and training staff or related to course content. A lack of appreciation of cultural differences among students and staff, lack of BME representation among medical school staff, and offensive behaviour towards BME staff and of medical staff or patients towards BME students were common issues across the studies (Morrison et al. 2019; Claridge et al. 2018), leading to changes in student behaviour, e.g., appearance, clothing, being quieter, moderating their accent, etc. as a sense of responsibility to represent themselves and their ethnic group in a positive light (Morrison et al. 2019).
Staff interviews in the study of Claridge et al. (2018) raised two possible barriers to lower performance grouped as social factors (social integration, social networking, and family) and student–staff behaviour. Staff often perceived family pressure in the choice of course students take, which has a negative impact on academic performance. Additionally, fewer opportunities for BME students to socialise and network with both students and staff and a university structure that is not suitable for a diverse range of students were also reported. Changes in student behaviour, e.g., the way students speak in order to seem more “like a doctor”, or struggling with group work, as well as religious duties, staff insensitivity to students from different ethnicities, and insensitive behaviour of students towards BME staff, could possibly cause academic issues.
The study of Yeates et al. (2017) investigated the influence of racial stereotype bias on examiners’ scores, feedback, and recollections in undergraduate clinical exams using near-identical videos of medical student performances on a simulated OSCE using British Asian and White British actors. The findings suggested that although Asian stereotypes were activated (or at least active) in examiners’ minds (examiners responded to Asian stereotypical words faster than to neutral words (716 ms, 95% CI 702–731 ms vs. 769 ms, 95% CI 753–786 ms, p < 0.001)), examiner bias did not explain the lower attainment of Asian students, as it did not have an influence on examiners’ score, feedback, or memories for one performance.
3.2.3. Barriers to Learning about Culture, Race, and Ethnicity
One study (Roberts et al. 2010) assessed the way undergraduate medical students made sense of their learning experiences related to cultural diversity in two medical schools (School A, n = 30 and School B, n = 19) in the north of England with contrasting pedagogical approaches to teaching (paper-based problem-based learning, PBL), with cases of a series of clinical index situations and a personal and professional development (PPD) module delivered by practising doctors taught in small groups (10–12 student).
Despite the pedagogical approach used, two major competitive barriers to learning across both schools were identified: institutional marginalisation and student resistance.
Both medical schools were seen as institutions that failed to prioritise and encourage constructive discussion about ethnicity and cultural diversity, although cultural competence was perceived as essential for students’ successful professional practice.
In contrast, students showed individual resistance towards the topic, as it was perceived as less important compared to the biomedicine subjects. Additionally, students did not consider medical schools as an appropriate environment that would successfully support learning on the topic and felt that this would be better achieved by social networking and by students’ own peer groups.
4. Discussion
This scoping review examines available published primary research articles on discrimination, harassment, and stereotyping in medical undergraduate education in the UK since the Equality Act was published in 2010. To our knowledge, this is the first scoping review that reviews research articles in this topic area in the UK. The literature synthesis highlights significant gaps in the literature on discrimination, harassment, and stereotyping in medical education. Our findings emphasise how common the problem continues to be in undergraduate medical UK programmes despite its apparent underreporting (Kmietowicz 2020). These findings suggest that less progress has been made since the introduction of the Equality Act in 2010. Therefore, more efforts and resources are needed to explore and address existing structural and cultural barriers at the institutional, clinical, and academic training level. Inaction on these matters will not only have negative consequences for future doctors, academic performance and welfare, but also for closing the workforce shortage gap due to the potential dropout of students from clinical training courses.
With regard to our identified prevalence of discrimination and harassment theme, there is a clear tendency in the included studies of a high prevalence of discrimination and harassment experienced by medical students in UK medical schools. A meta-analytic study published in 2014 clearly confirms this trend (Fnais et al. 2014). When they extracted data from 51 studies, the authors found that 59.4% of medical trainees had experienced at least one form of harassment or discrimination during their training. Another piece of evidence supporting the high trend in our review comes from a report published by the Equality and Human Rights Commission using data from 141 UK universities (EHRC 2019). The findings revealed that 24% of students from an ethnic minority background said that they had experienced racial harassment manifesting in the form of racist name-calling, insults, and jokes. Medical students interviewed in this report mentioned examples of racial harassment from patients and hospital staff as well as senior clinicians they were shadowing during their clinical placements. Underreporting of incidences seems to be another significant issue frequently reported in our reviewed studies and highlighted as a real concern in dossiers evaluating racial reporting systems in higher education institutions in the UK (EHRC 2019). Worrying about the negative consequences of speaking up and raising complaints is particularly problematic in medical education, where fears of repercussions are imminent due to the close nature of the academic and clinical assessment of students by clinical professionals (EHRC 2019; Broad et al. 2018). Our UK findings in this subtheme resonate with international studies. A narrative review of discrimination experienced by medical students across a number of countries including the USA, Sweden, and Australia concluded that “discrimination is widely experienced and underreported by medical students, who are not empowered to challenge supervisors and senior staff” (Ng et al. 2019, p. 581). An interesting finding of the review concerned the types of discrimination. Most of the affected students observed racist remarks and derogatory labelling, and experienced differential treatment. The authors also reported on students’ responses to discrimination, which were described as negative or problematic and included experienced psychological states of anger, fear, anxiety, depression, and trauma (Ng et al. 2019). Similar to our findings in the UK, medical students across the included studies were reluctant to report mistreatment and discrimination.
Differential attainment by ethnicity in medical undergraduate training is another theme in our review that led to research in medical education. A meta-analytic study including sixteen reports measuring academic performance in undergraduate medical assessment found that students from ethnic minority backgrounds are up to three times more likely to fail an examination compared to their White counterparts (Woolf et al. 2011). The attainment gap found in medicine seems to match trends in UK higher education. The most recent data among 2017–18 graduates show a 13% gap between the likelihood of White students and students from ethnic minority backgrounds achieving a first- or upper second-class degree (Universities UK 2019). Woolf et al. (2011) conclude, in their work on medical education, that “ethnic differences in attainment seem to be a consistent feature of medical education in the UK, being present across medical schools, exam types, and undergraduate and postgraduate assessments, and have persisted for at least the past three decades” (p. 12). A narrative review in the United States compared the academic performance of underrepresented minority medical students (URM) to non-URM. The authors confirmed the overall findings in the UK. They conclude that ‘URM students consistently scored lower on, or were more likely to fail, standardized exams, such as the USMLE and its predecessor, the National Board of Medical Examiners (NBME) exam’ (Orom et al. 2013, p. 1768). In addition, with regard to academic progress, their findings showed that URM students were more likely than non-URM students to experience graduation delays and failure.
The reasons for this gap in attainment are complex and multifaceted (Alexander and Shankley 2020; Esmail and Everington 2021; Woolf et al. 2011). At the individual level, underlying mechanisms can be related to stereotype threats (Steele and Aronson 1995; Woolf et al. 2008), implicit racial bias (Van Ryn et al. 2011), and micro-aggressions (Ackerman-Barger et al. 2020). At the assessment level, for example during OSCEs, there is a risk of unconscious bias and stereotype activation, as explored by Yeates et al. (2017) using an experimental research method. At the institutional level, there is now wide recognition, as highlighted in many reports (EHRC 2019; Universities UK 2019), that toxic cultures and structural barriers play a crucial role (Arday and Mirza 2018). This is further confirmed internationally. For example, a number of US studies found differential experiences of URM compared to non-URM perceptions of medical schools’ social environment, social support, and students’ satisfaction with their learning environment (Orom et al. 2013). A strong sense of belonging, racially diverse and inclusive environments, and a diverse and culturally trained teaching workforce are identified remedies to close the attainment gap for ethnic minority medical students (Woolf 2020).
Barriers to learning about culture, race, and ethnicity were a frequent theme across all studies in our review. Roberts et al. (2010), for example, found that despite the differential EDI pedagogy and approaches in the two studied medical schools/institutions, it is students who posed stronger resistance to formally learning about cultural diversity. They felt a topic of that gravity would be better taught through social situations, as there is a perceived disconnect between teaching methods and their practical application. Another barrier identified in these studies (Broad et al. 2018; Claridge et al. 2018; Morrison et al. 2019; Roberts et al. 2010) was how ill-equipped, uncomfortable, or uninterested teaching staff were to teach about diversity, discrimination, and racism. These findings will be especially useful for medical schools who are exploring the effectiveness of EDI training and the question of where this content is positioned in the curriculum, in which format, and who delivers it. Given that EDI training is a new addition to most university curricula, the impact of EDI at the medical school level is still relatively unknown, so there is a need to focus on EDI evaluation and implementation research. A meta-analytical integration of over 40 years of research on diversity training evaluation paints a rather complex and mixed picture of the effectiveness of diversity training. Importantly, the positive effects of diversity training were greater when training was complemented by other diversity initiatives, targeted to both awareness and skills development, and conducted over a significant period of time. One significant limitation of diversity training seems to be the time factor. The authors compared the immediate versus long-term effects of diversity training and found that diversity training effects on reactions and attitudinal/affective learning decayed over time (Bezrukova et al. 2016). More recent evidence also suggests that a systems approach to training interventions that includes different stakeholders in the organization is more effective (Curtis et al. 2007). These research findings have important implications for medical schools, as they indicate not only challenges regarding training content and design but also organizational support and penetration across all units of educational delivery.
5. Limitations
One limitation of our review is the small number of studies assessing the scope, prevalence, and trends of harassment and discrimination in the investigated twelve-year period. Underreporting and inaccessible and inefficient reporting systems must be addressed if we want to stop or lower the prevalence of harassment and discrimination. Another limitation is the narrow search: from 2010 onwards and the inclusion of studies focusing on undergraduate medical education only. However, given that the Equality Act (2010) was introduced in the UK at the time to reduce racial inequality and address discrimination, we considered it as relevant to review if there was any progress made in the last twelve years. The focus on undergraduate medical students is also not trivial, given that the formative years are crucial for students’ professional development and their perception of the clinical environment. Lastly, as per the scoping review approach, the quality of included studies was not assessed, and this should be taken into consideration when extrapolating results.
6. Conclusions
Our scoping review suggests that there is a high prevalence rate of discrimination, harassment, and stereotyping experienced by ethnic minority undergraduate medical students in the UK. Although it is increasingly being seen as an area of concern across the UK higher education sector, including medical schools, there is noticeably less primary research being conducted in the UK compared to other countries with a similarly ethnically diverse student population, such as the United States and Canada. Exploring and comprehending the lived experiences of UK medical students, however, will not only allow institutions to better equip themselves to deal with diversity and the changing landscape, but equally increase the intake rate of students with minority and wider participation backgrounds. The fact that ethnic minority students seem to feel that educators are often failing to protect them is an urgent call for action.
With a clearer understanding of the structural barriers, more constructive solutions can be created to assist institutions in effectively monitoring racism, harassment, and discrimination whilst also reducing the attainment gap. In sum, the gap in research and policy implementation, such as a robust reporting system, would suggest that less progress than anticipated has been made since the introduction of the Equality Act in 2010.
Future research may include the following:
- The prevention and effective monitoring of harassment and discrimination in medical educational institutions;
- The standardisation of tools that measure harassment and discrimination;
- Detailed reporting on specific areas of any type of inequity in medical education are needed;
- One area of research here that requires quantitative analysis is the barrier to reporting; this may inform future interventions and reporting systems.
Author Contributions
Conceptualization, A.M.; methodology, T.G.-H.; data curation, H.A., B.A., J.W., N.A., C.I.; writing—original draft preparation, A.M., C.I.; writing—review and editing, A.M., T.G.-H., H.A., B.A., J.W., N.A., C.I. All authors have read and agreed to the published version of the manuscript.
Funding
University of Central Lancashire, The Institute of Citizenship, Society and Change (ICSC).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Summary of included articles.
Table A1.
Summary of included articles.
| Study ID and Location | Aims, Objectives | Study Type | Recruitment, Sampling, Data Collection, and Analysis | Participant Description | Results | Limitations | Conclusions |
|---|---|---|---|---|---|---|---|
| Broad et al. (2018) Bristol | 1. Prevalence of harassment and discrimination 2. Reporting and factors that influence reporting | Mixed-method: quantitative survey, qualitative free-text reporting, and two single-gendered focus groups | 1318 medical students were e-mailed twice in March 2014. Convenience sampling was used to recruit eight male and eight female focus group participants for two focus groups. 16 students were included in the focus groups. Proportions and confidence intervals (CIs) were analysed using the Wilson score method, and associations were assessed with chi-squared analysis. The focus groups: framework analysis for the qualitative data and degrees of convergence. | 259 medical students all year groups. Gender: M 83 F 167, ethnicity: White 192, BME 61, heterosexual: 291, disability: 9 | 259 students responded to the survey (20%). Most participants experienced (63.3%, 95% CI 57.3 to 69.0) or witnessed (56.4%, 95% CI 50.3 to 62.3) at least one type of discrimination or harassment. Stereotyping was the most commonly witnessed (43.2%, 95%CI 37.4 to 49.3). Black and minority ethnic (BME) students witnessed and religious students experienced higher lack of provision (X2 4.73, p = 0.03; X2 4.38, p = 0.04); non-heterosexual students experienced higher joking, (X2 3.99, p = 0.04); students with disabilities experienced more stereotyping (X2 13.5, p < 0.01). Female students and students in clinical years had 2.6 (95% CI 1.3 to 5.3) and 3.6 (95% CI 1.9 to 7.0) greater likelihood of experiencing or witnessing all types of discrimination and harassment, respectively. Seven students reported incidents (5%, 95%CI 2.4 to 10.0); reporting was perceived as ineffective and victimising. | No validated questionnaire. The small sample size and the self-selected nature of the sample limit the conclusions. | Harassment and discrimination are prevalent in this sample and associated with gender, ethnicity, sexuality, disability, and year group. Reporting was rare and perceived as ineffective. |
| Study ID and Location | Aims, Objectives | Study Type | Recruitment, Sampling, Data Collection, and Analysis | Participant Description | Results | Limitations | Conclusions |
| Claridge et al. (2018) London | Exploring experiences of medical and biomedical science students and factors contributing to lower attainment | Qualitative, focus groups Audio-recorded, semi-structured interviews and ethnically homogenous student-led focus groups | An invitation was emailed to all ‘home’ students on undergraduate biomedical sciences and medicine courses (n = 1862) Exclusion: non-British non-domestic students. Participants for six focus groups were purposively recruited by ethnicity; Asian/Asian British (‘Asian’), Black/African/Caribbean/Black British (‘Black’), or White: English/Welsh/Scottish/Northern Irish/British. Staff range from lecturers to deans. | 41 students and 8 staff. 41 student participants with mean (SD, range) age = 21 (2.78, 18 to 31). Interviews were conducted with 24 students (12 female, 12 male, nine biomedical sciences, 15 medicine), with the following from each ethnicity: Asian: Bangladeshi (1), Chinese (1), Indian (5), Pakistani (3), and Other (2); Black: African (2) and Caribbean (1); White (8); and Irish (1) | Student data were best explained by two main themes: social factors and stereotyping, whilst staff data were also best explained by two main themes: social factors and student and staff behaviour. Social factors suggested that ethnically defined social networks and the informal transfer of knowledge impacted academic performance, isolating minority groups from useful academic information. BAME students may also be at a further disadvantage, being unable to attend social and academic functions for cultural or family reasons. Black students also mentioned changing their behaviour to combat negative stereotypes in a variety of contexts. | The gender, ethnicity, and age of the interviewer may have impacted how both students and staff responded in the interviews, with some perhaps uncomfortable discussing some topics in greater depth than others. It is possible that participants were not representative of all attainment levels. | Conscious or unconscious discrimination may negatively impact the abilities of BAME students, both in examinations and in coursework choice. Social networks are important for the transfer of academic knowledge and the impact ethnicity may have on their formation, with issues around segregation and information sharing outside defined groups. |
| Study ID and Location | Aims, Objectives | Study Type | Recruitment, Sampling, Data Collection, and Analysis | Participant Description | Results | Limitations | Conclusions |
| Yeates et al. (2017) West Midlands Medical School | Influence of students’ ethnicity (White vs. British Asian) on (1) the scores and feedback from OSCE examiners and (2) examiners’ cognitive processing of those performances, including their recollection accuracy and activation of an Asian stereotype when examining Asian students | Two-group, double-blinded, randomised, Internet-based experimental design | Participants were current UK undergraduate Objective Structured Clinical Exam (OSCE) examiners. Recruitment was undertaken by email; medical schools around the UK disseminated the invitation to OSCE examiners. Data analysed using ANOVA. | Scripted video materials of OSCE of medical students with different ethnic backgrounds were analysed. Examiners performed different cognitive tests (cf. Objective measures) | 159 OSCE examiners from 20 UK medical schools, broad range of clinical specialties, predominantly of White ethnicity.... Examiners responded to Asian stereotypical words (716 ms, 95% confidence interval (CI) 702–731 ms) faster than neutral words (769 ms, 95% CI 753–786 ms, p < 0.001), suggesting Asian stereotypes were activated (or at least active) in examiners’ minds. This occurred regardless of whether examiners observed stereotype-consistent or stereotype-inconsistent performances. Student ethnicity had no influence on examiners’ scores, on the feedback examiners gave, or on examiners’ memories for one performance. | Study was conducted in a simulated context, rather than in a real OSCE. Cannot exclude the possibility that examiners’ judgements could be influenced by students’ ethnicity after a more prolonged series of performances due to (for example) fatigue or lapses in concentration, or that different samples of performance (displaying a different range of behaviours by Asian students) could produce an effect. | Examiners had a stereotype that was active at the time of judging performances, which does not appear to have been applied to their judgements. Examiner bias is not responsible for differential attainment by BME students. |
| Study ID and Location | Aims, Objectives | Study Type | Recruitment, Sampling, Data Collection, and Analysis | Participant Description | Results | Limitations | Conclusions |
| Roberts et al. (2010) Two medical schools in northern England | To explore the impact on students of two contrasting pedagogic approaches (a school offering early patient contact in the first 2 years was compared with one using paper-based patient scenarios only) to undergraduate learning about cultural diversity | An exploratory, qualitative research method was used, adopting an ‘inductive’ approach to data analysis and theory generation | Pragmatic recruitment. Focus groups were conducted at each site over a 3-month period, in small teaching rooms familiar to the students. Discussion was audio-recorded after seeking informed written consent from all participants. | Students (years 1 and 2) from seven selected groups (n = 49) were recruited pragmatically at sites A and B. Ethnic minority students = 20 (40.8%) | Barriers to learning about race, culture and ethnicity identified: (a) ‘institutional marginalisation’ of the subject, and (b) ‘student resistance’ to formal learning about cultural diversity. | The study was conducted using only year two medical students. Data collection was limited to two medical schools situated in northern England. Research team composition was British, White, and female. | The study found two potentially competing views. First, students claimed that although cultural diversity was important, their medical schools marginalised and failed to adequately support effective teaching. Second, in contrast, they claimed that the medical school was an ‘inappropriate’ setting for successful teaching about cultural diversity. Students did not consider the subject matter to be of central relevance to biomedicine. |
| Study ID and Location | Aims, Objectives | Study Type | Recruitment, Sampling, Data Collection, and Analysis | Participant Description | Results | Limitations | Conclusions |
| Morrison et al. (2019) | Examining the potential reasons for under performance by BME graduate-entry medical students, exploring their experiences of undergraduate medical training and their perceptions of barriers and facilitators to performance | Qualitative methods (focus groups with semi-structured interviews) | Graduate-entry MBChB students from all four cohorts were recruited using volunteer and snowball sampling. For each group, participants were randomly assigned a number to ease anonymisation during transcription. Participants were subsequently asked to self-report their ethnicity using the 2011 UK census categories. | 24 graduate-entry MBChB students self-identified as being from Black and Minority Ethnic (BME) backgrounds | Lack of BME representation and lack of understanding of cultural differences among staff impacted their experiencee. Students also reported a lack of trust in the institution’s ability to support BME students, with many not seeking support. Students’ narratives indicated that they had to mask their identity to fit in among their peers and to avoid negative stereotyping. Although rare, students faced overt racism from their peers and from patients. Many students reported feelings of isolation, reduced self-confidence, and low self-esteem. | BME students were not a homogeneous group: as individuals, they had unique identities as well as different ethnic, cultural, socioeconomic, and educational backgrounds. This study was not able to examine how these intersect to shape individual students’ experiences of medical education. | BME students reported experiencing relationship issues with other students and academic and clinical staff, lack of trust in the institution, and some racist events. |
Table A2.
Excluded studies and reason for exclusion.
Table A2.
Excluded studies and reason for exclusion.
| Excluded Studies | Reason for Exclusion |
|---|---|
| Al-Haddad et al. (2022) | Meta-ethnography (systematic review) |
| Joseph et al. (2021) | Narrative review |
| Khan and Mian (2020) | Opinion letter |
| Lim et al. (2021) | View of students on institutional discrimination—not a primary study |
| Woolf et al. (2018) | Postgraduate medical education |
| Gostelow et al. (2018) | Symposium workshop of students on institutional discrimination—not a primary study |
| Nightingale et al. (2022) | No medical students included in this study |
| Alwazzan (2018) | Review |
| Clements et al. (2020) | Postgraduate students |
| Denney et al. (2013) | Postgraduate students |
| Woolf et al. (2018) | Postgraduate students |
| Fyfe et al. (2022) | Guidelines |
Appendix B. MEDLINE EBSCOhost Platform
| # | Query | Limiters/Expanders | Last Run Via | Results |
| S22 | S14 AND S21 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S21 | S17 OR S20 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S20 | S18 OR S19 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S19 | “junior doctor” OR (MH “Physician Assistants+”) OR (MH “Medical Staff, Hospital”) | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S18 | junior doctor | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S17 | S15 OR S16 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S16 | postgraduate medical education | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S15 | (MH “Education, Medical+”) OR (MH “Education, Medical, Undergraduate”) OR (MH “Education, Medical, Graduate+”) OR (MH “Education, Medical, Continuing”) OR (MH “Education, Premedical”) OR “medical education” | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S14 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S13 | inequity | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S12 | inequality | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S11 | (MH “Discrimination, Psychological+”) OR (MH “Discrimination Learning”) OR (MH “Social Discrimination+”) OR (MH “Racism+”) OR (MH “Sexism”) OR (MH “Weight Prejudice”) OR (MH “Speech Discrimination Tests”) OR “discrimination” | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S10 | (MH “Bullying+”) OR “bullying” OR (MH “Cyberbullying”) | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S9 | S5 OR S6 OR S7 OR S8 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S8 | “stereotype” | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S7 | stereotype | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S6 | (MH “Stereotyping”) | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S5 | stereotyping | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S4 | “Intimidation” | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S3 | S1 OR S2 | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S2 | “harassment” | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
| S1 | (MH “Harassment, Non-Sexual+” | Expanders- Apply equivalent subjects Search modes- Boolean/Phrase | Interface- EBSCOhost Research Databases Search Screen- Basic Search Database- MEDLINE with Full Text | Display |
References
- Ackerman-Barger, Kupiri, Dowin Boatright, Rosana Gonzalez-Colaso, Regina Orozco, and Darin Latimore. 2020. Seeking Inclusion Excellence: Understanding Racial Microaggressions as Experienced by Underrepresented Medical and Nursing Students. Academic medicine: Journal of the Association of American Medical Colleges 95: 758–763. [Google Scholar] [CrossRef] [PubMed]
- Alexander, Claire, and Jason Arday. 2015. Aiming Higher: Race, Inequality and Diversity in the Academy. London: Runnymede Trust. [Google Scholar]
- Alexander, Claire, and William Shankley. 2020. Ethnic inequalities in the state education system in England. In Ethnicity and Race in the UK: State of the Nation, 1st ed. Edited by Claire Alexander, William Shankley, Bridget Byrne, Omar Khan and James Nazro. Bristol: Bristol University Press, pp. 93–126. [Google Scholar] [CrossRef]
- Al-Haddad, Moh, Susan Jamieson, and Evi Germeni. 2022. International medical graduates’ experiences before and after migration: A meta-ethnography of qualitative studies. Medical Education 56: 504–15. [Google Scholar] [CrossRef] [PubMed]
- Alwazzan, Lulu. 2018. Conceptualising discrimination in medical education: The hierarchy, the power. Medical Education 52: 356–58. [Google Scholar] [CrossRef] [PubMed]
- Arday, Jason, and Heidi S. Mirza, eds. 2018. Dismantling Race in Higher Education. Basingstoke: Palgrave Macmillan. [Google Scholar]
- Arksey, Hilary, and Lisa O’Malley. 2005. Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology 8: 19–32. [Google Scholar] [CrossRef]
- Bezrukova, Katerina, Chester S. Spell, Jamie L. Perry, and Karen A. Jehn. 2016. A meta-analytical integration of over 40 years of research on diversity training evaluation. Psychological Bulletin 142: 1227. [Google Scholar] [CrossRef]
- BMA (British Medical Assocation). 2022. Racism in Medicine. Available online: https://www.bma.org.uk/media/5746/bma-racism-in-medicine-survey-report-15-june-2022.pdf (accessed on 13 May 2022).
- Broad, Jonathan, Marion Matheson, Fabienne Verrall, Anna K. Taylor, Daniel Zahra, Louise Alldridge, and Gene Feder. 2018. Discrimination, harassment and non-reporting in UK medical education. Medical Education 52: 414–26. [Google Scholar] [CrossRef]
- Carter, Madeline, Neill Thompson, Paul Crampton, Gill Morrow, Bryan Burford, Christopher Gray, and Jan Illing. 2013. Workplace bullying in the UK NHS: A questionnaire and interview study on prevalence, impact and barriers to reporting. BMJ Open 3: e002628. [Google Scholar] [CrossRef]
- Claridge, Hugh, Stone Khadija, and Michael Ussher. 2018. The ethnicity attainment gap among medical and biomedical science students: A qualitative study. BMC Medical Education 18: 1–12. [Google Scholar] [CrossRef]
- Clements, Joshua M., Martin King, Rebecca Nicholas, Oliver Burdall, Elizabeth Elsey, Vittoria Bucknall, Ayoola Awopetu, Helen Mohan, Gemma Humm, Deirdre M. Nally, and et al. 2020. Bullying and undermining behaviours in surgery: A qualitative study of surgical trainee experiences in the United Kingdom (UK) and Republic of Ireland (ROI). International Journal of Surgery 84: 219–25. [Google Scholar] [CrossRef]
- Curtis, Ellen F., Janice L. Dreachslin, and Marie Sinioris. 2007. Diversity and cultural competence training in health care organizations: Hallmarks of success. The Health Care Manager 26: 255–62. [Google Scholar] [CrossRef]
- Daniel, Michelle, Morris Gordon, Madalena Patricio, Ahmad Hider, Cameron Pawlik, Rhea Bhagdev, Shoaib Ahmad, Sebastian Alston, Sophie Park, Teresa Pawlikowska, and et al. 2021. An update on developments in medical education in response to the COVID-19 pandemic: A BEME scoping review: BEME Guide No. 64. Medical Teacher 43: 253–71. [Google Scholar] [CrossRef]
- Denney, Mei L., Adrian Freeman, and Richard Wakeford. 2013. MRCGP CSA: Are the examiners biased, favouring their own by sex, ethnicity, and degree source? British Journal of General Practice 63: e718–e725. [Google Scholar] [CrossRef]
- EHRC (Equalities and Human Rights Commission). 2019. Tackling Racial Harassment: Universities Challenged. Available online: https://www.equalityhumanrights.com/en/publication-download/tackling-racial-harassment-universities-challenged (accessed on 10 June 2022).
- Equality Act. 2010. s. 9 (1). Available online: www.legislation.gov.uk/ukpga/2010/15/section/9 (accessed on 10 June 2022).
- Esmail, Aneez, and Sam Everington. 2021. Eradicating ethnic disadvantage in medical education and regulation. BMJ 374: n1725. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, Chloë, and Samia Hurst. 2017. Implicit bias in healthcare professionals: A systematic review. BMC Medical Ethics 18: 1–18. [Google Scholar] [CrossRef]
- Fnais, Naif, Charlene Soobiah, Maggie H. Chen, Erin Lillie, Laure Perrier, Mariam Tashkhandi, Sharon E. Straus, Muhammad Mamdani, Mohammed Al-Omran, and Andrea C. Tricco. 2014. Harassment and discrimination in medical training: A systematic review and meta-analysis. Academic Medicine 89: 817–27. [Google Scholar] [CrossRef] [PubMed]
- Fyfe, Molly, Jo Horsburgh, Julia Blitz, Neville Chiavaroli, Sonia Kumar, and Jennifer Cleland. 2022. The do’s, don’ts and don’t knows of redressing differential attainment related to race/ethnicity in medical schools. Perspectives on Medical Education 11: 1–14. [Google Scholar] [CrossRef] [PubMed]
- General Medical Council. 2014. National Training Surveys. Available online: https://www.gmc-uk.org/education/surveys.asp (accessed on 10 April 2023).
- GMC (General Medical Council). 2022. Equality. Diversity and Inclusion Policy 2022. Available online: https://www.gmc-uk.org/about/how-we-work/equality-diversity-and-inclusion (accessed on 16 April 2023).
- Gordon, Morris, and Trevor Gibbs. 2014. STORIES Statement: Publication Standards for Healthcare Education Evidence Synthesis. BMC Medicine 12: 143. [Google Scholar] [CrossRef]
- Gostelow, Naomi, Amali Lokugamage, and Faye Gishen. 2018. Celebrating diversity to promote and create inclusive curricula. Medical Education 52: 551–52. [Google Scholar] [CrossRef]
- Green, Kaye-Alese, Rebecca Wolinsky, Sabreea J. Parnell, Daniela Del Campo, Ajay S. Nathan, Priya S. Garg, Samantha E. Kaplan, and Shoumita Dasgupta. 2022. Deconstructing Racism, Hierarchy, and Power in Medical Education: Guiding Principles on Inclusive Curriculum Design. Academic Medicine 97: 804–11. [Google Scholar] [CrossRef]
- Halim, Usman A., and David M. Riding. 2018. Systematic review of the prevalence, impact and mitigating strategies for bullying, undermining behaviour and harassment in the surgical workplace. British Journal of Surgery 105: 1390–97. [Google Scholar]
- Hammick, Marilyn, Timothy Dornan, and Yvonne Steinert. 2010. Conducting a best evidence systematic review. Part 1: From idea to data coding. BEME Guide No. 13. Medical Teacher 32: 3–15. [Google Scholar] [CrossRef]
- Haq, Inam, Jenny Higham, Richard Morris, and Jane Dacre. 2005. Effect of ethnicity and gender on performance in undergraduate medical examinations. Medical Education 39: 1126–28. [Google Scholar] [CrossRef] [PubMed]
- Hill, Katherine A., Elizabeth A. Samuels, Cary P. Gross, Mayur M. Desai, Nicole Sitkin Zelin, Darin Latimore, Stephen J. Huot, Laura D. Cramer, Ambrose H. Wong, and Dowin Boatright. 2020. Assessment of the prevalence of medical student mistreatment by sex, race/ethnicity, and sexual orientation. JAMA Internal Medicine 180: 653–65. [Google Scholar] [CrossRef]
- Johnson, Sarah. 2016. NHS Staff Lay Bare a Bullying Culture; The Guardian. Available online: https://www.theguardian.com/society/2016/oct/26/nhs-staff-bullying-culture-guardian-survey (accessed on 10 April 2023).
- Joseph, Olivia Rochelle, Stuart W. Flint, Rianna Raymond-Williams, Rossby Awadzi, and Judith Johnson. 2021. Understanding Healthcare Students’ Experiences of Racial Bias: A Narrative Review of the Role of Implicit Bias and Potential Interventions in Educational Settings. International Journal of Environmental Research and Public Health 18: 12771. [Google Scholar] [CrossRef] [PubMed]
- Khan, Shujhat, and Areeb Mian. 2020. Racism and medical education. Lancet Infect Dis 20: 1009. [Google Scholar] [CrossRef]
- Kmietowicz, Zosia. 2020. Are medical schools turning a blind eye to racism? BMJ 368: m420. [Google Scholar] [CrossRef] [PubMed]
- Lim, Guan Hui Tricia, Zeluleko Sibanda, Joshua Erhabor, Soham Bandyopadhyay, and The Neurology and Neurosurgery Interest Group. 2021. Students’ perceptions on race in medical education and healthcare. Perspectives on Medical Education 10: 130–34. [Google Scholar] [CrossRef]
- Morrison, Nariell, Michelle Machado, and Clare Blackburn. 2019. Student perspectives on barriers to performance for black and minority ethnic graduate-entry medical students: A qualitative study in a West Midlands medical school. BMJ Open 9: e032493. [Google Scholar] [CrossRef]
- Nagpaul, Chaand. 2022a. Racism in Medicine must be Tacked for the NHS to Honour Its Founding Principles and Maximise Its Workforce Potential. NHS Race and Health Observatory Blog. Available online: https://www.nhsrho.org/blog/racism-in-medicine-must-be-tackled-if-the-nhs-is-to-maximise-its-workforce-potential-and-honour-its-founding-principles/ (accessed on 20 May 2022).
- Nagpaul, Chaand. 2022b. Racism is wrecking the lives of doctors, affecting patient care, and jeopardising services. BMJ 377: o1515. [Google Scholar] [CrossRef]
- Ng, Lillian, Charlie Lin, and Marcus A. Henning. 2019. A Narrative Review of Discrimination Experienced by Medical Students. Medical Science Educator 30: 577–84. [Google Scholar] [CrossRef]
- Nightingale, Julie, Jackie Parkin, Pete Nelson, Shirley Masterson-Ng, Jacqui Brewster, Temitope Labinjo, Deborah Amoakoh, David Lomas, Ifrah Salih, and Deborah Harrop. 2022. Multiple stakeholder perspectives of factors influencing differential outcomes for ethnic minority students on health and social care placements: A qualitative exploration. BMC Medical Education 22: 17. [Google Scholar] [CrossRef] [PubMed]
- Orom, Heather, Teresa Semalulu, and Willie Underwood, 3rd. 2013. The social and learning environments experienced by underrepresented minority medical students: A narrative review. Academic Medicine 88: 1765–77. [Google Scholar] [CrossRef] [PubMed]
- RCP (Royal College of Physicians). 2019. Survey of Medical Certificate of Completion of Training (CCT) Holders’ Career Progression. Available online: https://www.rcplondon.ac.uk/projects/outputs/2019-survey-medical-certificate-completion-training-cct-holders-career-progression (accessed on 20 May 2022).
- Roberts, Jane H., Tom Sanders, Karen Mann, and Val Wass. 2010. Institutional marginalisation and student resistance: Barriers to learning about culture, race and ethnicity. Advances in Health Sciences Education 15: 559–71. [Google Scholar] [CrossRef] [PubMed]
- Steele, Claude M., and Joshua Aronson. 1995. Stereotype threat and the intellectual test performance of African Americans. Journal of Personality and Social Psychology 69: 797. [Google Scholar] [CrossRef]
- Sue, Derald Wing, Christina M. Capodilupo, Gina C. Torino, Jennifer M. Bucceri, Aisha M. B. Holder, Kevin L. Nadal, and Marta Esquilin. 2007. Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist 62: 271. [Google Scholar] [CrossRef]
- Tricco, Andrea C., Erin Lillie, Wasifa Zarin, Kelly K. O’Brien, Heather Colquhoun, Danielle Levac, David Moher, Micah D. J. Peters, Tanya Horsley, Laura Weeks, and et al. 2018. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine 169: 467–73. [Google Scholar] [CrossRef] [PubMed]
- Universities UK. 2019. Black and Ethnic Minority Student Attainment at UK Universities: Closing the Gap. Available online: https://www.universitiesuk.ac.uk/sites/default/files/field/downloads/2021-07/bame-student-attainment.pdf (accessed on 20 May 2022).
- Van Ryn, Michelle, Diana J. Burgess, John F. Dovidio, Sean M. Phelan, Somnath Saha, Jennifer Malat, Joan M. Griffin, Steven S. Fu, and Sylvia Perry. 2011. The impact of racism on clinician cognition, behavior, and clinical decision making. Du Bois Review 8: 199–218. [Google Scholar] [CrossRef]
- Vaughan, Suzanne. 2013. Medical Students’ Experience and Achievement: The Effect of Ethnicity and Social Networks. Doctoral thesis, University of Manchester, Manchester, UK. [Google Scholar]
- Woolf, Katherine. 2009. The academic underperformance of medical students from ethnic minorities. Ph.D. thesis, UCL, (University College London), London, UK. [Google Scholar]
- Woolf, Katherine. 2020. Differential attainment in medical education and training. BMJ 368: m339. [Google Scholar] [CrossRef]
- Woolf, Katherine, Henry W. W. Potts, and Chris I. McManus. 2011. Ethnicity and academic performance in UK trained doctors and medical students: Systematic review and meta-analysis. BMJ 342: d901. [Google Scholar] [CrossRef]
- Woolf, Katherine, Judith Cave, Trisha Greenhalgh, and Jane Dacre. 2008. Ethnic stereotypes and the underachievement of UK medical students from ethnic minorities: Qualitative study. BMJ 337: a1220. [Google Scholar] [CrossRef]
- Woolf, Katherine, Rowena Viney, Antonia Rich, Hirosha Jayaweera, and Ann Griffin. 2018. Organisational perspectives on addressing differential attainment in postgraduate medical education: A qualitative study in the UK. BMJ Open 8: e021314. [Google Scholar] [CrossRef] [PubMed]
- Yeates, Peter, Katherine Woolf, Emyr Benbow, Ben Davies, Mairhead Boohan, and Kevin Eva. 2017. A randomised trial of the influence of racial stereotype bias on examiners’ scores, feedback and recollections in undergraduate clinical exams. BMC Medicine 15. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).