
rhEGF-Loaded Hydrogel in the Treatment of Chronic Wounds in Patients with Diabetes: Clinical Cases

 , , and
, , and
Abstract
:1. Introduction
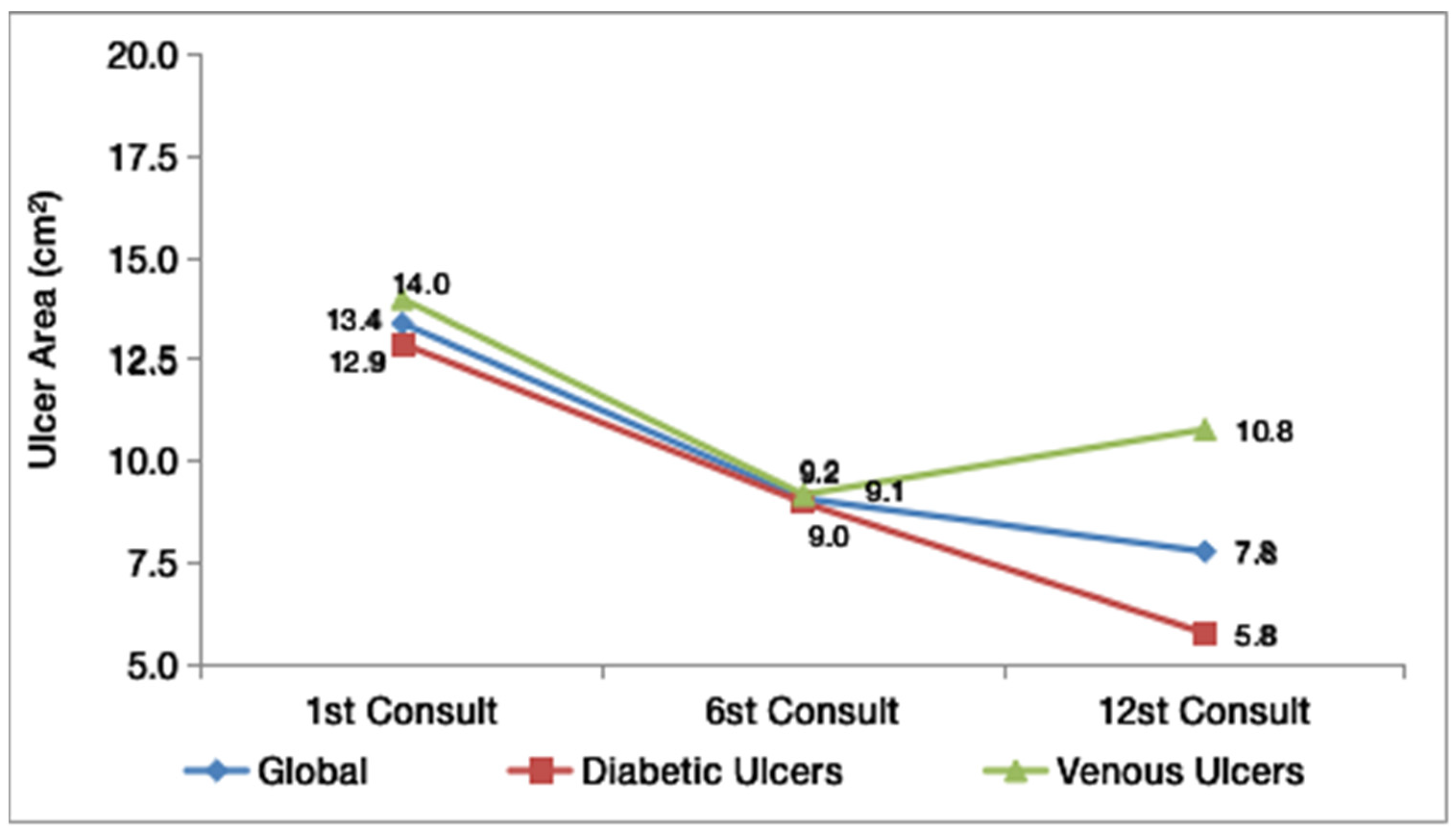
2. Results
3. Discussion
Limitations
4. Conclusions
5. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armstrong, D.G.; Eidt, J.F.; Berman, R.S. Clinical assessment of chronic wounds. Wolters Kluwer Up Date 2019, 1, 12–18. [Google Scholar]
- Martinengo, L.; Olsson, M.; Bajpai, R.; Soljak, M.; Upton, Z.; Schmidtchen, A.; Car, J.; Järbrink, K. Prevalence of chronic wounds in the general population: Systematic review and meta-analysis of observational studies. Ann. Epidemiol. 2019, 29, 8–15. [Google Scholar] [CrossRef]
- Järbrink, K.; Ni, G.; Sönnergren, H.; Schmidtchen, A.; Pang, C.; Bajpai, R.; Car, J. Prevalence and incidence of chronic wounds and related complications: A protocol for a systematic review. Syst. Rev. 2016, 5, 152. [Google Scholar] [CrossRef] [Green Version]
- Menke, N.B.; Ward, K.R.; Witten, T.M.; Bonchev, D.G.; Diegelmann, R.F. Impaired wound healing. Clin. Dermatol. 2007, 25, 19–25. [Google Scholar] [CrossRef]
- Infinity Pharma. Epifactor® Revolução da Regeneração da pele. São Paulo. 2019. Available online: https://infinitypharma.com.br/wp-content/uploads/2019/12/Epifactor.pdf (accessed on 20 April 2022).
- Esquirol-Caussa, J.; Herrero-Vila, E. Human recombinant epidermal growth factor in skin lesions: Cases in EPItelizando project. J. Dermatol. Treat. 2018, 30, 96–101. [Google Scholar] [CrossRef]
- Pyun, D.G.; Choi, H.J.; Yoon, H.S.; Thambi, T.; Lee, D.S. Polyurethane foam containing rhEGF as a dressing material for healing diabetic wounds: Synthesis, characterization, in vitro and in vivo studies. Colloids Surf. B Biointerfaces 2015, 135, 699–706. [Google Scholar] [CrossRef]
- Chan, L.K.; Chiu, Y.T.; Sze, K.M.F.; Ng, I.O.L. Tensin4 is up-regulated by EGF-induced ERK1/2 activity and promotes cell proliferation and migration in hepatocellular carcinoma. Oncotarget 2015, 6, 209–264. [Google Scholar] [CrossRef] [Green Version]
- Khanbanha, N.; Atyabi, F.; Taheri, A.; Talaie, F.; Mahbod, M.; Dinarvand, R. Healing efficacy of an EGF impregnated triple gel based wound dressing: In vitro and in vivo studies. Biomed. Res. Int. 2014, 2014, 493732. [Google Scholar]
- Zhou, C.; Huang, Z.; Huang, Y.; Wang, B.; Yang, P.; Fan, Y.; Hou, A.; Yang, B.; Zhao, Z.; Quan, G.; et al. In situ gelation of rhEGF-containing liquid crystalline precursor with good cargo stability and system mechanical properties: A novel delivery system for chronic wounds treatment. Biomater. Sci. 2019, 7, 995–1010. [Google Scholar] [CrossRef]
- Ahmad, Z.; Salman, S.; Khan, S.A.; Amin, A.; Rahman, Z.U.; Al-Ghamdi, Y.O.; Akhtar, K.; Bakhsh, E.M.; Khan, S.B. Versatility of Hydrogels: From Synthetic Strategies, Classification, and Properties to Biomedical Applications. Gels 2022, 8, 167. [Google Scholar] [CrossRef]
- Kong, M.S.; Koh, W.G.; Lee, H.J. Controlled Release of Epidermal Growth Factor from Furfuryl-Gelatin Hydrogel Using in Situ Visible Light-Induced Crosslinking and Its Effects on Fibroblasts Proliferation and Migration. Gels 2022, 8, 214. [Google Scholar] [CrossRef]
- Abazari, M.F.; Gholizadeh, S.; Karizi, S.Z.; Birgani, N.H.; Abazari, D.; Paknia, S.; Derakhshankhah, H.; Allahyari, Z.; Amini, S.M.; Hamidi, M.; et al. Recent Advances in Cellulose-Based Structures as the Wound-Healing Biomaterials: A Clinically Oriented Review. Appl. Sci. 2021, 11, 7769. [Google Scholar] [CrossRef]
- Yang, S.; Geng, Z.; Ma, K.; Sun, X.; Fu, X. Efficacy of topical recombinant human epidermal growth factor for treatment of diabetic foot ulcer: A systematic review and meta-analysis. Int. J. Low Extrem. Wounds 2016, 15, 120–125. [Google Scholar] [CrossRef]
- Hashemi, S.A.; Madani, S.A.; Abediankenari, S. The review on properties of Aloe vera in healing of cutaneous wounds. Biomed. Res. Int. 2015, 2015, 714216. [Google Scholar] [CrossRef] [Green Version]
- Ferroni, L.; Gardin, C.; De Pieri, A.; Sambataro, M.; Seganfreddo, E.; Iacopi, E.; Piaggesi, A. Treatment of diabetic foot ulcers with Therapeutic Magnetic Resonance (TMR®) improves the quality of granulation tissue. Eur. J. Histochem. 2017, 61, 2800. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, V.; Juttada, U.; Babu, M. Efficacy of Recombinant Human Epidermal Growth Factor (Regen-D 150) in Healing Diabetic Foot Ulcers: A Hospital-Based Randomized Controlled Trial. Int. J. Low Extrem. Wounds 2019, 19, 158–164. [Google Scholar] [CrossRef]
- Gomez-Villa, R.; Aguilar-Rebolledo, F.; Lozano-Platonoff, A.; Teran-Soto, J.M.; Fabian-Victoriano, M.R.; Kresch-Tronik, N.S.; Garrido-Espíndola, X.; Garcia-Solis, A.; Bondani-Guasti, A.; Bierzwinsky-Sneider, G.; et al. Efficacy of intralesional recombinant human epidermal growth factor in diabetic foot ulcers in Mexican patients: A randomized double-blinded controlled trial. Wound Repair Regen. 2014, 22, 497–503. [Google Scholar] [CrossRef]
- Tuyet, H.L.; Nguyen Quynh, T.T.; Vo Hoang Minh, H.; Thi Bich, D.N.; Do Dinh, T.; Le Tan, D.; Tran Trong, T.N. The efficacy and safety of epidermal growth factor in treatment of diabetic foot ulcers: The preliminary results. Int. Wound J. 2009, 6, 159–166. [Google Scholar] [CrossRef]
- Oliveira, F.P.D.; Oliveira, B.G.R.B.D.; Santana, R.F.; Silva, B.D.P.; Candido, J.D.S.C. Nursing interventions and outcomes classifi cations in patients with wounds: Cross-mapping. Rev. Gauch. Enferm. 2016, 37, e55033. [Google Scholar]
- Radischat, N.; Augustin, M.; Herberger, K.; Wille, A.; Goroncy-Bermes, P. Influence of human wound exudate on the bactericidal efficacy of antiseptic agents in quantitative suspension tests on the basis of European Standards (DIN EN 13727). Int. Wound J. 2020, 17, 781–789. [Google Scholar] [CrossRef]
- Carstens, M.H.; Gómez, A.; Cortés, R.; Turner, E.; Pérez, C.; Ocon, M.; Correa, D. Non-reconstructable peripheral vascular disease of the lower extremity in ten patients treated with adipose-derived stromal vascular fraction cells. Stem. Cell Res. 2017, 18, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Abreu, A.M.; Oliveira, B.G.R.B. A study of the Unna Boot compared with the elastic bandage in venous ulcers: A randomized clinical trial. Rev. Lat. Enferm. 2015, 23, 571–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frykberg, R.G.; Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 2015, 4, 560–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Everett, E.; Mathioudakis, N. Update on management of diabetic foot ulcers. Ann. N. Y. Acad. Sci. 2018, 1411, 153. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.; Franco, S.; Sanches, F.L.F.Z.; Rosalva, R.; Hack, J.; Meotti, N.; Magro, M. Nutritional Characterization of Patients with Chronic Ulcer of Lower Limb in the Outpatient Treatment of Wounds of the Campus Cedeteg Unicentro, Guarapuava-PR. J. Health Sci. 2015, 17, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Patil, M.D.; Gunasekaran, U.; La Fontaine, J.; Meneghini, L. Does Improving Glycemic Control Accelerate Healing of Diabetic Foot Ulcers? Am. Diabetes Assoc. 2018, 67, 14–20. [Google Scholar] [CrossRef]
- Niculescu, A.G.; Grumezescu, A.M. An up-to-date review of biomaterials application in wound management. Polymers 2022, 14, 421. [Google Scholar] [CrossRef]
- Carvalho, M.R.; Silveira, I.A.; Oliveira, R.B.; Guitton, B. Treatment of venous ulcers with growth factors: Systematic review and meta-analysis. Rev. Bras. Enferm. 2019, 72, 200–210. [Google Scholar] [CrossRef]
- Gilligan, A.M.; Waycaster, C.R.; Motley, T.A. Cost effectiveness of becaplermin gel on wound healing of diabetic foot ulcers. Wound Repair Regen. 2015, 23, 353–360. [Google Scholar] [CrossRef]
- Lantis, J.C.; Boone, D.; Gendics, C.; Todd, G. Analysis of patient cost for recombinant human platelet-derived growth factor therapy as the first-line treatment of the insured patient with a diabetic foot ulcer. Adv. Ski. Wound Care 2009, 22, 167–171. [Google Scholar] [CrossRef]
- Lund, H.; Curtin, J. Management of a non-healing postoperative wound using a bacteria and fungi-binding mesh. Wounds Int. 2014, 5, 20–22. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Category | Absolute Frequency | Relative Frequency |
|---|---|---|---|
| Sex | Female | 3 | 30% |
| Male | 7 | 70% | |
| Baseline Diseases | DM * | 2 | 20% |
| DM + SAH & | 7 | 70% | |
| DM + SAH + CVI @ | 1 | 10% | |
| Etiology of Injury | |||
| Diabetic Ulcers | 6 | 60% | |
| Venous Ulcers | 4 | 40% | |
| Time of the lesion | Up until 1 year | 3 | 30% |
| >1 year to 5 years | 4 | 40% | |
| More than 5 years | 3 | 30% | |
| Median | Standard Deviation | Coefficient of variation | |
| Age (years) | 61.92 | 9.41 | 0.15 |
| Time of the lesion (Months) | 63.4 | 74.3 | 1.17 |
| Body Mass Index (kg/m²) | 32.17 | 6.32 | 0.20 |
| Glycated Hemoglobin (%) | 61.92 | 2.71 | 0.04 |
| Ankle-Brachial Index | 0.94 | 0.21 | 0.22 |
| Global | Diabetic Ulcers | Venous Ulcers | |
|---|---|---|---|
| Relative reduction (%) | |||
| Minimum | 2.7 | 3.4 | 2.7 |
| Median | 23.6 | 23.6 | 18.9 |
| Maximum | 79.8 | 79.8 | 48.1 |
| Mean | 28.9 | 33.4 | 22.1 |
| Standard Deviation | 25.9 | 30.0 | 20.1 |
| Coefficient of variation | 0.90 | 0.90 | 0.91 |
| Absolute Reduction (cm2) | |||
| Minimum | 0.2 | 0.4 | 0.2 |
| Median | 1.3 | 1.3 | 1.8 |
| Maximum | 38.0 | 38.0 | 9.0 |
| Mean | 5.6 | 7.2 | 3.2 |
| Standard Deviation | 11.7 | 15.1 | 4.1 |
| Coefficient of variation | 2.09 | 2.10 | 1.28 |
| Granulation Tissue | Epithelialization Tissue | Devitalized Tissue | ||||
|---|---|---|---|---|---|---|
| (%) | 1st Consult | 12st Consult | 1st Consult | 12st Consult | 1st Consult | 12st Consult |
| 76–100 | 30% | 10% | 0% | 0% | 0% | 0% |
| 51–75 | 50% | 50% | 0% | 0% | 20% | 0% |
| 26–50 | 0% | 30% | 0% | 10% | 0% | 0% |
| 1–25 | 20% | 10% | 0% | 30% | 50% | 40% |
| 0 | 0% | 0% | 100% | 60% | 30% | 60% |
| p-valor * | 0.463 | 0.066 | 0.107 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira, B.G.R.B.; Oliveira, B.C.; Deutsch, G.; Pessanha, F.S.; Thiré, R.M.d.S.M.; de Castilho, S.R. rhEGF-Loaded Hydrogel in the Treatment of Chronic Wounds in Patients with Diabetes: Clinical Cases. Gels 2022, 8, 523. https://doi.org/10.3390/gels8080523
de Oliveira BGRB, Oliveira BC, Deutsch G, Pessanha FS, Thiré RMdSM, de Castilho SR. rhEGF-Loaded Hydrogel in the Treatment of Chronic Wounds in Patients with Diabetes: Clinical Cases. Gels. 2022; 8(8):523. https://doi.org/10.3390/gels8080523
Chicago/Turabian Stylede Oliveira, Beatriz Guitton Renaud Baptista, Bianca Campos Oliveira, Gabriela Deutsch, Fernanda Soares Pessanha, Rossana Mara da Silva Moreira Thiré, and Selma Rodrigues de Castilho. 2022. "rhEGF-Loaded Hydrogel in the Treatment of Chronic Wounds in Patients with Diabetes: Clinical Cases" Gels 8, no. 8: 523. https://doi.org/10.3390/gels8080523
APA Stylede Oliveira, B. G. R. B., Oliveira, B. C., Deutsch, G., Pessanha, F. S., Thiré, R. M. d. S. M., & de Castilho, S. R. (2022). rhEGF-Loaded Hydrogel in the Treatment of Chronic Wounds in Patients with Diabetes: Clinical Cases. Gels, 8(8), 523. https://doi.org/10.3390/gels8080523