1. Introduction
Vehicles are becoming more advanced as they incorporate emerging technologies and the push for increasingly autonomous operation intensifies. Many of these technologies aim to reduce the chances of a crash or, when a crash occurs, reduce its severity [
1]. Although these improvements in vehicle safety have reduced crash rates [
1], crashes still occur. The National Highway Traffic Safety Association reported that the United States saw an overall 2% decrease in fatal crashes in 2017 from 2016. Despite the decrease, there were still 37,133 reported fatal crashes that year [
2]. When crashes do occur, particularly those of a higher severity, occupants rely on emergency medical services (EMS) for a rapid and efficient response that provides them with initial treatment and transportation to a medical facility. In this context, EMS primarily refers to emergency medical technicians (EMTs). However, depending on the location and available resources, fire, rescue, and law enforcement services may also be required to perform some EMS functions. In performing their tasks, however, EMS personnel encounter many challenges and difficulties beyond those inherent in identifying injuries and providing treatment to the victims. These challenges can adversely affect the quality and rapidity of the EMS response to a vehicular crash.
Research and technology advancement to identify and address the challenges and difficulties faced by EMS personnel responding to vehicular crashes has been limited. Emergency response to motor vehicle collisions (MVCs) is a complex chain of events that is dependent on the cooperation of multiple parties, a characteristic which in turn offers multiple opportunities for potential improvements. Three important areas where previous research has identified and suggested potential improvements in EMS performance are: (1) response time, (2) injury type and severity prediction, and (3) dispatching optimization.
Response time is one of the primary ways in which emergency response effectiveness is evaluated. Observations of response time not only provide an overall measure for the different system components [
3], but also represent an important factor in MVC investigation—longer EMS response times are associated with higher rates of MVC mortality [
4,
5]. Given that one of the primary delays present in the time between MVC occurrence and EMS response is in the notification of the MVC, many efforts to reduce EMS response times have focused on the development of automatic crash notification (ACN) and advanced ACN (AACN) systems [
6]. Generally, the presence of an ACN/AACN system is expected to promptly alert EMS of the crash, eliminate the time lost by indirectly alerting EMS (e.g., a 911 call being directed to a dispatching center operator, who then contacts relevant/available EMS and reiterates the contents of the call), and electronically convey accurate and pertinent information about the crash [
6]. Previous research has attempted to predict the impact that ACN/AACN systems will have on response times and MVC mortality, with general consensus that such systems will have measurable benefits [
7,
8,
9]. However, although these previous studies emphasize the importance of reducing response times to MVCs, the information that would be needed from ACN/AACN systems to improve care is generally not specified and the analyses exclusively focus on MVC mortality. Improved response times may not only reduce fatalities, but also decrease the severity or harmful effects of non-fatal injuries [
10].
A second area of technological advancement that can improve EMS response effectiveness involves the development of injury prediction metrics based on MVC kinematics. Weaver et al. [
11] produced predictive injury risk curves per affected body regions for specified frontal, single-impact crashes. Theoretically, their injury detection algorithm could be combined with electronic data recorder (EDR) outputs on a quasi-real time basis to provide EMS with an initial assessment of potential injuries during an MVC, as suggested by some AACN future development plans. Stigson et al. [
12] and Andricevic et al. [
13] similarly produced injury risk curves for frontal and oblique frontal impacts, respectively, but their models tended to be less specific than those in Weaver et al. [
11], as they were based on a maximum abbreviated injury scale (MAIS) score of 2+ that was not differentiated by body region. These prediction algorithms can also be influenced by occupant details such as age, height, and weight, (as also noted in [
10]) which may not be easy to obtain prior to EMS arrival at an MVC scene. Other similar predictive studies are less useful in the immediate EMS response, focusing more on the prolonged recovery from particular injuries suffered during an MVC (e.g., [
10,
14]).
A third area of EMS response effectiveness improvement concerns the formulation of better strategies for dispatching of EMS to MVCs. The estimated annual average of crashes involving ambulances is 4500 crashes per year in the United States, 34% of which result in injuries of personnel and/or patients [
15]. Ideally, improvements to EMS resource dispatching could result in shorter travel distances to MVCs, shorter response times, and reduced time pressures on EMS vehicle operators. A simulated study was conducted that evaluated multiple dispatching methodologies using real data from the city of San Francisco (California), where factors like response times and injury severity (non-life threatening vs. life threatening) were recorded in the Calls-For-Service database [
16]. Findings showed that, in some circumstances, simply assigning the closest immediate EMS resource to an MVC—particularly if the injuries were non-life threatening—was not the most appropriate response and could limit overall effectiveness of emergency services if multiple MVCs occurred. Additionally, other studies have investigated factors that specifically influence response times to identify how key elements (e.g., community density, roadway infrastructure, socio-demographic characteristics) affect EMS travel and response [
17,
18]. These studies concluded that response times greatly differ for urban communities compared to rural ones and are influenced by multiple factors. These findings should influence the development of better dispatching and resource management practices.
Achieving optimal resource allocation would require EMS dispatchers to understand accurately the extent of the injuries faced by occupants in MVCs, which is often not possible with current technology and limited ACN/AACN capabilities. In part to address this gap, the state of Alabama conducted a three-part study that examined the implementation of an electronic data system, the use of handheld data collection devices, and the development of tools that can predict MVC occupant injury [
19]. The study showed success in the collection and implementation of the electronic data and concluded that the data can improve EMS response to MVCs. Further, Geetla et al. evaluated roadway infrastructure with embedded acoustic sensors and ACN/AACN features to detect MVCs and provide extremely accurate crash locations. If effective, such a system could reduce response times and allow for increased EMS resource optimization [
20]. Simulated results showed effective crash detection performance and very small crash location errors (~5 m).
In general, these studies showcase the need for more accurate near-real time information about MVCs, a greater amount of such information, and the potential benefits that would come with that information, but not necessarily which data elements would be most relevant and useful. Consequently, this study was designed to leverage EMTs interviews about their experiences in working with MVCs. The primary objective of these interviews was to identify potential types of information that could improve emergency medical response to MVCs. EMTs were also asked about additional challenges that they face in their responses to these events.
2. Materials and Methods
This study includes structured interviews from 15 EMTs serving in southwest Virginia who consented to participate. The study was conducted in accordance with the Declaration of Helsinki and the protocol was approved by the Virginia Tech Institutional Review Board on 21 October 2019 (IRB# 19-848). Each interview was guided by a set of ten questions (
Appendix A) and conducted by the first author. The first five questions were focused on identifying issues with dispatching, initial response to incidents, and traveling to and from the scene. Questions six and seven solicited feedback on what information the EMTs felt they needed or wanted in order to improve response or provide better care. Finally, questions eight through ten addressed recent trends that EMTs may have noticed and the extent to which they receive feedback from medical facilities to which they deliver patients. Participants were first verbally consented and provided with a copy of their consent form. Handwritten notes were taken for each interview, along with an audio recording when consented by the participant. The interviews took place either at the Virginia Tech Transportation Institute in Blacksburg, Virginia or in a private area at the respective EMS station of the interview participant. The interviews generally lasted about 25 min, with the longest lasting 35 min and the shortest 14 min.
After all interviews were completed, the responses to the first seven questions were grouped into thematic categories. This method of quantifying responses was modeled after Terry et al. [
21], who quantified emergency service personnel feedback on how autonomous vehicles should interact with emergency vehicles. To identify the themes that would be used in this study, the notes and recordings of the interviews were first evaluated to extract commonalities. An initial list of themes was drafted based on this exercise. Given the variety in participant experience and his or her ability to articulate topic areas succinctly, each unique thought from each participant was counted only once. A unique thought was identified as an independent topic addressed by the interview participant; these were often preceded and followed by a period of silence as the interview participant thought about their answer, or were preceded by a phrase that signaled a new topic (e.g., “Another issue is…”). To assist with consistency in identification of a unique thought, transcribed notes were typed based on the handwritten notes, and audio recordings when applicable, and were formatted as bullet points, where each bullet point represented a unique thought. The list of themes was then revised into its final form to ensure the themes were overarching and not too vague or too specific. An “other” category was included to account for all additional unique thoughts shared.
Two interviews were interrupted by emergency calls and were not finished due to subsequent participant unavailability. Completed sections for these interviews were, however, included in the analysis. The EMTs interviewed served in six different locations throughout the southwest Virginia geographical area. Four participants primarily served in urban communities, five primarily served in suburban communities, and six primarily served in rural communities. Many of the participants also volunteered in other states and communities at the time of the interview or previously, contributing to breadth in the feedback received.
3. Results
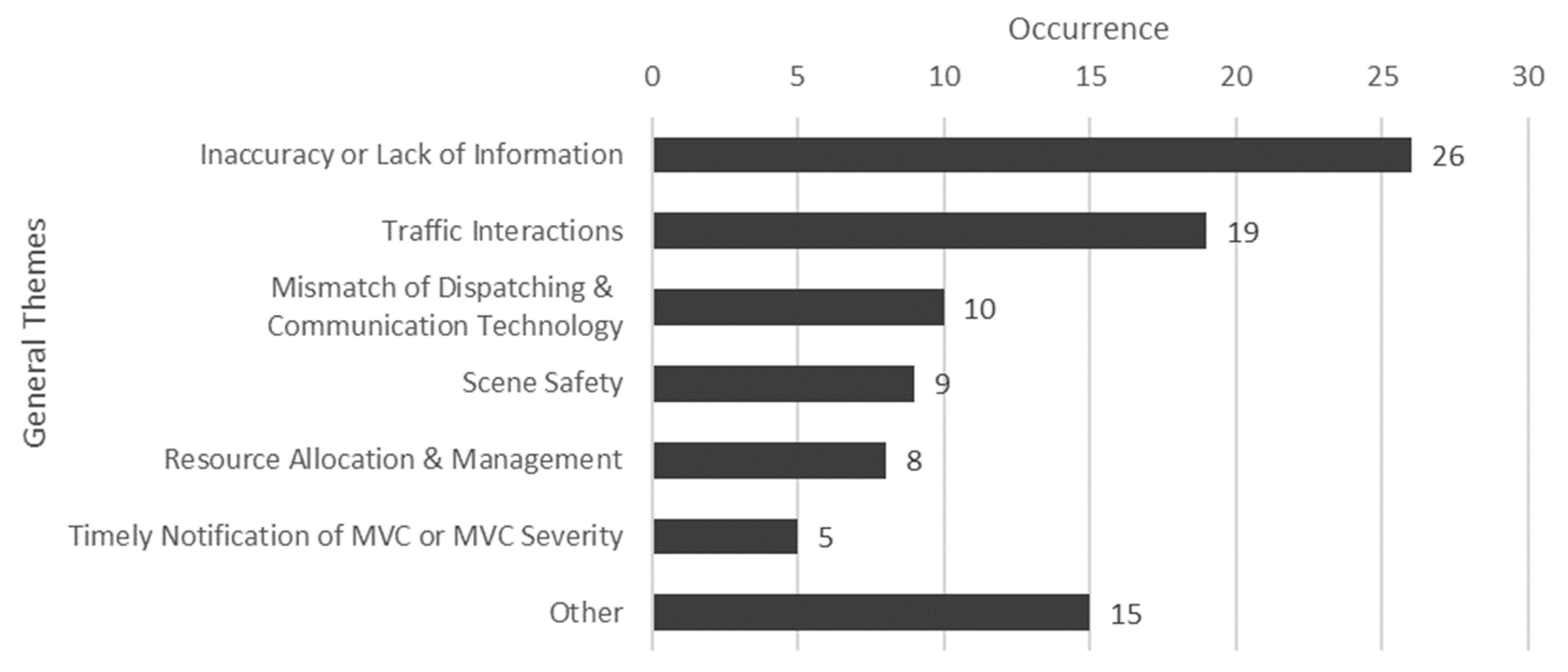
The first five interview questions aimed to uncover difficulties EMS personnel have faced during the initial response to an MVC and the transportation processes involved in responding to an incident, since these practices are not necessarily crash-type dependent. After collecting 14 responses from participants that fully answered this section of the interview, several thematic categories emerged (
Figure 1). The most common theme encompassed the difficulties that arise from the inaccuracy or lack of information that is available during the response to an MVC. The second most common theme pertained to difficulties that occur from interactions between EMS vehicles or personnel and other traffic. These difficulties included delay in response time, interactions with unpredictable driver behavior as drivers are approached by an emergency vehicle, and increases in secondary incidents that require EMS attention as a result of road congestion. The third most frequent theme was the mismatch of dispatching and communication technologies. This category encompassed difficulties that arose from too much unnecessary information transmitted over the radio, the poor quality of communication devices that limit the amount of information that can be shared, and the delay or absence in communication that results from different organizations using incompatible technology. Scene safety, resource allocation and management, and the timely notification of MVC occurrence and/or severity were also prevalent themes mentioned by interviewees. Examples of comments classified in the “Other” category included helicopter accessibility, hospital staff interactions, and the training of private (e.g., OnStar) dispatchers.
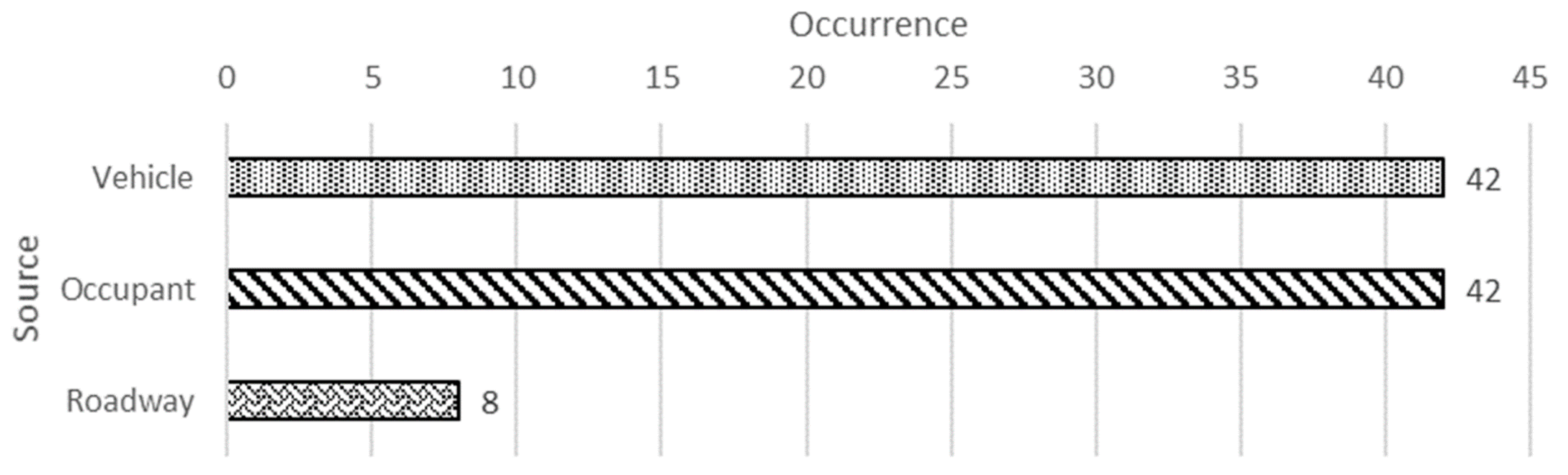
Interview questions six and seven were aimed at developing a list of information that EMS personnel believed would improve the efficiency and level of care when responding to an MVC. Responses from all 15 interview participants were included. Information about vehicles and information about occupants were mentioned most frequently, whereas information about the roadway, while also discussed, was not at the forefront of perceived informational needs (
Figure 2).
A more detailed examination of these three information sources reveals that six different types of vehicle-related data were mentioned (
Figure 3), with vehicle details and location being the most mentioned vehicle data element. This included the desire for more accurate vehicle-based transmission of the crash GPS location, the propulsion mechanism of the vehicle, and the location of airbags. The second most prevalent theme was vehicle deformation and extrication, which included the desire to know the level of deformation, particularly of the interior cabin, and whether vehicle extrication would be necessary. The remaining vehicle themes included vehicle kinematics, hazard detection, and rollover detection. The “Other” category for vehicle data included comments on reporting the number of vehicles involved, automating vehicle hazard light activation, and the easy on-scene availability of the aforementioned data element.
Information about the vehicle occupants was summarized into three themes (
Figure 3). The most common theme for this information source was occupant details and passive safety. This theme mainly encompassed information of how many occupants were in the vehicle at the time of the crash, how many of these occupants were belted, and which of these occupants interacted with airbags. The second theme under occupants concerned the victims’ vital signs that are most relevant during an MVC response, especially those that are used in injury severity calculations. Particularly, EMTs were interested in having access to information about the occupants’ heart rate, pulse, respiratory rate, and consciousness. The “Other” category included mentions of a desire to know general occupant injuries and having occupant pre-registration of health conditions (e.g., history of stroke, diabetes, allergies) linked to the vehicle.
Information about the roadway was summarized into three themes. The most common theme was roadway interaction where EMS personnel would like to have at their disposal a larger quantity and quality of programmable signs to alert and warn drivers of potential hazards. In addition, the potential for more accurate and precise roadway-based traffic updates for drivers was mentioned. In the roadway improvements theme, EMTs mentioned the development of roadway improvements that may help increase scene safety and reduce the possibility of inappropriate traffic interactions with emergency vehicles. The “Other” category included mentions of better incorporation of helicopter access and better labeled emergency vehicle compliant alternate routes.
The last three questions during the interviews were aimed at assessing whether the interviewees observed any injury correlations in particular types of vehicle crashes, gauge how EMS personnel receive feedback about patients they transport, and provide participants with the opportunity to comment on anything that they thought would assist the study. Thirteen of the interview participants answered the questions in this section. A vast majority of the interviewees (N = 10) indicated having observed correlations between crash types and injury characteristics. However, the relationships mentioned were generally well-known injury mechanisms (e.g., rib injuries experienced by belted occupants). All participants indicated receiving performance feedback from hospital staff, but only when they ask for such feedback. This questioning generally emerged from a particular interest in the outcome of a critical patient or as a self-evaluation tool on the quality of care that was provided. Three of the participants added that they, as leaders in their station, collect such feedback for use in personnel training sessions. Seven participants provided additional comments, but they primarily elaborated or emphasized on previous topics.
4. Discussion
In general, the interviews revealed some expected and some unexpected results. In the first phase of the interview, it was expected that inaccuracy or lack of information would be mentioned frequently, and this was indeed the most common difficulty expressed (
Figure 1). This theme encompassed the hurdles that come with having to plan for all scenarios due to gaps in knowledge about any given MVC. Whether the crash is notified by a bystander, an MVC occupant, or a vehicle service (e.g., ACN systems like OnStar) representative, there is large variability in the quantity and reliability of the information provided. One of the reasons for this observation may be lack of training. As an example, one of the participants mentioned that people are trained to call in emergencies at a young age (often kindergarten) but the process is never again addressed in an educational setting. Another anticipated issue was the timely notification of MVCs and/or estimations of their severities. Interviewees, who stressed the importance of this issue particularly in the context of instances when MVC occupants are unable to summon help by themselves, greatly emphasized this theme. These circumstances can arise because of lack of cellular service, because the vehicle is no longer visible to bystanders or other traffic, or because the occupants are incapacitated. In general, the sooner an incident can be reported, the more effectively the care can be provided [
4,
5]. A third anticipated issue was resource allocation and management. Closely linked to receiving timely notifications of MVCs, many participants highlighted that the sooner that accurate details can be understood about an MVC, the sooner appropriate resources can be directed to the crash scene. These resources can include extrication tools, the appropriate amount of medical care for the number of patients, or additional help to clear the scene and reduce traffic congestion. This theme was emphasized by participants who served rural communities, who generally experience longer travel distances—and time—to an MVC. The fourth anticipated issue was scene safety and was commonly expressed by participants who respond to interstate-highway crashes. EMS personnel often rely on the positioning of their vehicles alone to protect themselves and others from injury by other active traffic around the scene. Some participants mentioned that, due to this reason, in their jurisdiction EMTs cannot leave their vehicle to perform care until a second unit is present, despite how long that may take. Depending on the type of MVC, roadside environment, or available resources, strategic placement of EMS vehicles alone may not be an adequate safety measure for emergency responders.
One unexpected issue was the mismatch between dispatching and communication technology. With modern advances in radio and cellular technology, it was surprising to hear accounts of emergency response being hindered by incompatible or limited technologies. For example, one participant mentioned that their department sends a text description of the incident to the onboard computer in their ambulances, but the text provided is limited to 160 characters. This limitation in message size means that important information may be left out or must be provided in separate messages. A second unanticipated issue was the difficulties that arise from traffic interactions while in transit. Interview participants frequently expressed difficulties in interactions with other drivers, which affected their perception of safety and their response time to a crash scene. Both Byrne et al. [
4] and Ma et al. [
5] indicate that response time is the most critical component out of the entire emergency response chain of events. Drivers that respond incorrectly to approaching emergency vehicles, or simply do not know how to respond, greatly hinder the response process while also increasing the chance of causing another MVC. Difficulties interacting with other drivers are not limited to travel to the scene, but also arise when transporting victims to medical facilities for further treatment. Several participants expressed how difficult it is to pull away from a crash scene, even with lights and sirens activated.
The types of information required by EMS personnel generally followed the expectations, primarily focusing on vehicle and occupants (
Figure 2). Ideally, this information would be transmitted to EMS dispatching immediately after the vehicle crash occurred, as this would greatly impact the amount, type, and timeliness of resources sent in response. Interviewees also suggested that the desired information be collected from several independent sources to alleviate the possibility that one failure critically limits system performance. Further, since the vehicle(s) involved are most likely deformed by the crash, redundancy should be built into automated notification systems in case some system elements are compromised.
A more detailed observation into issues related to information about the vehicle suggested several important areas. There was an expectation that information about the vehicle kinematics and presence of a rollover would be mentioned, as it aligned with the necessary inputs for previous predictive injury studies [
11,
12,
13,
14]. Less expected, however, was the expressed interest in quantifying and conveying the degree of deformation experienced by the vehicle, particularly within the occupant compartment. Several EMTs discussed the possibility that such a measurement could be used to estimate the possibility of entrapment, which would assist with the resource allocation issues mentioned previously. Interviewees were also generally consistent in requesting that information including vehicle make, model, location, propulsion system, airbag location, and instructions on disabling any onboard hazards (e.g., high-voltage systems) be transmitted when a call is dispatched. With the increasing presence of electric and other alternative propulsion vehicles, in addition to manufacturer differences, EMTs struggle to identify quickly the vehicle’s critical components and how to interact with them safely in emergency scenarios. The difficulty associated with identifying and disarming active airbags was also frequently mentioned. Many participants mentioned being aware of cases where other EMTs had been injured or died as a result of accidental airbag activation while responding to an MVC. Interviewees were also interested in being alerted to the presence of water at the scene (e.g., if the vehicle was in a stream or pond) or fire. These circumstances have great influence on the type of resources required.
In terms of information about the occupants, although it was expected that participants would be interested in metrics to help evaluate the severity of the occupants’ injuries, most interviewees were interested in basic information about the occupants’ attributes and any interaction they may have had with the safety features in the vehicle. This included how many occupants were present at the time of the MVC, where they were sitting, if they were belted, and what airbags they may have interacted with. Several participants mentioned the need to explicitly know if a child occupied a child seat prior to the crash, as sometimes driver shock or incapacitation does not allow them to properly respond to EMT queries related to other vehicle occupants. Extensive searches may then result for potentially ejected children that may not have been present in the vehicle. Additional desired occupant-related information included vitals that could be used to gauge the level of trauma of the occupants. These elements included heart rate, presence of radial pulse, respiratory rate, blood pressure, and an assessment of consciousness. Finally, some interviewees mentioned that some MVCs occur due to sudden onset medical emergencies. Especially with older populations, the ability to associate medical history or conditions with the vehicle they drive may increase the effectiveness of their care.
Two limitations of this study should be considered when interpreting these results. First, although an effort was made to interview EMTs from rural, suburban, and urban communities, all participants resided in the southwest region of the state of Virginia, USA. While, given the experience level of our participants, many had served EMS organizations in other regions of the United States, their responses to this study may be biased to reflect their current operations area. Previous research has suggested that there are meaningful differences in EMS across rural and urban communities [
17,
18]. Future work should attempt to examine the congruence of these findings with the experience of EMS personnel in other areas of the United States and other countries. Second, the sample of participants that could be included in this study was relatively small. Larger samples of participants should be examined in future studies, which may leverage the information obtained in this study into the development of comprehensive surveys that can be answered and analyzed more efficiently than the interview results examined herein.
The findings of this investigation suggest several areas that could benefit from additional research work. First, evaluation of in-service EMS interactions with other traffic should be assessed, and typical conflicts between these vehicles categorized. Results of such analysis may lead to the development of procedures and/or technology candidates that improve traffic interactions between the general driver population and emergency vehicles. Second, approaches for leveraging existing vehicle technology into useful information transmitted through AACN systems should be explored [
6,
7,
8,
9]. Kinematic data and rollover identification, for example, could be obtained from sources such as EDRs. Information on how many occupants were present, which occupants were belted, and which occupants interacted with deployed airbags, could be retrieved from various integrated sensors in newer vehicles. For example, the weight sensor in seats that trigger the seatbelt warning, if it was extended to the rear seats, could be used to establish the number of occupants, the location of occupants, and which occupants were belted. Pairing of this information with the relay systems that trigger airbags could be used to determine which occupants may have interacted with deployed airbags. Once all this data are collected and processed, the challenge becomes establishing an effective way to communicate the resulting information with the appropriate services, ideally though an AACN system. Finally, new technologies could be leveraged to assist in obtaining some of the desired information. For example, a system that measures the amount of deformation in the occupant compartment and identifies whether any large foreign objects have breached the cabin would be useful in allowing EMTs to expect certain types of injuries and determine the need for extrication tools. On the occupant side, an interactive system could be created that deploys in response to a detected crash and can be used to evaluate the occupants’ vitals and convey them to responding services. The transmitted information can be further coupled with improved EMS trauma triage training to increase quality of care [
22].



{kind=link}
{kind=link}
{kind=link}


