1. Introduction
This study aligns with UNESCO’s recognition of the vital importance of traditional medical knowledge, offering a nuanced analysis of the intersection between agricultural biodiversity and healthcare practices within Aymara communities.
The Aymara, also known as Aimara, are an indigenous people native to the Andean regions and the Altiplano of South America. Approximately 2.3 million Aymara people primarily reside in northwest Argentina, western Bolivia, northern Chile, and southern Peru.
The ancestors of the Aymara inhabited this region for centuries before being incorporated into the Inca Empire in the late 15th or early 16th century. Following the Spanish conquest in the 16th century, the Aymara people came under Spanish rule.
Traditionally, the Aymara people have relied on agriculture and livestock farming for their livelihoods.
The communities in the Altiplano and inter-Andean valleys are primarily dedicated to cultivating tubers, cereals, and grains, as detailed below, as well as raising cattle, sheep, camelids, and other small animals. Among the most important crops in Aymara agriculture are native species domesticated locally or in the region, such as
ch’uqi or
papa (
Solanum tuberosum L. and other
Solanum spp.),
cañawa (
Chenopodium pallidicaule Aellen),
quinua (
Chenopodium quinoa Willd.),
oca (
Oxalis tuberosa Molina),
isaño (
Tropaeolum tuberosum Ruiz & Pav.),
kiwicha (
Amaranthus caudatus L.),
ulluku (
Ullucus tuberosus Caldas),
racacha (
Arracacia xanthorrhiza Bancr.), and
tarwi (
Lupinus mutabilis Sweet), among others. Additionally, crops introduced from Europe such as onions (
Allium cepa L.), oats (
Avena sativa L.), Swiss chard (
Beta vulgaris L.), barley (
Hordeum vulgare L.), wheat (
Triticum aestivum L.), and broad beans (
Vicia fava L.), and, in pre-Hispanic times, from other parts of the Americas, such as maize (
Zea mays L.), have been integrated into their farming systems [
1,
2].
Puna ecosystems, found in the high Central Andes from northern Peru to northern Argentina, are vital reservoirs of food and medicinal resources. This extensive region boasts diverse vegetation, including dense highland grasslands, cushion plant communities, and distinctive tolar formations characterized by resinous shrubs.
Despite the harsh high-altitude environment, these ecosystems support an impressive array of approximately 1500 plant species. Many of these species hold significant value for both agriculture and traditional medicine [
3].
Regarding traditional Aymara medicine, several early works provide valuable insights:
Early Colonial Period (16th–17th centuries): Chroniclers like Pedro Cieza de León [
4] and Bernabé Cobo [
5,
6] wrote about Andean cultures, including some mentions of medicinal practices. While not specifically focused on the Aymara, these works offer some of the earliest written accounts potentially relevant to their traditions.
19th Century: One of the earliest studies with some Aymara focus was conducted by the Swiss-Peruvian naturalist Johann Jakob von Tschudi. His work,
Die Kechua-Sprache [
7], although primarily focused on the Quechua language, included some information about the Aymara people.
In the early 20th century: Valdizán and Maldonado’s book [
8] on popular medicine offers valuable insights. Enrique Oblitas Poblete’s
Plantas medicinales de Bolivia [
9] is often cited as one of the earliest comprehensive studies on Bolivian medicinal plants, including those used by the Aymara people.
From the mid-20th century onwards, more specialized ethnobotanical studies on Aymara medicinal traditions emerged, notably the works of Jan G. R. Elferink [
10] and Ina Rösing [
11,
12,
13,
14].
Traditional knowledge of medicinal plants in the Altiplano includes essential elements such as empirical classification systems, recognition of species’ habitats, and traditional techniques for harvesting, storing, preparing, and administering these plants to the population. In this context, itinerant healers and local markets play a crucial role in the transmission and preservation of this ancestral knowledge [
15,
16,
17].
The Aymara agricultural system adheres to strict traditional practices, including a distinctive rotation of cultivation and fallow periods. In the high-altitude Andean regions, land is managed in extended cycles that alternate between individual cultivation—where harvests are privately used—and collective rest periods of 3–10 years, primarily supporting pastoral activities [
18]. Productive cycles are closely aligned with climate patterns, with key agricultural tasks, such as sowing, being timed to these conditions.
Historically, Aymara communities have synchronized agricultural activities with Christian festivals. For instance, in Compi (Omasuyos province, La Paz), the agricultural year begins after the feast of Carmen, marked by bean sowing. This is followed by quinoa and oca planting around Santa Rosa, while potato planting occurs during several saint days, including San Mateo, San Calixto, and San Clemente [
19,
20].
Export-oriented agriculture has significantly impacted Aymara crop diversity. Rising international quinoa demand has reduced native agrobiodiversity, displacing traditional species like
olluco (
Ullucus tuberosus Caldas),
isaño (
Tropaeolum tuberosum Ruiz & Pav.),
kañiwa (
Chenopodium pallidicaule Aellen),
oca (
Oxalis tuberosa Molina), and
tarwi (
Lupinus mutabilis Sweet). This shift toward market-driven, intensive production models has decreased the agricultural diversity available to self-sufficient Aymara families, posing potential risks to food security and nutritional health [
21].
This study provides a comprehensive analysis of the medicinal significance of agrobiodiversity within Aymara communities of the Andean Altiplano, focusing on cultivated plants and agricultural weeds as vital resources for traditional healthcare. Specifically, our research aims to:
Analyze the diversity and therapeutic potential of medicinal plants from cultivated fields and agricultural margins, examining the complex relationship between crop systems and traditional medicine.
Investigate the roles of native and introduced species in Aymara ethnomedicinal practices, emphasizing the dynamic nature of these medicinal plant resources.
Examine gendered dimensions of knowledge and use, with a focus on the pivotal role of Aymara women in preserving and transmitting botanical healthcare practices.
Evaluate the broader implications of agrobiodiversity for community health, cultural heritage, and sustainable resource management in the Andean region.
By documenting the rich medicinal plant knowledge embedded within agricultural landscapes, we seek to contribute to the understanding of how traditional farming systems serve as crucial repositories of therapeutic knowledge and cultural resilience. Our research not only catalogues the medicinal uses of crops and weeds but also critically analyzes their significance in supporting community health and maintaining cultural continuity.
2. Materials and Methods
2.1. Study Area and Ethnographic Context
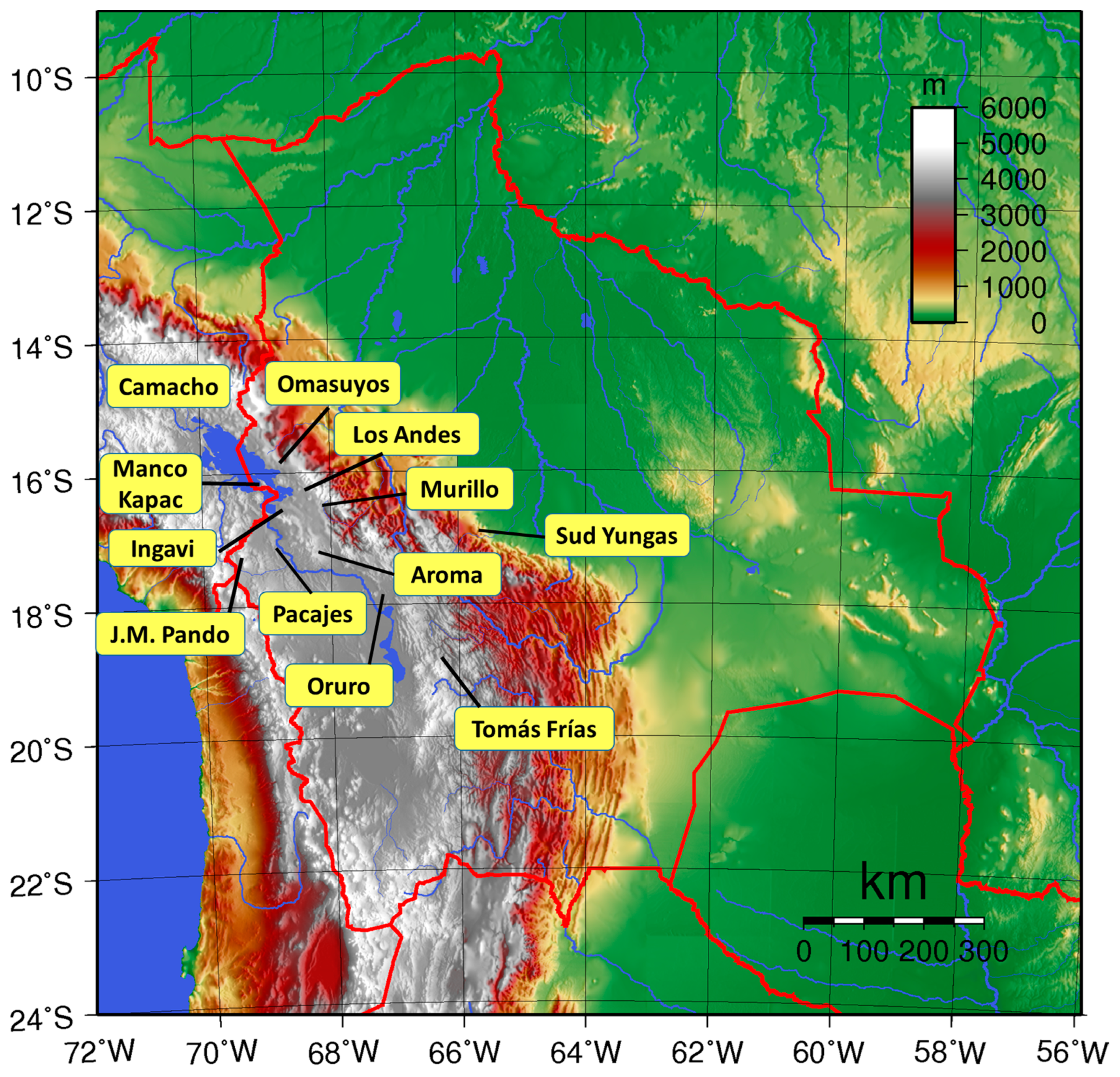
This study examines Aymara communities primarily located in Bolivia’s La Paz Department, with some participants from other Bolivian departments (
Table 1) and neighboring areas in Peru (
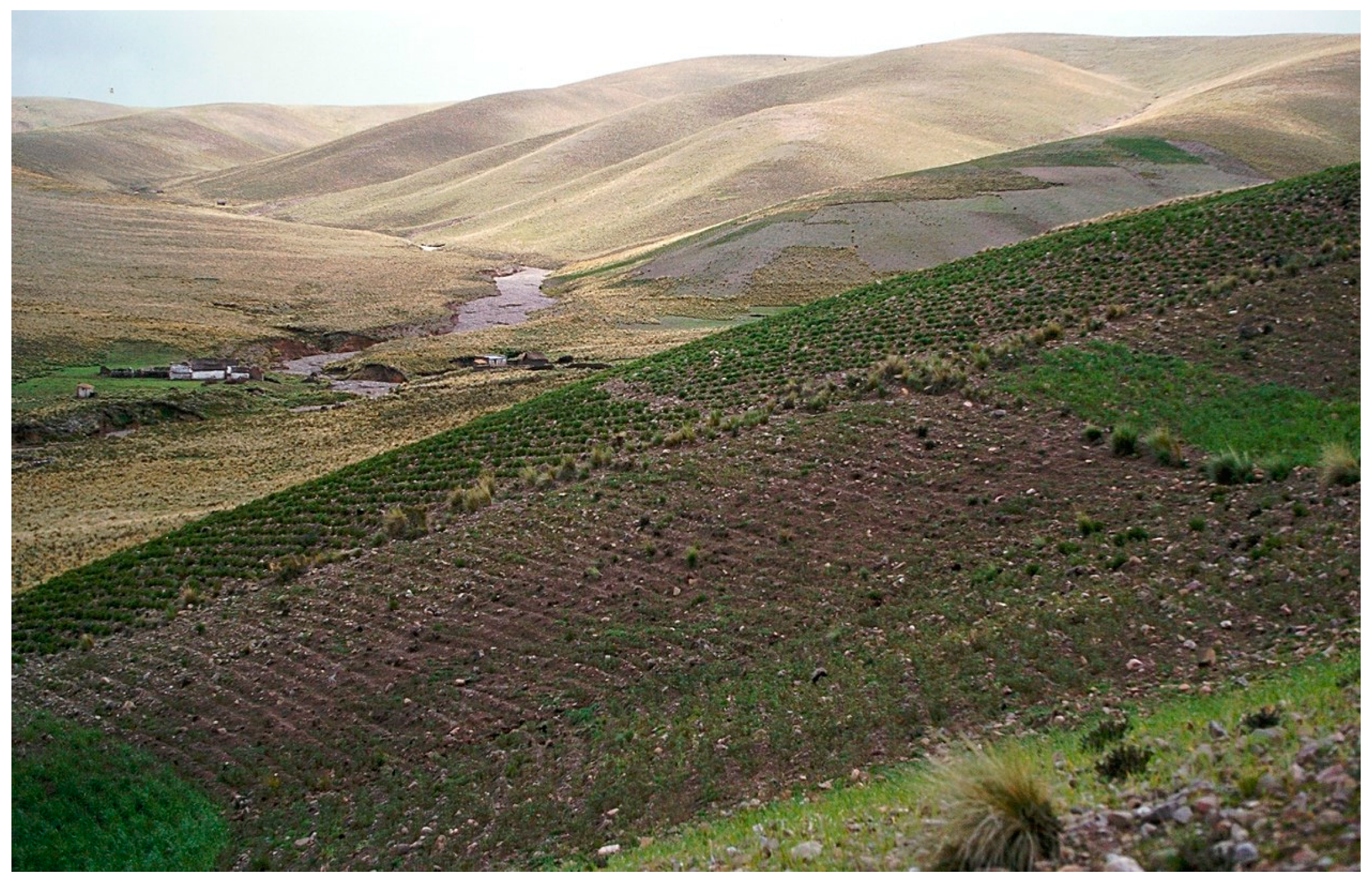
Figure 1). The La Paz Department lies in western Bolivia and features diverse geography. Its landscape ranges from high Andean peaks through middle-elevation valleys down to lowland plains. This varied terrain creates distinct patterns in climate, vegetation, and human settlement.
The high altitude of the region, often above 3000 m, shapes its cold, dry climate and affects both human life and Andean vegetation. While most people live in the cities of La Paz and El Alto, rural areas have smaller populations but preserve rich traditions and ancient knowledge. The economy differs between rural and urban zones: rural areas focus on small farming, livestock, and mining, while cities center on services, industry, and trade.
In summary, the Department of La Paz is a region rich in contrasts, where nature and history have shaped a unique landscape and culture. The altitude, climate, and distribution of natural resources have influenced the way of life of its inhabitants, creating a diversity of ecosystems and lifestyles.
2.2. Data Collection and Analysis
Our research used ethnographic methods including fieldwork, interviews, and a literature review. We conducted essentially semi-structured interviews with 228 informants (
Table 1) and integrated within communities during fieldwork from 2001 to 2015. All interviews followed verbal consent procedures aligned with the ISE Code of Ethics [
22]. Team member Simón Cocarico documented plants, ceremonies, markets, farms, and community events through photography.
Plant specimens were collected through a systematic process encompassing both informant-cited species and those documented through direct observation. The collection methodology covered diverse ecological zones, including community-managed agricultural plots, uncultivated areas, and abandoned fields, encompassing hundreds of hectares across the study region. Specimens were collected, pressed, and dried according to standard herbarium procedures.
Ethnobotanical documentation prioritized recording local nomenclature in situ with informants whenever possible, though some taxonomic identifications necessitated subsequent laboratory analysis. The collection protocol was expanded to include market specimens, with plant materials obtained from Altiplano markets being processed and preserved to document commercialized ethnobotanical resources.
Voucher specimens of the plants were deposited in the Herbario Nacional de Bolivia (LPB) at the Universidad Mayor de San Andrés in La Paz (Bolivia).
We recorded data in field notebooks and transferred them to Excel workbooks with separate sheets for informants, locations, medicinal plants, germplasm, agriculture, food, fuels, and forages. For this study, we focused on the informants, medicinal plants, and germplasm data. We standardized plant names using the
Catálogo de las Plantas Vasculares de Bolivia [
23] and POWO [
24] and classified health conditions using WHO’s ICD-11 framework [
25]. These standardized classifications helped generate our tables and figures.
Therapeutic applications were validated through participant observation conducted by a researcher who is both an investigator and a member of the Aymara community, supplemented by consultations with local experts when available. Medical conditions were documented in both Aymara and Spanish nomenclature and subsequently standardized according to WHO’s International Classification of Diseases (ICD-11) [
25]. The research methodology primarily employed participant observation, with non-participant observation conducted in select localities. Data collection focused on agricultural practices, genetic resources, medicinal and veterinary applications, and traditional food preparation and crafting techniques.
The study population comprised 228 informants selected primarily through purposive sampling targeting key knowledge holders (traditional healers, experienced farmers, and other specialists) rather than random sampling. The sampling strategy ensured demographic diversity: the gender distribution achieved approximate parity (50% male/female ratio), and the age range extended from 14 to 100 years, with a mean age of 48 years. The majority of informants engaged in either exclusively agricultural activities or combined farming with supplementary occupations such as construction and traditional crafts.
Field research was conducted systematically during ecologically and culturally significant periods, including distinct climatic seasons (spring and summer) and traditional festivities, particularly harvest celebrations. The methodology incorporated multiple observational approaches: direct observation of daily household activities documented relevant ethnobotanical practices and processes; observation of community-level activities encompassed collective work sessions, ceremonial gatherings, and religious celebrations where plants played significant roles; and systematic observation at weekly markets recorded plant material commerce and exchange patterns between Altiplano and Valley inhabitants.
The research intensity was substantial, with fieldwork conducted for at least three months annually during 2001–2003, followed by continuous engagement with Aymara communities thereafter. The cumulative fieldwork exceeded 100 site visits, including both extended stays and shorter expeditions. One researcher’s sustained immersion in and cultural affiliation with the Aymara community provided additional ethnographic depth through participatory observation and cultural understanding.
Geographically, the study centered on the provinces of Los Andes, Camacho, and Manco Kapac, with supplementary research conducted in Ingavi and Murillo provinces, and occasional investigations in adjacent regions. Primary research bases were established in Jacha Puni, Escoma, and Tihuanaco, facilitating comprehensive coverage of the study area.
3. Results
3.1. Demographic Profile of Informants
The study encompassed 228 informants, comprising 116 women (51%) and 112 men (49%). The female participants had a mean age of 40 years, with the eldest being 85, while the male participants had a mean age of 48 years, with the eldest being 100.
The interviews were conducted with participants willing to share their knowledge selected through both random and pre-arranged sampling. Initially, structured interviews were attempted, comprising primarily open-ended questions with few closed-ended ones. However, this approach was abandoned after approximately ten interviews due to several limitations: heterogeneity in participants’ knowledge levels, time constraints, and instances where informants possessed expertise beyond the scope of the predetermined questions. Additionally, structured interviews were only feasible with closely known participants, requiring significant time investment, which often led to respondent fatigue and decreased response quality.
Given these constraints, the methodology shifted to semi-structured and open interviews. Semi-structured interviews, guided by interview protocols, were conducted with pre-arranged participants who demonstrated sufficient rapport and reliability. The depth of questioning was adjusted according to the participant’s knowledge level and areas of expertise. Open interviews were conducted randomly with community members encountered during field visits, with the information gathered varying in depth according to participants’ knowledge and time availability.
Regarding the language of communication, 59% of the interviews were conducted in Aymara, 33% in both Aymara and Spanish, and 8% exclusively in Spanish. The occupational distribution of the informants was predominantly agricultural, with 128 participants identifying as farmers. Other occupations included market vendors (23), students (15), artisans (5), and livestock farmers (5). Most of them were from Bolivia and lived in small rural communities in La Paz Department (
Table 1).
3.2. Overview of Medicinal Plant Species and Habitats
This study identified 239 species and varieties of medicinal vascular plants utilized by Aymara communities (further details can be found in
Table S1). These species belonged to six classes of plant sensu GBIF [
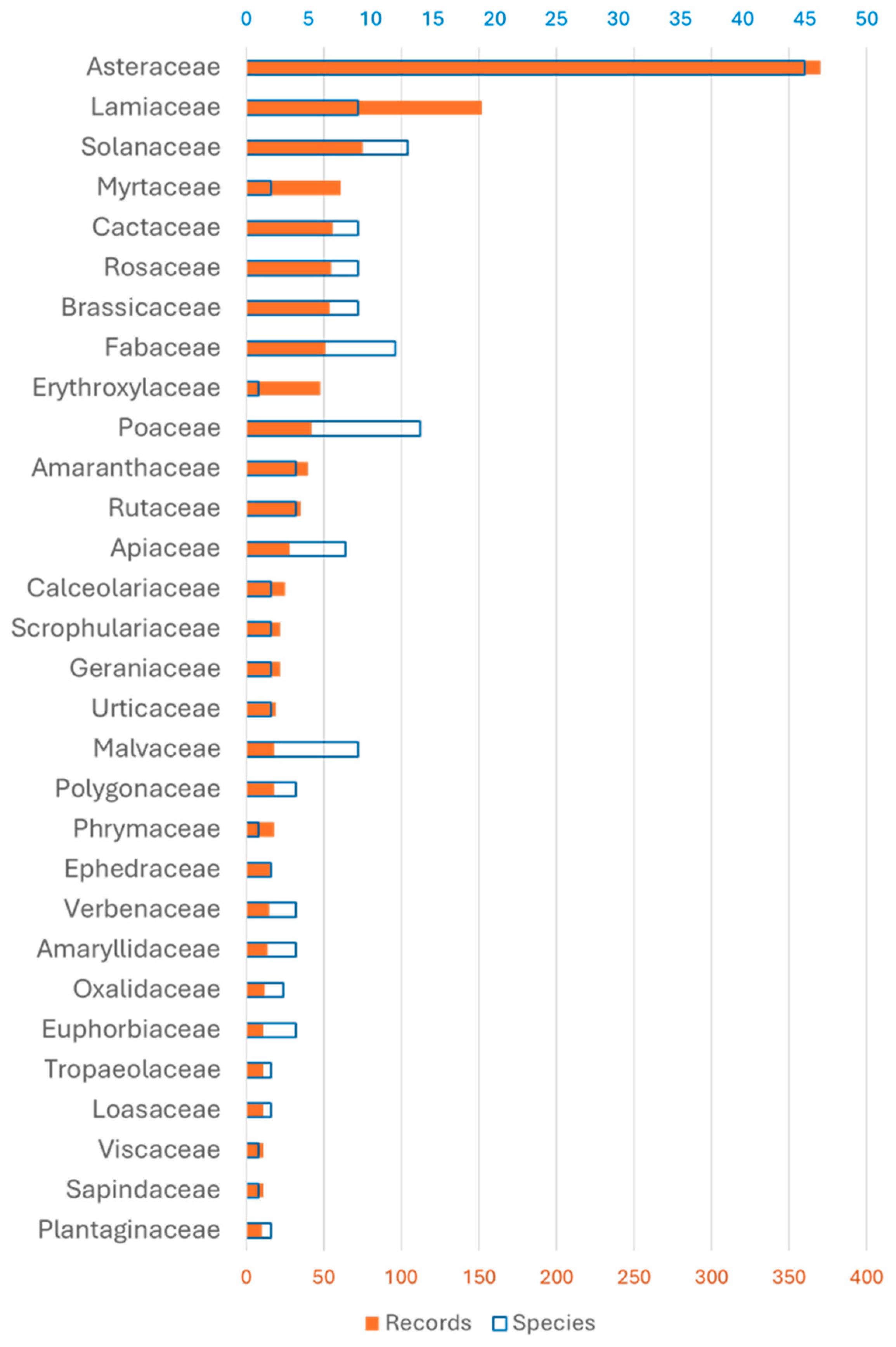
26]: Lycopodiopsida (1 species), also known as lycophytes (clubmosses and related plants); Polypodiopsida (2), also known as ferns; Pinopsida (2), also known as gymnosperms (conifers); Gnetopsida (2), also known as gymnosperms (gnetophytes); Liliopsida (27), also known as monocots; and Magnoliopsida (205), also known as eudicots and basal dicots. Among the 69 families of vascular plants, Asteraceae, Lamiaceae, and Solanaceae were predominant in terms of both species diversity and recorded uses (
Figure 2). Within the identified medicinal plant species, 92 taxa (38.8%) occurred in agricultural landscapes either as cultivated crops or associated ruderal species. This significant representation underscores the importance of horticultural systems as repositories of ethnomedicinal plant diversity within Bolivian Aymara communities. These agroecosystems thus served as crucial venues for both food production and the preservation of traditional medicinal resources, highlighting the multifunctional nature of local agricultural practices.
Other classes of organisms represented by one single species were Insecta (Dactylopius coccus Costa, 1829), Agaricomycetes (Ganoderma lucidum (Curtis) P.Karst.), Ulvophyceae (Rhizoclonium hieroglyphicum (C.Agardh) Kützing), and Lecanoromycetes (Thamnolia vermicularis (Sw.) Schaer.).
Analysis of plant life forms revealed the prevalence of perennial, annual, subshrub, and shrub species, which collectively accounted for over 67% of the species and 73% of records. Arboreal species, while present, exhibited comparatively lower frequencies in terms of records (
Table 2).
The ecological distribution of Aymara crop and weed medicinal species encompassed seven major biome types, as classified by Plants of the World Online (POWO) [
24] (
Table 3). The analysis revealed a notable concentration of medicinal plants in temperate, subtropical, and montane tropical biomes, which collectively accounted for the majority of both species diversity and usage records. The temperate biome exhibited the highest richness with 72 species and 517 documented uses, followed by the subtropical biome with 56 species and 338 records. The montane tropical biome ranked third in importance, hosting 40 species with 280 recorded uses.
A clear gradient was observed from these dominant biomes to the less represented ones. Seasonally dry tropical and wet tropical biomes occupied an intermediate position, containing 30 and 19 species, respectively. The subalpine or subarctic biome and desert or dry shrubland biome showed the lowest diversity of medicinal species, with 13 and 11 species, respectively, and correspondingly fewer usage records. This distribution pattern suggests a potential correlation between biome type and the prevalence of Aymara traditional medicinal plant knowledge and utilization which is related to the Puna as the primary habitat of the Aymara communities in the Bolivian altiplano.
3.3. Medicinal Plant Organs: Therapeutic Applications, Preparation Methods, and Routes of Administration
Regarding the utilization of different plant parts, leaves demonstrated clear predominance, being employed in 50% of cases. Flowers constituted the second most frequently used organ (10%), followed by fruits, shoots, bulbs, tubers, and other plant structures in smaller proportions.
The predominant methods for processing plant material for medicinal applications were infusion (28%), decoction (26%), maceration (20%), fresh preparation (9%), roasting (2%), and fumigation (1.5%), with various other methods comprising the remainder. In some instances, multiple processing techniques were applied sequentially, such as maceration followed by decoction.
The administration routes of processed medicinal plant preparations in Aymara communities demonstrated a clear predominance of oral administration (54.6% of recorded uses). Topical applications constituted the second most significant category, comprising external applications as plasters (17.0%) and direct topical treatments (13.6%). Therapeutic baths represented 9.9% of the documented applications, while inhalation therapy accounted for 2.8% of administration methods. Massage-based applications were less frequent, representing only 0.5% of the total recorded administration routes. This distribution pattern suggests a strong cultural preference for internal administration methods, with various forms of external applications collectively forming a substantial secondary category of therapeutic delivery systems.
The study has documented 260 pathologies in terms of emic categories, which have subsequently been analyzed and classified into broader nosological groups. Concerning administration methods, oral administration predominated, employed in over 40% of cases, followed by external application in the form of poultices, patches, ointments, or washes. A smaller percentage of species was consumed directly as medicinal food.
This comprehensive ethnobotanical investigation not only elucidated the rich pharmacopeia of Aymara communities but also underscored the intricate relationship between traditional ecological knowledge and local healthcare practices. The findings provide valuable insights into the biodiversity of medicinal plants in the region and their applications, potentially informing future horticultural and pharmacological research and conservation efforts.
3.4. Cultivated Plants in Traditional Aymara Medicine
Cultivated species play a pivotal role in Aymara traditional medicine, accounting for approximately 25% of both the total species diversity and recorded medicinal uses. It is noteworthy that an additional 19 native species were identified as occurring in both wild and cultivated states, as well as 17 ruderal weedy species, potentially increasing this proportion further.
The cultivated species, exclusively occurring in crop fields, with medicinal applications exhibited diverse life forms, notably annual and perennial. This distribution of life forms among cultivated medicinal species is summarized in
Table 4.
Medicinal and aromatic plants from agricultural fields were the most documented species in traditional pharmacopeia. These cultivated plants showed higher medicinal use than common wild species like
Clinopodium bolivianum (Benth.) Kuntze (syn.
Satureja boliviana (Benth.) Briq.), the weed
Sonchus oleraceus L., and purchased
Erythroxylum coca Lam. The cultivated plants included both native species and adapted foreign varieties (
Figure 3), showing how traditional farming systems successfully adopt useful plants regardless of their origin.
The significant incorporation of primarily food-producing species within the Aymara pharmacopeia (
Figure 3) exemplifies the sophisticated interface between traditional agricultural systems and ethnomedicine. This dual-purpose cultivation strategy, where food crops simultaneously serve therapeutic functions, demonstrates the optimization of agricultural resources within these communities. Furthermore, this agricultural-medicinal integration reflects a complex ethnobotanical knowledge system that encompasses both plant domestication processes and therapeutic applications, ensuring sustained access to essential phytomedicinal resources while maximizing land use efficiency.
The presence of 19 species found both wild and cultivated shows the connection between natural and managed landscapes in Aymara medicine. This overlap may signal ongoing plant domestication or the preservation of wild plants as local genetic resources.
The cultivated medicinal plants ranged from annual herbs to trees, showing the depth of Aymara plant knowledge and their skilled use of diverse plant types for healthcare.
The ethnobotanical study compiled over 2000 records on local germplasm knowledge, enabling a detailed categorization of plants according to their cultivation status and use: currently cultivated plants with known names and uses: 57% of records; plants cultivated until recently prior to the interview: 10% of records; plants considered lost by informants but with remembered names and uses: 33% of records.
Current data showed signs of cultural knowledge loss, as many plant species were remembered but no longer grown. The importance of cultivated species as genetic resources varied (
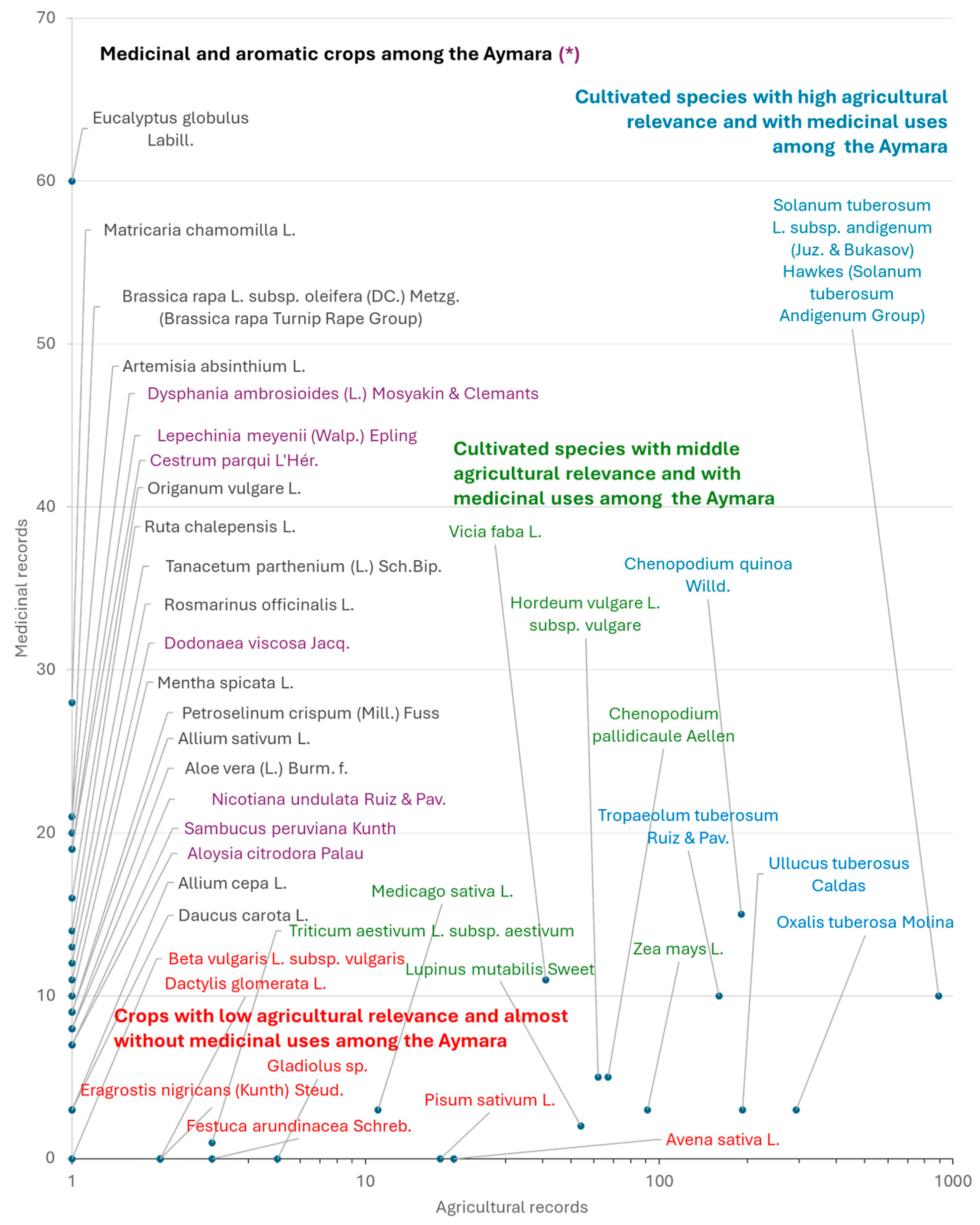
Figure 3). The Andean highlands contain valuable crop diversity, notably:
Solanum tuberosum L. and other
Solanum species (
papa or
ch’uqi): 42% of records but only 14 medicinal mentions (
Figure 4);
Oxalis tuberosa Molina (oca, apilla): 14% of records with 3 medicinal mentions;
Ullucus tuberosus Caldas (ulluku): 9% of records with 3 medicinal mentions;
Chenopodium quinoa Willd. (quinoa or jupha): 9% of records with 15 medicinal mentions;
Tropaeolum tuberosum Ruiz & Pav. (isañu): 8% of records with 7 medicinal mentions.
While these Andean crops are crucial genetic resources, their medicinal use is limited, except for quinoa. This suggests a need for more research on their traditional uses.
This pattern contrasts notably with other cultivated species which, although less prominent in agricultural terms, showed greater relevance in the medicinal domain. The introduced medicinal crops were notably
Eucalyptus globulus Labill. (
likaliktu) with 60 records of medicinal use,
Artemisia absinthium L. (
ajinju) with 30 records,
Matricaria chamomilla L. (
manzanilla) with 28 records,
Brassica rapa L. (
ñustasa) with 23 records, and
Tanacetum parthenium (L.) Sch.Bip. (
Santa mariya) (
Figure 5) with 13 records. It is particularly noteworthy that these latter medicinal crops, despite their significant presence in the medicinal repertoire, were not mentioned by informants as relevant agricultural resources.
This discrepancy between the agricultural importance and medicinal use of cultivated species suggests a complex interaction between traditional agricultural and medicinal knowledge systems. While some species like potato maintain a central position in local agrobiodiversity, others, possibly of more recent introduction or of lesser food importance, have acquired a prominent role in traditional pharmacopoeia. This phenomenon could reflect processes of adaptation and evolution in ethnomedicinal practices, possibly influenced by factors such as the introduction of new species, changes in morbidity patterns, or the influence of external medical systems. It also raises questions about the resilience and adaptability of ethnobotanical knowledge in the face of socioecological changes.
Among plants found both wild and cultivated (local domesticates), several species showed notable medicinal use:
Dysphania ambrosioides (L.) Mosyakin & Clemants (payqu): 20 medicinal uses;
Cestrum parqui L’Hér. (Andrés waylla) and Lepechinia meyenii (Walp.) Epling: 19 uses each;
Dodonaea viscosa Jacq.: 11 uses;
Nicotiana undulata Ruiz & Pav.: 8 uses;
Aloysia citrodora Palau (sitruna/cedrón) and Sambucus peruviana Kunth (qhula): 7 uses each;
Notably, informants rarely mentioned these plants’ agricultural importance despite their significant role in traditional medicine, revealing a distinct difference in how communities value these species.
The study’s findings underscore the dynamic nature of traditional ecological knowledge and highlight the need for integrated approaches in ethnobotanical research that consider both agricultural and medicinal dimensions of plant use. Furthermore, this research provides valuable insights into conservation strategies, emphasizing the importance of preserving not only plant genetic resources but also the associated traditional knowledge.
3.5. Weeds in Traditional Medicine
Traditional agriculture challenges conventional agronomic views of spontaneous field plants (“weeds”) by recognizing their nutritional and medicinal value. Our research among Aymara communities in the Bolivian Altiplano documented 128 medicinal applications across 17 such species (
Table 4), with relative importance shown in
Table 5. Most species arrived with European crops and livestock centuries ago. Our analysis shows that 67% of documented uses involve annual species, while 33% involve perennial plants.
Of particular interest is the extensive medicinal utilization of Sonchus oleraceus, colloquially known as common sow thistle. This species demonstrates a remarkably diverse range of therapeutic applications, addressing an array of health concerns. These applications span multiple medical categories, including but not limited to infectious and parasitic diseases; disorders of the digestive system; ailments of the genitourinary tract; dermatological conditions; substance use disorders and addictive behaviors; external causes of morbidity and mortality; febrile states of unknown or diverse etiology; mental, behavioral, and neurodevelopmental disorders; as well as various symptoms, signs, and clinical findings not elsewhere classified in standard medical taxonomies.
The extensive use of a single species for a wide range of medical conditions reflects the depth of ethnobotanical knowledge preserved within indigenous communities. This underscores the potential of these often-overlooked plants to contribute to modern pharmacological research and drug discovery. The contrast between their conventional agronomic classification as weeds and their significant role in traditional medicine offers a compelling avenue for interdisciplinary research, bridging agricultural practices, ethnobotany, and modern medical science.
3.6. Native vs. Introduced Species
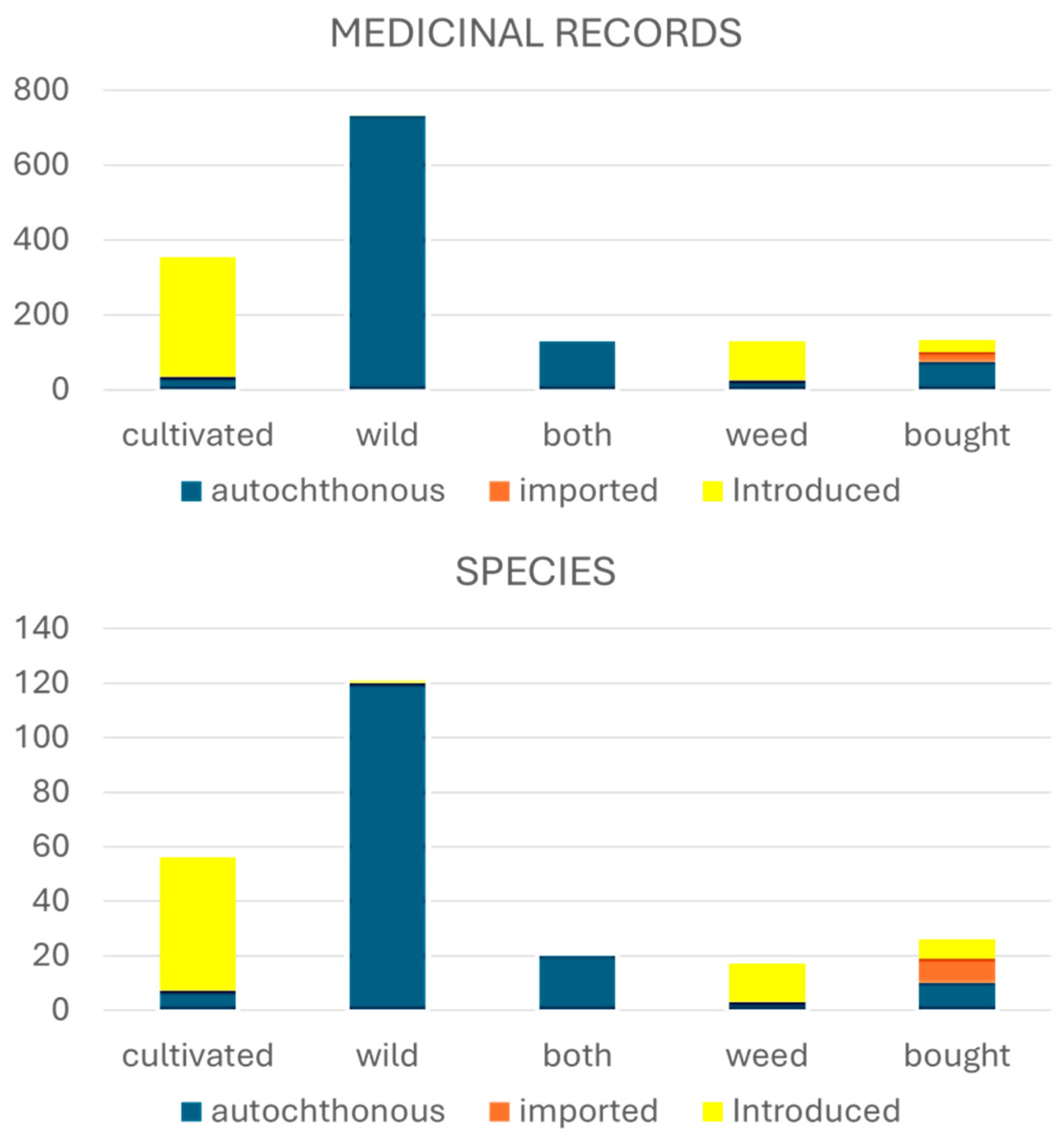
Approximately 67% of medicinal records and species are native, but the remaining 33% are introduced (30%) or in lesser proportion imported (3%). Most introduced species are crops or weeds (
Figure 6). The frequency of introduced species in this medicinal flora raises interesting questions about the adaptive capacity of traditional knowledge systems. It suggests a dynamic process of knowledge acquisition and integration, wherein communities have incorporated non-native plants into their pharmacopoeia over time. This adaptability not only demonstrates the resilience of traditional medicinal practices but also offers insights into the potential for cross-cultural exchange of botanical knowledge in historical and contemporary contexts.
A particularly noteworthy aspect of our research is the significant contribution of introduced species to the medicinal resources obtained from cultivated fields in the Bolivian Altiplano. These non-native species demonstrate a remarkable predominance, both in terms of taxonomic diversity and documented therapeutic applications. Regarding species composition, introduced plants constitute over 80% of the flora in cultivated areas and comprise the entirety (100%) of species categorized as weeds. This predominance becomes even more pronounced when examining records of medicinal use, where introduced species account for more than 90% of therapeutic applications in crops and 100% in weed species (
Figure 6).
Analysis of the native geographical distribution of the studied species, based on data from the Plants of the World Online (POWO) database [
24], reveals a biogeographic nucleus centered in the region spanning Peru to northwestern Argentina, including Bolivian territory (
Table 5). Interestingly, while the Mediterranean basin contribution to the Aymara medicinal flora exhibits relatively low species diversity, it stands out for its significant number of documented medicinal uses. This contrast between limited taxonomic representation and high therapeutic relevance may be attributed to the complex historical interactions between indigenous populations and Spanish colonizers, including clergy and monastic orders, over several centuries.
The pronounced representation of Mediterranean species in the medicinal repertoire of the Bolivian Altiplano, despite their lower taxonomic diversity, reveals complex patterns of ethnobotanical knowledge transmission and adaptation. This phenomenon exemplifies the profound cultural and scientific influence of Spanish colonization on local ethnomedical practices while simultaneously demonstrating the remarkable plasticity of local traditional knowledge systems.
The prevalence of non-indigenous medicinal crop species in both agricultural landscapes and therapeutic applications challenges conventional perspectives of traditional medicinal practices as static or isolated systems. Instead, it highlights an intricate process of knowledge exchange and assimilation, where indigenous healing traditions have become systematically interwoven with European botanical and medical concepts. This dynamic integration process has resulted in a sophisticated pharmacopeia that transcends simple categorizations of native versus introduced elements.
This cultural synthesis has profound implications for several domains of scientific inquiry. From an ethnobotanical standpoint, it highlights the remarkable adaptability of traditional knowledge systems. These systems demonstrate the capacity to effectively integrate and utilize introduced plant species while upholding core cultural principles.
Understanding contemporary medicinal plant use patterns necessitates a nuanced analytical framework that considers the interplay of historical, cultural, and social dynamics.
The findings also have substantial implications for conservation biology and sustainable resource management in the Andean region. The representation of introduced species in therapeutic practices raises important questions about the relative contribution of native versus non-native flora to ecosystem services, particularly those related to human health and wellbeing. This understanding is crucial for developing comprehensive conservation strategies that acknowledge both ecological and cultural dimensions of plant resource management.
Moreover, this cultural-ecological synthesis offers valuable insights for contemporary applications. The demonstrated capacity for cross-cultural integration of medicinal knowledge suggests potential pathways for developing synergistic approaches in modern ethnopharmacological research and healthcare systems. This has relevance in the context of increasing globalization and environmental change, where adaptive and integrative approaches to health resource management are becoming increasingly crucial.
This complex interplay between traditional knowledge, introduced species, and adaptive practices in the Bolivian Altiplano provides a compelling case study of ethnobotanical knowledge evolution. It underscores the importance of interdisciplinary approaches that integrate traditional knowledge systems, ecological research, and conservation planning to ensure sustainable management of medicinal plant resources while preserving cultural heritage in an era of rapid global change.
3.7. Relevance of Crops and Weeds as Specific Medicinal Resources
During our research, we documented over 380 distinct pathologies in emic terms, which, after a process of consolidation and elimination of synonymies, were reduced to approximately 260 discrete nosological entities classified into 28 major groups following WHO’s ICD-11 guidelines. The relevance of these pathologies, in terms of their frequency of occurrence, presents marked heterogeneity.
Table 6 provides a synthesis of those conditions that were recorded 20 or more times, with digestive disorders, fractures resulting from traumatic events, and cholera (although it is pertinent to note that this latter category may encompass other infectious diseases with similar symptomatology) emerging as particularly prominent.
With the aim of systematizing the identified pathologies and graphically representing the relative importance of various medicinal resources, we employed the taxonomy proposed by the International Classification of Diseases in its eleventh revision (ICD-11) by the World Health Organization (WHO) [
25]. This methodological approach allowed us to ascertain, as illustrated in
Figure 7, that plant species originating from cultivated fields constituted a predominant source of therapeutic resources, providing more than 40% of the remedies in the most frequent nosological categories.
This finding underscores the significant contribution of flora associated with agroecosystems to the ethnopharmacological repertoire of the studied region. The preponderance of cultivated and adventitious species in the treatment of the most common pathologies, such as cough and fever, suggests an intricate relationship between traditional agricultural practices and local medical knowledge systems. Furthermore, this phenomenon raises questions about the resilience and adaptability of ethnomedicinal systems in the face of transformations in the agricultural landscape and the introduction of new plant species over time.
The utilization of the ICD-11 framework for categorizing local health conditions not only facilitates comparative analyses with other ethnobotanical studies but also bridges the gap between traditional medical knowledge and contemporary biomedical classifications. This approach enhances the potential for integrating traditional healing practices with modern healthcare systems, potentially leading to more culturally sensitive and effective health interventions in the region.
Moreover, the substantial contribution of cultivated and weedy species to the local pharmacopoeia highlights the often-overlooked medicinal value of plants commonly perceived as primarily agricultural or even undesirable weeds. This observation challenges conventional distinctions between food and medicine in traditional contexts and underscores the multifunctional nature of many plant species in indigenous agroecosystems. Such findings have important implications for agrobiodiversity conservation strategies and the development of sustainable agricultural practices that maintain both food security and traditional medicinal resources.
3.8. The Role of Aymara Women in the Production and Use of Food and Medicinal Plants
Significantly, while our research indicates comparable numbers of species and medicinal use records between male and female informants, substantial gender-based differences emerged in the knowledge and utilization patterns of cultivated species and ruderal plants (
Table 7). This gender differentiation in ethnobotanical knowledge reflects distinct roles and expertise within the traditional agricultural and medicinal system.
The data present compelling evidence for gender-differentiated knowledge patterns in traditional medicinal plant use, with particularly notable female dominance in cultivated species knowledge. This is demonstrated through multiple quantitative indicators.
In terms of cultivated species, women demonstrated substantially higher engagement, accounting for 58% of all records compared to men’s 42%. More striking is the species-level analysis, where women’s knowledge encompassed 89% of all cultivated medicinal species (50 species), while men’s knowledge extended to only 46% (26 species). This marked disparity suggests women’s deeper involvement in and familiarity with home gardens and agricultural spaces where medicinal plants are cultivated.
The pattern extended to weedy species, which are often found in agricultural contexts, where women again showed higher engagement, with 55% of records and knowledge of 81% of species, compared to men’s 45% of records and 50% of species. Similarly, for purchased medicinal plants, women demonstrated greater knowledge (92% of species versus men’s 15%).
Interestingly, the gender distribution became more balanced or slightly reversed for wild species, where men showed marginally higher engagement (52% of records versus women’s 48%). However, women still maintained broader species knowledge even in this category, recognizing 76% of wild species compared to men’s 50%.
This comprehensive analysis suggests that women’s role is particularly crucial in the management and knowledge of cultivated medicinal plants, likely reflecting their traditional responsibilities in home garden maintenance and domestic healthcare. The data indicate that women not only maintain more frequent interaction with cultivated medicinal species but also possess more extensive knowledge of their varieties and applications.
Statistical evidence strongly supports women’s position as primary knowledge holders in the domain of cultivated medicinal plants while also demonstrating their substantial expertise across all categories of medicinal plant resources.
Analysis of gender-differentiated agricultural knowledge reveals distinct patterns in crop management responsibilities. Female respondents demonstrated significantly higher levels of horticultural expertise for several species, including Allium cepa L. (onions), Beta vulgaris L. (chards), Daucus carota L. (carrots), Gladiolus sp., and Zea mays L. (corn). This pattern strongly suggests women’s predominant role in maintaining household gardens and managing domestic food production spaces.
For Andean tuber crops—specifically Oxalis tuberosa Molina (oca), Tropaeolum tuberosum Ruiz (mashua), and Ullucus tuberosus Caldas (ulluco)—the knowledge distribution appeared relatively balanced between genders, indicating shared cultivation responsibilities. In contrast, pastoral agriculture, particularly the management of cultivated meadow grasses, emerged as an exclusively male domain according to the collected data.
Regarding major staple crops such as Chenopodium quinoa (quinoa) and Solanum tuberosum (potato), while both genders demonstrated substantial agricultural knowledge, male respondents provided a higher proportion of the documented information. This gender-based variation in agricultural expertise reflects complex social dynamics in traditional farming systems and suggests distinct but complementary roles in agricultural management.
5. Conclusions
This research provides a comprehensive analysis of the medicinal significance of agrobiodiversity in Aymara communities of the Bolivian Andean Altiplano. The findings highlight the essential roles of cultivated plants, agricultural weeds, and wild-gathered flora in traditional healthcare practices, with household gardens serving as key reservoirs of both introduced and locally domesticated species. Women play a pivotal role in these systems, holding knowledge of 81% (193) of medicinal plant species compared to 47% (113) for men. Record frequencies also underscore women’s greater engagement with medicinal plants, particularly cultivated species (89%, or 50 species, versus men’s 46%, or 26 species). This gendered knowledge disparity extends to the commercialization of medicinal plants, where women are familiar with 92% of purchased species compared to men’s 15%.
Interestingly, major staple crops such as Chenopodium quinoa and Solanum tuberosum contribute minimally to medicinal use, with greater emphasis placed on specifically cultivated medicinal plants, ruderal species, and wild-gathered flora. This finding illustrates the dynamic relationship between agricultural diversity and ethnomedicinal knowledge, reflecting both ecological adaptations and the resilience of Aymara traditional knowledge systems amid historical and ongoing ecological and sociocultural changes.
The integration of native and introduced plant species into ethnomedicinal practices reveals that introduced species dominate therapeutic applications of crop plants and account for all weed species used medicinally. This suggests a capacity for innovation within traditional knowledge systems in response to changing environments and sociopolitical contexts.
Future research should focus on (1) the gendered dimensions of medicinal plant knowledge, particularly the role of Aymara women in sustaining and transmitting ethnobotanical practices; (2) the historical pathways of plant introductions and their incorporation into local pharmacopoeias; (3) conservation strategies that integrate both biological and cultural dimensions of medicinal plant resources; (4) applications of this knowledge to contemporary drug discovery efforts; and (5) mechanisms that enable traditional systems to adapt to environmental and social changes while maintaining therapeutic efficacy.
These findings enhance our understanding of the complexity and adaptability of traditional medical systems, emphasizing the need for their preservation in rapidly changing socioecological contexts. They also underscore the critical importance of gender-specific knowledge in maintaining local therapeutic resources and healthcare practices.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}