
Validation of Quantitative Ultrasound and Texture Derivative Analyses-Based Model for Upfront Prediction of Neoadjuvant Chemotherapy Response in Breast Cancer

 , , , ,
, , , ,  , , and
, , and 
Abstract
1. Introduction
2. Material and Methods
2.1. Developmental Cohort
2.2. Ultrasound Data Collection
2.3. Quantitative Ultrasound Parameters
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumour Characteristics
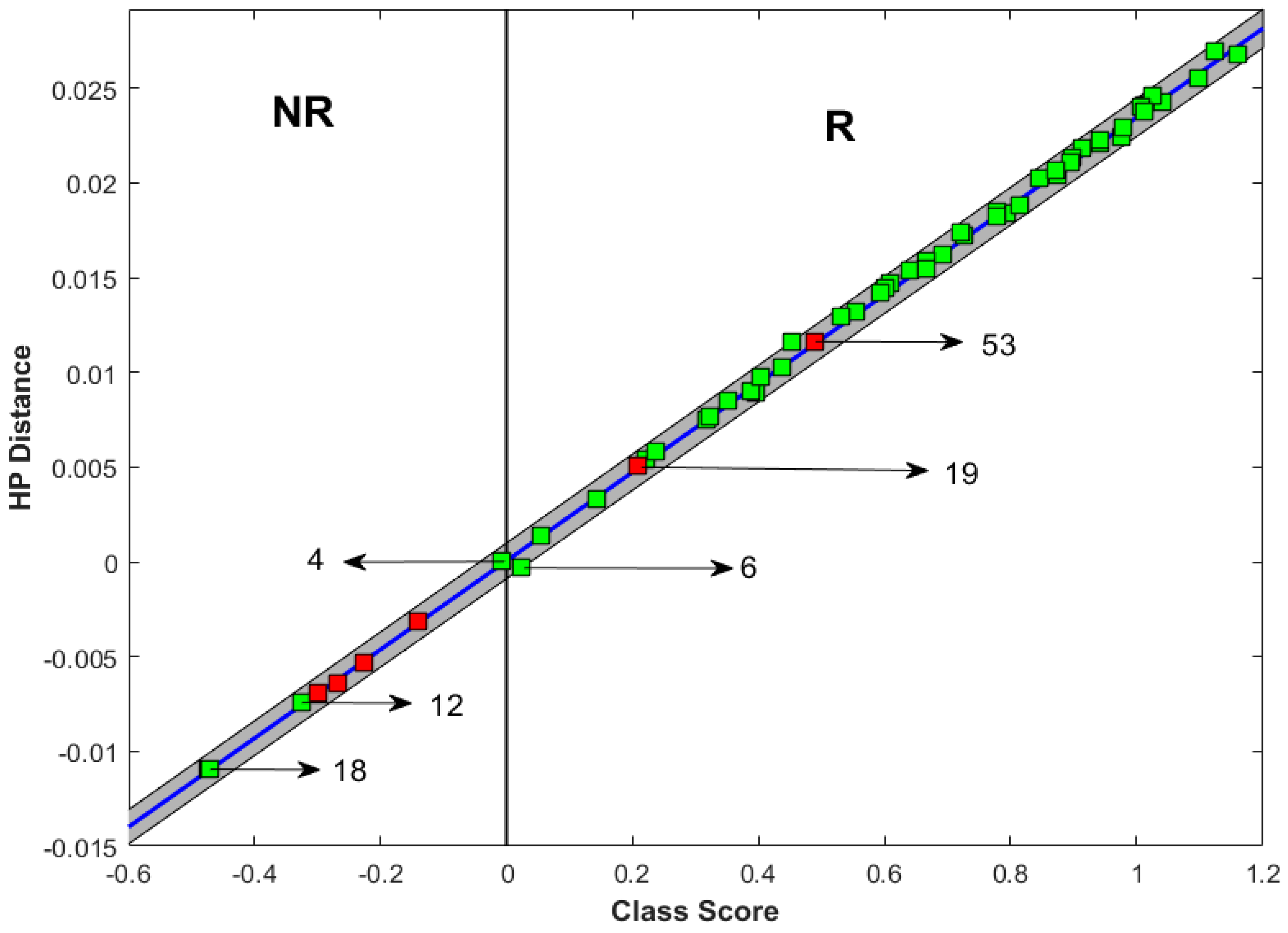
3.2. Prediction of Response
3.3. Incorrect Prediction
4. Discussion
5. Future Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Shelley Hwang, E.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 13. [Google Scholar] [CrossRef]
- Rapoport, B.L.; Demetriou, G.S.; Moodley, S.D.; Benn, C.A. When and How Do i Use Neoadjuvant Chemotherapy for Breast Cancer? Curr. Treat. Options Oncol. 2014, 15, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Caudle, A.S.; Gonzalez-Angulo, A.M.; Hunt, K.K.; Pusztai, L.; Kuerer, H.M.; Mittendorf, E.A.; Hortobagyi, G.N.; Meric-Bernstam, F. Impact of Progression during Neoadjuvant Chemotherapy on Surgical Management of Breast Cancer. Ann. Surg. Oncol. 2011, 18, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.; Mazouni, C.; Liedtke, C.; Kau, S.-W.; Frye, D.; Green, M.; Gonzalez-Angulo, A.M.; Symmans, W.F.; Hortobagyi, G.N.; Pusztai, L. HER2 Expression and Efficacy of Preoperative Paclitaxel/FAC Chemotherapy in Breast Cancer. Breast Cancer Res. Treat. 2008, 108, 183–190. [Google Scholar] [CrossRef]
- Fountzila, E.; Ignatiadis, M. Neoadjuvant Immunotherapy in Breast Cancer: A Paradigm Shift? Ecancermedicalscience 2020, 14, 1147. [Google Scholar] [CrossRef] [PubMed]
- Stavros, A.T.; Thickman, D.; Rapp, C.L.; Dennis, M.A.; Parker, S.H.; Sisney, G.A. Solid Breast Nodules: Use of Sonography to Distinguish between Benign and Malignant Lesions. Radiology 1995, 196, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Joo, S.; Yang, Y.S.; Moon, W.K.; Kim, H.C. Computer-Aided Diagnosis of Solid Breast Nodules: Use of an Artificial Neural Network Based on Multiple Sonographic Features. IEEE Trans. Med. Imaging 2004, 23, 834617. [Google Scholar] [CrossRef]
- Chen, C.M.; Chou, Y.H.; Han, K.C.; Hung, G.S.; Tiu, C.M.; Chiou, H.J.; Chiou, S.Y. Breast Lesions on Sonograms: Computer-Aided Diagnosis with Nearly Setting-Independent Features and Artificial Neural Networks. Radiology 2003, 226, 504–514. [Google Scholar] [CrossRef]
- Klimonda, Z.; Karwat, P.; Dobruch-Sobczak, K.; Piotrzkowska-Wróblewska, H.; Litniewski, J. Breast-Lesions Characterization Using Quantitative Ultrasound Features of Peritumoral Tissue. Sci. Rep. 2019, 9, 7963. [Google Scholar] [CrossRef]
- Piotrzkowska-Wroblewska, H.; Litniewski, J.; Szymanska, E.; Nowicki, A. Quantitative Sonography of Basal Cell Carcinoma. Ultrasound Med. Biol. 2015, 41, 748–759. [Google Scholar] [CrossRef]
- Piotrzkowska-Wróblewska, H.; Dobruch-Sobczak, K.; Litniewski, J. Quantitative Ultrasonography as a Tool for the Evaluation of Breast Tumor Response to Neoadjuvant Chemotherapy. J. Ultrason. 2022, 22, 86–92. [Google Scholar] [CrossRef]
- Dobruch-Sobczak, K.; Piotrzkowska-Wróblewska, H.; Klimonda, Z.; Karwat, P.; Roszkowska-Purska, K.; Clauser, P.; Baltzer, P.A.T.; Litniewski, J. Multiparametric Ultrasound Examination for Response Assessment in Breast Cancer Patients Undergoing Neoadjuvant Therapy. Sci. Rep. 2021, 11, 2501. [Google Scholar] [CrossRef] [PubMed]
- Klimonda, Z.; Karwat, P.; Dobruch-Sobczak, K.; Piotrzkowska-Wróblewska, H.; Litniewski, J. Assessment of Breast Cancer Response to Neoadjuvant Chemotherapy Based on Ultrasound Backscattering Envelope Statistics. Med. Phys. 2022, 49, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Dobruch-Sobczak, K.S.; Piotrzkowska-Wróblewska, H.; Karwat, P.; Klimonda, Z.; Markiewicz-Grodzicka, E.; Litniewski, J. Quantitative Assessment of the Echogenicity of a Breast Tumor Predicts the Response to Neoadjuvant Chemotherapy. Cancers 2021, 13, 3546. [Google Scholar] [CrossRef]
- Dobruch-Sobczak, K.; Piotrzkowska-Wróblewska, H.; Klimonda, Z.; Roszkowska-Purska, K.; Litniewski, J. Ultrasound Echogenicity Reveals the Response of Breast Cancer to Chemotherapy. Clin. Imaging 2019, 55, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Piotrzkowska-Wróblewska, H.; Dobruch-Sobczak, K.; Klimonda, Z.; Karwat, P.; Roszkowska-Purska, K.; Gumowska, M.; Litniewski, J. Monitoring Breast Cancer Response to Neoadjuvant Chemotherapy with Ultrasound Signal Statistics and Integrated Backscatter. PLoS ONE 2019, 14, e0213749. [Google Scholar] [CrossRef]
- Karwat, P.; Piotrzkowska-Wróblewska, H.; Klimonda, Z.; Dobruch-Sobczak, K.S.; Litniewski, J. Monitoring Breast Cancer Response to Neoadjuvant Chemotherapy Using Probability Maps Derived from Quantitative Ultrasound Parametric Images. IEEE Trans. Biomed. Eng. 2024, 71, 2620–2629. [Google Scholar] [CrossRef]
- Byra, M.; Dobruch-Sobczak, K.; Piotrzkowska-Wroblewska, H.; Klimonda, Z.; Litniewski, J. Explaining a Deep Learning Based Breast Ultrasound Image Classifier with Saliency Maps. J. Ultrason. 2022, 22, 70. [Google Scholar] [CrossRef]
- Byra, M.; Jarosik, P.; Dobruch-Sobczak, K.; Klimonda, Z.; Piotrzkowska-Wroblewska, H.; Litniewski, J.; Nowicki, A. Joint Segmentation and Classification of Breast Masses Based on Ultrasound Radio-Frequency Data and Convolutional Neural Networks. Ultrasonics 2022, 121, 106682. [Google Scholar] [CrossRef]
- Byra, M.; Dobruch-Sobczak, K.; Piotrzkowska-Wroblewska, H.; Klimonda, Z.; Litniewski, J. Prediction of Response to Neoadjuvant Chemotherapy in Breast Cancer with Recurrent Neural Networks and Raw Ultrasound Signals. Phys. Med. Biol. 2022, 67, 185007. [Google Scholar] [CrossRef]
- Byra, M.; Dobruch-Sobczak, K.; Klimonda, Z.; Piotrzkowska-Wroblewska, H.; Litniewski, J. Early Prediction of Response to Neoadjuvant Chemotherapy in Breast Cancer Sonography Using Siamese Convolutional Neural Networks. IEEE J. Biomed. Health Inform. 2021, 25, 797–805. [Google Scholar] [CrossRef]
- Sannachi, L.; Gangeh, M.; Tadayyon, H.; Gandhi, S.; Wright, F.C.; Slodkowska, E.; Curpen, B.; Sadeghi-Naini, A.; Tran, W.; Czarnota, G.J. Breast Cancer Treatment Response Monitoring Using Quantitative Ultrasound and Texture Analysis: Comparative Analysis of Analytical Models. Transl. Oncol. 2019, 12, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Lizzi, F.L.; Astor, M.; Liu, T.; Deng, C.; Coleman, D.J.; Silverman, R.H. Ultrasonic Spectrum Analysis for Tissue Assays and Therapy Evaluation. Int. J. Imaging Syst. Technol. 1997, 8, 3–10. [Google Scholar] [CrossRef]
- Insana, M.F.; Hall, T.J. Parametric Ultrasound Imaging from Backscatter Coefficient Measurements: Image Formation and Interpretation. Ultrason. Imaging 1990, 12, 245–267. [Google Scholar] [PubMed]
- Dasgupta, A.; Brade, S.; Sannachi, L.; Quiaoit, K.; Fatima, K.; DiCenzo, D.; Osapoetra, L.O.; Saifuddin, M.; Trudeau, M.; Gandhi, S.; et al. Quantitative Ultrasound Radiomics Using Texture Derivatives in Prediction of Treatment Response to Neo-Adjuvant Chemotherapy for Locally Advanced Breast Cancer. Oncotarget 2020, 11, 3782–3792. [Google Scholar] [CrossRef]
- Li, S.; Yu, K.-D.; Fan, L.; Hou, Y.-F.; Shao, Z.-M. Predicting Breast Cancer Recurrence Following Breast-Conserving Therapy: A Single-Institution Analysis Consisting of 764 Chinese Breast Cancer Cases. Ann. Surg. Oncol. 2011, 18, 2492–2499. [Google Scholar] [CrossRef]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients with Triple-Negative Breast Cancer. J. Clin. Oncol. 2008, 26, 1271–1281. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Untch, M.; Blohmer, J.U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and Impact of Pathologic Complete Response on Prognosis after Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef]
- Sannachi, L.; Osapoetra, L.O.; DiCenzo, D.; Halstead, S.; Wright, F.; Look-Hong, N.; Slodkowska, E.; Gandhi, S.; Curpen, B.; Kolios, M.C.; et al. A Priori Prediction of Breast Cancer Response to Neoadjuvant Chemotherapy Using Quantitative Ultrasound, Texture Derivative and Molecular Subtype. Sci. Rep. 2023, 13, 22687. [Google Scholar] [CrossRef]
- Collins, G.S.; Dhiman, P.; Ma, J.; Schlussel, M.M.; Archer, L.; Van Calster, B.; Harrell, F.E.; Martin, G.P.; Moons, K.G.M.; van Smeden, M.; et al. Evaluation of Clinical Prediction Models (Part 1): From Development to External Validation. BMJ 2024, 384, e074819. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to Build a Bridge from a Population-based to a More “Personalized” Approach to Cancer Staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.H.; Litière, S.; De Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and Clarification: From the RECIST Committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef]
- Tadayyon, H.; Sannachi, L.; Gangeh, M.J.; Kim, C.; Ghandi, S.; Trudeau, M.; Pritchard, K.; Tran, W.T.; Slodkowska, E.; Sadeghi-Naini, A.; et al. A Priori Prediction of Neoadjuvant Chemotherapy Response and Survival in Breast Cancer Patients Using Quantitative Ultrasound. Sci. Rep. 2017, 7, 45733. [Google Scholar] [CrossRef]
- Tsai, H.Y.; Tsai, T.Y.; Wu, C.H.; Chung, W.S.; Wang, J.C.; Hsu, J.S.; Hou, M.F.; Chou, M.C. Integration of Clinical and CT-Based Radiomic Features for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Systemic Therapy in Breast Cancer. Cancers 2022, 14, 6261. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Chang, J.; He, X.; Peng, M.; Zhang, Y.; Wu, T.; Xu, P.; Chu, W.; Gao, C.; Cao, S.; et al. PET/CT-Based Radiomics Analysis May Help to Predict Neoadjuvant Chemotherapy Outcomes in Breast Cancer. Front. Oncol. 2022, 12, 849626. [Google Scholar] [CrossRef]
- Graeser, M.; Harbeck, N.; Gluz, O.; Würstlein, R.; zu Eulenburg, C.; Schumacher, C.; Grischke, E.M.; Forstbauer, H.; Dimpfl, M.; Braun, M.; et al. The Use of Breast Ultrasound for Prediction of Pathologic Complete Response in Different Subtypes of Early Breast Cancer within the WSG-ADAPT Subtrials. Breast 2021, 59, 58–66. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Y.; Wang, Y.; Xie, Y.; Cui, Y.; Feng, S.; Yao, M.; Qiu, B.; Shen, W.; Chen, D.; et al. Early Prediction of Treatment Response to Neoadjuvant Chemotherapy Based on Longitudinal Ultrasound Images of HER2-Positive Breast Cancer Patients by Siamese Multi-Task Network: A Multicentre, Retrospective Cohort Study. eClinicalMedicine 2022, 52, 101562. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Huang, C.-S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Sannachi, L.; Gangeh, M.; Naini, A.S.; Bhargava, P.; Jain, A.; Tran, W.T.; Czarnota, G.J. Quantitative Ultrasound Monitoring of Breast Tumour Response to Neoadjuvant Chemotherapy: Comparison of Results Among Clinical Scanners. Ultrasound Med. Biol. 2020, 46, 1142–1157. [Google Scholar] [CrossRef]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Goetz, M.P.; Olson, J.A.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef]
- Johnston, S.R.D.; Toi, M.; O’Shaughnessy, J.; Rastogi, P.; Campone, M.; Neven, P.; Huang, C.S.; Huober, J.; Jaliffe, G.G.; Cicin, I.; et al. Abemaciclib plus Endocrine Therapy for Hormone Receptor-Positive, HER2-Negative, Node-Positive, High-Risk Early Breast Cancer (MonarchE): Results from a Preplanned Interim Analysis of a Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2023, 24, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.N.J.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Age | ER/PR/ HER-2 | Histology | Grade | Pre-NAC Tumour Size (cm) | Pre-NAC T Stage | Pre-NAC N Stage | Treatment |
|---|---|---|---|---|---|---|---|---|
| 1 | 47 | +-- | IDC | III | 3 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 2 | 37 | ++- | IDC | II-III | 4.4 | 3 | 0 | FEC100 x3, then Doce100x3 |
| 3 | 47 | ++- | IDC | III | 6.7 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 4 | 50 | +-- | IDC | III | 1.9 | 1 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 5 | 42 | +-- | IDC | III | 8.5 | 3 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 6 | 50 | ++- | IDC | I-II | 6.1 | 2 | 1 | FEC100 x3, then Doce100 + Tras x3 |
| 7 | 35 | +++ | IDC | II | 8 | 1 | 1 | AC x4, then Paclitaxel (DD) + Tras x4 |
| 8 | 67 | --+ | IDC | II | 4 | 3 | 1 | FEC100 x3, then Doce100 + Tras x3 |
| 9 | 60 | +-- | IDC | II | 2.4 | 3 | 3 | FEC100 x3, then Doce100x3 |
| 10 | 45 | --- | IDC | III | 2.7 | 3 | 1 | AC x4, then Paclitaxel (DD) + Tras x4 |
| 11 | 50 | +++ | IDC | II | 10.7 | 2 | 1 | AC x4, then Paclitaxel (DD) + Tras x4 |
| 12 | 51 | ++- | IDC | III | 4 | 2 | 1 | FEC100 x3, then Doce100x3 |
| 13 | 40 | +++ | IDC | II | 5.9 | 3 | 1 | FEC100 x3, then Doce100x3 |
| 14 | 72 | +++ | IDC | III | 3.5 | 1 | 1 | FEC100 x3, then Doce100 + Tras x3 |
| 15 | 63 | --- | IDC | III | 4 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 16 | 56 | +-- | IDC | III | 3.5 | 4 | 1 | Docetaxel-cyclophosphamide, 4 cycles |
| 17 | 49 | +++ | IDC | II | 4.9 | 2 | 0 | FEC100 x3, then Doce100 + Tras x3 |
| 18 | 50 | ++- | IDC | I | 3 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 19 * | 60 | --- | IDC | II | 7.3 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 20 | 41 | +-- | IDC | II–III | 7.5 | 3 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 21 * | 72 | --- | IMC | III | 4.7 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 22 | 53 | --- | IDC | III | 3.1 | 3 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 23 | 63 | ++- | IDC | II | 7.4 | 2 | 2 | FEC100 x3, then Doce100x3 |
| 24 | 64 | +++ | IDC | I-II | 3.4 | 2 | 0 | FEC100 x3, then Doce100 + Tras x3 |
| 25 | 71 | +-- | IDC | III | 1.7 | 2 | 0 | Weekly Paclitaxel x12+Tras x4 |
| 26 | 43 | --- | IDC | II-III | 5.6 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 27 | 80 | --- | IDC | III | 10 | 2 | 1 | AC x4, then weekly paclitaxel x12 |
| 28 | 37 | ++- | ILC | I-II | 12 | 3 | 1 | FEC100 x3, then Doce100x3 |
| 29 | 27 | --- | IDC | II-III | 1.8 | 1 | 0 | AC—Paclitaxel, DD, 8 cycles |
| 30 | 37 | +++ | IDC | II | 2.6 | 2 | 0 | FEC100 x3, then Doce100x3 |
| 31 | 60 | --- | IDC | III | 3.2 | 3 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 32 | 72 | ++- | IDC | I | 3.4 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 33 | 45 | ++- | IDC | III | 9.5 | 2 | 1 | AC x4, then weekly paclitaxel x12 |
| 34 | 43 | --- | IDC | III | 2.1 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 35 | 53 | --+ | IDC | III | 2.5 | 2 | 1 | AC x4, then Paclitaxel (DD) + Tras x4 |
| 36 | 54 | +-+ | IDC | II | 3.5 | 2 | 0 | FEC100 x3, then Doce100 + Tras x3 |
| 37 | 48 | +-+ | IDC | III | 7.5 | 1 | 1 | FEC100 x3, then Doce100 + Tras x3 |
| 38 | 68 | +-- | IDC | III | 3.6 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 39 | 51 | ++- | IDC | II | 11 | 3 | 1 | FEC100 x3, then Doce100x3 |
| 40 | 73 | ++- | IDC | III | 7.8 | 3 | 2 | AC—Paclitaxel (DD), 8 cycles |
| 41 | 61 | --+ | IDC | III | 2.9 | 2 | 0 | FEC100 x3, then Doce100 + Tras x3 |
| 42 | 44 | +-- | IDC | III | 6.4 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 43 | 29 | ++- | IDC | III | 8.3 | 3 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 44 | 65 | --- | IDC | II | 2.3 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 45 | 43 | --- | IDC | III | 2.4 | 4 | 0 | AC (DD) x4, then weekly paclitaxel x12 |
| 46 | 32 | +++ | IDC | II | 7.5 | 3 | 1 | AC (DD) x4, then weekly paclitaxel x12 + Tras x 4 |
| 47 | 68 | ++- | IDC | II | 5 | 4 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 48 | 41 | ++- | IDC | II | 2.9 | 1 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 49 | 34 | --- | IDC | III | 1.9 | 1 | 1 | Docetaxel-cyclophosphamide, 4 cycles |
| 50 | 51 | --- | IDC | III | 1.9 | 1 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 51 | 42 | --+ | IDC | III | 3.6 | 2 | 1 | AC (DD) x4, then weekly paclitaxel x12 + Tras x 4 |
| 52 | 51 | ++- | IDC | III | 3.3 | 2 | 0 | AC—Paclitaxel (DD), 8 cycles |
| 53 * | 31 | +++ | IDC | III | 2.6 | 2 | 1 | AC (DD) x4, then weekly paclitaxel x12 + Tras x 4 |
| 54 | 44 | --+ | IDC | III | 3.7 | 2 | 0 | FEC100 x3, then Doce100 + Tras x3 |
| 55 | 47 | ++- | IDC | III | 4.8 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| 56 | 34 | ++- | IDC | II | 3.2 | 2 | 1 | AC—Paclitaxel (DD), 8 cycles |
| No | Post-NAC Tumour Size (cm) | Overall Cellularity | RCB Score | Actual Response | Predicted Response |
|---|---|---|---|---|---|
| 1 | 2.7 | 50 | 2.24 | NR | NR |
| 2 | 2.5 | 11.25 | 2.92 | R | R |
| 3 | 3 | 3 | 2.51 | R | R |
| 4 | 1.3 | 75 | 1.98 | R | NR |
| 5 | 0 | 0 | 0 | R | R |
| 6 | 5.28 | 13.3 | 3.51 | R | R |
| 7 | 5.7 | 0.2 | 0.92 | R | R |
| 8 | 0 | 15 | 0 | R | R |
| 9 | 7.2 | 5 | 2.72 | R | R |
| 10 | 2.5 | 3 | 1.27 | R | R |
| 11 | 2.4 | 9 | 3.24 | R | R |
| 12 | 2 | 5 | 2.36 | R | NR |
| 13 | 6 | 0 | 0 | R | R |
| 14 | 1.2 | 0 | 0 | R | R |
| 15 | 0.5 | 40 | 1.58 | R | R |
| 16 | 1.9 | 80 | 3.09 | R | R |
| 17 | 2.5 | 10 | 1.59 | R | R |
| 18 | 3.2 | 10 | 3.09 | R | NR |
| 19 * | 4 | 10 | 3.01 | NR | R |
| 20 | 2 | 0 | 0 | R | R |
| 21 * | 3.5 | - | - | NR | NR |
| 22 | 1.5 | 0 | 0 | R | R |
| 23 | 7.5 | 15 | 3.82 | R | R |
| 24 | 1.7 | 5 | no score | R | R |
| 25 | 0 | 0 | 0 | R | R |
| 26 | 1.8 | 1 | 0.37 | R | R |
| 27 | 4 | 10 | 3.20 | R | R |
| 28 | 8 | 15 | 3.62 | R | R |
| 29 | 1.5 | 10 | 1.29 | R | R |
| 30 | 2.5 | 10 | 2.35 | R | R |
| 31 | 2.5 | 30 | 1.94 | R | R |
| 32 | 1.5 | 30 | 2.87 | R | R |
| 33 | 4 | 25 | 1.99 | R | R |
| 34 | 0.2 | 10 | 0.95 | R | R |
| 35 | 2.5 | 3.66 | 0.92 | R | R |
| 36 | 0 | 0 | pCR | R | R |
| 37 | 0.65 | 5 | 2.41 | R | R |
| 38 | 4 | 40 | 3.83 | R | R |
| 39 | 8.85 | 6.5 | 3.56 | R | R |
| 40 | 4.5 | 1 | 1.2 | R | R |
| 41 | 1.4 | 10 | 1.33 | R | R |
| 42 | 4 | 0 | pCR | R | R |
| 43 | 8 | 2 | 2.72 | R | R |
| 44 | 0.9 | 15 | 1.43 | R | R |
| 45 | 2 | 0 | 0 | R | R |
| 46 | 6.6 | 5.5 | 3.48 | R | R |
| 47 | 2 | 12.5 | 1.60 | R | R |
| 48 | 2.8 | 25 | 3.07 | R | R |
| 49 | 1.3 | 0 | pCR | R | R |
| 50 | 2.5 | 70 | 3.88 | NR | NR |
| 51 | 3.5 | 1 | 0.78 | R | R |
| 52 | 5.5 | 0.05 | 0.72 | R | R |
| 53 * | 7.86 | 1.72 | 1.12 | NR | R |
| 54 | 0 | 0 | pCR | R | R |
| 55 | 2 | 75 | 3.85 | R | R |
| 56 | 6.5 | 15 | 3.12 | NR | NR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, A.W.; Sannachi, L.; Moore-Palhares, D.; Dasgupta, A.; Gandhi, S.; Pezo, R.; Eisen, A.; Warner, E.; Wright, F.C.; Hong, N.L.; et al. Validation of Quantitative Ultrasound and Texture Derivative Analyses-Based Model for Upfront Prediction of Neoadjuvant Chemotherapy Response in Breast Cancer. J. Imaging 2025, 11, 109. https://doi.org/10.3390/jimaging11040109
Chan AW, Sannachi L, Moore-Palhares D, Dasgupta A, Gandhi S, Pezo R, Eisen A, Warner E, Wright FC, Hong NL, et al. Validation of Quantitative Ultrasound and Texture Derivative Analyses-Based Model for Upfront Prediction of Neoadjuvant Chemotherapy Response in Breast Cancer. Journal of Imaging. 2025; 11(4):109. https://doi.org/10.3390/jimaging11040109
Chicago/Turabian StyleChan, Adrian Wai, Lakshmanan Sannachi, Daniel Moore-Palhares, Archya Dasgupta, Sonal Gandhi, Rossanna Pezo, Andrea Eisen, Ellen Warner, Frances C. Wright, Nicole Look Hong, and et al. 2025. "Validation of Quantitative Ultrasound and Texture Derivative Analyses-Based Model for Upfront Prediction of Neoadjuvant Chemotherapy Response in Breast Cancer" Journal of Imaging 11, no. 4: 109. https://doi.org/10.3390/jimaging11040109
APA StyleChan, A. W., Sannachi, L., Moore-Palhares, D., Dasgupta, A., Gandhi, S., Pezo, R., Eisen, A., Warner, E., Wright, F. C., Hong, N. L., Sadeghi-Naini, A., Skarpathiotakis, M., Curpen, B., Betel, C., Kolios, M. C., Trudeau, M., & Czarnota, G. J. (2025). Validation of Quantitative Ultrasound and Texture Derivative Analyses-Based Model for Upfront Prediction of Neoadjuvant Chemotherapy Response in Breast Cancer. Journal of Imaging, 11(4), 109. https://doi.org/10.3390/jimaging11040109