
Impact of Modelling Surface Roughness in an Arterial Stenosis



Abstract
:1. Introduction
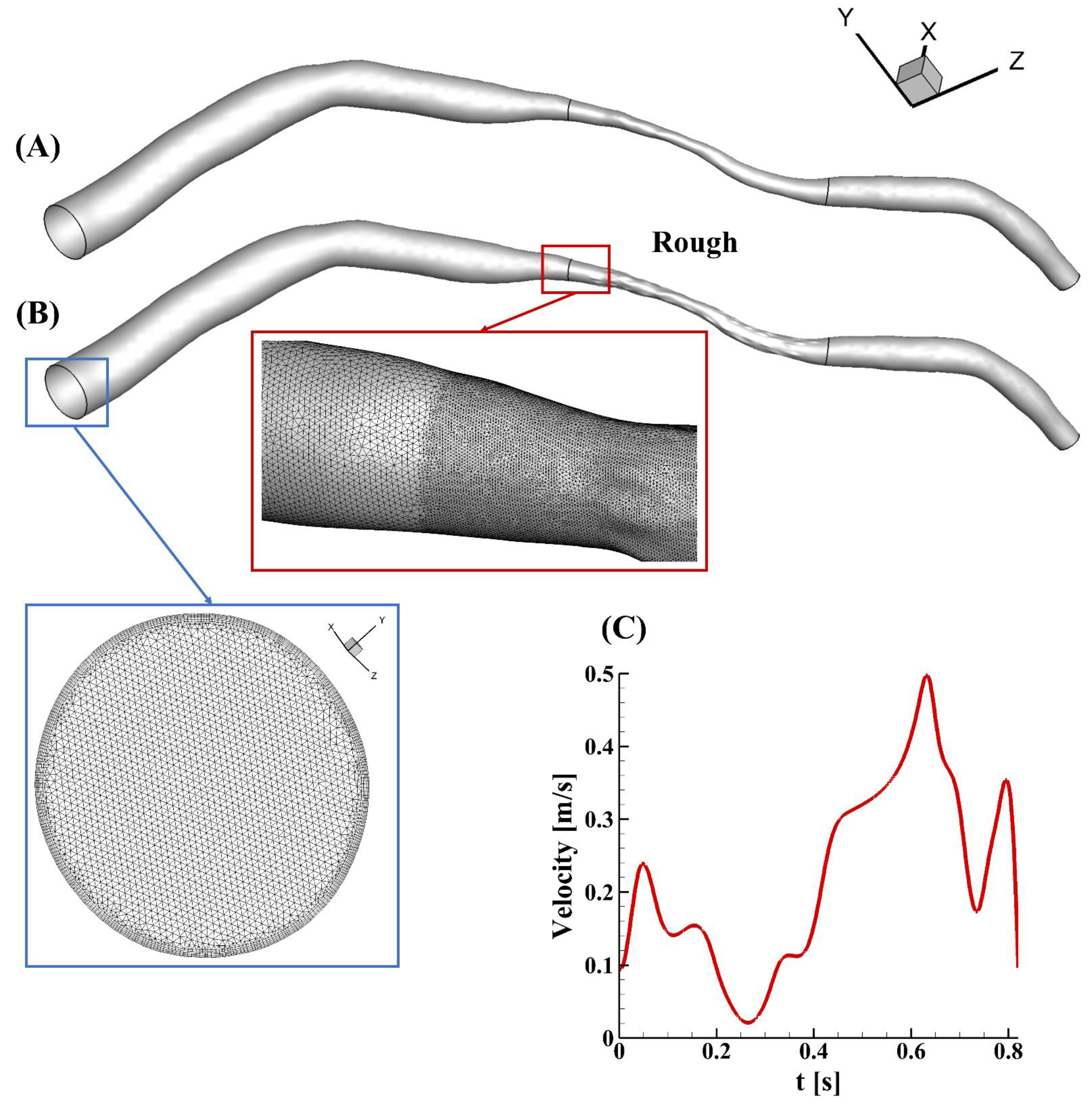
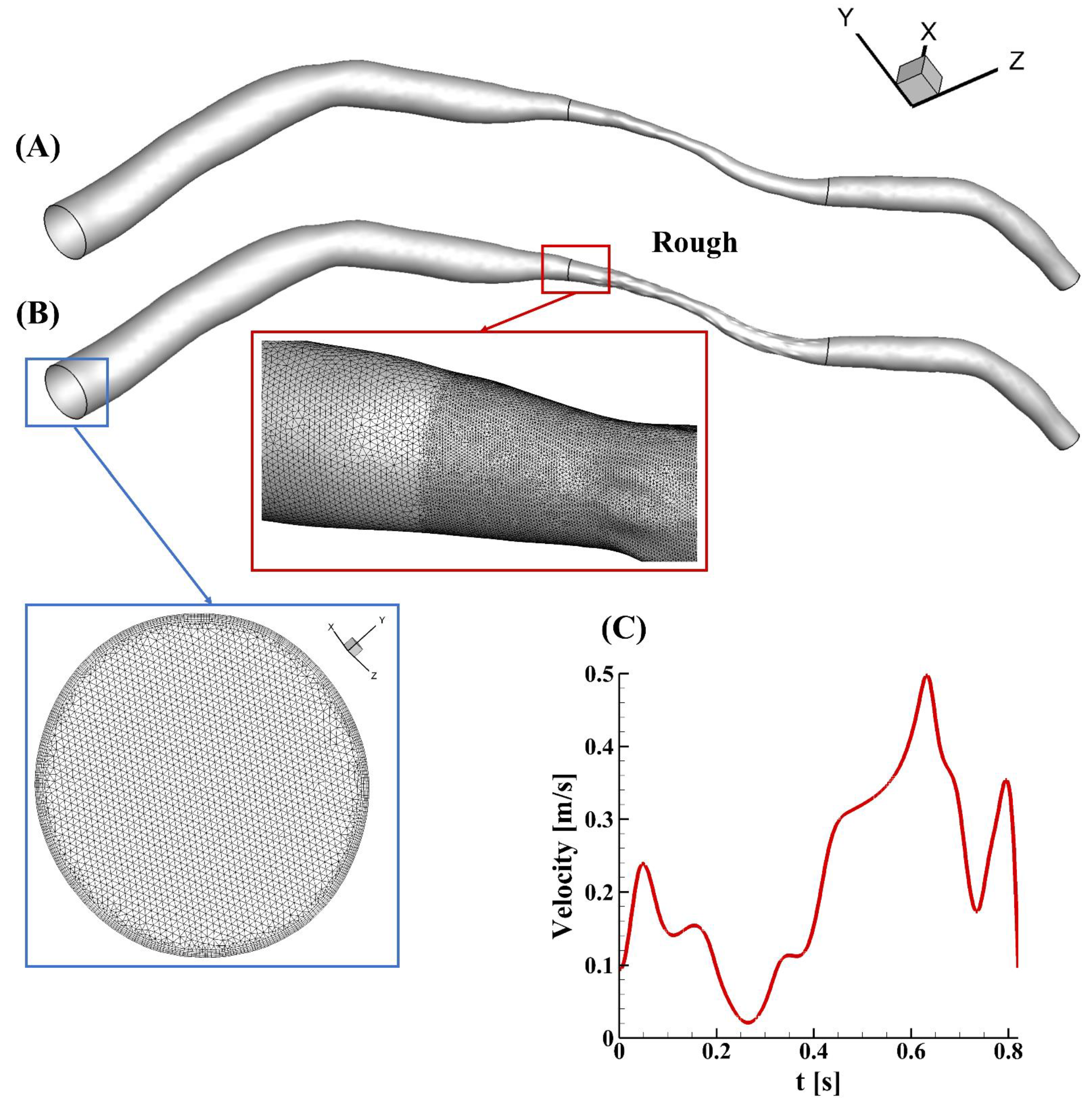
2. Materials and Methods
3. Results and Discussion
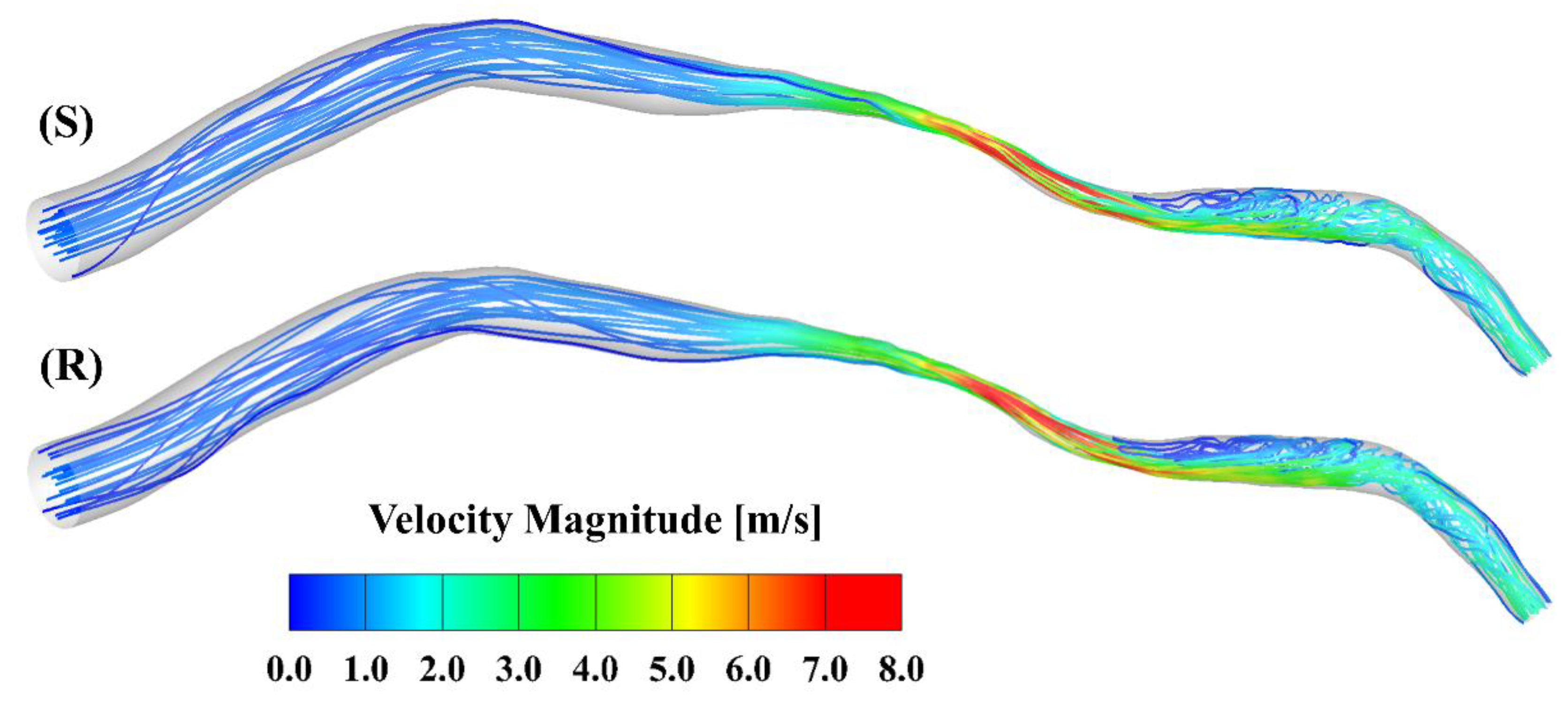
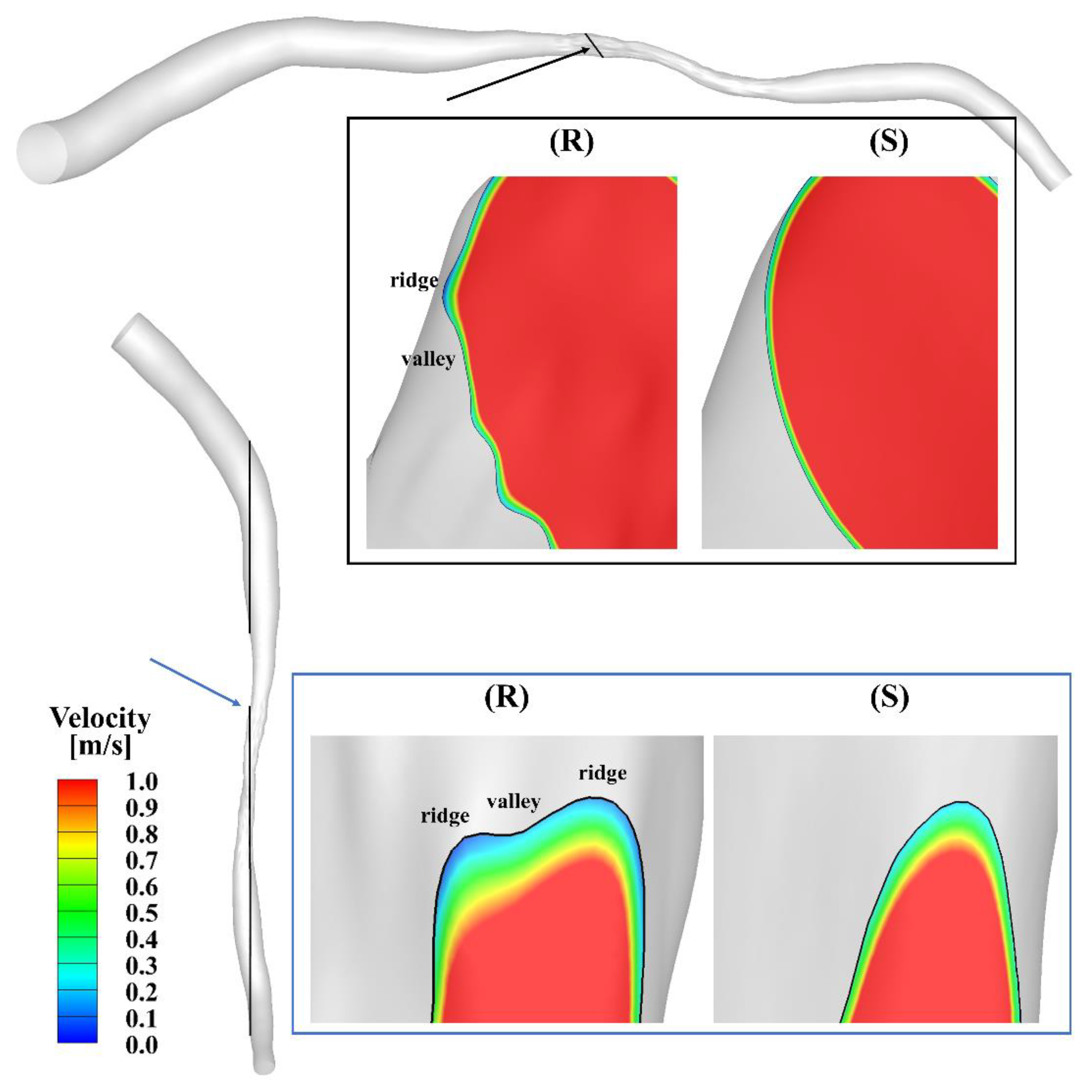
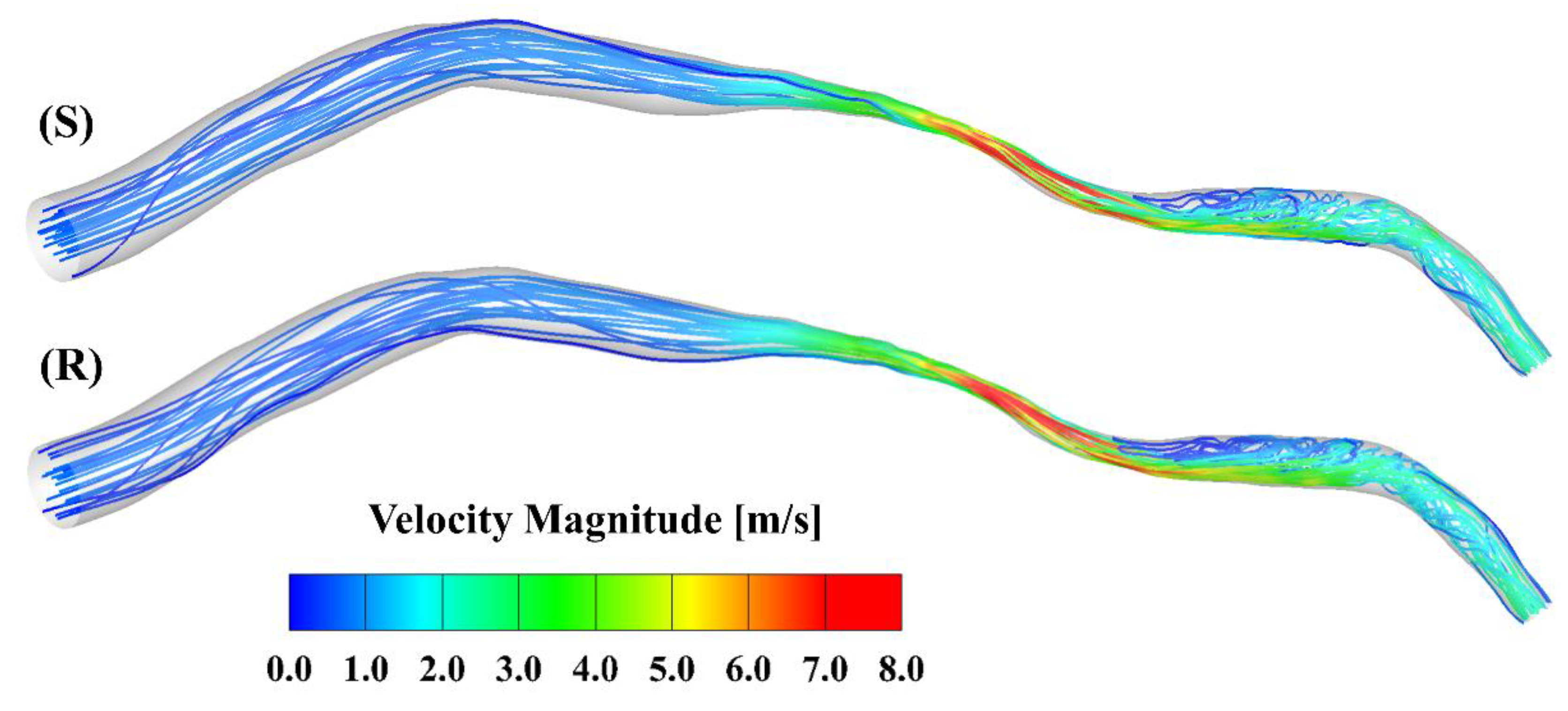
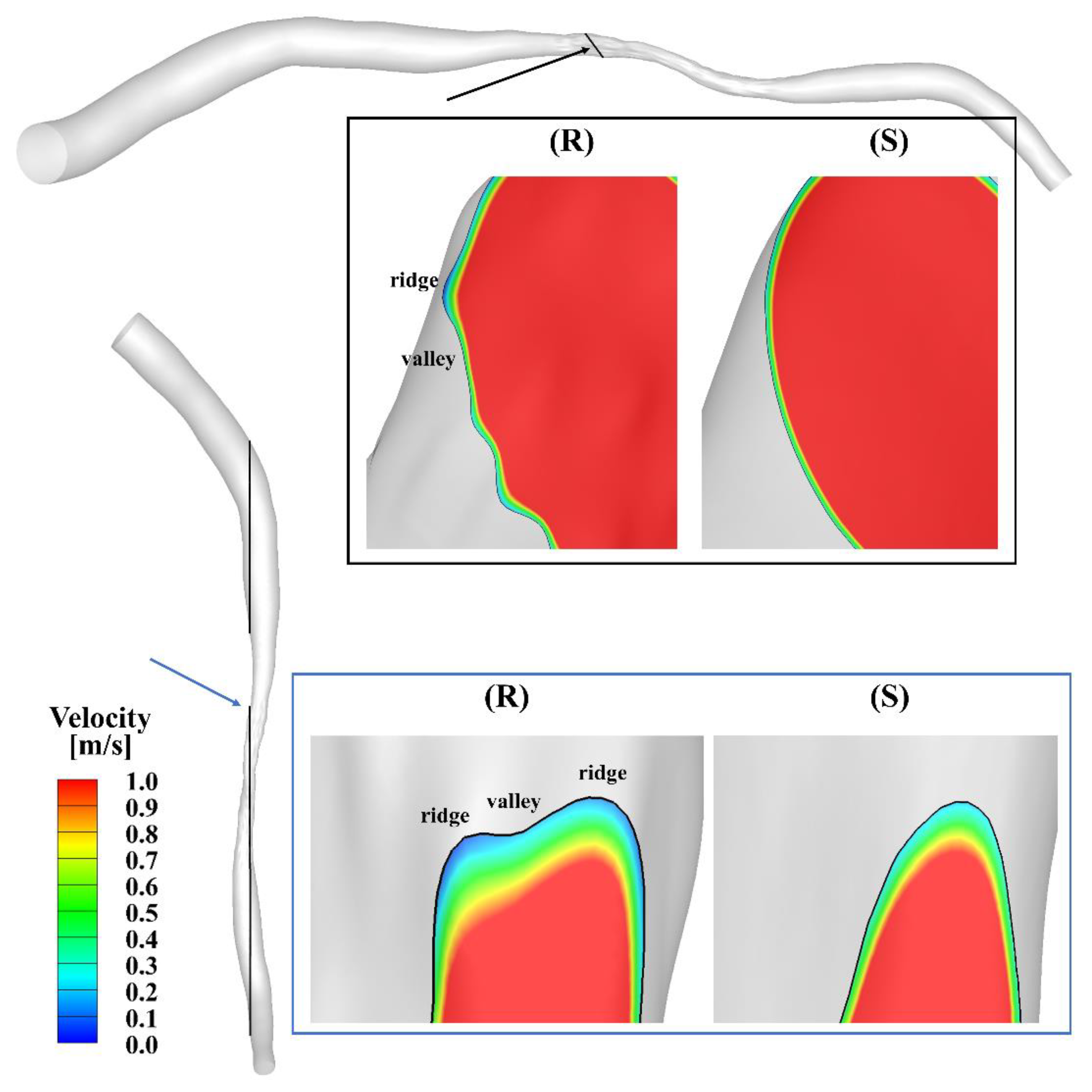
3.1. Velocity
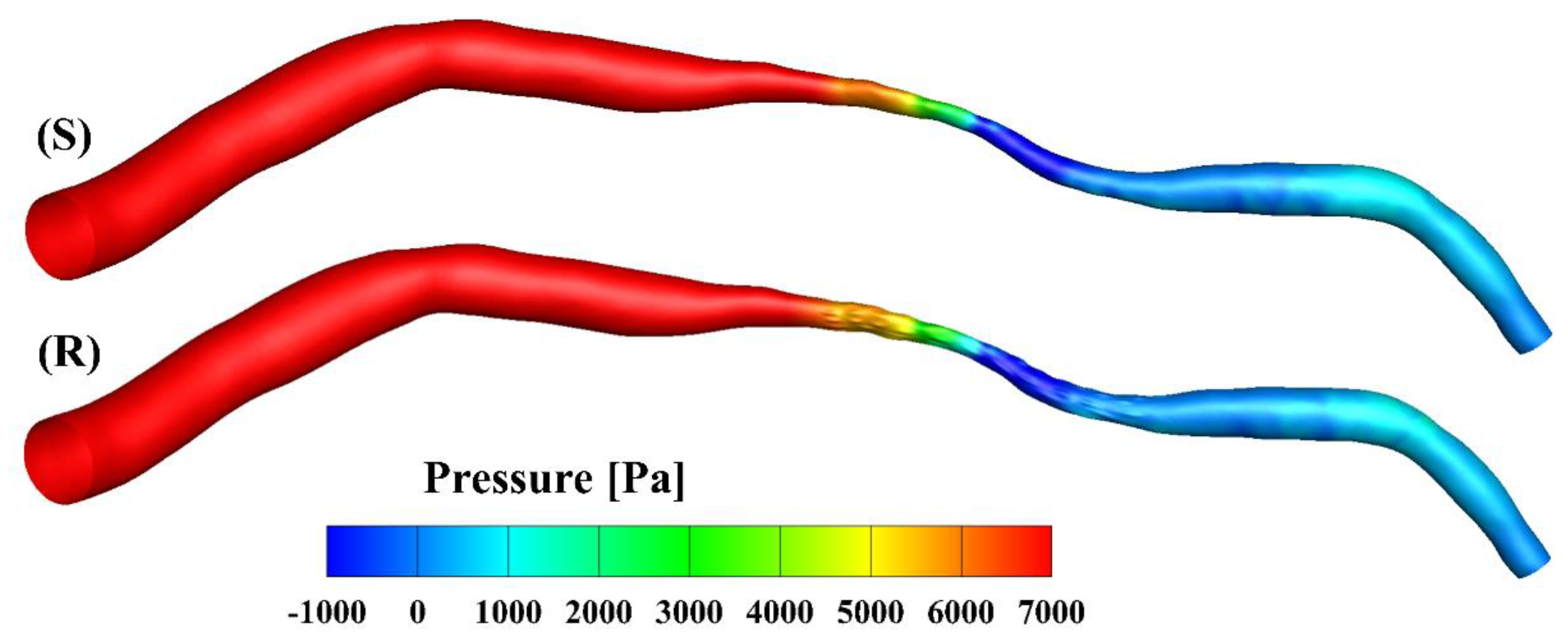
3.2. Pressure
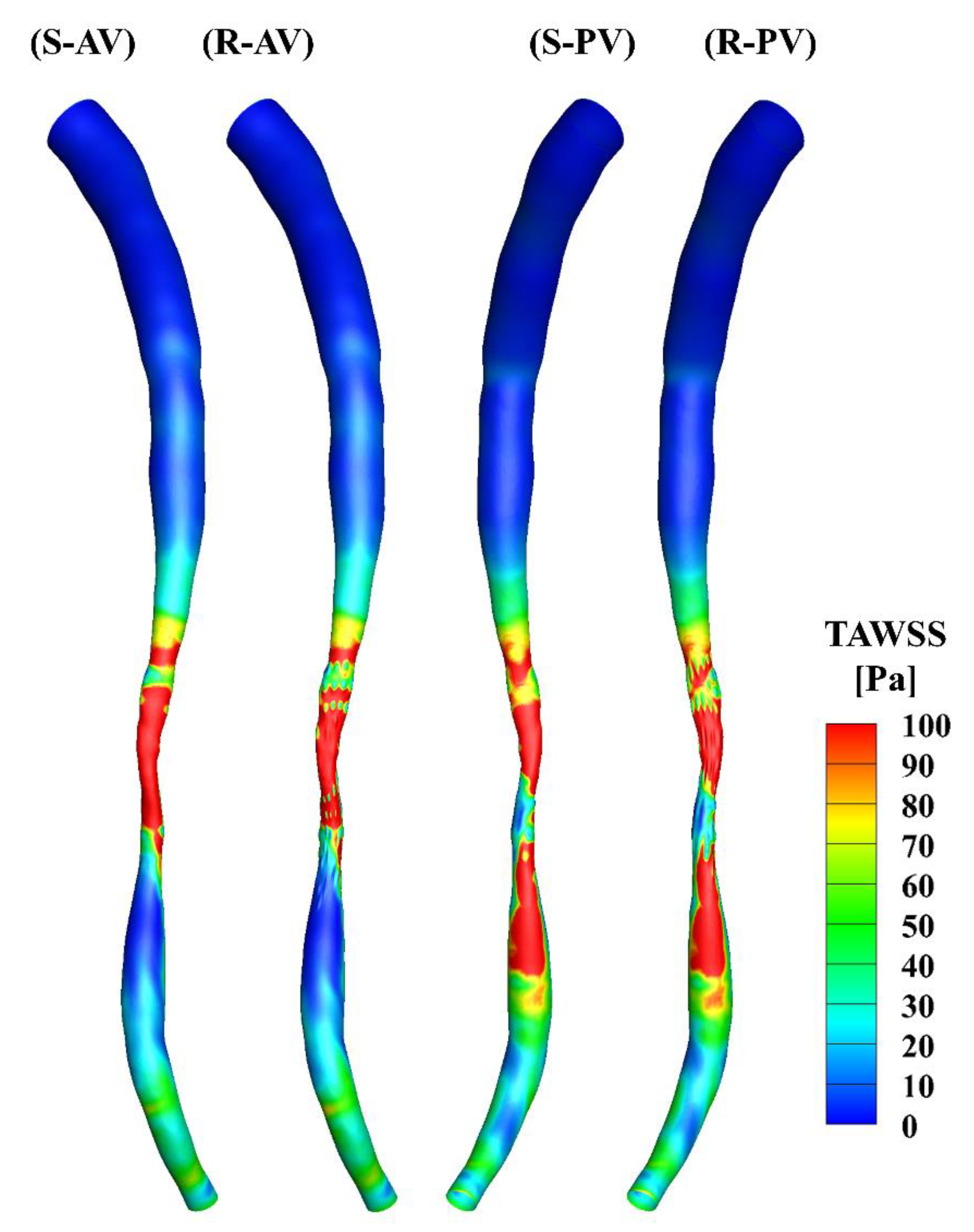
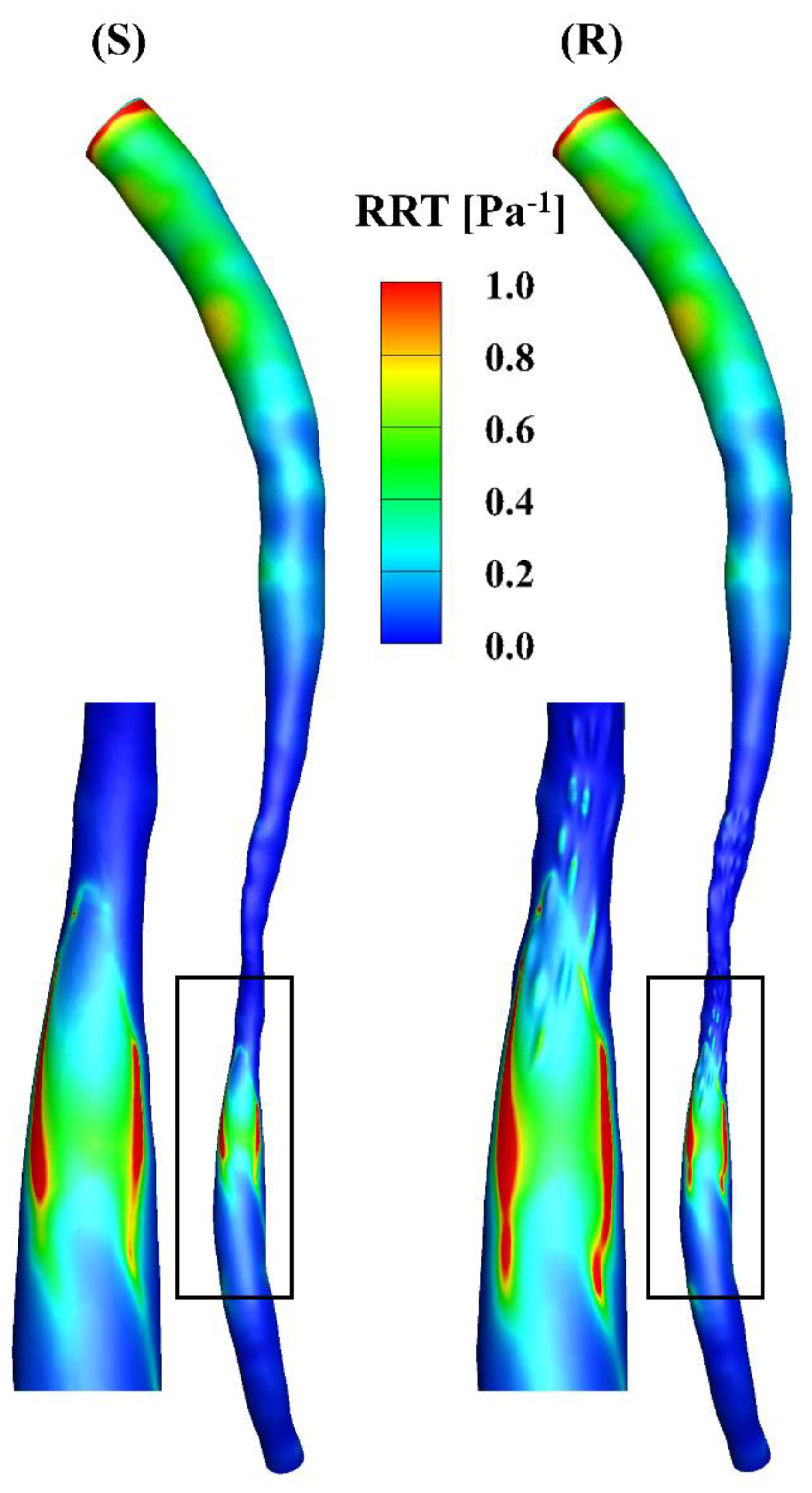
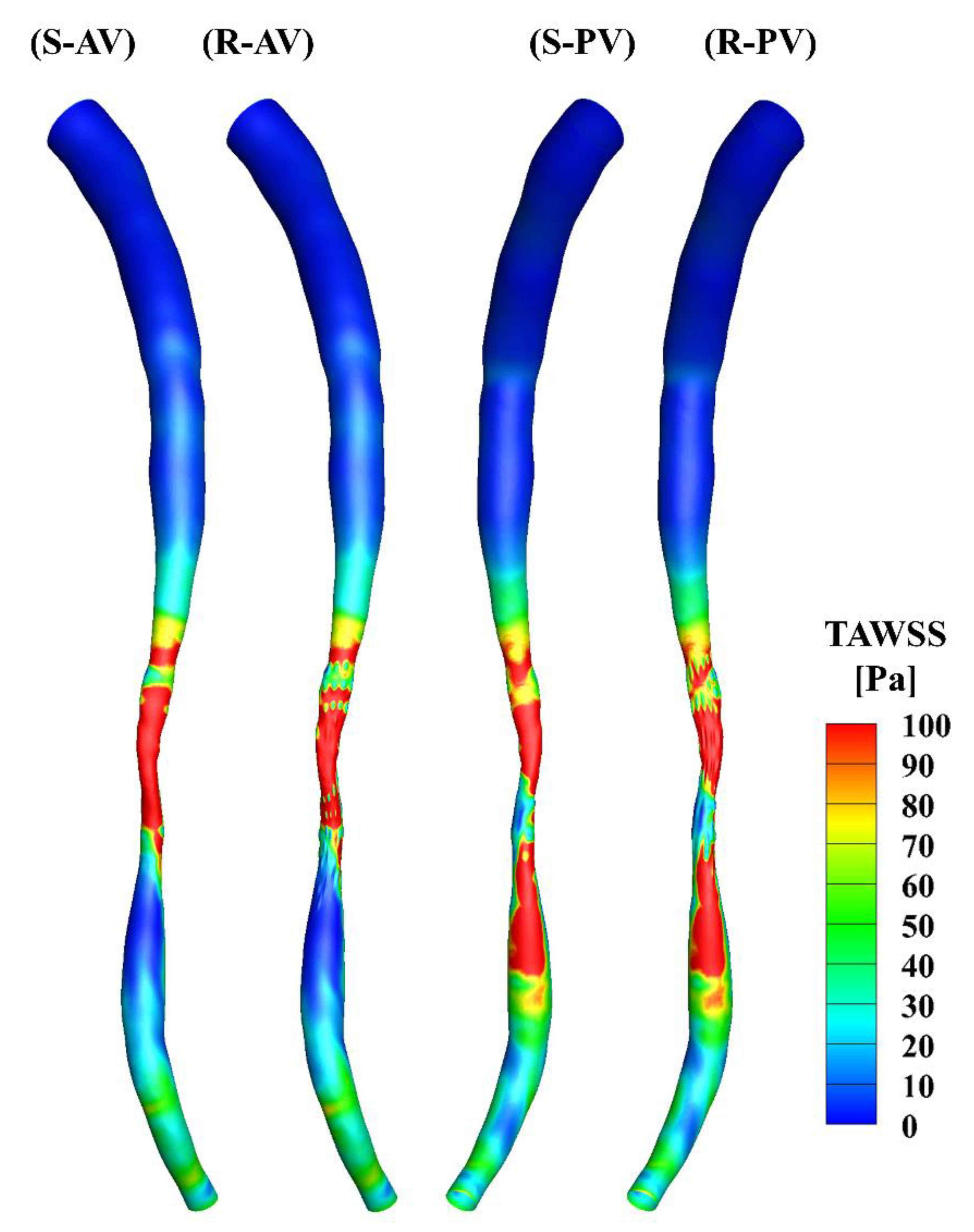
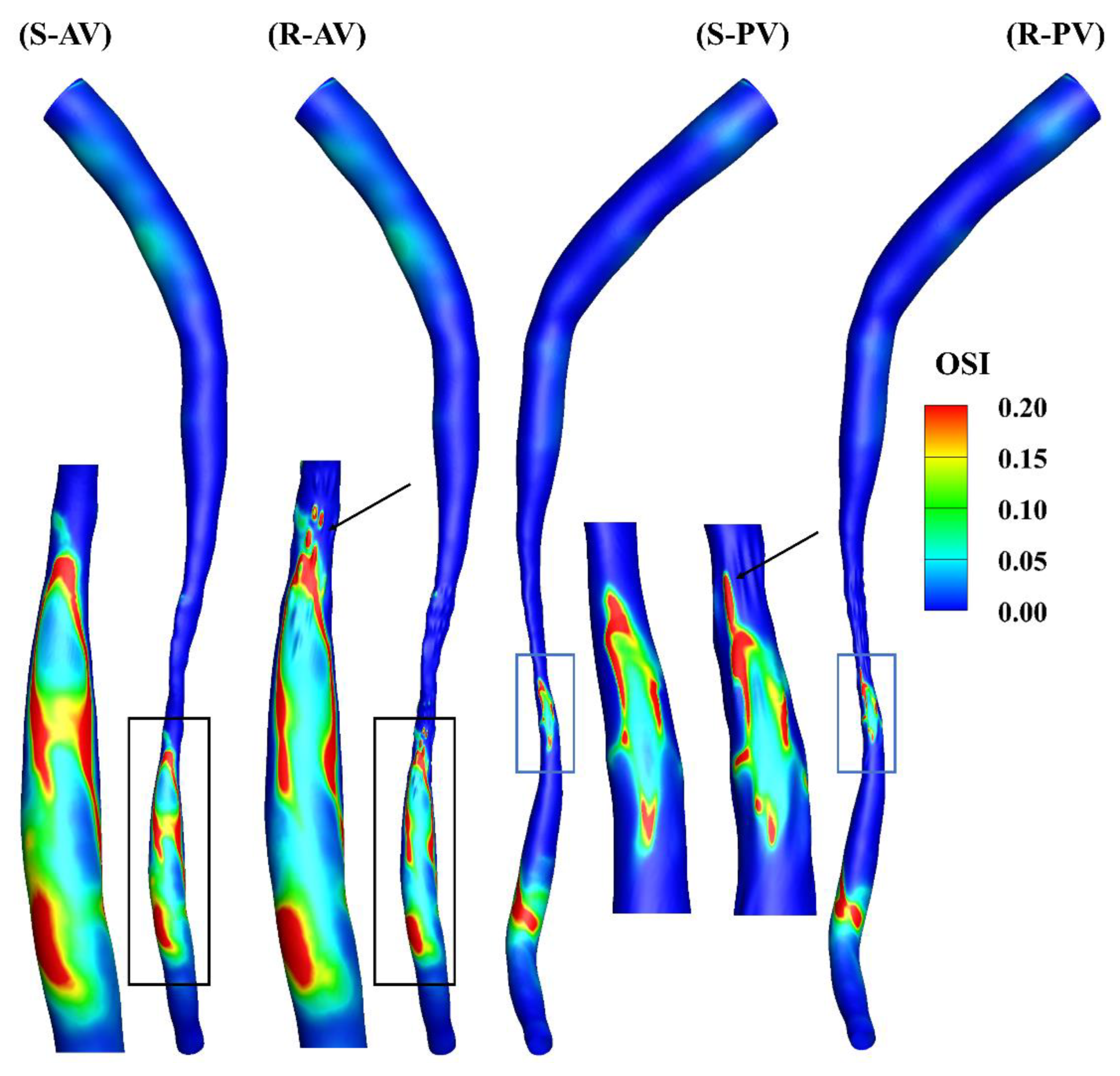
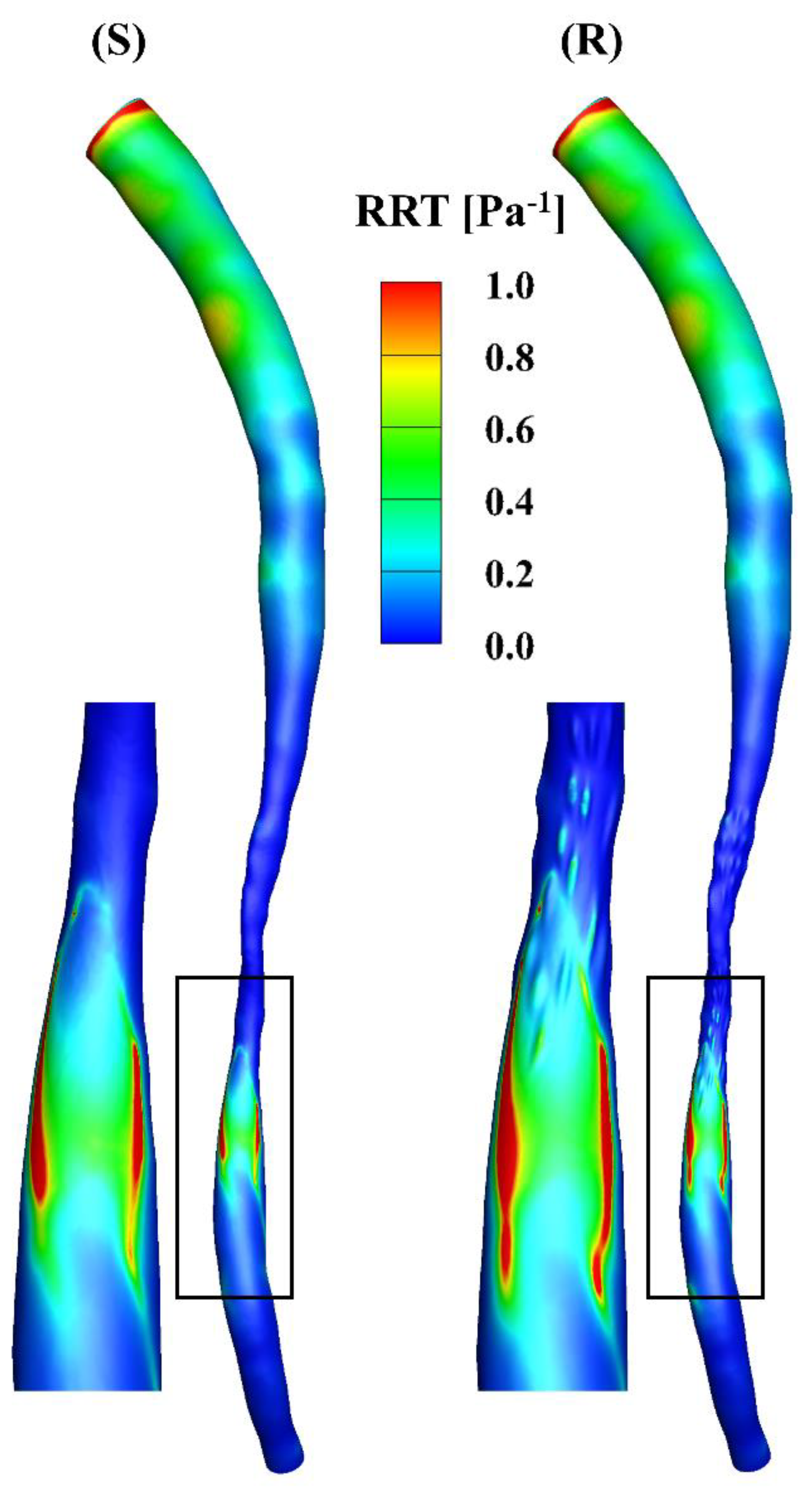
3.3. WSS
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ezzati, M.; Obermeyer, Z.; Tzoulaki, I.; Mayosi, B.M.; Elliott, P.; Leon, D.A. Contributions of risk factors and medical care to cardiovascular mortality trends. Nat. Rev. Cardiol. 2015, 12, 508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deplano, V.; Siouffi, M. Experimental and numerical study of pulsatile flows through stenosis: Wall shear stress analysis. J. Biomech. 1999, 32, 1081–1090. [Google Scholar] [CrossRef]
- Van Wyk, S.; Wittberg, L.P.; Fuchs, L. Wall shear stress variations and unsteadiness of pulsatile blood-like flows in 90-degree bifurcations. Comput. Biol. Med. 2013, 43, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Eckmann, D.M.; Grotberg, J.B. Experiments on transition to turbulence in oscillatory pipe flow. J. Fluid Mech. 1991, 222, 329–350. [Google Scholar] [CrossRef]
- Bhaganagar, K. Direct numerical simulation of flow in stenotic channel to understand the effect of stenotic morphology on turbulence. J. Turbul. 2009, 10, N41. [Google Scholar] [CrossRef]
- Marques, P.F.; Oliveira, M.E.C.; Franca, A.S.; Pinotti, M. Modeling and simulation of pulsatile blood flow with a physiologic wave pattern. Artif. Organs 2003, 27, 478–485. [Google Scholar] [CrossRef]
- Varghese, S.S.; Frankel, S.H. Numerical modeling of pulsatile turbulent flow in stenotic vessels. J. Biomech. Eng. 2003, 125, 445–460. [Google Scholar] [CrossRef]
- Barber, T.J.; Simmons, A. Large eddy simulation of a stenosed artery using a femoral artery pulsatile flow profile. Artif. Organs 2011, 35, E155–E160. [Google Scholar] [CrossRef]
- Sherwin, S.J.; Blackburn, H.M. Three-dimensional instabilities and transition of steady and pulsatile axisymmetric stenotic flows. J. Fluid Mech. 2005, 533, 297–327. [Google Scholar] [CrossRef] [Green Version]
- Griffith, M.D.; Leweke, T.; Thompson, M.C.; Hourigan, K. Steady inlet flow in stenotic geometries: Convective and absolute instabilities. J. Fluid Mech. 2008, 616, 111. [Google Scholar] [CrossRef]
- Kitamura, K.; Hasegawa, H.; Kanai, H. Accurate estimation of carotid luminal surface roughness using ultrasonic radio-frequency echo. Jpn. J. Appl. Phys. 2012, 51, 07GF08. [Google Scholar] [CrossRef]
- Nagai, Y.; Cinthio, M.; Hasegawa, H.; Bengtsson, M.; Evander, M.; Albinsson, J.; Kanai, H. In vitro experiment using porcine artery for evaluation of ultrasonic measurement of arterial luminal surface profile. J. Med. Ultrason. 2014, 41, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Yakhot, A.; Grinberg, L.; Nikitin, N. Modeling rough stenoses by an immersed-boundary method. J. Biomech. 2005, 38, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Stroud, J.; Berger, S.; Saloner, D. Influence of stenosis morphology on flow through severely stenotic vessels: Implications for plaque rupture. J. Biomech. 2000, 33, 443–455. [Google Scholar] [CrossRef]
- Johnston, P.R.; Kilpatrick, D. Mathematical modelling of flow through an irregular arterial stenosis. J. Biomech. 1991, 24, 1069–1077. [Google Scholar] [CrossRef]
- Umezu, M.; Yamada, T.; Fujimasu, H.; Fujimoto, T.; Ranawake, M.; Nogawa, A.; Kijima, T. Effects of surface roughness on mechanical hemolysis. Artif. Organs 1996, 20, 575–578. [Google Scholar] [CrossRef]
- Mustapha, N.; Mandal, P.K.; Johnston, P.R.; Amin, N. A numerical simulation of unsteady blood flow through multi-irregular arterial stenoses. Appl. Math. Model. 2010, 34, 1559–1573. [Google Scholar] [CrossRef]
- Bark Jr, D.L.; Ku, D.N. Wall shear over high degree stenoses pertinent to atherothrombosis. J. Biomech. 2010, 43, 2970–2977. [Google Scholar] [CrossRef]
- Xiong, G.; Taylor, C.A. Influence of vessel roughness on wall shear stress in image-based blood flow modeling. In Proceedings of the 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Rotterdam, The Netherlands, 14–17 April 2010; pp. 33–36. [Google Scholar]
- Cho, Y.I.; Back, L.H.; Crawford, D.W.; Cuffel, R.F. Experimental study of pulsatile and steady flow through a smooth tube and an atherosclerotic coronary artery casting of man. J. Biomech. 1983, 16, 933–946. [Google Scholar] [CrossRef]
- Back, L.; Cho, Y.; Crawford, D.; Cuffel, R. Effect of mild atherosclerosis on flow resistance in a coronary artery casting of man. J. Biomech. Eng. 1984, 106, 48–53. [Google Scholar] [CrossRef]
- Sarifuddin; Chakravarty, S.; Mandal, P.K. Effect of asymmetry and roughness of stenosis on non-Newtonian flow past an arterial segment. Int. J. Comput. Methods 2009, 6, 361–388. [Google Scholar] [CrossRef]
- Kenner, T. The measurement of blood density and its meaning. Basic Res. Cardiol. 1989, 84, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Mayer, G.A. Blood viscosity in healthy subjects and patients with coronary heart disease. Can. Med. Assoc. J. 1964, 91, 951. [Google Scholar] [PubMed]
- Myers, J.; Moore, J.; Ojha, M.; Johnston, K.; Ethier, C. Factors influencing blood flow patterns in the human right coronary artery. Ann. Biomed. Eng. 2001, 29, 109–120. [Google Scholar] [CrossRef]
- El Zahab, Z.; Divo, E.; Kassab, A. A localized collocation meshless method (LCMM) for incompressible flows CFD modeling with applications to transient hemodynamics. Eng. Anal. Bound. Elem. 2009, 33, 1045–1061. [Google Scholar] [CrossRef]
- He, X.; Ku, D.N. Pulsatile flow in the human left coronary artery bifurcation: Average conditions. J. Biomech. Eng. 1996, 118, 74–82. [Google Scholar] [CrossRef]
- Himburg, H.A.; Grzybowski, D.M.; Hazel, A.L.; LaMack, J.A.; Li, X.-M.; Friedman, M.H. Spatial comparison between wall shear stress measures and porcine arterial endothelial permeability. Am. J. Physiol.-Heart Circ. Physiol. 2004, 286, H1916–H1922. [Google Scholar] [CrossRef] [Green Version]
- Peiffer, V.; Sherwin, S.J.; Weinberg, P.D. Computation in the rabbit aorta of a new metric–the transverse wall shear stress–to quantify the multidirectional character of disturbed blood flow. J. Biomech. 2013, 46, 2651–2658. [Google Scholar] [CrossRef] [Green Version]
- Yi, J.; Tian, F.-B.; Simmons, A.; Barber, T. A Computational Analysis of the Influence of a Pressure Wire in Evaluating Coronary Stenosis. Fluids 2021, 6, 165. [Google Scholar] [CrossRef]
- Gijsen, F.; Katagiri, Y.; Barlis, P.; Bourantas, C.; Collet, C.; Coskun, U.; Daemen, J.; Dijkstra, J.; Edelman, E.; Evans, P.; et al. Expert recommendations on the assessment of wall shear stress in human coronary arteries: Existing methodologies, technical considerations, and clinical applications. Eur. Heart J. 2019, 40, 3421–3433. [Google Scholar] [CrossRef] [Green Version]
- Malek, A.M.; Alper, S.L.; Izumo, S. Hemodynamic Shear Stress and Its Role in Atherosclerosis. JAMA 1999, 282, 2035–2042. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Yin, L.; Xu, L.; Liang, F.J.J.o.b. Non-periodicity of blood flow and its influence on wall shear stress in the carotid artery bifurcation: An in vivo measurement-based computational study. J. Biomech. 2020, 101, 109617. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-W.; Steinman, D.A. On the relative importance of rheology for image-based CFD models of the carotid bifurcation. J. Biomech. Eng. 2007, 129, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Moyle, K.R.; Antiga, L.; Steinman, D.A.J.J.o.b.e. Inlet conditions for image-based CFD models of the carotid bifurcation: Is it reasonable to assume fully developed flow? J. Biomech. Eng. 2006, 128, 371–379. [Google Scholar] [CrossRef]
- Ramasamy, A.; Jin, C.; Tufaro, V.; Bajaj, R.; Kilic, Y.; Safi, H.; Amersey, R.; Jones, D.; Torii, R.; Lansky, A.; et al. Computerised Methodologies for Non-Invasive Angiography-Derived Fractional Flow Reserve Assessment: A Critical Review. J. Interv. Cardiol. 2020, 2020, 6381637. [Google Scholar] [CrossRef]
- Jhand, A.; Gordon, P.C.; Sharaf, B.L.; Seto, A.H.; Amin, A.P.; Naidu, S.S.; Goldsweig, A.M. Contrast Fractional Flow Reserve (cFFR) and Computed Tomography Fractional Flow Reserve (CT-FFR) Guidance for Percutaneous Coronary Intervention (PCI). Curr. Cardiovasc. Imaging Rep. 2020, 13, 23. [Google Scholar] [CrossRef]
- Morris, P.D.; van de Vosse, F.N.; Lawford, P.V.; Hose, D.R.; Gunn, J.P. “Virtual” (Computed) Fractional Flow Reserve: Current Challenges and Limitations. JACC Cardiovasc. Interv. 2015, 8, 1009–1017. [Google Scholar] [CrossRef] [Green Version]
- Taylor, C.A.; Fonte, T.A.; Min, J.K. Computational Fluid Dynamics Applied to Cardiac Computed Tomography for Noninvasive Quantification of Fractional Flow Reserve: Scientific Basis. J. Am. Coll. Cardiol. 2013, 61, 2233–2241. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equation | Description | |
|---|---|---|
| Time-averaged wall shear stress (TAWSS) | Time average of the WSS magnitude over a cardiac cycle | |
| Oscillatory shear index (OSI) | Oscillatory variation in the WSS [27] | |
| Relative residence time (RRT) | Near-wall flow stagnation [28] | |
| Transverse wall shear stress (transWSS) | Multi-directionality of the flow field [29] |
| WSS Metrics | Threshold | Smooth | Rough | Difference |
|---|---|---|---|---|
| TAWSS (Pa) | < 5 | 4.51% | 5.16% | 0.65% |
| 5–10 | 3.14% | 3.37% | 0.23% | |
| 10–50 | 19.15% | 22.87% | 3.72% | |
| 50–100 | 31.63% | 31.72% | 0.09% | |
| > 100 | 41.57% | 36.88% | 4.69% | |
| OSI | < 0.1 | 95.10% | 94.50% | 0.60% |
| 0.1–0.2 | 2.93% | 3.04% | 0.11% | |
| 0.2–0.5 | 1.97% | 2.47% | 0.50% | |
| RRT (Pa−1) | < 0.2 | 94.42% | 93.14% | 1.28% |
| 0.2–0.5 | 4.36% | 5.21% | 0.85% | |
| > 0.5 | 1.22% | 1.62% | 0.40% | |
| TransWSS (Pa) | < 5 | 74.39% | 77.11% | 2.72% |
| 5–10 | 20.67% | 18.44% | 2.23% | |
| > 10 | 4.95% | 4.44% | 0.51% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, J.; Tian, F.-B.; Simmons, A.; Barber, T. Impact of Modelling Surface Roughness in an Arterial Stenosis. Fluids 2022, 7, 179. https://doi.org/10.3390/fluids7050179
Yi J, Tian F-B, Simmons A, Barber T. Impact of Modelling Surface Roughness in an Arterial Stenosis. Fluids. 2022; 7(5):179. https://doi.org/10.3390/fluids7050179
Chicago/Turabian StyleYi, Jie, Fang-Bao Tian, Anne Simmons, and Tracie Barber. 2022. "Impact of Modelling Surface Roughness in an Arterial Stenosis" Fluids 7, no. 5: 179. https://doi.org/10.3390/fluids7050179
APA StyleYi, J., Tian, F.-B., Simmons, A., & Barber, T. (2022). Impact of Modelling Surface Roughness in an Arterial Stenosis. Fluids, 7(5), 179. https://doi.org/10.3390/fluids7050179