The Effect of All-Terrain Vehicle Crash Location on Emergency Medical Services Time Intervals


Abstract
1. Introduction
2. Materials and Methods
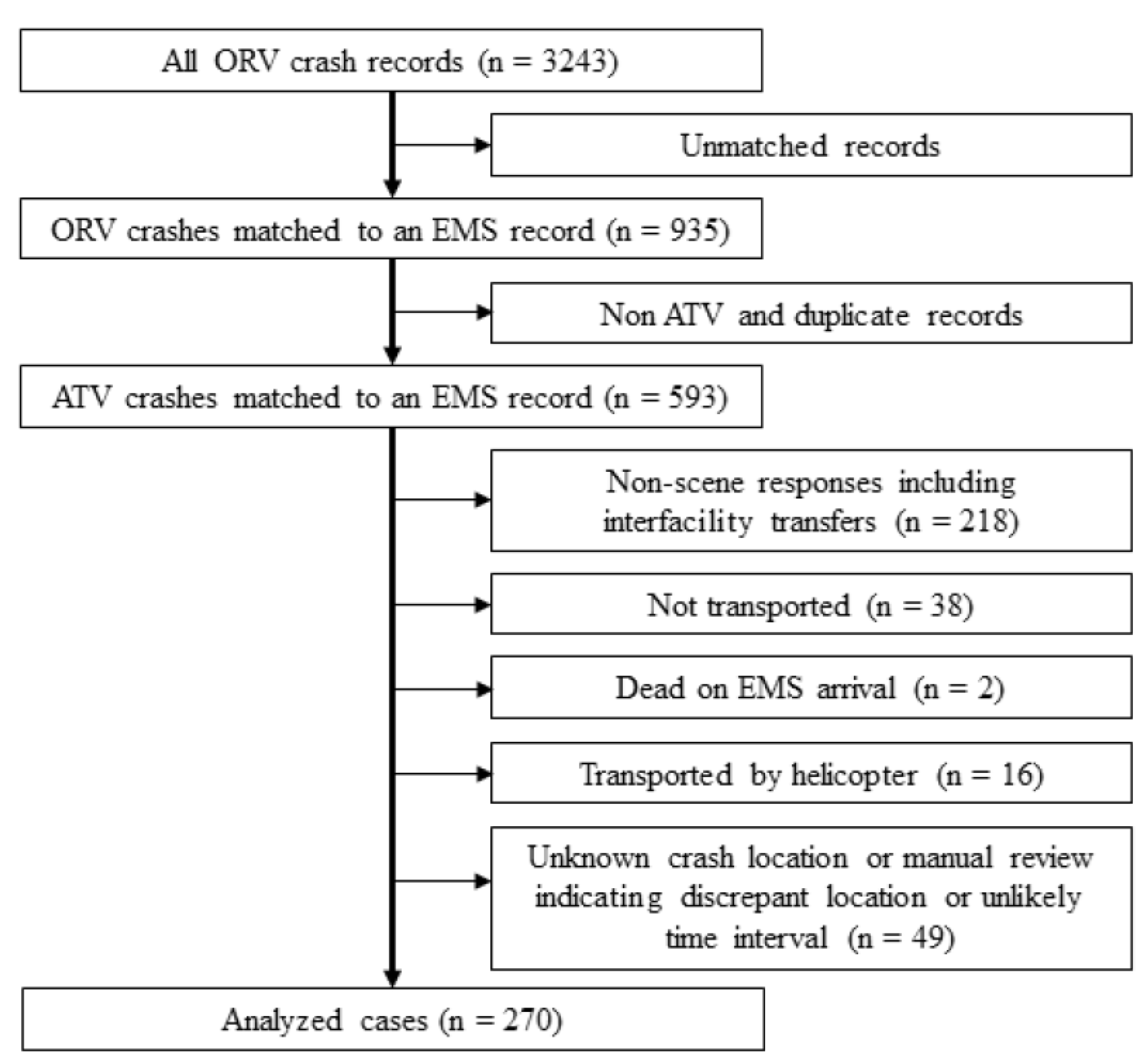
2.1. Identifying EMS Responses to ATV Crashes
2.2. Inclusion and Exclusion
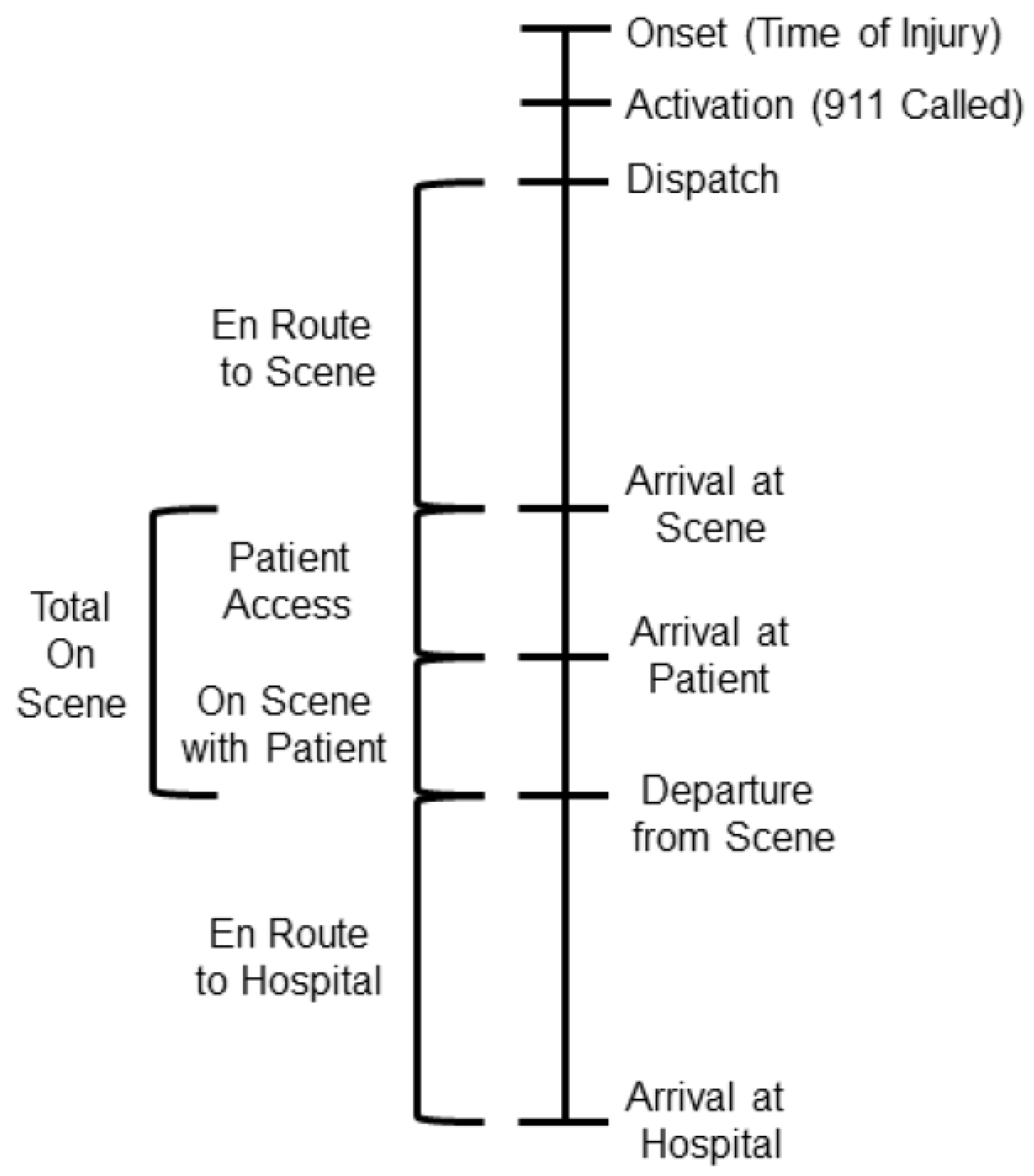
2.3. Study Variables
2.4. Data Analysis
3. Results
3.1. EMS Response Characteristics
3.2. Characteristics by Crash Location
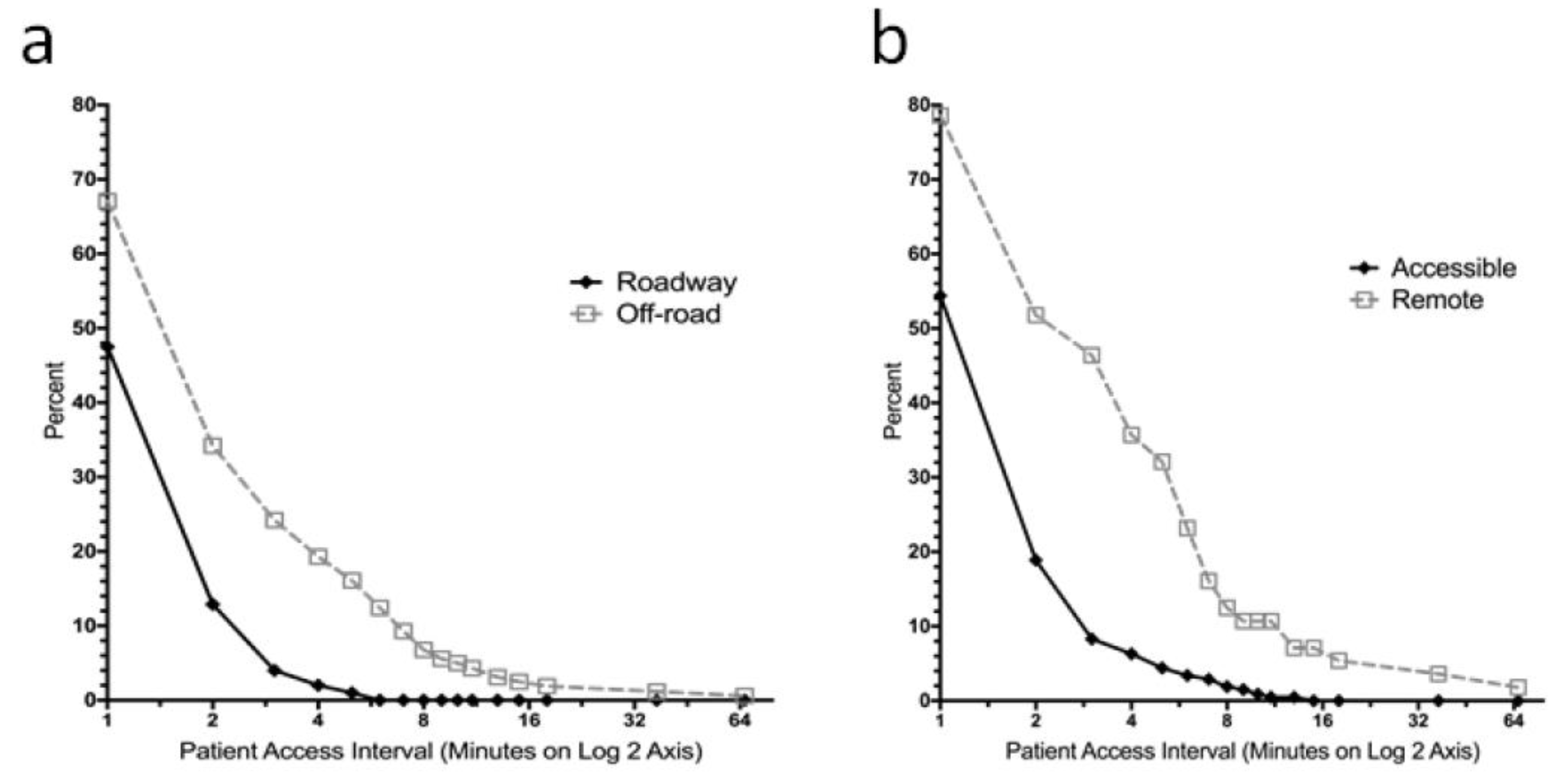
3.3. Time Interval Comparisons by Crash Location
3.4. Patient Outcomes by Crash Location
4. Discussion
4.1. Patient Access Interval
4.2. Comparisons by Crash Location
4.3. On Scene Interval
4.4. Practical Implications
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- U.S. Consumer Product Safety Commission. Annual Report of ATV-Related Deaths and Injuries. 2016. Available online: https://www.cpsc.gov/s3fs-public/atv_annual_Report_2016.pdf?vIcLfTM9VNDc23qe6FQyhJq7A7454xCr (accessed on 10 January 2019).
- Garay, M.; Hess, J.; Armstrong, D.; Hennrikus, W. Pediatric ATV injuries in a statewide sample: 2004 to 2014. Pediatrics 2017, 140, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Safety Officials Concerned with ATV Trail Where Chattooga County Woman Killed. Times Free Press. 2012. Available online: https://www.timesfreepress.com/news/news/story/2012/apr/03/whitfield-county-woman-dies-after-atv-fall/74525/ (accessed on 10 January 2019).
- Stanislaus County Department of Parks and Recreation. FAQ for Off-Highway Vehicle Parks. 2016. Available online: https://www.stancounty.com/parks/pdf/faq%20ohv%20parksstanco.pdf (accessed on 4 January 2019).
- Nevada Department of Conservation and Natural Resources. Application to the State of Nevada Off-Highway Vehicles Program. 2017. Available online: https://ohv.nv.gov/assets/etc/pdfs/Lyon_Co._Walker_River_SRA_Initiative_pdf (accessed on 10 January 2019).
- Baker, J.; Pat McKay, M. Analysis of emergency medical services activations in Shenandoah National Park from 2003 to 2007. Prehosp. Emerg. Care 2010, 14, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Nehme, Z.; Andrew, E.; Smith, K. Factors influencing the timeliness of emergency medical service response to time critical emergencies. Prehosp. Emerg. Care 2016, 20, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Bigdeli, M.; Khorasani-Zavareh, D.; Mohammadi, R. Pre-Hospital care time intervals among victims of road traffic injuries in Iran: A Cross-Sectional study. BMC Public Health 2010, 10. Available online: http://www.biomedcentral.com/1471-2458/10/406 (accessed on 10 January 2019). [CrossRef]
- Yeap, E.E.; Morrison, J.J.; Apodaca, A.N.; Egan, G.; Jansen, J.O. Trauma care in Scotland: Effect of rurality on ambulance travel times and level of destination healthcare facility. Eur. J. Trauma Emerg. Surg. 2014, 40, 295–302. [Google Scholar] [CrossRef]
- Grossman, D.C.; Kim, A.; Macdonald, S.C.; Klein, P.; Copass, M.K.; Maier, R.V. Urban-rural differences in prehospital care of major trauma. J. Trauma 1997, 42, 723–729. [Google Scholar] [CrossRef]
- Pell, J.P.; Sirel, J.M.; Marsden, A.K.; Ford, I.; Cobbe, S.M. Effect of reducing ambulance response times on deaths from out of hospital cardiac arrest: Cohort study. BMJ 2001, 322, 1385–1388. [Google Scholar] [CrossRef]
- Rajan, S.; Wissenberg, M.; Folke, F.; Hansen, S.M.; Gerds, T.A.; Kragholm, K.; Hansen, C.M.; Karlsson, L.I.M.; Lippert, F.K.; Køber, L.; et al. Association of bystander cardiopulmonary resuscitation and survival according to ambulance response times after out-of-hospital cardiac arrest. Circulation 2016, 134, 2095–2104. [Google Scholar] [CrossRef]
- O’Keeffe, C.; Nicholl, J.; Turner, J.; Goodacre, S. Role of ambulance response times in the survival of patients with out-of-hospital cardiac arrest. Emerg. Med. J. 2011, 28, 703–706. [Google Scholar] [CrossRef]
- Jena, A.B.; Mann, N.C.; Wedlund, L.N.; Olenski, A. Delays in emergency care and mortality during major U.S. marathons. N. Engl. J. Med. 2017, 376, 1441–1450. [Google Scholar] [CrossRef]
- Campbell, J.P.; Gratton, M.C.; Salomone, J.A.; Watson, A.W. Ambulance arrival to patient contact: The hidden component of prehospital response time intervals. Ann. Emerg. Med. 1993, 22, 1254–1257. [Google Scholar] [CrossRef]
- Morrison, L.J.; Angelini, M.P.; Vermeulen, M.J.; Schwartz, B. Measuring the EMS patient access time interval and the impact of responding to high-rise buildings. Prehosp. Emerg. Care 2005, 9, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, D.; Kitamura, T.; Kiyohara, K.; Nishiyama, C.; Hayashida, S.; Fujii, T.; Izawa, J.; Shimamoto, T.; Matsuyama, T.; Hatakeyama, T.; et al. High-rise buildings and neurologically favorable outcome after out-of-hospital cardiac arrest. Int. J. Cardiol. 2016, 224, 178–182. [Google Scholar] [CrossRef] [PubMed]
- McCoy, C.E.; Menchine, M.; Sampson, S.; Anderson, C.; Kahn, C. Emergency medical services out-of-hospital scene and transport times and their association with mortality in trauma patients presenting to an urban level I trauma center. Ann. Emerg. Med. 2013, 61, 167–174. [Google Scholar] [CrossRef]
- Brown, J.B.; Rosengart, M.R.; Forsythe, R.M.; Reynolds, B.R.; Gestring, M.L.; Hallinan, W.M.; Peitzman, A.B.; Billiar, T.R.; Sperry, J.L. Not all prehospital time is equal: Influence of scene time on mortality. J. Trauma Acute Care Surg. 2016, 81, 93–100. [Google Scholar] [CrossRef]
- Mathiesen, W.T.; Bjørshol, C.A.; Kvaløy, J.T.; Søreide, E. Effects of modifiable prehospital factors on survival after out-of-hospital cardiac arrest in rural versus urban areas. Crit. Care 2018, 22, 99. [Google Scholar] [CrossRef]
- Denning, G.; Jennissen, C.; Harland, K.; Ellis, D.; Buresh, C. All-terrain vehicles (ATVs) on the road: A serious traffic safety and public health concern. Traffic Inj. Prev. 2013, 14, 78–85. [Google Scholar] [CrossRef]
- Denning, G.; Jennissen, C.; Harland, K.; Ellis, D.G.; Buresh, C.T. Off-highway vehicle parks: Combining environment, knowledge, and enforcement for all-terrain vehicle injury prevention. Accid. Anal. Prev. 2013, 52, 64–70. [Google Scholar] [CrossRef]
- Qin, E.S.; Jennissen, C.A.; Wadman, C.A.; Denning, G.M. Using Geospatial Mapping to Determine the Impact of All-Terrain Vehicle Crashes on Both Rural and Urban Communities. West. J. Emerg. Med. 2017, 18, 913–922. [Google Scholar] [CrossRef]
- MedMedia First Aid for Data Collection. EM Stat Database Dictionary: Version 3.1. 2004. [Google Scholar]
- National Highway Traffic Safety Administration (NHTSA) EMS Division. NHTSA Uniform Pre-Hospital Emergency Medical Services (EMS) Dataset: Version 2.2; National Highway Traffic Safety Administration (NHTSA): Washington, DC, USA, 2005.
- Registry Plus(TM) Link Plus. 2.0 ed: Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/cancer/npcr/tools/registryplus/lp.htm (accessed on 10 January 2019).
- Baker, S.P.; O’Neill, B.; Haddon, W.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Copes, W.S.; Champion, H.R.; Sacco, W.J.; Lawnick, M.M.; Keast, S.L.; Bain, L.W. The Injury Severity Score revisited. J. Trauma 1988, 28, 69–77. [Google Scholar] [CrossRef] [PubMed]
- WWAMI RUCA Rural Health Research Center. RUCA Data: ZIP Code RUCA Approximation. 2004. Available online: http://depts.washington.edu/uwruca/ruca-approx.php (accessed on 10 January 2019).
- Harland, K.K.; Greenan, M.; Ramirez, M. Not just a rural occurrence: Differences in agricultural equipment crash characteristics by rural-urban crash site and proximity to town. Accid. Anal. Prev. 2014, 70, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.P.; Gratton, M.C.; Salomone, J.A.; Lindholm, D.J.; Watson, W.A. System implications of the ambulance arrival-to-patient contact interval on response interval compliance. Prehosp. Disaster Med. 1994, 9, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Denning, G.M.; Harland, K.K.; Ellis, D.G.; Jennissen, C.A. More fatal all-terrain vehicle crashes occur on the roadway than off: Increased risk-taking characterises roadway fatalities. Inj. Prev. 2013, 19, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Denning, G.M.; Jennissen, C.A. All-terrain vehicle fatalities on paved roads, unpaved roads, and off-road: Evidence for informed roadway safety warnings and legislation. Traffic Inj. Prev. 2016, 17, 406–412. [Google Scholar] [CrossRef]
- Denning, G.M.; Harland, K.K.; Jennissen, C.A. Age-based risk factors for pediatric ATV-related fatalities. Pediatrics 2014, 134, 1094–1102. [Google Scholar] [CrossRef]
- The Gisborne Herald. Beacon Brings Rescuers to Injured Farmer: Quad Bike Accident on Farm near Wairoa. 2017. Available online: http://gisborneherald.co.nz/localnews/3144234-135/beacon-brings-rescuers-to-injured-farmer (accessed on 10 January 2019).
- Almanack, A.; Lynch, M. Personal Locator Beacon Key to Mount Marcy Rescue. 2016. Available online: https://www.adirondackalmanack.com/2016/02/locator-beacon-key-to-marcy-rescue.html (accessed on 10 January 2019).
- Maritime New Zealand. Distress Beacon and Helmet Save Injured Farmer and Dogs from Bull Attack. 2018. Available online: https://www.maritimenz.govt.nz/public/news/media-releases-2018/20180202b.asp (accessed on 10 January 2019).
- PLB Usage Grows in U.S. More Rescues Credited to the Use of the Satellite Detectable Locator Beacons; BusinessWire: Fort Lauderdale, FL, USA, 2008; Available online: https://www.businesswire.com/news/home/20080410005115/en/PLB-Usage-Grows-U.S. (accessed on 10 January 2019).
- Knight, T. ATV Rider Crashes and Man Falls off Cliff over Holiday Weekend in FULTON. Watershed Post. 2016. Available online: http://www.watershedpost.com/2016/atv-rider-crashes-and-man-falls-cliff-over-holiday-weekend-fulton (accessed on 10 January 2019).
- Lehman, D. BLOG: Busy Season on the Trails. The Post Star. 2018. Available online: https://poststar.com/blogs/don_lehman/blog-new-winter-tourism-site-for-when-snow-arrives/article_6e4e8ca2-0e9d-11e9-91d0-07622a8da2c6.html (accessed on 10 January 2019).
- Brown, L.H.; Owens, C.F., Jr.; March, J.A.; Archino, E.A. Does ambulance crew size affect on-scene time or number of prehospital interventions? Prehosp. Disaster Med. 1996, 11, 214–217. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sex | n (Col %) 1 | Roadway | n (Col %) 1 |
|---|---|---|---|
| Male | 189 (77%) | Off | 166 (61%) |
| Female | 57 (23%) | On | 104 (39%) |
| Age (years old) | Location | ||
| <16 | 58 (22%) | Remote | 58 (21%) |
| 16–35 | 121 (45%) | Accessible | 212 (79%) |
| 36 and older | 91 (34%) | Spinal Immobilization | |
| GCS | Yes | 171 (63%) | |
| <15 | 76 (32%) | No | 99 (37%) |
| 15 | 159 (68%) | IV Placement | |
| ISS | Yes | 155 (57%) | |
| >15 | 62 (27%) | No | 115 (43%) |
| ≤15 | 164 (73%) | Cardiac Monitoring | |
| Eventual Fatality | Yes | 127 (47%) | |
| Yes | 13 (5%) | No | 143 (53%) |
| No | 233 (95%) | CPR | |
| Crew Training | Yes | 5 (2%) | |
| BLS | 49 (20%) | No | 265 (98%) |
| ALS | 195 (80%) | Intubation | |
| Rurality | Yes | 10 (4%) | |
| Isolated Rural | 48 (19%) | No | 260 (96%) |
| Small Rural | 40 (16%) | Number of Treatments | |
| Large Rural | 65 (26%) | 0–1 | 78 (29%) |
| Urban | 101 (40%) | 2–8 | 192 (71%) |
| Characteristics | Crash Location n (Col %) 1 | p-Value 2 | Crash Location n (Col %) 1 | p-Value 2 | ||
|---|---|---|---|---|---|---|
| Off-Road | Roadway | Remote | Accessible | |||
| Sex | ||||||
| Male | 124 (81%) | 65 (71%) | 0.076 | 46 (82%) | 143 (75%) | 0.28 |
| Female | 30 (19%) | 27 (29%) | 10 (18%) | 47 (25%) | ||
| Age (years) | ||||||
| <16 | 29 (17%) | 29 (28%) | 0.13 | 6 (10%) | 52 (25%) | 0.060 |
| 16–35 | 79 (48%) | 42 (40%) | 31 (53%) | 90 (42%) | ||
| >36 | 58 (35%) | 33 (32%) | 21 (36%) | 70 (33%) | ||
| GCS | ||||||
| <15 | 37 (25%) | 39 (44%) | 0.003 | 12 (24%) | 64 (35%) | 0.13 |
| 15 | 109 (75%) | 50 (56%) | 39 (76%) | 120 (65%) | ||
| ISS | ||||||
| >15 | 37 (24%) | 25 (34%) | 0.14 | 16 (30%) | 46 (27%) | 0.68 |
| ≤15 | 115 (76%) | 49 (66%) | 38 (70%) | 126 (63%) | ||
| Eventual Fatality | ||||||
| Yes | 1 (<1%) | 12 (12%) | 0.00027 | 1 (2%) | 12 (6%) | 0.47 3 |
| No | 146 (99%) | 87 (88%) | 47 (98%) | 186 (94%) | ||
| Crew Level | ||||||
| BLS | 26 (17%) | 23 (25%) | 0.12 | 8 (15%) | 41 (22%) | 0.27 |
| ALS | 127 (83%) | 68 (75%) | 46 (85%) | 149 (78%) | ||
| Rurality | ||||||
| Isolated Rural | 22 (14%) | 26 (27%) | 0.11 | 8 (15%) | 40 (20%) | 0.59 |
| Small Rural | 26 (17%) | 14 (14%) | 9 (17%) | 31 (15%) | ||
| Large Rural | 42 (27%) | 23 (23%) | 17 (32%) | 48 (24%) | ||
| Urban | 66 (42%) | 35 (36%) | 19 (36%) | 82 (41%) | ||
| Number of Interventions | ||||||
| 2–8 | 116 (70%) | 76 (73%) | 0.57 | 46 (79%) | 146 (69%) | 0.12 |
| 0–1 | 50 (30%) | 28 (27%) | 12 (21%) | 66 (31%) | ||
| Crash Location (n) 1 | Range | Mean (SD) | Median (IQR: Q1–Q3) | p-Value 2 |
|---|---|---|---|---|
| En Route to Scene | ||||
| Off-Road (166) | 0–43 | 9.9 (6.5) | 9.0 (6–13) | 0.40 |
| Roadway (104) | 0–25 | 10.2 (5.5) | 9.0 (6.5–14) | |
| Remote (58) | 0–40 | 10.2 (6.7) | 9.0 (6–14) | 0.85 |
| Accessible (212) | 0–43 | 9.9 (6.0) | 9.0 (6–13) | |
| Patient Access | ||||
| Off-Road (161) | 0–66 | 2.6 (6.5) | 1.0 (0–2) | <0.001 |
| Roadway (101) | 0–5 | 0.7 (0.9) | 0.0 (0–1) | |
| Remote (58) | 0–66 | 4.9 (10.2) | 2.0 (1–5) | <0.001 |
| Accessible (212) | 0–13 | 1.0 (1.8) | 1.0 (0–1) | |
| On Scene with Patient | ||||
| Off-Road (161) | 2–71 | 16.3 (9.4) | 14.0 (10–20) | 0.076 |
| Roadway (101) | 1–83 | 14.7 (10.6) | 13.0 (9–18) | |
| Remote (58) | 5–49 | 17.8 (8.4) | 16.5 (13–21.5) | 0.004 |
| Accessible (212) | 1–83 | 15.1 (10.2) | 13.0 (9–19) | |
| Total On Scene | ||||
| Off-Road (166) | 2–81 | 19.0 (11.8) | 16.0 (12–22) | 0.002 |
| Roadway (104) | 1–83 | 15.2 (10.6) | 13.0 (9–19) | |
| Remote (58) | 5–80 | 22.4 (12.6) | 19.5 (15–26) | <0.001 |
| Accessible (212) | 1–83 | 16.2 (10.8) | 14.0 (10–19) | |
| En Route to Hospital | ||||
| Off-Road (152) | 0–90 | 19.5 (12.8) | 16.0 (11–26) | 0.36 |
| Roadway (92) | 0–65 | 18.2 (12.2) | 16.5 (10–23) | |
| Remote (58) | 2–61 | 16.5 (10.8) | 15.0 (9–21) | 0.087 |
| Accessible (212) | 0–90 | 19.7 (13.0) | 17.0 (10–26) |
| Hospital Stay Characteristics | Crash Location n (Col %) 1 | p-Value 2 | Crash Location n (Col %) 1 | p-Value 2 | ||
|---|---|---|---|---|---|---|
| Off-road | Roadway | Remote | Accessible | |||
| ICU Days | ||||||
| 0 | 142 (89%) | 69 (86%) | 0.58 | 46 (85%) | 165 (89%) | 0.48 |
| ≥1 | 18 (11%) | 11 (14%) | 8 (15%) | 21 (11%) | ||
| Hospital Days | ||||||
| 0 | 79 (49%) | 42 (53%) | 0.65 | 21 (39%) | 100 (54%) | 0.054 |
| ≥1 | 81 (51%) | 38 (48%) | 33 (61%) | 86 (46%) | ||
| Hospital Days | ||||||
| 0–1 | 106 (66%) | 54 (68%) | 0.85 | 29 (54%) | 131 (70%) | 0.022 |
| ≥2 | 54 (34%) | 26 (32%) | 25 (46%) | 55 (30%) | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wubben, B.M.; Denning, G.M.; Jennissen, C.A. The Effect of All-Terrain Vehicle Crash Location on Emergency Medical Services Time Intervals. Safety 2019, 5, 73. https://doi.org/10.3390/safety5040073
Wubben BM, Denning GM, Jennissen CA. The Effect of All-Terrain Vehicle Crash Location on Emergency Medical Services Time Intervals. Safety. 2019; 5(4):73. https://doi.org/10.3390/safety5040073
Chicago/Turabian StyleWubben, Brandon M., Gerene M. Denning, and Charles A. Jennissen. 2019. "The Effect of All-Terrain Vehicle Crash Location on Emergency Medical Services Time Intervals" Safety 5, no. 4: 73. https://doi.org/10.3390/safety5040073
APA StyleWubben, B. M., Denning, G. M., & Jennissen, C. A. (2019). The Effect of All-Terrain Vehicle Crash Location on Emergency Medical Services Time Intervals. Safety, 5(4), 73. https://doi.org/10.3390/safety5040073