
The Effect of Sharrows, Painted Bicycle Lanes and Physically Protected Paths on the Severity of Bicycle Injuries Caused by Motor Vehicles


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Geographic Identification of Bicycle Lanes and Use
2.3. Modeling Injury Risk
- The intercept (β0) is the risk when both path/lane and intervention period are set to zero, i.e., the baseline rate in the non-bicycle route areas before the intervention
- The β1 coefficient is the effect when path or lane is set to 1 and the time period is set to zero
- β2 is the post-intervention effect when path or lane is held to zero, from which we can calculate the rate in the non-path/lane areas following the intervention time period, which is β0 + β2
- The interaction term β3 is the effect when both bicycle path or lane and intervention time period are set to 1. The coefficient for the interaction term for time period and intervention status is interpreted as a measure of the change in incidence density ratios from the pre-intervention period to the post-intervention period
2.4. Individual Data Analysis of Injury Severity
2.5. Geographic Clustering of Injury Severity
3. Results
3.1. Injury Risk Analysis
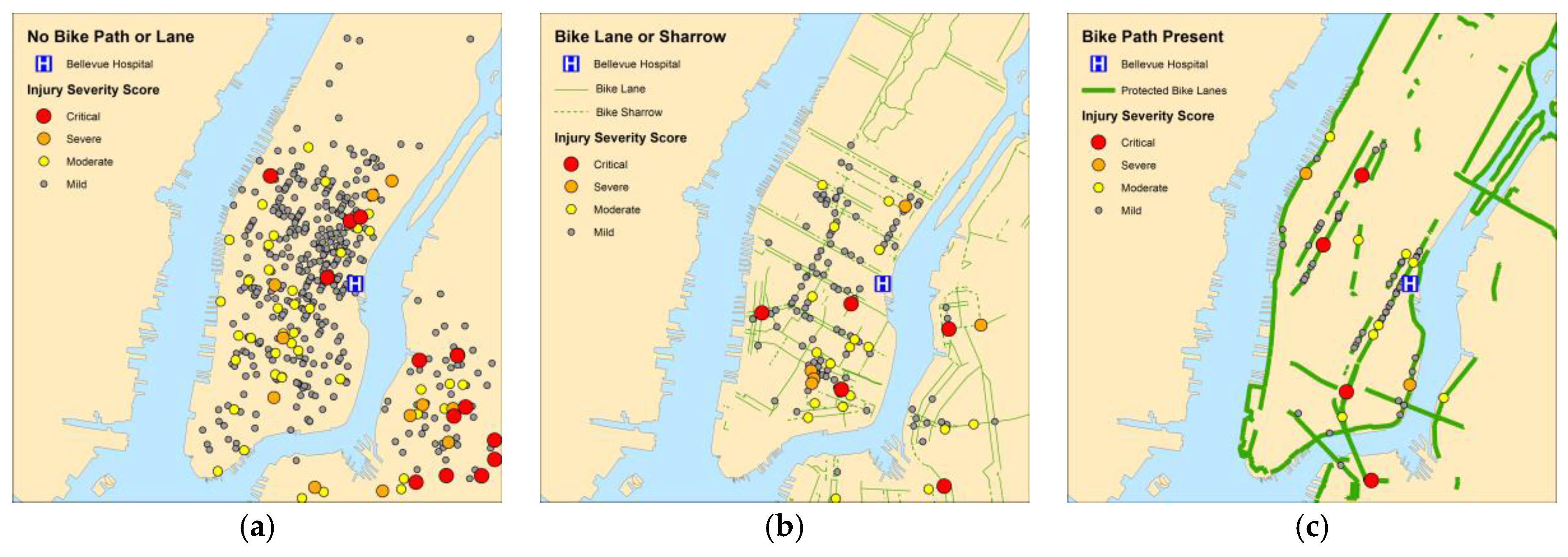
3.2. Geographic Analysis
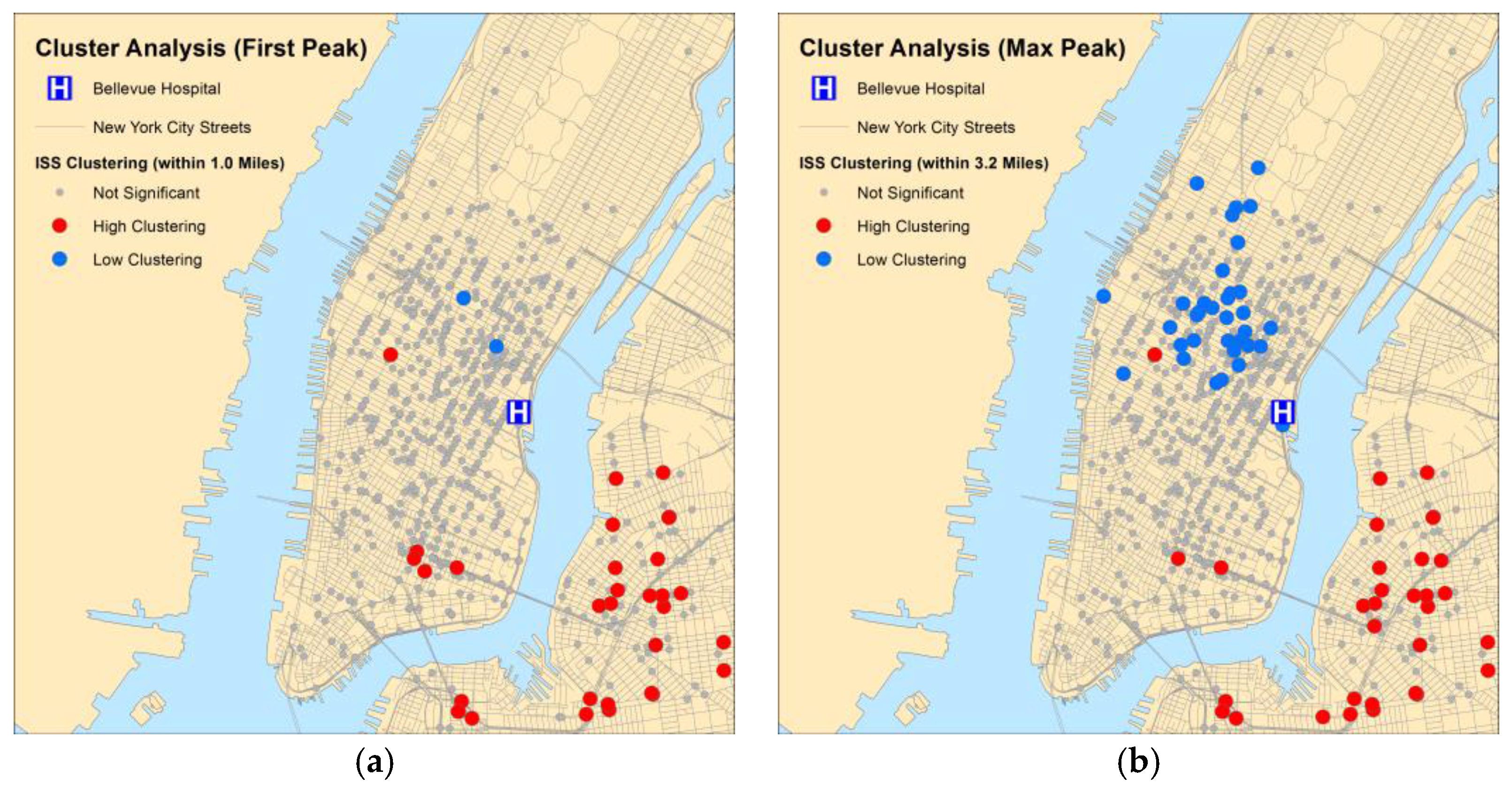
3.3. Geographic Clustering of Injury Severity Scores
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| US | United States |
| NYC | New York City |
| Bellevue | Bellevue Hospital |
| AOR | Adjusted Odds Ratio |
| CI | Confidence Interval |
| ED | Emergency Department |
| EMS | Emergency Medical Services |
| GCS | Glasgow Coma Scale |
| ISS | Injury Severity Score |
| NTDB | National Trauma Data Bank |
| GIS | Geographic Information System |
| DOT | Department of Transportation |
| IDR | Incidence Density Ratio |
Appendix A. Geospatial Analysis
References
- Boone-Heinonen, J.; Jacobs, D.R., Jr.; Sidney, S.; Sternfeld, B.; Lewis, C.E.; Gordon-Larsen, P. A walk (or cycle) to the park: Active transit to neighborhood amenities: The cardia study. Am. J. Prev. Med. 2009, 37, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Larsen, P.; Boone-Heinonen, J.; Sidney, S.; Sternfeld, B.; Jacobs, D.R., Jr.; Lewis, C.E. Active commuting and cardiovascular disease risk: The cardia study. Arch. Intern. Med. 2009, 169, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, G.; Macmillan, A.; Woodward, A. Moving urban trips from cars to bicycles: Impact on health and emissions. Aust. N. Z. J. Public Health 2011, 35, 54–60. [Google Scholar] [CrossRef] [PubMed]
- NHTSA. Bicyclists and Other Cyclists: 2014 Data. Available online: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812282 (accessed on 21 August 2016).
- CDC. Bicycle Safety. Available online: https://www.cdc.gov/motorvehiclesafety/bicycle/ (accessed on 21 August 2016).
- Bambach, M.R.; Mitchell, R.J.; Grzebieta, R.H.; Olivier, J. The effectiveness of helmets in bicycle collisions with motor vehicles: A case-control study. Accid. Anal. Prev. 2013, 53, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Shen, Q. Built environment effects on cyclist injury severity in automobile-involved bicycle crashes. Accid. Anal. Prev. 2016, 86, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Cripton, P.A.; Shen, H.; Brubacher, J.R.; Chipman, M.; Friedman, S.M.; Harris, M.A.; Winters, M.; Reynolds, C.C.; Cusimano, M.D.; Babul, S.; et al. Severity of urban cycling injuries and the relationship with personal, trip, route and crash characteristics: Analyses using four severity metrics. BMJ Open 2015, 5, e006654. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.; Giacomo Prato, C. A spatial analysis of land use and network effects on frequency and severity of cyclist-motorist crashes in the Copenhagen region. Traffic Inj. Prev. 2015, 16, 724–731. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.K.; Kim, S.; Ulfarsson, G.F.; Porrello, L.A. Bicyclist injury severities in bicycle-motor vehicle accidents. Accid. Anal. Prev. 2007, 39, 238–251. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.N.; Schneider, W.H.t.; Savolainen, P.T.; Farzaneh, M. Mixed logit analysis of bicyclist injury severity resulting from motor vehicle crashes at intersection and non-intersection locations. Accid. Anal. Prev. 2011, 43, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Teschke, K.; Frendo, T.; Shen, H.; Harris, M.A.; Reynolds, C.C.; Cripton, P.A.; Brubacher, J.; Cusimano, M.D.; Friedman, S.M.; Hunte, G.; et al. Bicycling crash circumstances vary by route type: A cross-sectional analysis. BMC Public Health 2014, 14, 1205. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lu, L.; Lu, J. Statistical analysis of bicyclists' injury severity at unsignalized intersections. Traffic Inj. Prev. 2015, 16, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Ma, M.; Huang, H.; Abdel-Aty, M.; Wu, C. Motor vehicle-bicycle crashes in Beijing: Irregular maneuvers, crash patterns, and injury severity. Accid. Anal. Prev. 2011, 43, 1751–1758. [Google Scholar] [CrossRef] [PubMed]
- Mulvaney, C.A.; Smith, S.; Watson, M.C.; Parkin, J.; Coupland, C.; Miller, P.; Kendrick, D.; McClintock, H. Cycling infrastructure for reducing cycling injuries in cyclists. Cochrane Database Syst. Rev. 2015, 12, CD010415. [Google Scholar]
- Lusk, A.C.; Asgarzadeh, M.; Farvid, M.S. Database improvements for motor vehicle/bicycle crash analysis. Inj. Prev. 2015, 21, 221–230. [Google Scholar] [CrossRef] [PubMed]
- De Rome, L.; Boufous, S.; Georgeson, T.; Senserrick, T.; Richardson, D.; Ivers, R. Bicycle crashes in different riding environments in the Australian capital territory. Traffic Inj. Prev. 2014, 15, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Dultz, L.A.; Foltin, G.; Simon, R.; Wall, S.P.; Levine, D.A.; Bholat, O.; Slaughter-Larkem, D.; Jacko, S.; Marr, M.; Glass, N.E.; et al. Vulnerable roadway users struck by motor vehicles at the center of the safest, large US city. J. Trauma 2013, 74, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Dultz, L.A.; Frangos, S.; Foltin, G.; Marr, M.; Simon, R.; Bholat, O.; Levine, D.A.; Slaughter-Larkem, D.; Jacko, S.; Ayoung-Chee, P.; et al. Alcohol use by pedestrians who are struck by motor vehicles: How drinking influences behaviors, medical management, and outcomes. J. Trauma 2011, 71, 1252–1257. [Google Scholar] [CrossRef] [PubMed]
- Kroyer, H.R. The relation between speed environment, age and injury outcome for bicyclists struck by a motorized vehicle—A comparison with pedestrians. Accid. Anal. Prev. 2015, 76, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Rivara, F.P.; Thompson, D.C.; Thompson, R.S. Epidemiology of bicycle injuries and risk factors for serious injury. 1997. Inj. Prev. 2015, 21, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Sethi, M.; Heidenberg, J.; Wall, S.P.; Ayoung-Chee, P.; Slaughter, D.; Levine, D.A.; Jacko, S.; Wilson, C.; Marshall, G.; Pachter, H.L.; et al. Bicycle helmets are highly protective against traumatic brain injury within a dense urban setting. Injury 2015, 46, 2483–2490. [Google Scholar] [CrossRef] [PubMed]
- Sethi, M.; Heyer, J.H.; Wall, S.; DiMaggio, C.; Shinseki, M.; Slaughter, D.; Frangos, S.G. Alcohol use by urban bicyclists is associated with more severe injury, greater hospital resource use, and higher mortality. Alcohol 2016, 53, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, D.R.; Williams, N.; Wall, S.P.; Glass, N.E.; Simon, R.; Todd, S.R.; Bholat, O.S.; Jacko, S.; Roe, M.; Wilson, C.T.; et al. A community traffic safety analysis of pedestrian and bicyclist injuries based on the catchment area of a trauma center. J. Trauma 2014, 76, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Office of the Mayor City of New York. Vision Zero Action Plan 2014; Mayor, O., Ed.; Office of the Mayoyr, City of New York: New York, NY, USA, 2014.
- New York City Department of Transportation. 2013 Bicycle Crash Data Report; New York City Department of Transportation: New York, NY, USA, 2014.
- Aaron, K.; Ye, J.; Ma, L.; Keefe, J.; Veltman, N.; Stark, K. Mean Streets 2014. Available online: https://project.wnyc.org/traffic-deaths/ (accessed on 3 April 2016).
- New York City Department of Transportation. Protected Bicycle Lanes in NYC; New York City Department of Transportation: New York, NY, USA, 2014.
- New York City Department of Transportation. New York City Bike Routes. Available online: http://www.nyc.gov/html/dot/downloads/misc/nyc-bike-routes.zip (accessed on 3 April 2016).
- New York City Department of Transportation. Bi-Annual Pedestrian Counts. Available online: http://www.nyc.gov/html/dot/html/about/datafeeds.shtml-Pedestrians (acessed on 14 July 2016).
- Allison, P.D. Missing Data; Sage Publications: Thousand Oaks, CA, USA, 2002; p. 93. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; Wiley: Hoboken, NJ, USA, 2013; p. 500. [Google Scholar]
- DeGroote, J.P.; Sugumaran, R.; Ecker, M. Landscape, demographic and climatic associations with human west nile virus occurrence regionally in 2012 in the united states of america. Geospat Health 2014, 9, 153–168. [Google Scholar] [CrossRef] [PubMed]
- Zou, B.; Peng, F.; Wan, N.; Mamady, K.; Wilson, G.J. Spatial cluster detection of air pollution exposure inequities across the united states. PLoS ONE 2014, 9, e91917. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Chen, C.; Ewing, R.; McKnight, C.E.; Srinivasan, R.; Roe, M. Safety countermeasures and crash reduction in New York City—Experience and lessons learned. Accid. Anal. Prev. 2013, 50, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Chen, C.; Srinivasan, R.; McKnight, C.E.; Ewing, R.; Roe, M. Evaluating the safety effects of bicycle lanes in New York City. Am. J. Public Health 2012, 102, 1120–1127. [Google Scholar] [CrossRef] [PubMed]
- Lusk, A.C.; Furth, P.G.; Morency, P.; Miranda-Moreno, L.F.; Willett, W.C.; Dennerlein, J.T. Risk of injury for bicycling on cycle tracks versus in the street. Inj. Prev. 2011, 17, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Abdel-Aty, M.; Lee, J.; Lee, C. Developing crash modification functions to assess safety effects of adding bike lanes for urban arterials with different roadway and socio-economic characteristics. Accid. Anal. Prev. 2015, 74, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Vision_Zero_Initiative. Traffic Safety by Sweden. Available online: http://www.visionzeroinitiative.com/en/ (acessed on 26 March 2016).
- Bailey, T.C.; Gatrell, A.C. Interactive Spatial Data Analysis, 1st ed.; Pearson Education Limited: Harlow, Essex, UK, 1995. [Google Scholar]
- Incremental Spatial Autocorrelation. Available online: http://resources.arcgis.com/en/help/main/10.1/index.html#//005p0000004z000000 (accessed on 14 April 2015).
- Cluster and Outlier Analysis (Anselin Local Moran’s I). Available online: http://resources.arcgis.com/en/help/main/10.1/index.html#/Cluster_and_Outlier_Analysis_Anselin_Local_Moran_s_I/005p0000000z000000 (accessed on 14 April 2015).
- Spatial Autocorrelation (Global Moran’s I). Available online: http://resources.arcgis.com/en/help/main/10.1/index.html#/Spatial_Autocorrelation_Global_Moran_s_I/005p0000000n000000 (accessed on 14 April 2015).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ISS ≤8 (None or Mild) | ISS >8 (Moderate, Severe or Critical) | |||
|---|---|---|---|---|
| Variable | n (%) | 95% CI | n (%) | 95% CI |
| Bicycle Route | ||||
| None | 486 (72%) | 69%–76% | 78 (60%) | 51%–69% |
| Sharrow | 38 (5.6%) | 4.0%–7.7% | 13 (10%) | 5.4%–16% |
| Painted Bicycle Lane | 91 (14%) | 11%–16% | 22 (17%) | 11%–24% |
| Physically Protected Path | 58 (8.4%) | 6.6%–11% | 17 (13%) | 7.8%–20% |
| Gender | ||||
| Male | 589 (84%) | 81%–87% | 119 (84%) | 77%–90% |
| Female | 109 (16%) | 13%–19% | 22 (16%) | 10%–23% |
| Age | ||||
| <18 | 31 (4.5%) | 3.0%–6.3% | 4 (3.0%) | 0.78%–7.1% |
| 18–55 | 622 (89%) | 87%–91% | 114 (81%) | 73%–87% |
| >55 | 45 (6.5%) | 4.7%–8.5% | 23 (16%) | 11%–23% |
| Ethnicity | ||||
| Non-Latino White | 256 (37%) | 33%–41% | 73 (52%) | 43%–60% |
| Black | 92 (13%) | 11%–16% | 8 (5.7%) | 2.5%–11% |
| Latino | 247 (36%) | 32%–39% | 39 (28%) | 20%–36% |
| East Asian | 67 (9.6%) | 7.6%–12% | 16 (11%) | 6.6%–18% |
| South Asian | 15 (2.2%) | 1.2%–3.5% | 3 (2.1%) | 0.44%–6.1% |
| Other | 18 (2.2%) | 1.5%–4.1% | 2 (1.2%) | 0.17%–5.0% |
| Alcohol Use | ||||
| No | 663 (95%) | 93%–96% | 119 (84%) | 77%–90% |
| Yes | 35 (5.0%) | 3.5%–6.9% | 22 (16%) | 10%–23% |
| Bicycle Share | ||||
| No | 346 (95%) | 92%–97% | 83 (97%) | 90%–99% |
| Yes | 19 (5.0%) | 3.2%–8.0% | 3 (3.0%) | 0.73%–9.9% |
| Wore Helmet | ||||
| No | 454 (66%) | 62%–70% | 96 (70%) | 62%–76% |
| Yes | 234 (34%) | 30%–38% | 41 (30%) | 22%–38% |
| Delivery Worker | ||||
| No | 421 (62%) | 58%–65% | 114 (84%) | 77%–90% |
| Yes | 263 (38%) | 35%–42% | 21 (16%) | 10%–23% |
| Self Reported Speed | ||||
| <5 mph | 66 (21%) | 16%–25% | 18 (28%) | 17%–40% |
| 5–15 mph | 230 (72%) | 67%–77% | 39 (60%) | 47%–72% |
| >15 mph | 24 (7.0%) | 5.0%–11% | 8 (12%) | 5.5%–23% |
| Hit by Turning Vehicle | ||||
| No | 230 (40%) | 36%–45% | 51 (55%) | 44%–65% |
| Yes | 339 (60%) | 55%–64% | 42 (45%) | 35%–56% |
| Distracted Riding (cell phones, audio equipment, etc.) | ||||
| No | 616 (90% ) | 88%–92% | 116 (91%) | 84%–95% |
| Yes | 68 (10%) | 8.0%–12% | 12 (9%) | 5.0%–16% |
| Salmoning (riding against traffic) | ||||
| No | 590 (92%) | 90%–94% | 102 (89%) | 81%–94% |
| Yes | 51 (8.0%) | 6.0%–10% | 13 (11%) | 6.0%–18% |
| Motor Vehicle Type | ||||
| Passenger Car | 258 (42%) | 38%–46% | 54 (49%) | 39%–58% |
| Taxi | 261 (42%) | 38%–46% | 26 (23%) | 16%–32% |
| SUV, Van, or Truck | 98 (16%) | 13%–19% | 31 (28%) | 20%–37% |
| Road Condition | ||||
| Normal | 610 (89%) | 86%–91% | 122 (90%) | 84%–95% |
| Wet or Iced | 75 (11%) | 8.7%–14% | 13 (10%) | 5.2%–16% |
| At Stop Sign | ||||
| No | 652 (98 ) | 96%–99% | 117 (94%) | 89%–98% |
| Yes | 15 (2.0%) | 1.3%–3.7% | 7 (6.0%) | 2.3%–11% |
| At Traffic Signal | ||||
| No | 320 (50%) | 46%–54% | 44 (38%) | 29%–47% |
| Yes | 322 (50%) | 46%–54% | 73 (62%) | 53%–71% |
| Daylight Condition | ||||
| Daylight | 221 (68%) | 62%–73% | 26 (50%) | 36%–64% |
| Night | 106 (32%) | 28%–38% | 26 (50%) | 36%–64% |
| A.M. Rush Hour | ||||
| No | 639 (93%) | 91%–95% | 127 (91%) | 85%–95% |
| Yes | 50 (7.0%) | 5.0%–10% | 12 (8.0%) | 5.0%–15% |
| P.M. Rush Hour | ||||
| No | 592 (86%) | 83%–89% | 122 (88%) | 81%–93% |
| Yes | 96 (14%) | 11%–17% | 17 (12%) | 7.3%–19% |
| Road Classification | ||||
| Local Street | 326 (75%) | 70%–79% | 58 (67%) | 56%–76% |
| Avenue or Two Way Arterial | 110 (25%) | 21%–30% | 29 (33%) | 24%–44% |
| ISS ≤8 (None or Mild) | ISS >8 (Moderate, Severe or Critical) | |||
|---|---|---|---|---|
| Variable | n (%) | 95% CI | n (%) | 95% CI |
| Brought in by EMS | ||||
| No | 65 (9.0%) | 7.0%–12% | 2 (1.0% ) | 0.17%–5.0% |
| Yes | 633 (91%) | 88%–93% | 139 (99%) | 95%–100% |
| GCS <15 | ||||
| No | 654 (95%) | 93%–96% | 104 (76%) | 68%–83% |
| Yes | 37 (5.0%) | 3.8%–7.3% | 33 (24%) | 17%–32% |
| Admitted or Died | ||||
| No | 610 (87%) | 85%–90% | 23 (16% ) | 11%–23% |
| Yes | 88 (13%) | 10%–15% | 118 (84%) | 77%–89% |
| Unadjusted Model | Odds Ratio | p Value | 95% CI |
|---|---|---|---|
| Sharrow | 2.02 | 0.040 | 1.03–3.94 |
| Painted Bicycle Lane | 1.50 | 0.130 | 0.89–2.53 |
| Physically Protected Path | 1.79 | 0.052 | 0.99–3.21 |
| Adjusted Model | |||
| Sharrow | 1.94 | 0.086 | 0.91–4.15 |
| Painted Bicycle Lane | 1.52 | 0.159 | 0.85–2.71 |
| Physically Protected Path | 1.66 | 0.136 | 0.85–3.22 |
| Female | 0.68 | 0.172 | 0.39–1.18 |
| Age 18–55 | 0.48 | 0.010 | 0.26–0.84 |
| Alcohol Use | 1.94 | 0.235 | 0.65–5.81 |
| Bicycle Share | 0.90 | 0.893 | 0.21–3.92 |
| Wore Helmet 2 | 0.93 | 0.731 | 0.60–1.44 |
| Delivery Worker | 0.35 | 0.000 | 0.21–0.61 |
| Bicycle Speed 5–15 mph | 0.77 | 0.415 | 0.41–1.45 |
| Bicycle Speed >15 mph | 1.37 | 0.633 | 0.37–5.12 |
| Hit by Turning Vehicle | 0.78 | 0.471 | 0.39–1.54 |
| Distracted Riding | 0.82 | 0.603 | 0.38–1.74 |
| Salmoning | 1.25 | 0.528 | 0.62–2.54 |
| Hit by Taxi | 0.59 | 0.068 | 0.34–1.04 |
| Hit by SUV, Van, or Truck | 1.59 | 0.102 | 0.91–2.78 |
| Wet or Iced Road | 1.09 | 0.819 | 0.53–2.25 |
| Hit at Intersection 3 | 1.47 | 0.102 | 0.93–2.34 |
| Hit at Night | 1.44 | 0.481 | 0.52–4.00 |
| Hit During A.M. Rush | 1.14 | 0.747 | 0.51–2.57 |
| Hit During P.M. Rush | 0.97 | 0.932 | 0.49–1.91 |
| Hit on Avenue or Two Way Artery | 1.27 | 0.462 | 0.67–2.42 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wall, S.P.; Lee, D.C.; Frangos, S.G.; Sethi, M.; Heyer, J.H.; Ayoung-Chee, P.; DiMaggio, C.J. The Effect of Sharrows, Painted Bicycle Lanes and Physically Protected Paths on the Severity of Bicycle Injuries Caused by Motor Vehicles. Safety 2016, 2, 26. https://doi.org/10.3390/safety2040026
Wall SP, Lee DC, Frangos SG, Sethi M, Heyer JH, Ayoung-Chee P, DiMaggio CJ. The Effect of Sharrows, Painted Bicycle Lanes and Physically Protected Paths on the Severity of Bicycle Injuries Caused by Motor Vehicles. Safety. 2016; 2(4):26. https://doi.org/10.3390/safety2040026
Chicago/Turabian StyleWall, Stephen P., David C. Lee, Spiros G. Frangos, Monica Sethi, Jessica H. Heyer, Patricia Ayoung-Chee, and Charles J. DiMaggio. 2016. "The Effect of Sharrows, Painted Bicycle Lanes and Physically Protected Paths on the Severity of Bicycle Injuries Caused by Motor Vehicles" Safety 2, no. 4: 26. https://doi.org/10.3390/safety2040026
APA StyleWall, S. P., Lee, D. C., Frangos, S. G., Sethi, M., Heyer, J. H., Ayoung-Chee, P., & DiMaggio, C. J. (2016). The Effect of Sharrows, Painted Bicycle Lanes and Physically Protected Paths on the Severity of Bicycle Injuries Caused by Motor Vehicles. Safety, 2(4), 26. https://doi.org/10.3390/safety2040026