

Evaluation of Non-Invasive Methods for (R)-[11C]PK11195 PET Image Quantification in Multiple Sclerosis

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Image Acquisition
2.3. Image Reconstruction
2.4. Image Processing
2.5. Input Functions: Extraction
2.6. PET Quantification
2.7. Statistical Analysis
3. Results
3.1. Input Functions: Extraction and Corrections
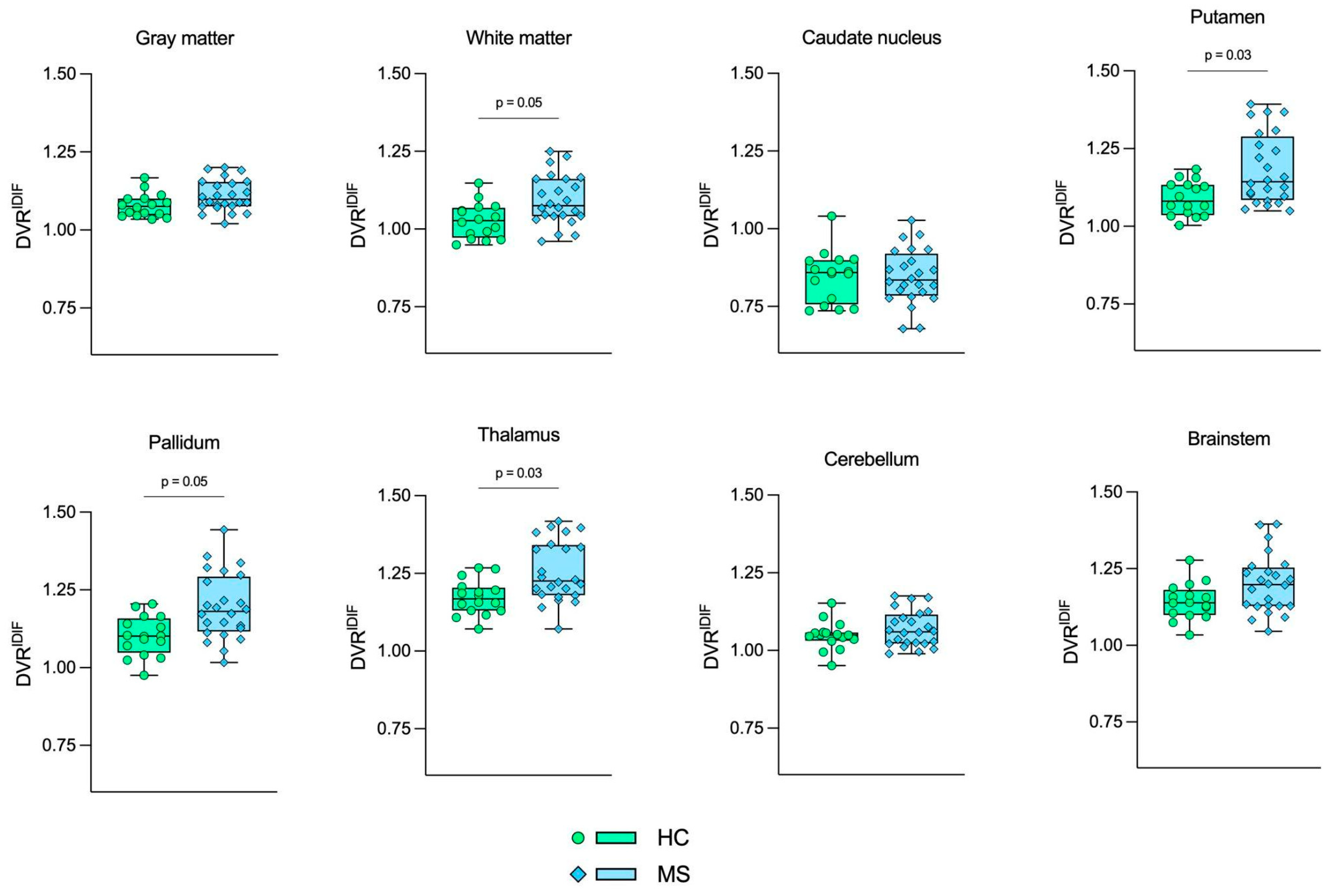
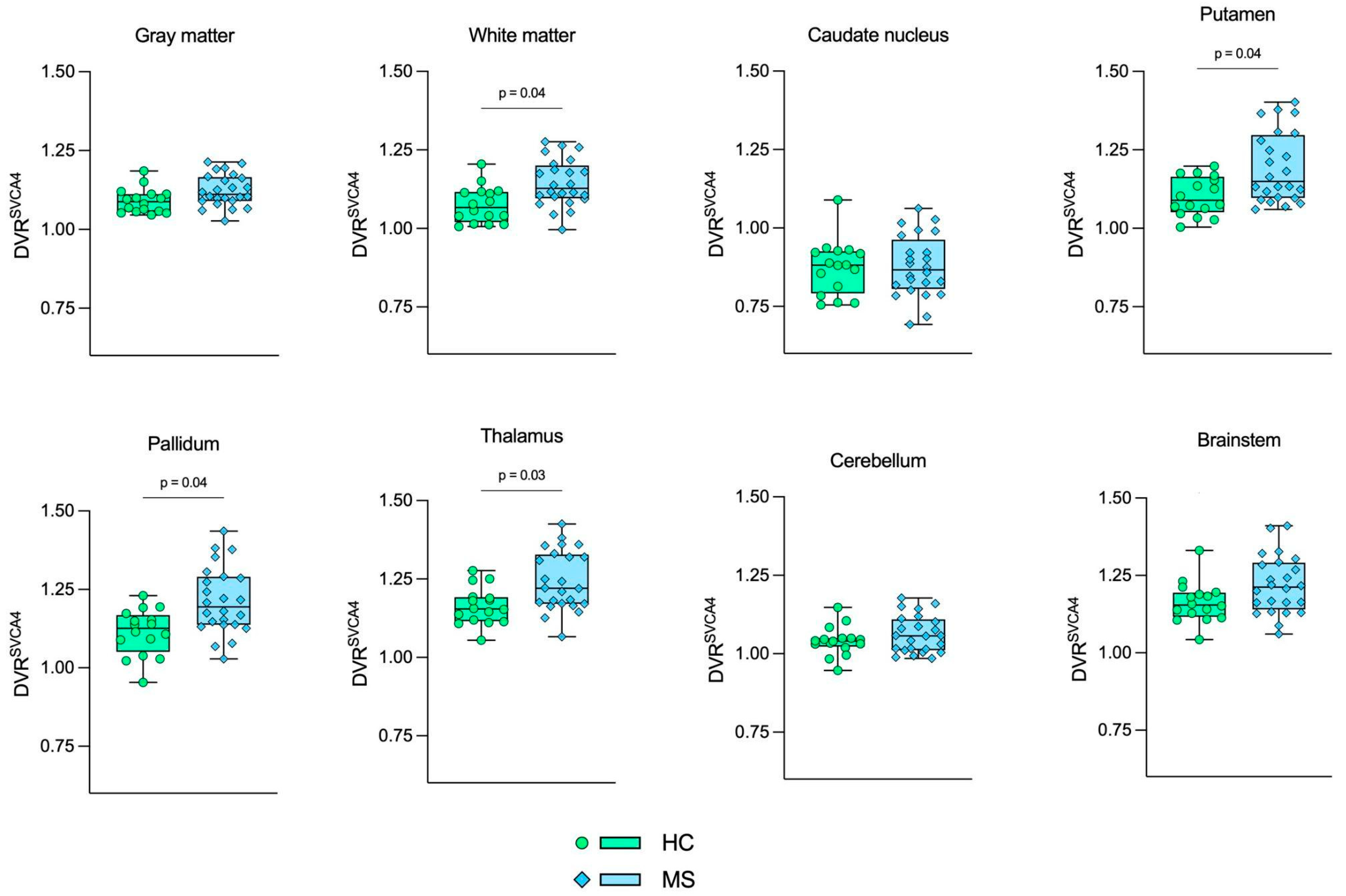
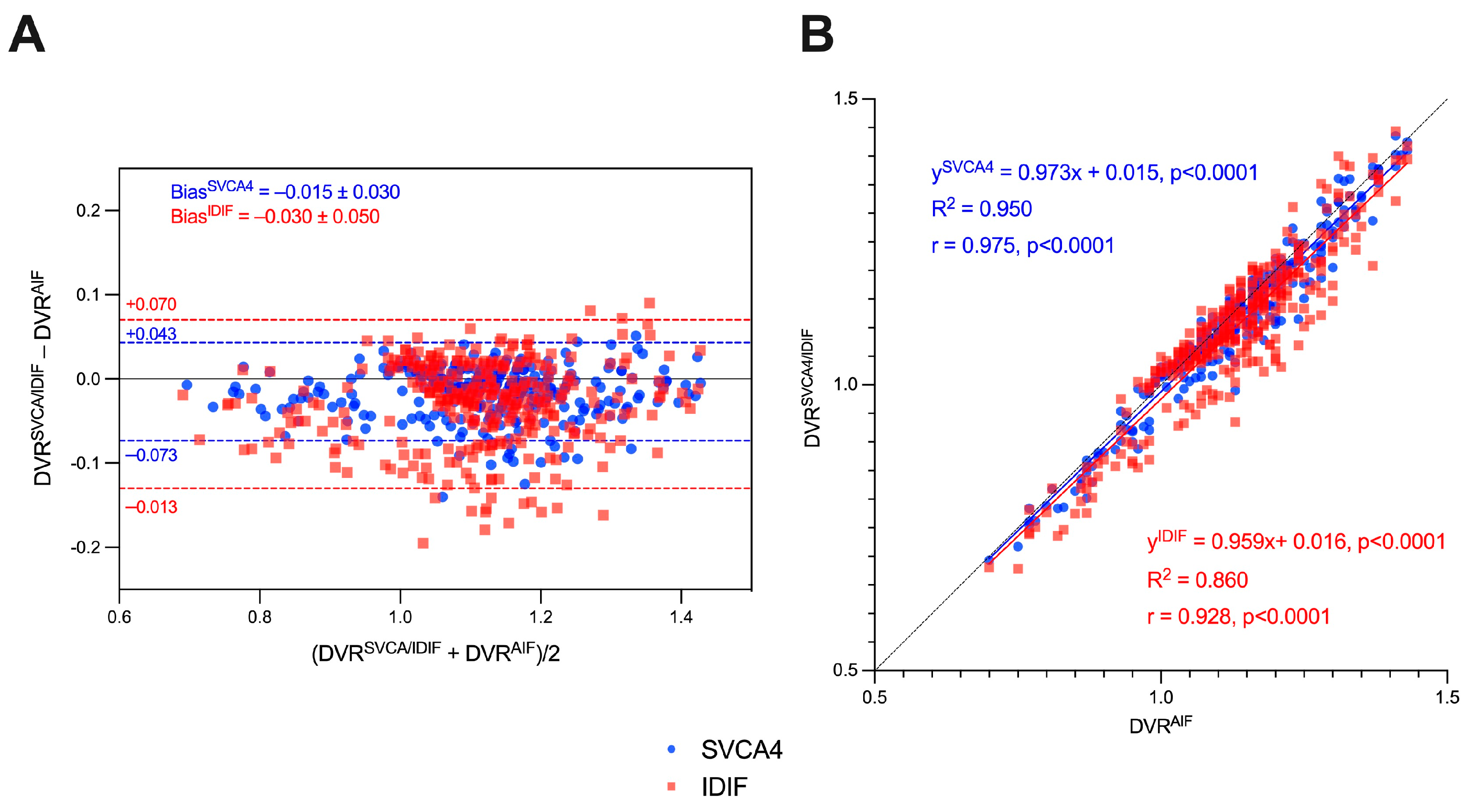
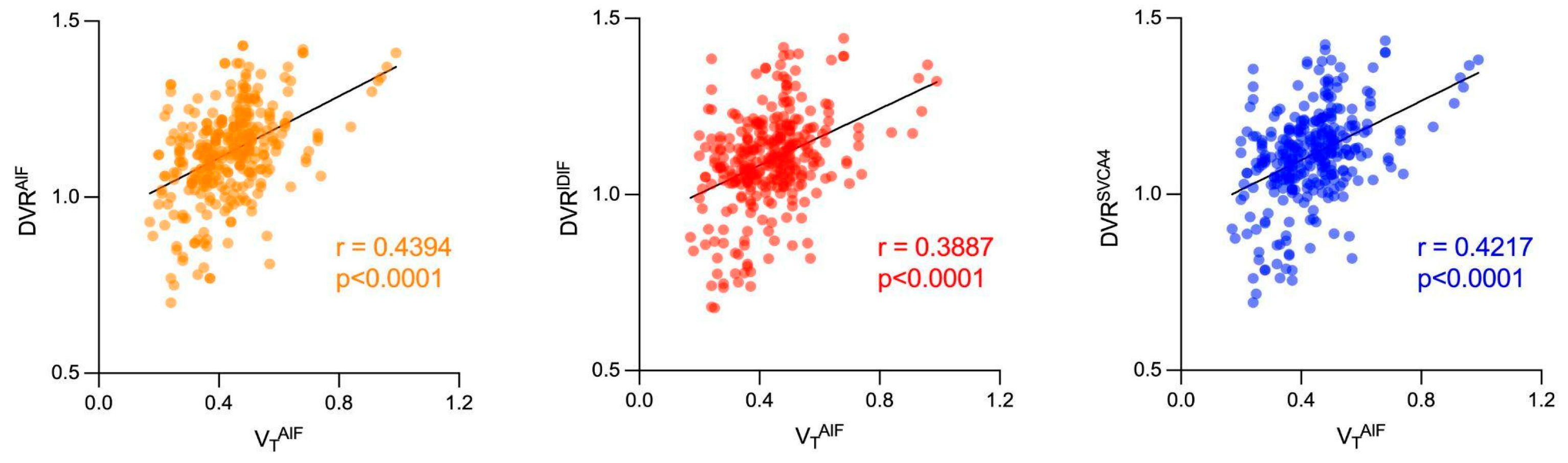
3.2. Image Quantification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finkelsztejn, A.; Cristovam, R.d.A.; Moraes, G.S.; Lopes, M.G.; Silva, A.V.; Garcia, M.S.; Cola, C.M.; Bastiani, C.E.; Ferreira, L.B.; da Costa, A.L.; et al. Clinical features of multiple sclerosis in the south of Brazil: A partial analysis. Arq. Neuropsiquiatr. 2009, 67, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Samkoff, L.M.; Goodman, A.D. (Eds.) Multiple Sclerosis and CNS Inflammatory Disorders; John Wiley & Sons Inc.: Chichester, UK, 2014; 1p. [Google Scholar]
- Banati, R.B.; Newcombe, J.; Gunn, R.N.; Cagnin, A.; Turkheimer, F.; Heppner, F.; Price, G.; Wegner, F.; Giovannoni, G.; Miller, D.H.; et al. The peripheral benzodiazepine binding site in the brain in multiple sclerosis. Brain 2000, 123, 2321–2337. [Google Scholar] [CrossRef] [PubMed]
- Jučaite, A.; Cselényi, Z.; Arvidsson, A.; Ahlberg, G.; Julin, P.; Varnäs, K.; Stenkrona, P.; Andersson, J.; Halldin, C.; Farde, L. Kinetic analysis and test-retest variability of the radioligand [11C](R)-PK11195 binding to TSPO in the human brain—A PET study in control subjects. EJNMMI Res. 2012, 2, 15. [Google Scholar] [CrossRef]
- Lammertsma, A.A. Forward to the Past: The Case for Quantitative PET Imaging. J. Nucl. Med. 2017, 58, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Rahmim, A.; Gunn, R.N. PET Parametric Imaging: Past, Present, and Future. IEEE Trans. Radiat. Plasma Med. Sci. 2020, 4, 663–675. [Google Scholar] [CrossRef] [PubMed]
- van der Weijden, C.W.J.; Mossel, P.; Bartels, A.L.; Dierckx, R.A.J.O.; Luurtsema, G.; Lammertsma, A.A.; Willemsen, A.T.M.; de Vries, E.F.J. Non-invasive kinetic modelling approaches for quantitative analysis of brain PET studies. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 1636–1650. [Google Scholar] [CrossRef] [PubMed]
- Zanotti-Fregonara, P.; Fadaili, E.M.; Maroy, R.; Comtat, C.; Souloumiac, A.; Jan, S.; Ribeiro, M.J.; Gaura, V.; Bar-Hen, A.; Trébossen, R. Comparison of Eight Methods for the Estimation of the Image-Derived Input Function in Dynamic [18F]-FDG PET Human Brain Studies. J. Cereb. Blood Flow. Metab. 2009, 29, 1825–1835. [Google Scholar] [CrossRef] [PubMed]
- Zanotti-Fregonara, P.; Liow, J.S.; Comtat, C.; Zoghbi, S.S.; Zhang, Y.; Pike, V.W.; Fujita, M.; Innis, R.B. Image-derived input function in PET brain studies: Blood-based methods are resistant to motion artifacts. Nucl. Med. Commun. 2012, 33, 982–989. [Google Scholar] [CrossRef]
- Croteau, E.; Lavallée, E.; Labbe, S.M.; Hubert, L.; Pifferi, F.; Rousseau, J.A.; Cunnane, S.C.; Carpentier, A.C.; Lecomte, R.; Bénard, F. Image-derived input function in dynamic human PET/CT: Methodology and validation with 11C-acetate and 18F-fluorothioheptadecanoic acid in muscle and 18F-fluorodeoxyglucose in brain. Eur. J. Nucl. Med. Mol. Imaging. 2010, 37, 1539–1550. [Google Scholar] [CrossRef]
- Politis, M.; Giannetti, P.; Su, P.; Turkheimer, F.; Keihaninejad, S.; Wu, K.; Waldman, A.; Malik, O.; Matthews, P.M.; Reynolds, R.; et al. Increased PK11195 PET binding in the cortex of patients with MS correlates with disability. Neurology 2012, 79, 523–530. [Google Scholar] [CrossRef]
- Kang, Y.; Schlyer, D.; Kaunzner, U.W.; Kuceyeski, A.; Kothari, P.J.; Gauthier, S.A. Comparison of two different methods of image analysis for the assessment of microglial activation in patients with multiple sclerosis using (R)-[N-methyl-carbon-11]PK11195. PLoS ONE 2018, 13, e0201289. [Google Scholar] [CrossRef]
- Kaunzner, U.W.; Kang, Y.; Zhang, S.; Morris, E.; Yao, Y.; Pandya, S.; Rua, S.M.H.; Park, C.; Gillen, K.M.; Nguyen, T.D.; et al. Quantitative susceptibility mapping identifies inflammation in a subset of chronic multiple sclerosis lesions. Brain 2019, 142, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Kropholler, M.A.; Boellaard, R.; Schuitemaker, A.; Folkersma, H.; van Berckel, B.N.; Lammertsma, A.A. Evaluation of Reference Tissue Models for the Analysis of [11C](R)-PK11195 Studies. J. Cereb. Blood Flow. Metab. 2006, 26, 1431–1441. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Veronese, M.; Tonietto, M.; Bodini, B.; Stankoff, B.; Wimberley, C.; Lavisse, S.; Bottlaender, M.; Bloomfield, P.S.; Howes, O.; et al. Generalization of endothelial modelling of TSPO PET imaging: Considerations on tracer affinities. J. Cereb. Blood Flow. Metab. 2019, 39, 874–885. [Google Scholar] [CrossRef] [PubMed]
- Stokholm, M.G.; Iranzo, A.; Østergaard, K.; Serradell, M.; Otto, M.; Svendsen, K.B.; Garrido, A.; Vilas, D.; Borghammer, P.; Santamaria, J.; et al. Assessment of neuroinflammation in patients with idiopathic rapid-eye-movement sleep behaviour disorder: A case-control study. Lancet Neurol. 2017, 16, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Passamonti, L.; Vázquez, R.P.; Hong, Y.; Allinson, K.S.; Williamson, D.; Borchert, R.J.; Sami, S.; Cope, T.; Bevan-Jones, W.; Jones, S.; et al. 18 F-AV-1451 positron emission tomography in Alzheimer’s disease and progressive supranuclear palsy. Brain 2017, 24, 340. [Google Scholar] [CrossRef]
- Turkheimer, F.E.; Edison, P.; Pavese, N.; Roncaroli, F.; Anderson, A.N.; Hammers, A.; Gerhard, A.; Hinz, R.; Tai, Y.F.; Brooks, D. Reference and target region modeling of [11C]-(R)-PK11195 brain studies. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 158–167. [Google Scholar]
- Boellaard, R.; Turkheimer, F.E.; Hinz, R.; Schuitemaker, A.; Scheltens, P.; van Berckel, B.N.M.; Lammertsma, A.A. Performance of a modified supervised cluster algorithm for extracting reference region input functions from (R)-(R)-[11C]PK11195 brain PET studies. In 2008 IEEE Nuclear Science Symposium Conference Record; IEEE: Dresden, Germany, 2008; pp. 5400–5402. Available online: http://ieeexplore.ieee.org/document/4774453 (accessed on 16 February 2023).
- Yaqub, M.; van Berckel, B.N.; Schuitemaker, A.; Hinz, R.; E Turkheimer, F.; Tomasi, G.; Lammertsma, A.A.; Boellaard, R. Optimization of Supervised Cluster Analysis for Extracting Reference Tissue Input Curves in (R)-[11C]PK11195 Brain PET Studies. J. Cereb. Blood Flow. Metab. 2012, 32, 1600–1608. [Google Scholar] [CrossRef]
- Giannetti, P.; Politis, M.; Su, P.; Turkheimer, F.; Malik, O.; Keihaninejad, S.; Wu, K.; Reynolds, R.; Nicholas, R.; Piccini, P. Microglia activation in multiple sclerosis black holes predicts outcome in progressive patients: An in vivo [(11)C](R)-PK11195-PET pilot study. Neurobiol. Dis. 2014, 65, 203–210. [Google Scholar] [CrossRef]
- Rissanen, E.; Tuisku, J.; Rokka, J.; Paavilainen, T.; Parkkola, R.; Rinne, J.O.; Airas, L. In Vivo Detection of Diffuse Inflammation in Secondary Progressive Multiple Sclerosis Using PET Imaging and the Radioligand 11C-PK11195. J. Nucl. Med. 2014, 55, 939–944. [Google Scholar] [CrossRef]
- Rissanen, E.; Tuisku, J.; Vahlberg, T.; Sucksdorff, M.; Paavilainen, T.; Parkkola, R.; Rokka, J.; Gerhard, A.; Hinz, R.; Talbot, P.S. Microglial activation, white matter tract damage, and disability in MS. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, e443. [Google Scholar] [CrossRef]
- Sucksdorff, M.; Rissanen, E.; Tuisku, J.; Nuutinen, S.; Paavilainen, T.; Rokka, J.; Rinne, J.; Airas, L. Evaluation of the Effect of Fingolimod Treatment on Microglial Activation Using Serial PET Imaging in Multiple Sclerosis. J. Nucl. Med. 2017, 58, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Kaunzner, U.W.; Kang, Y.; Monohan, E.; Kothari, P.J.; Nealon, N.; Perumal, J.; Vartanian, T.; Kuceyeski, A.; Vallabhajosula, S.; Mozley, P.D.; et al. Reduction of PK11195 uptake observed in multiple sclerosis lesions after natalizumab initiation. Mult. Scler. Relat. Disord. 2017, 15, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Pitombeira, M.S.; Koole, M.; Campanholo, K.R.; Souza, A.M.; Duran, F.L.S.; Solla, D.J.F.; Mendes, M.F.; Pereira, S.L.A.; Rimkus, C.M.; Busatto, G.F.; et al. Innate immune cells and myelin profile in multiple sclerosis: A multi-tracer PET/MR study. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 4551–4566. [Google Scholar] [CrossRef] [PubMed]
- de Souza, A.M.; Pitombeira, M.S.; de Souza, L.E.; Marques, F.L.N.; Buchpiguel, C.A.; Real, C.C.; de Paula Faria, D. 11C-PK11195 plasma metabolization has the same rate in multiple sclerosis patients and healthy controls: A cross-sectional study. Neural Regen. Res. 2021, 16, 2494. [Google Scholar] [PubMed]
- Hammers, A.; Allom, R.; Koepp, M.J.; Free, S.L.; Myers, R.; Lemieux, L.; Mitchell, T.N.; Brooks, D.J.; Duncan, J.S. Three-dimensional maximum probability atlas of the human brain, with particular reference to the temporal lobe. Hum. Brain Mapp. 2003, 19, 224–247. [Google Scholar] [CrossRef] [PubMed]
- Gousias, I.S.; Rueckert, D.; Heckemann, R.A.; Dyet, L.E.; Boardman, J.P.; Edwards, A.D.; Hammers, A. Automatic segmentation of brain MRIs of 2-year-olds into 83 regions of interest. NeuroImage 2008, 40, 672–684. [Google Scholar] [CrossRef]
- Schubert, J.; Tonietto, M.; Turkheimer, F.; Zanotti-Fregonara, P.; Veronese, M. Supervised clustering for TSPO PET imaging. Eur. J. Nucl. Med. Mol. Imaging 2021, 49, 257–268. [Google Scholar] [CrossRef]
- Logan, J. Graphical analysis of PET data applied to reversible and irreversible tracers. Nucl. Med. Biol. 2000, 27, 661–670. [Google Scholar] [CrossRef]
- Logan, J.; Fowler, J.S.; Volkow, N.D.; Wang, G.J.; Ding, Y.S.; Alexoff, D.L. Distribution Volume Ratios without Blood Sampling from Graphical Analysis of PET Data. J. Cereb. Blood Flow. Metab. 1996, 16, 834–840. [Google Scholar] [CrossRef]
- Wimberley, C.; Lavisse, S.; Hillmer, A.; Hinz, R.; Turkheimer, F.; Zanotti-Fregonara, P. Kinetic modeling and parameter estimation of TSPO PET imaging in the human brain. Eur. J. Nucl. Med. Mol. Imaging 2021, 49, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Hunter, C.R.R.N.; Klein, R.; Beanlands, R.S.; Dekemp, R.A. Patient motion effects on the quantification of regional myocardial blood flow with dynamic PET imaging. Med. Phys. 2016, 43, 1829–1840. [Google Scholar] [CrossRef] [PubMed]
- De Pierro, A.R. A modified expectation maximization algorithm for penalized likelihood estimation in emission tomography. IEEE Trans. Med. Imaging 1995, 14, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Qi, J.; Huesman, R.H. List mode reconstruction for PET with motion compensation: A simulation study. In Proceedings of the IEEE International Symposium on Biomedical Imaging, Washington, DC, USA, 7–10 July 2002; IEEE: Washington, WA, USA, 2002; pp. 413–416. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HC | RRMS | p-Value | |
|---|---|---|---|
| Age (years) | 41.8 ± 12.7 | 35.0 ± 7.6 | 0.06 & |
| Sex (F/M) | 11/5 | 16/8 | 0.73 # |
| Education (years) | 14.2 ± 3.9 | 13.7 ± 3.6 | 0.70 & |
| EDSS (range) | - | 1.0–6.0 | - |
| Disease duration (years) | - | 9.1 ± 6.4 | - |
| Number of relapses | - | 7.0 ± 8.0 | - |
| Use of DMT (Y/N) | - | 22/2 | - |
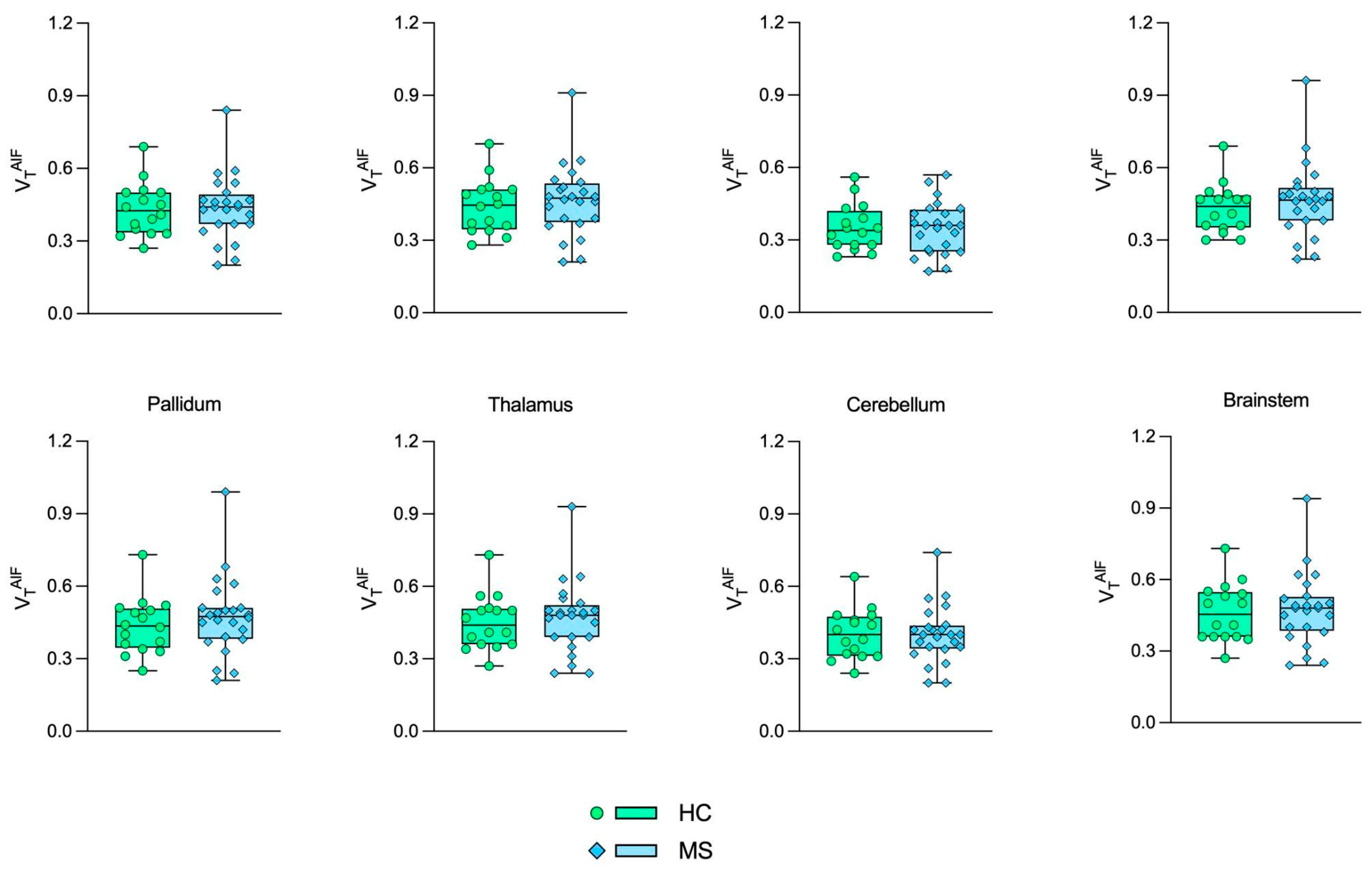
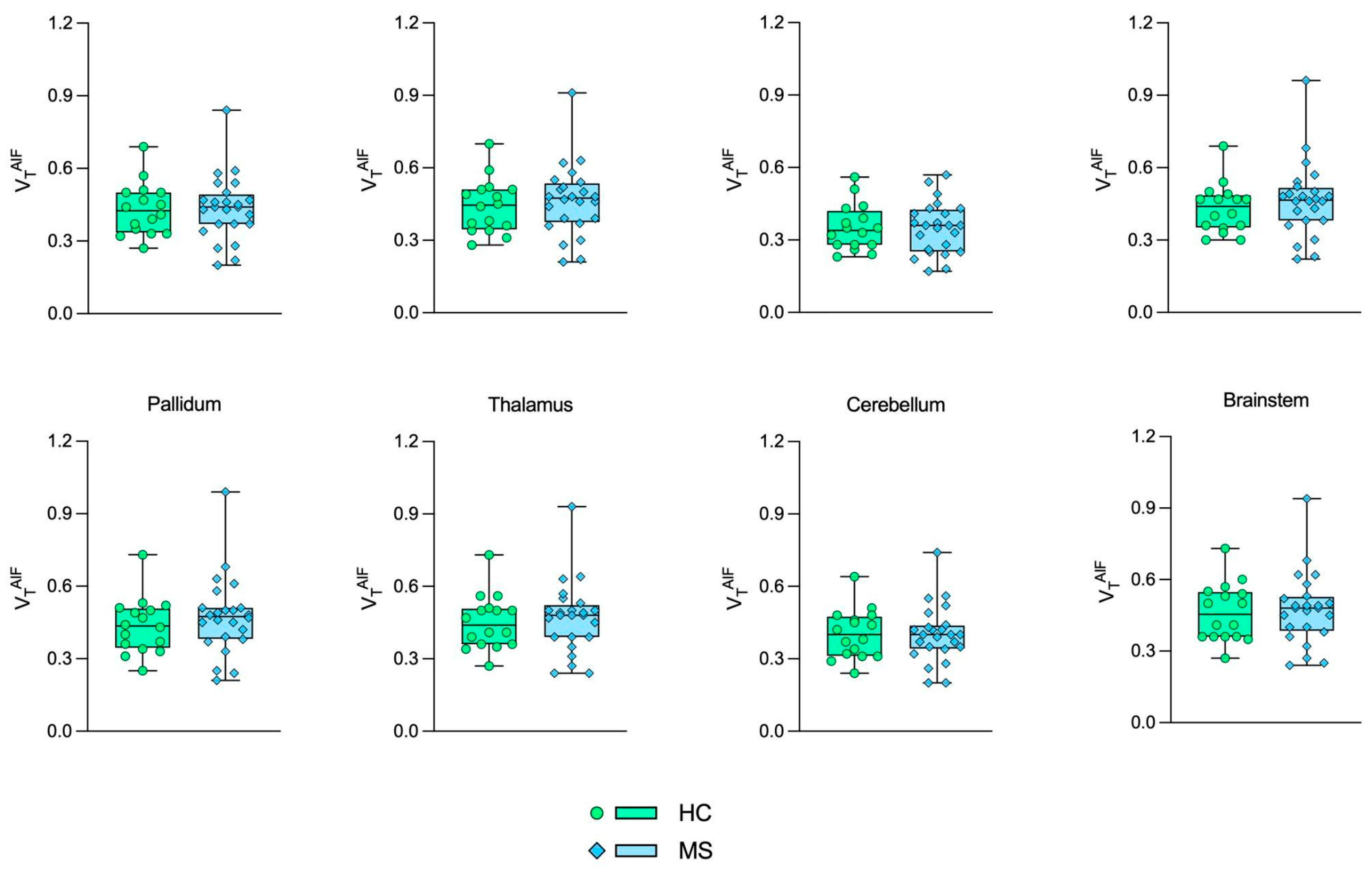
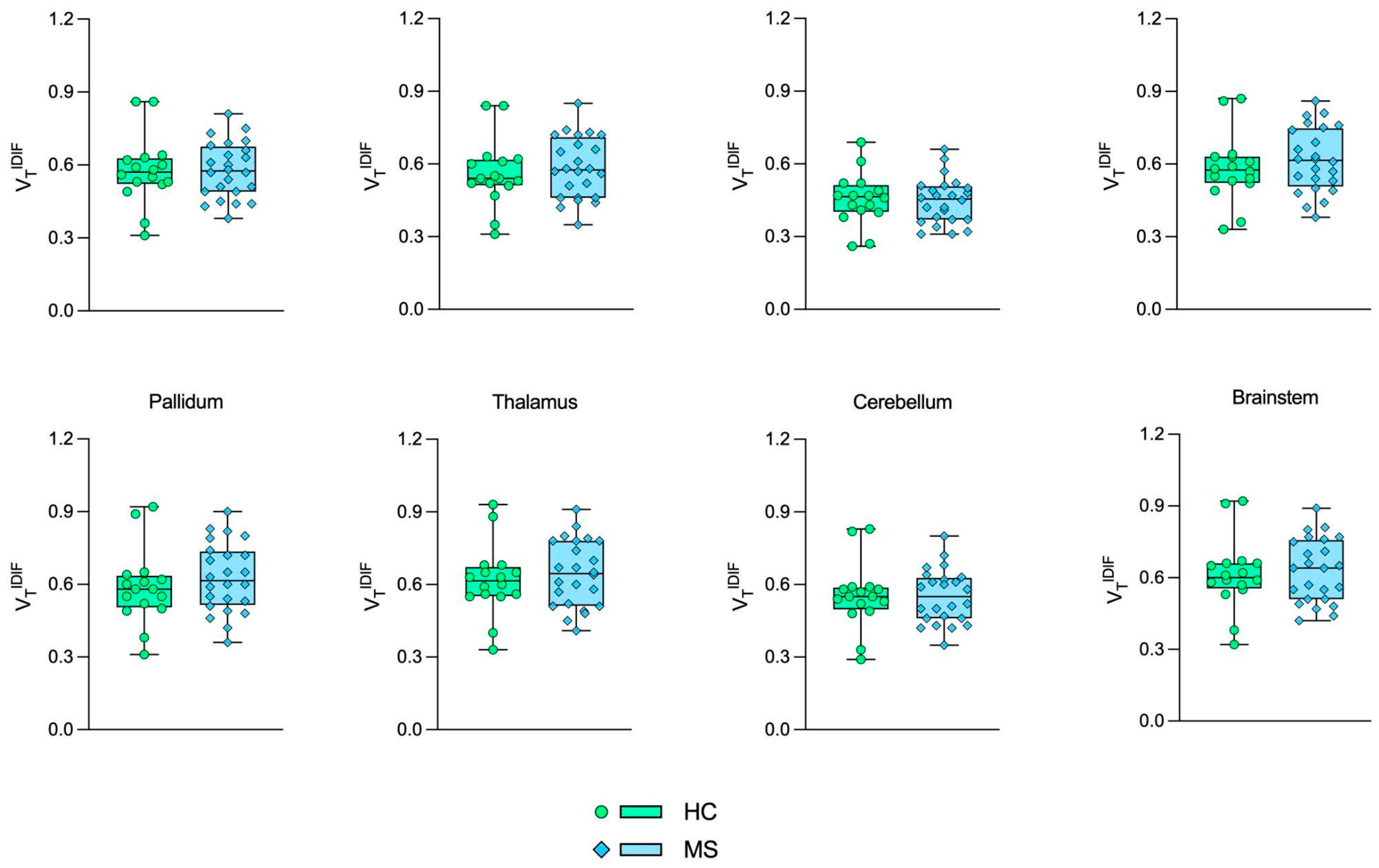
| AIF a | IDIF a | |||||
|---|---|---|---|---|---|---|
| HC b (n = 16) | MS b (n = 24) | p-Value c | HC b (n = 16) | MS b (n = 24) | p-Value c | |
| Gray matter | 0.43 ± 0.11 | 0.44 ± 0.13 | 0.86 | 0.58 ± 0.14 | 0.58 ± 0.12 | 0.24 |
| White matter | 0.44 ± 0.11 | 0.46 ± 0.15 | 0.80 | 0.56 ± 0.14 | 0.58 ± 0.13 | 0.23 |
| Caudate nucleus | 0.35 ± 0.09 | 0.35 ± 0.11 | 0.61 | 0.46 ± 0.11 | 0.45 ± 0.09 | 0.41 |
| Putamen | 0.43 ± 0.10 | 0.46 ± 0.15 | 0.77 | 0.58 ± 0.14 | 0.62 ± 0.13 | 0.17 |
| Pallidum | 0.44 ± 0.12 | 0.47 ± 0.16 | 0.77 | 0.59 ± 0.15 | 0.63 ± 0.14 | 0.18 |
| Thalamus | 0.45 ± 0.11 | 0.47 ± 0.15 | 0.84 | 0.62 ± 0.15 | 0.65 ± 0.14 | 0.19 |
| Cerebellum | 0.40 ± 0.10 | 0.40 ± 0.12 | 0.88 | 0.55 ± 0.14 | 0.55 ± 0.11 | 0.23 |
| Brainstem | 0.46 ± 0.12 | 0.47 ± 0.15 | 0.79 | 0.61 ± 0.15 | 0.63 ± 0.13 | 0.34 |
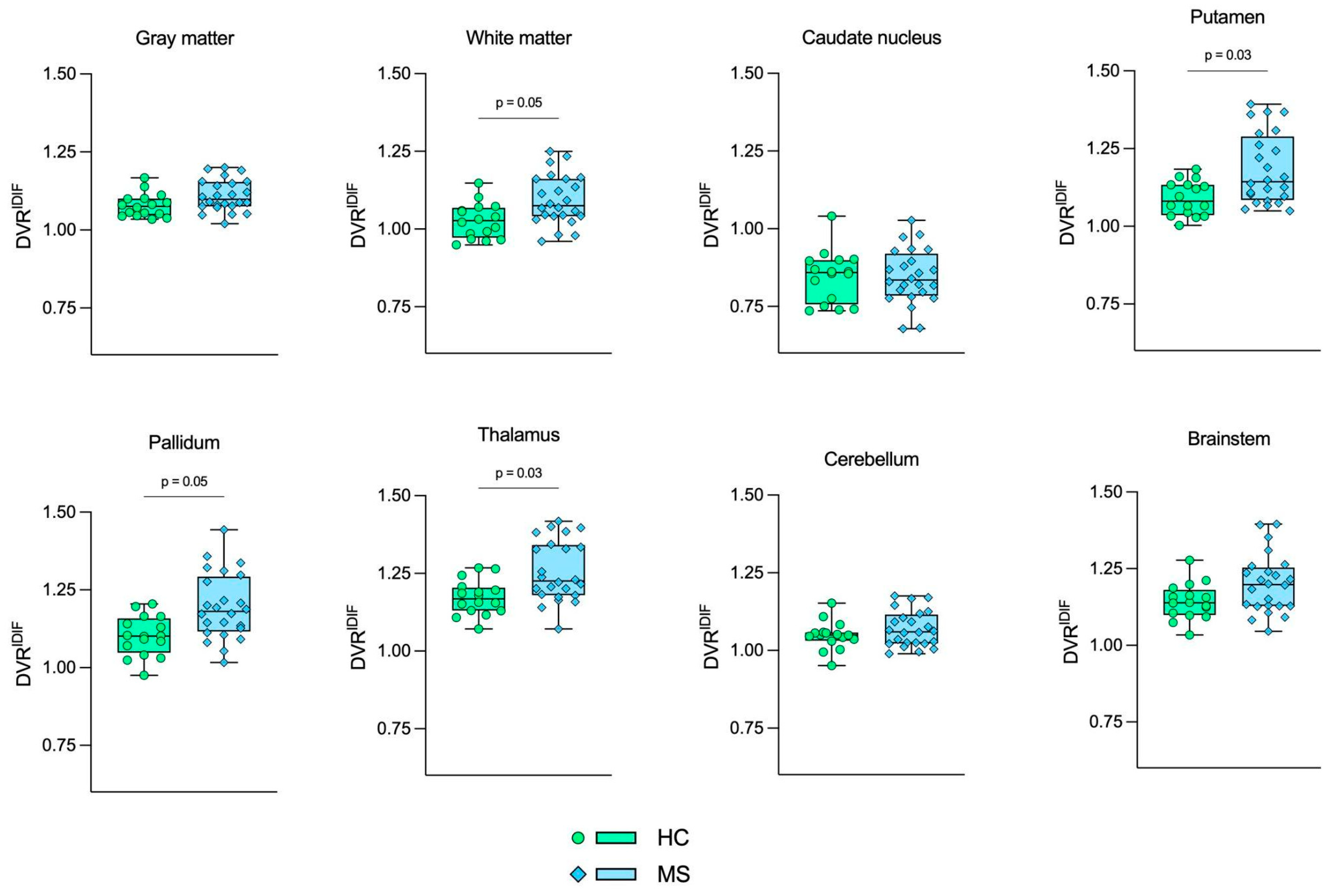
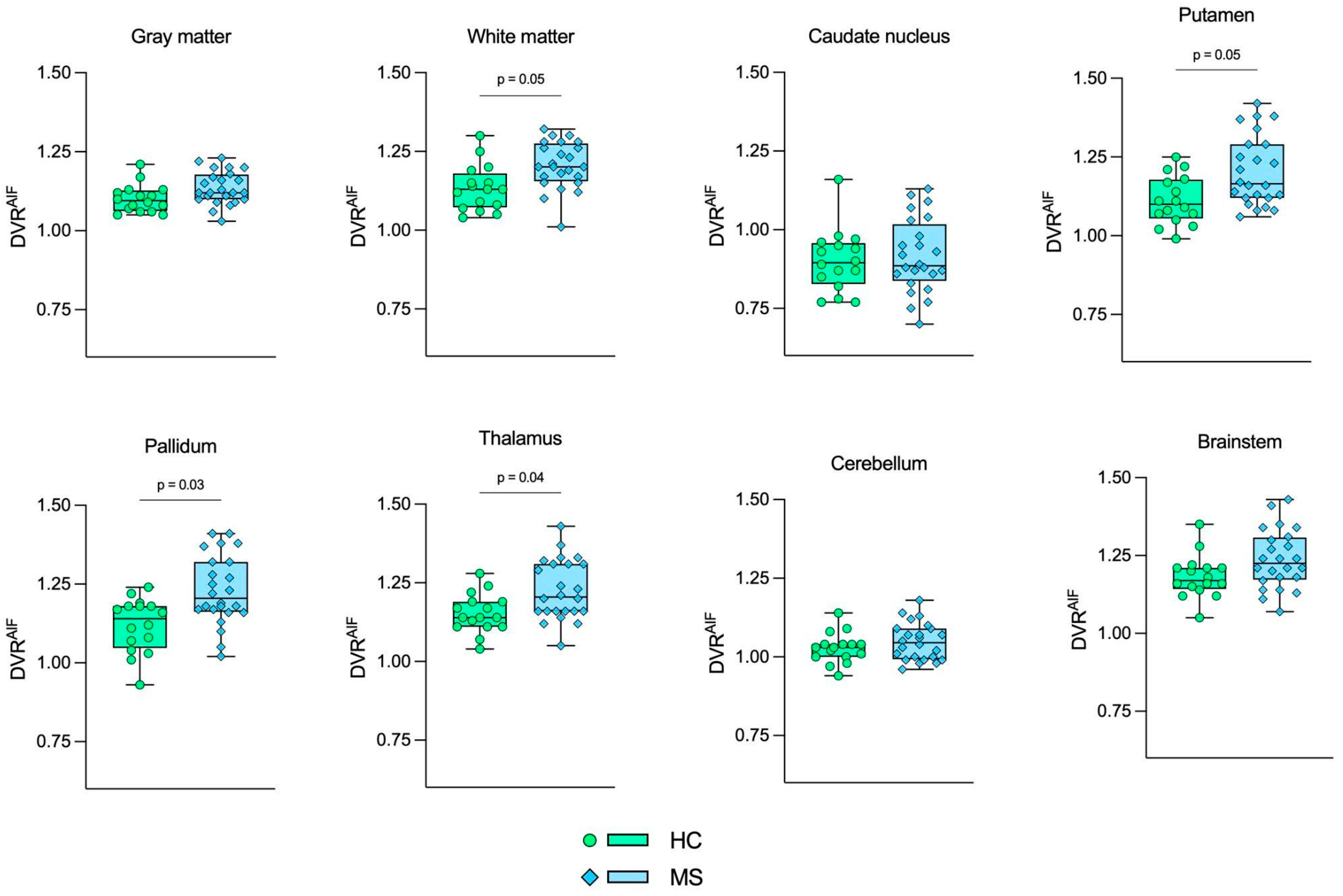
| AIF | IDIF | SVCA4 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HC a (n = 16) | MS a (n = 24) | p-Value b | HC a (n = 16) | MS a (n = 24) | p-Value b | HC a (n = 16) | MS a (n = 24) | p-Value b | |
| Gray matter | 1.10 ± 0.04 | 1.13 ± 0.05 | 0.12 | 1.07 ± 0.03 | 1.11 ± 0.05 | 0.08 | 1.09 ± 0.03 | 1.12 ± 0.05 | 0.09 |
| White matter | 1.13 ± 0.07 | 1.20 ± 0.07 | 0.05 * | 1.02 ± 0.05 | 1.09 ± 0.08 | 0.05 * | 1.07 ± 0.05 | 1.14 ± 0.07 | 0.04 * |
| Caudate nucleus | 0.90 ± 0.09 | 0.91 ± 0.11 | 0.77 | 0.84 ± 0.08 | 0.84 ± 0.08 | 0.95 | 0.87 ± 0.08 | 0.87 ± 0.09 | 0.90 |
| Putamen | 1.11 ± 0.07 | 1.20 ± 0.11 | 0.05 * | 1.09 ± 0.05 | 1.18 ± 0.11 | 0.03 * | 1.10 ± 0.06 | 1.19 ± 0.11 | 0.04 * |
| Pallidum | 1.11 ± 0.08 | 1.23 ± 0.11 | 0.03 * | 1.10 ± 0.06 | 1.19 ± 0.10 | 0.05 * | 1.11 ± 0.07 | 1.21 ± 0.10 | 0.04 * |
| Thalamus | 1.15 ± 0.06 | 1.22 ± 0.09 | 0.04 * | 1.17 ± 0.05 | 1.25 ± 0.09 | 0.03 * | 1.16 ± 0.05 | 1.24 ± 0.09 | 0.03 * |
| Cerebellum | 1.02 ± 0.04 | 1.04 ± 0.05 | 0.46 | 1.04 ± 0.04 | 1.06 ± 0.05 | 0.51 | 1.03 ± 0.04 | 1.06 ± 0.05 | 0.44 |
| Brainstem | 1.18 ± 0.06 | 1.23 ± 0.09 | 0.09 | 1.14 ± 0.05 | 1.20 ± 0.09 | 0.13 | 1.16 ± 0.06 | 1.21 ± 0.09 | 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mantovani, D.B.A.; Pitombeira, M.S.; Schuck, P.N.; de Araújo, A.S.; Buchpiguel, C.A.; de Paula Faria, D.; M. da Silva, A.M. Evaluation of Non-Invasive Methods for (R)-[11C]PK11195 PET Image Quantification in Multiple Sclerosis. J. Imaging 2024, 10, 39. https://doi.org/10.3390/jimaging10020039
Mantovani DBA, Pitombeira MS, Schuck PN, de Araújo AS, Buchpiguel CA, de Paula Faria D, M. da Silva AM. Evaluation of Non-Invasive Methods for (R)-[11C]PK11195 PET Image Quantification in Multiple Sclerosis. Journal of Imaging. 2024; 10(2):39. https://doi.org/10.3390/jimaging10020039
Chicago/Turabian StyleMantovani, Dimitri B. A., Milena S. Pitombeira, Phelipi N. Schuck, Adriel S. de Araújo, Carlos Alberto Buchpiguel, Daniele de Paula Faria, and Ana Maria M. da Silva. 2024. "Evaluation of Non-Invasive Methods for (R)-[11C]PK11195 PET Image Quantification in Multiple Sclerosis" Journal of Imaging 10, no. 2: 39. https://doi.org/10.3390/jimaging10020039
APA StyleMantovani, D. B. A., Pitombeira, M. S., Schuck, P. N., de Araújo, A. S., Buchpiguel, C. A., de Paula Faria, D., & M. da Silva, A. M. (2024). Evaluation of Non-Invasive Methods for (R)-[11C]PK11195 PET Image Quantification in Multiple Sclerosis. Journal of Imaging, 10(2), 39. https://doi.org/10.3390/jimaging10020039