
Intake of Sugar Substitute Gummy Candies Benefits the Glycemic Response in Healthy Adults: A Prospective Crossover Clinical Trial

 ,
,
Abstract
1. Introduction
2. Results
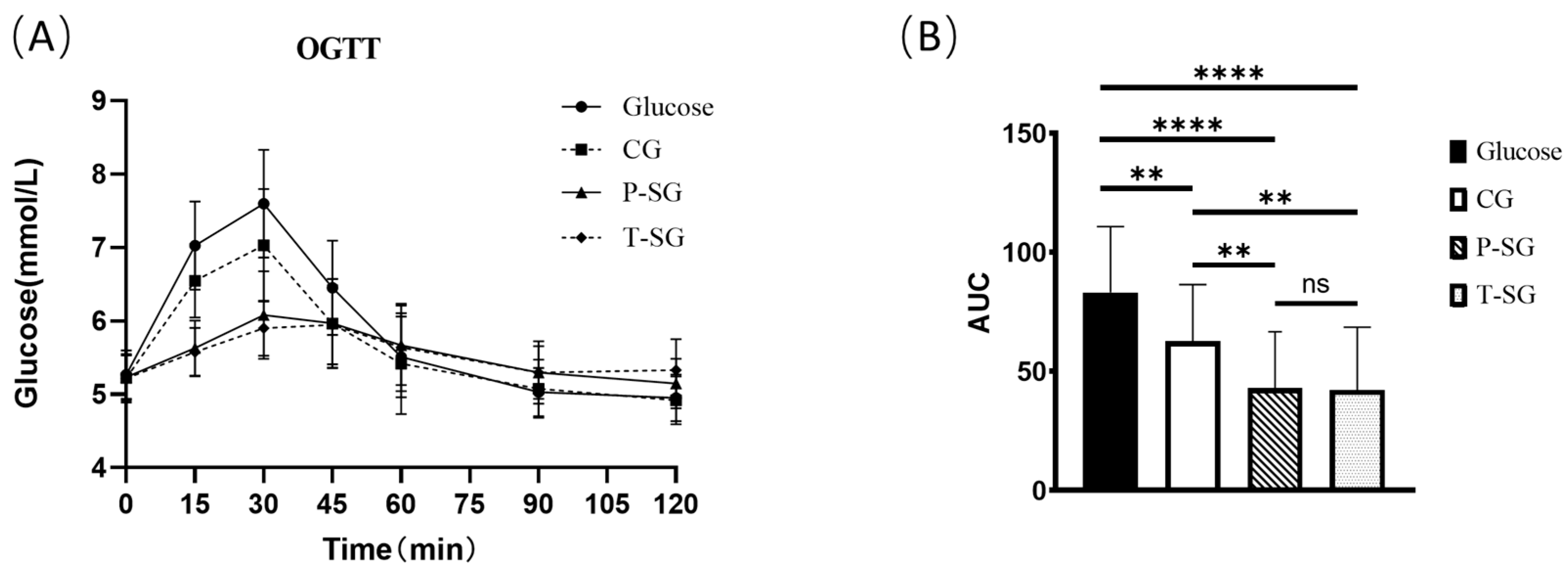
2.1. Glucose Tolerance Test of Gummy Candies
2.2. Glycemic Index (GI) and Glycemic Load (GL)
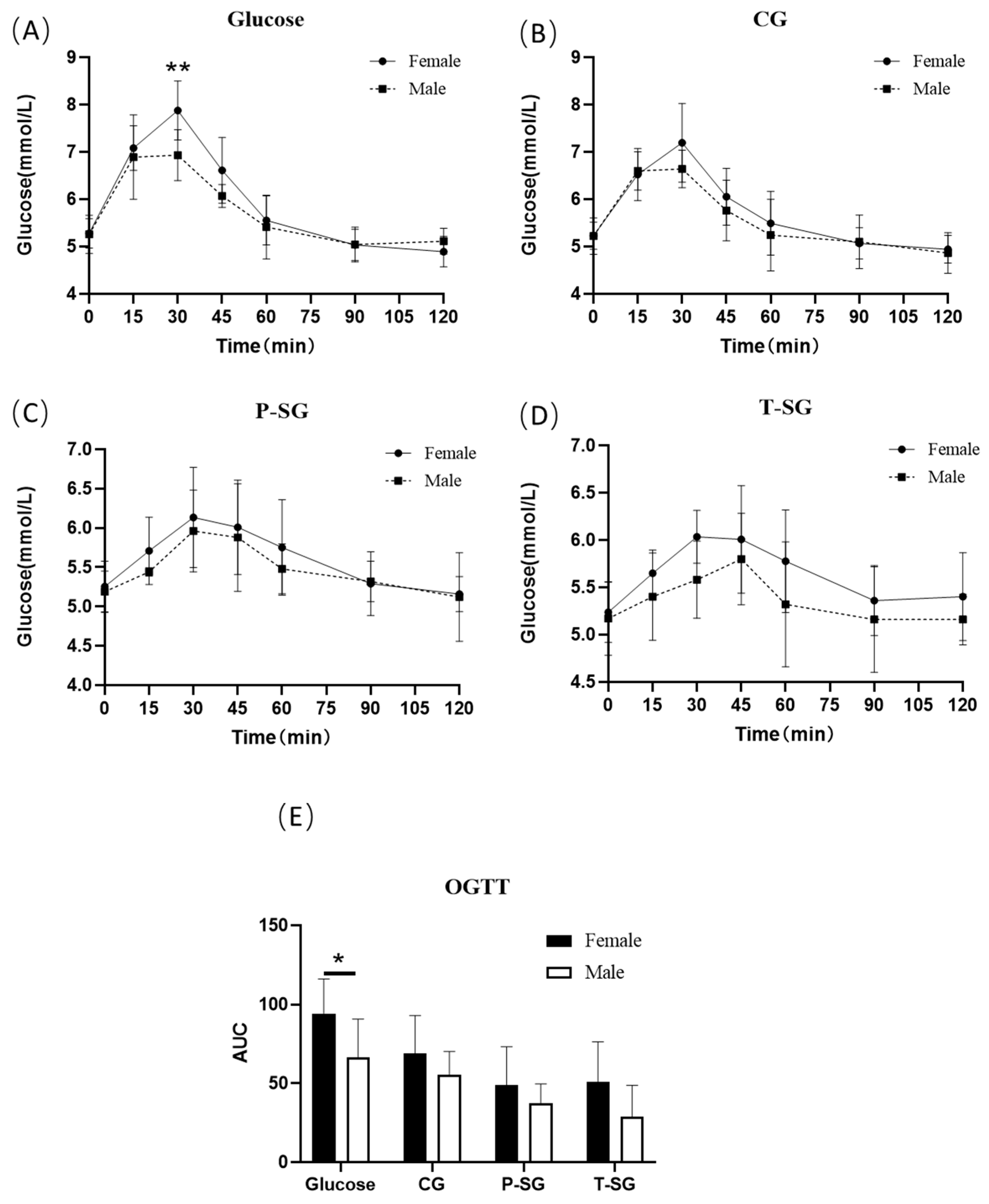
2.3. Differences in Glucose Tolerance between Male and Female
2.4. Mechanical Properties of Gummy Candies
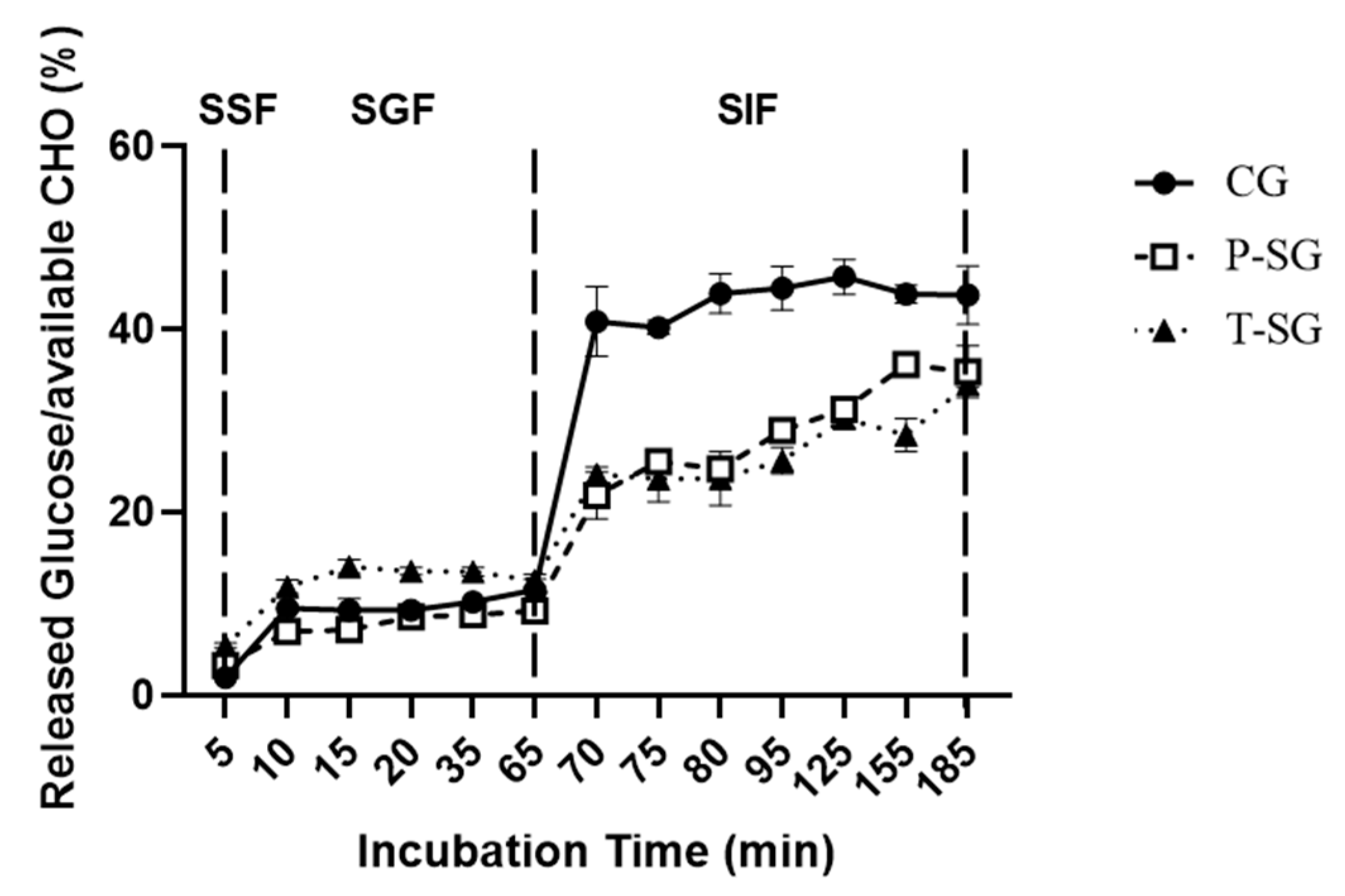
2.5. Glucose Release of Gummy Candies during In Vitro Digestion
3. Discussion
4. Conclusions
5. Materials and Methods
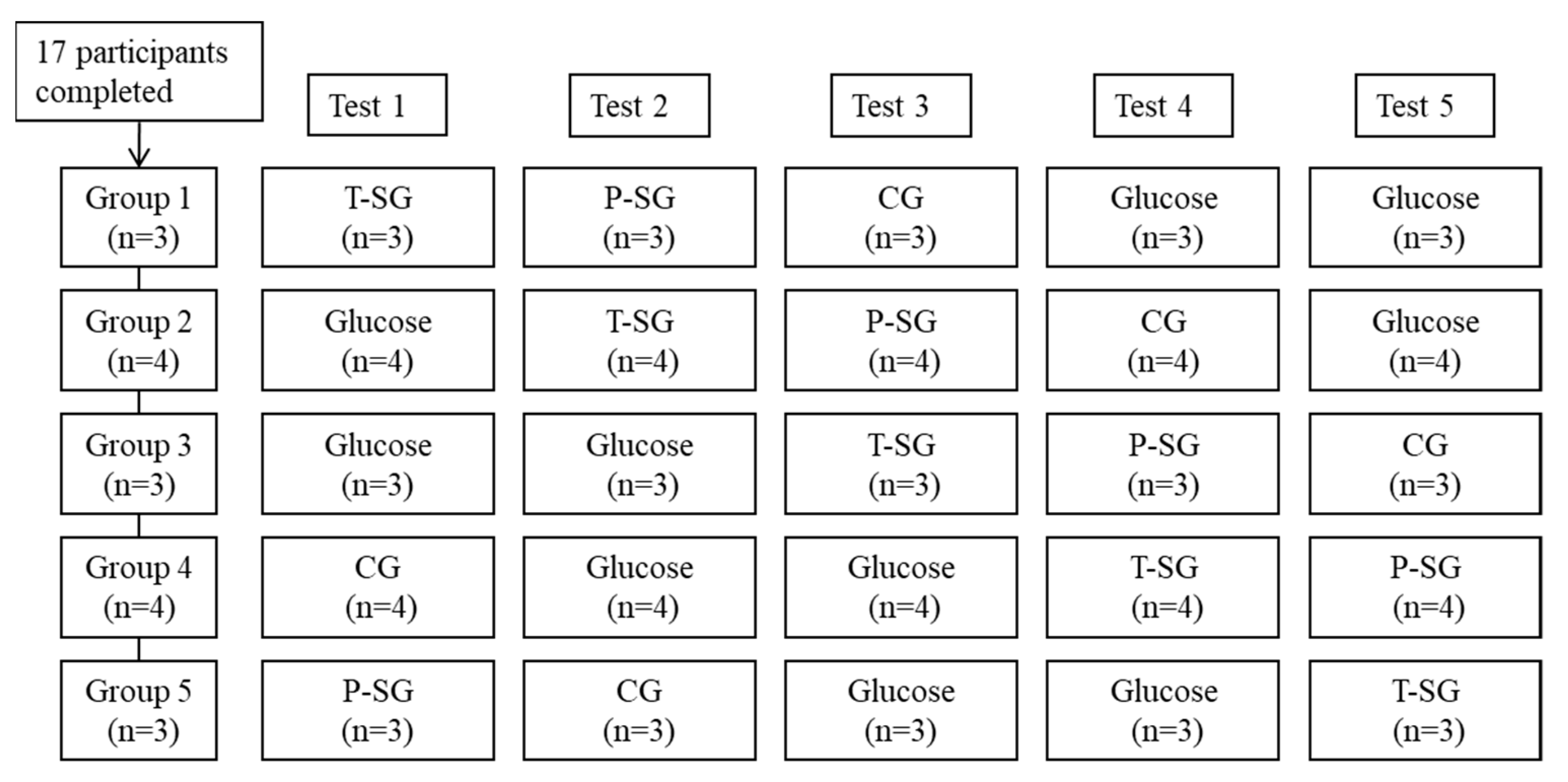
5.1. Clinical Study Design and Subjects
5.2. Panel Demographics and Subjects Baseline Characteristics
5.3. Procedures and Data Collection
5.4. Texture Profile Analysis
5.5. Glucose Release in Gummies during In Vitro Digestion
5.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeSalvo, K.B. Public Health 3.0: Applying the 2015-2020 Dietary Guidelines for Americans. Public Health Rep. 2016, 131, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.S.; Lay, S.; Yu, H.N.; Shen, S.R. Dietary Guidelines for Chinese Residents (2016): Comments and comparisons. J. Zhejiang Univ. Sci. B 2016, 17, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Björntorp, P. Obesity, Atherosclerosis and Diabetes Mellitus. Verh Dtsch Ges. Inn. Med. 1987, 93, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Brand-Miller, J.; Wolever, T.; Foster-Powell, K. The New Glucose Revolution: The Authoritative Guide to the Glycemic Index-The Dietary Solution for Lifelong Health; Marlowe & Company: New York, NY, USA, 2003; Volume 33. [Google Scholar]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The Diabetes Mellitus-Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int. J. Mol. Sci. 2020, 21, 1835. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Barker, H.; Fielden, H.; Baldwin, J.M.; Bowling, A.C.; Newman, H.C.; Jenkins, A.L.; Goff, D.V. Glycemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef]
- Ojo, O.; Ojo, O.O.; Adebowale, F.; Wang, X.H. The Effect of Dietary Glycaemic Index on Glycaemia in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2018, 10, 373. [Google Scholar] [CrossRef]
- Radulian, G.; Rusu, E.; Dragomir, A.; Posea, M. Metabolic effects of low glycaemic index diets. Nutr. J. 2009, 8, 5. [Google Scholar] [CrossRef]
- Periche, A.; Heredia, A.; Escriche, I.; Andrés, A.; Castelló, M.L. Optical, mechanical and sensory properties of based-isomaltulose gummy confections. Food Biosci. 2014, 7, 37–44. [Google Scholar] [CrossRef]
- Saha, D.; Bhattacharya, S. Hydrocolloids as thickening and gelling agents in food: A critical review. J. Food Sci. Technol. 2010, 47, 587–597. [Google Scholar] [CrossRef]
- Marfil, P.; Anhe, A.C.; Telis, V. Texture and Microstructure of Gelatin/Corn Starch-Based Gummy Confections. Food Biophys. 2012, 7, 236–243. [Google Scholar] [CrossRef]
- Mariel, S.A. Desarrollo de Formulaciones de Productos de Confitería de Bajo Aporte Calórico Empleando Polioles Como Edulcorantes. Ph.D. Thesis, Universidad Nacional Autónoma de México, Mexico City, México, 2011. [Google Scholar]
- Brand-Miller, J.; Hayne, S.; Petocz, P.; Colagiuri, S. Low-glycemic index diets in the management of diabetes: A meta-analysis of randomized controlled trials. Diabetes Care 2003, 26, 2261–2267. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, A.; Carrascosa, C.; Raheem, D.; Ramos, F.; Raposo, A. Maltitol: Analytical Determination Methods, Applications in the Food Industry, Metabolism and Health Impacts. Int. J. Environ. Res. Public Health 2020, 17, 5227. [Google Scholar] [CrossRef] [PubMed]
- Munro, I.C.; Berndt, W.O.; Borzelleca, J.F.; Flamm, G.; Lynch, B.S.; Kennepohl, E.; Bär, E.A.; Modderman, J. Erythritol: An interpretive summary of biochemical, metabolic, toxicological and clinical data. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 1998, 36, 1139–1174. [Google Scholar] [CrossRef]
- Huang, M.; Mao, Y.; Mao, Y.; Yang, H. Xylitol and Maltitol Improve the Rheological Property of Kappa-Carrageenan. Foods 2021, 11, 51. [Google Scholar] [CrossRef]
- Khin, M.N.; Goff, H.D.; Nsor-Atindana, J.; Ahammed, S.; Liu, F.; Zhong, F. Effect of texture and structure of polysaccharide hydrogels containing maltose on release and hydrolysis of maltose during digestion: In vitro study. Food Hydrocoll. 2021, 112, 106326. [Google Scholar] [CrossRef]
- Tharakan, A.; Norton, I.T.; Fryer, P.J.; Bakalis, S. Mass transfer and nutrient absorption in a simulated model of small intestine. J. Food Sci. 2010, 75, E339–E346. [Google Scholar] [CrossRef]
- McClements, D.J. Food hydrocolloids: Application as functional ingredients to control lipid digestion and bioavailability. Food Hydrocoll. 2021, 111, 106404. [Google Scholar] [CrossRef]
- Čižauskaitė, U.; Jakubaitytė, G.; Žitkevičius, V.; Kasparavičienė, G. Natural Ingredients-Based Gummy Bear Composition Designed According to Texture Analysis and Sensory Evaluation In Vivo. Molecules 2019, 24, 1442. [Google Scholar] [CrossRef]
- Kurt, A.; Bursa, K.; Toker, O.S. Gummy candies production with natural sugar source: Effect of molasses types and gelatin ratios. Food Sci. Technol. Int. 2022, 28, 118–127. [Google Scholar] [CrossRef]
- Livesey, G. Health potential of polyols as sugar replacers, with emphasis on low glycaemic properties. Nutr. Res. Rev. 2003, 16, 163–191. [Google Scholar] [CrossRef]
- den Hartog, G.J.; Boots, A.W.; Adam-Perrot, A.; Brouns, F.; Verkooijen, I.W.; Weseler, A.R.; Haenen, G.R.; Bast, A. Erythritol is a sweet antioxidant. Nutrition 2010, 26, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Nuutila, P.; Knuuti, M.J.; Mäki, M.; Laine, H.; Ruotsalainen, U.; Teräs, M.; Haaparanta, M.; Solin, O.; Yki-Järvinen, H. Gender and insulin sensitivity in the heart and in skeletal muscles. Studies using positron emission tomography. Diabetes 1995, 44, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Sicree, R.A.; Zimmet, P.Z.; Dunstan, D.W.; Cameron, A.J.; Welborn, T.A.; Shaw, J.E. Differences in height explain gender differences in the response to the oral glucose tolerance test- the AusDiab study. Diabet. Med. 2008, 25, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.H.; Arver, S.; Behre, H.M.; Buvat, J.; Meuleman, E.; Moncada, I.; Morales, A.M.; Volterrani, M.; Yellowlees, A.; Howell, J.D.; et al. Testosterone replacement in hypogonadal men with type 2 diabetes and/or metabolic syndrome (the TIMES2 study). Diabetes Care 2011, 34, 828–837. [Google Scholar] [CrossRef] [PubMed]
- Hackett, G.; Cole, N.; Bhartia, M.; Kennedy, D.; Raju, J.; Wilkinson, P. Testosterone replacement therapy improves metabolic parameters in hypogonadal men with type 2 diabetes but not in men with coexisting depression: The BLAST study. J. Sex. Med. 2014, 11, 840–856. [Google Scholar] [CrossRef]
- MacDonald, P.E.; El-Kholy, W.; Riedel, M.J.; Salapatek, A.M.; Light, P.E.; Wheeler, M.B. The multiple actions of GLP-1 on the process of glucose-stimulated insulin secretion. Diabetes 2002, 51 (Suppl. S3), S434–S442. [Google Scholar] [CrossRef]
- Passeri, C.R.; Andrade, J.A.; Tomal, K.T.; Pracucho, E.M.; Campos, L.P.; Sales-Peres, S.H. Masticatory Function Of Obese Candidates To Bariatric Surgery From Distinct Socioeconomic Classes. Arq. Bras. Cir. Dig. 2016, 29 (Suppl. S1), 53–58. [Google Scholar] [CrossRef]
- Sato, A.; Ohtsuka, Y.; Yamanaka, Y. Morning Mastication Enhances Postprandial Glucose Metabolism in Healthy Young Subjects. Tohoku J. Exp. Med. 2019, 249, 193–201. [Google Scholar] [CrossRef]
- Chen, L.; Yokoyama, W.; Liang, R.; Zhong, F. Enzymatic degradation and bioaccessibility of protein encapsulated β-carotene nano-emulsions during in vitro gastro-intestinal digestion. Food Hydrocoll. 2020, 100, 105177. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| B | SE | Wald Chi-Square | p Value | |
|---|---|---|---|---|
| Glucose | reference | |||
| CG | −0.238 | 0.105 | 5.169 | 0.023 |
| P-SG | −0.401 | 0.106 | 14.263 | <0.001 |
| T-SG | −0.419 | 0.109 | 14.673 | <0.001 |
| 0 min | reference | |||
| 15 min | 0.948 | 0.093 | 102.358 | <0.001 |
| 30 min | 1.412 | 0.109 | 166.478 | <0.001 |
| 45 min | 0.842 | 0.064 | 168.192 | <0.001 |
| 60 min | 0.319 | 0.059 | 28.668 | <0.001 |
| 90 min | −0.064 | 0.044 | 2.087 | 0.149 |
| 120 min | −0.153 | 0.041 | 13.658 | <0.001 |
| Glucose | CG | P-SG | T-SG | |
|---|---|---|---|---|
| GI | 100.00 | 81.9 | 54.1 | 49.9 |
| GL | - | 8.2 | 5.4 | 5.0 |
| Hardness | Springiness | Cohesiveness | Gumminess | Chewiness | Resilience | |
|---|---|---|---|---|---|---|
| CG | 273.03 ± 14.97 a | 0.99 ± 0.01 a | 0.9 ± 0.01 a | 245.35 ± 13.32 a | 242.18 ± 13.78 a | 0.45 ± 0.02 a |
| P-SG | 431.2 ± 24.77 b | 0.93 ± 0.01 b | 0.79 ± 0.03 b | 341.26 ± 24.78 b | 317.13 ± 24.84 b | 0.36 ± 0.02 b |
| T-SG | 496.7 ± 28.2 c | 0.93 ±0.02 b | 0.82 ± 0.02 b | 405.01 ± 26.74 c | 374.87 ± 26.39 c | 0.36 ± 0.02 b |
| Female (n = 12) | Male (n = 5) | |
|---|---|---|
| Age (year) | 28.6 ± 4.3 | 27.4 ± 3.1 |
| Height (cm) | 159.6 ± 5.8 | 172.0 ± 6.8 |
| Body weight (kg) | 54.5 ± 5.4 | 66.0 ± 8.5 |
| BMI (kg/m2) | 21.3 ± 1.3 | 22.2 ± 1.4 |
| Blood glucose (mmol/L) | 5.3 ± 0.3 | 5.2 ± 0.3 |
| Glucose | CG | P-SG | T-SG | |
|---|---|---|---|---|
| Carbohydrates * (%) | 100 | 76.6 | 78 | 78.5 |
| Protein (%) | 0 | 4.7 | 3.9 | 3.8 |
| Fat (%) | 0 | 4 | 4 | 4 |
| Water (%) | 0 | 14.7 | 14.1 | 13.7 |
| Glucose | CG | P-SG | T-SG | |
|---|---|---|---|---|
| Dosage (n)/test | - | 1 | 2 | 2 |
| Portion weight (g)/test | 10 | 14.15 | 25.64 | 25.86 |
| Calories (kcal)/test portion | 40 | 47.1 | 65.9 | 59.36 |
| Available carbohydrates (%) a | 100 | 71 | 39 | 39 |
| Available carbohydrates (g)/test portion b | 10 | 10 | 10 | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gan, D.; Xu, M.; Chen, L.; Cui, S.; Deng, C.; Qiao, Q.; Guan, R.; Zhong, F. Intake of Sugar Substitute Gummy Candies Benefits the Glycemic Response in Healthy Adults: A Prospective Crossover Clinical Trial. Gels 2022, 8, 642. https://doi.org/10.3390/gels8100642
Gan D, Xu M, Chen L, Cui S, Deng C, Qiao Q, Guan R, Zhong F. Intake of Sugar Substitute Gummy Candies Benefits the Glycemic Response in Healthy Adults: A Prospective Crossover Clinical Trial. Gels. 2022; 8(10):642. https://doi.org/10.3390/gels8100642
Chicago/Turabian StyleGan, Dan, Minjun Xu, Ling Chen, Shaohua Cui, Changyong Deng, Qian Qiao, Ruimiao Guan, and Fang Zhong. 2022. "Intake of Sugar Substitute Gummy Candies Benefits the Glycemic Response in Healthy Adults: A Prospective Crossover Clinical Trial" Gels 8, no. 10: 642. https://doi.org/10.3390/gels8100642
APA StyleGan, D., Xu, M., Chen, L., Cui, S., Deng, C., Qiao, Q., Guan, R., & Zhong, F. (2022). Intake of Sugar Substitute Gummy Candies Benefits the Glycemic Response in Healthy Adults: A Prospective Crossover Clinical Trial. Gels, 8(10), 642. https://doi.org/10.3390/gels8100642