

Penicillium digitatum, First Clinical Report in Chile: Fungal Co-Infection in COVID-19 Patient

 ,
,  , and
, and
Abstract
:1. Introduction
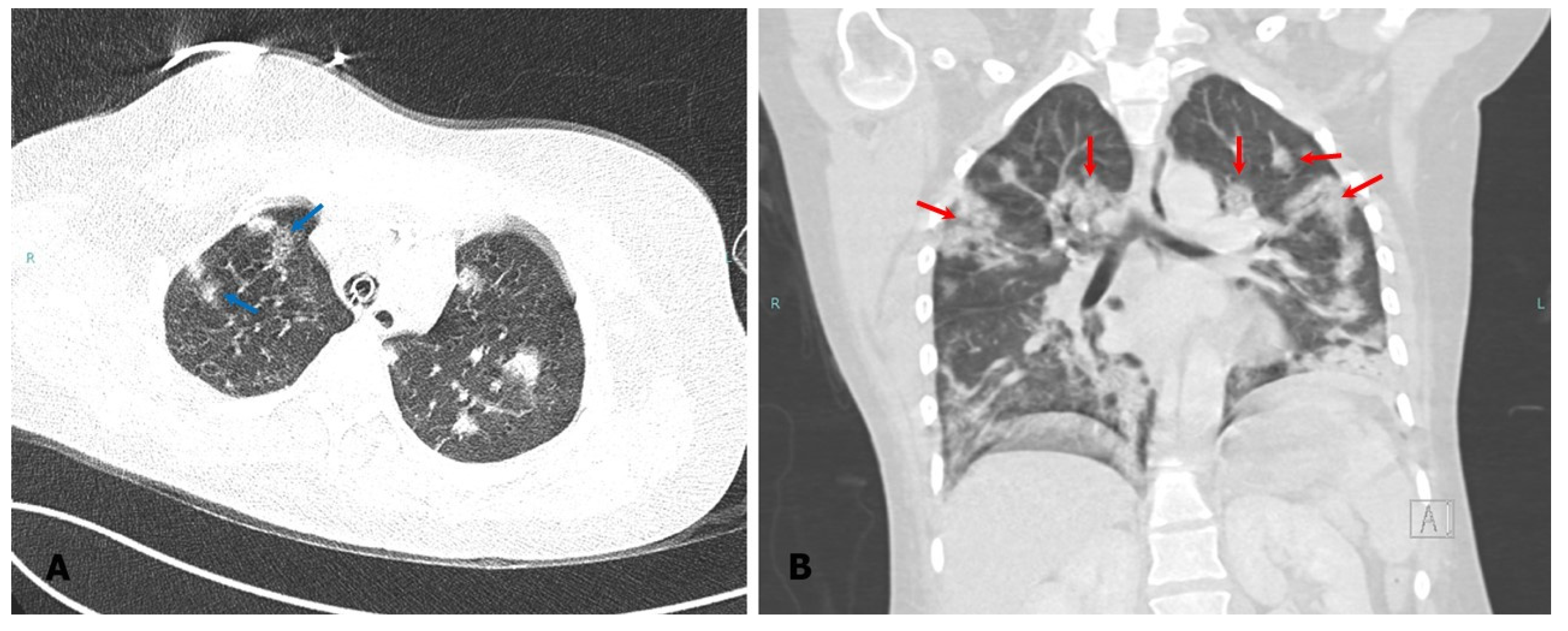
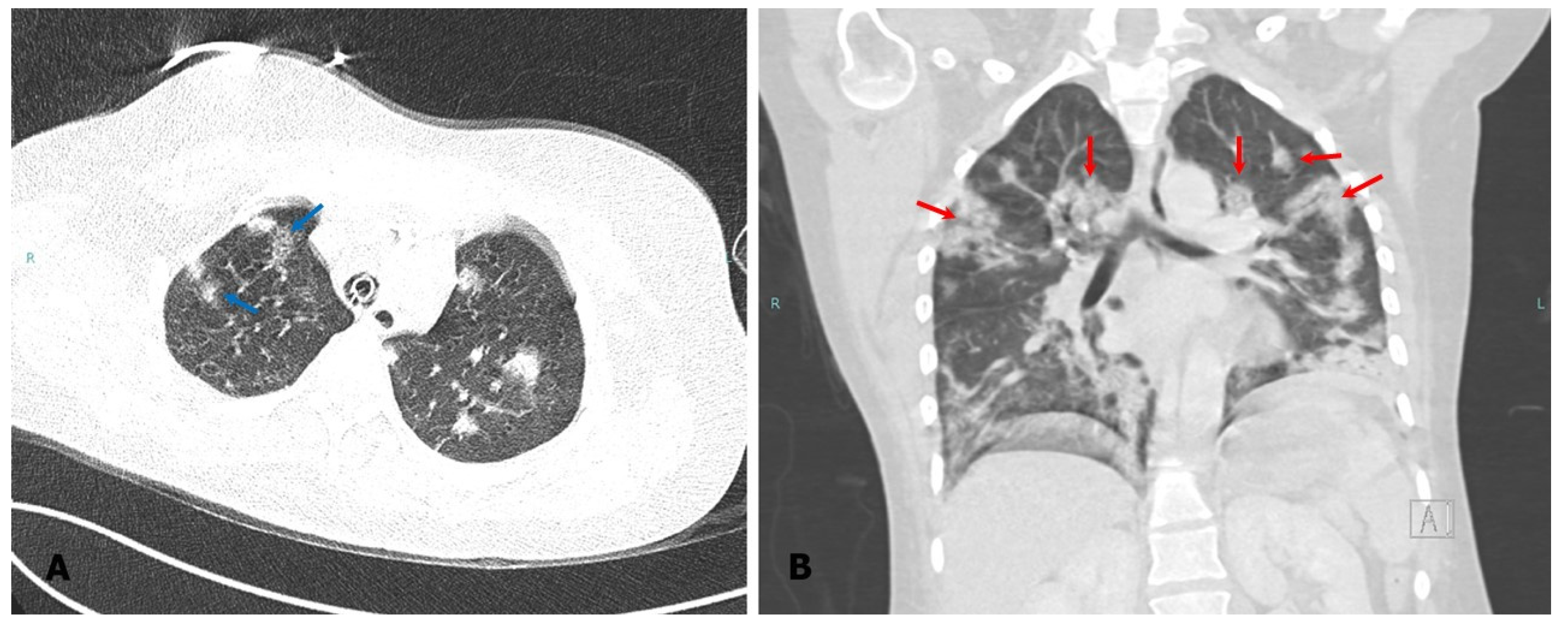
Case Presentation
2. Materials and Methods
2.1. Fungal Culture and Phenotypic Identification
2.2. Molecular Identification and Phylogenetic Analysis
2.3. In Vitro Antifungals Susceptibility Tests
2.4. Ethics Statement
3. Results
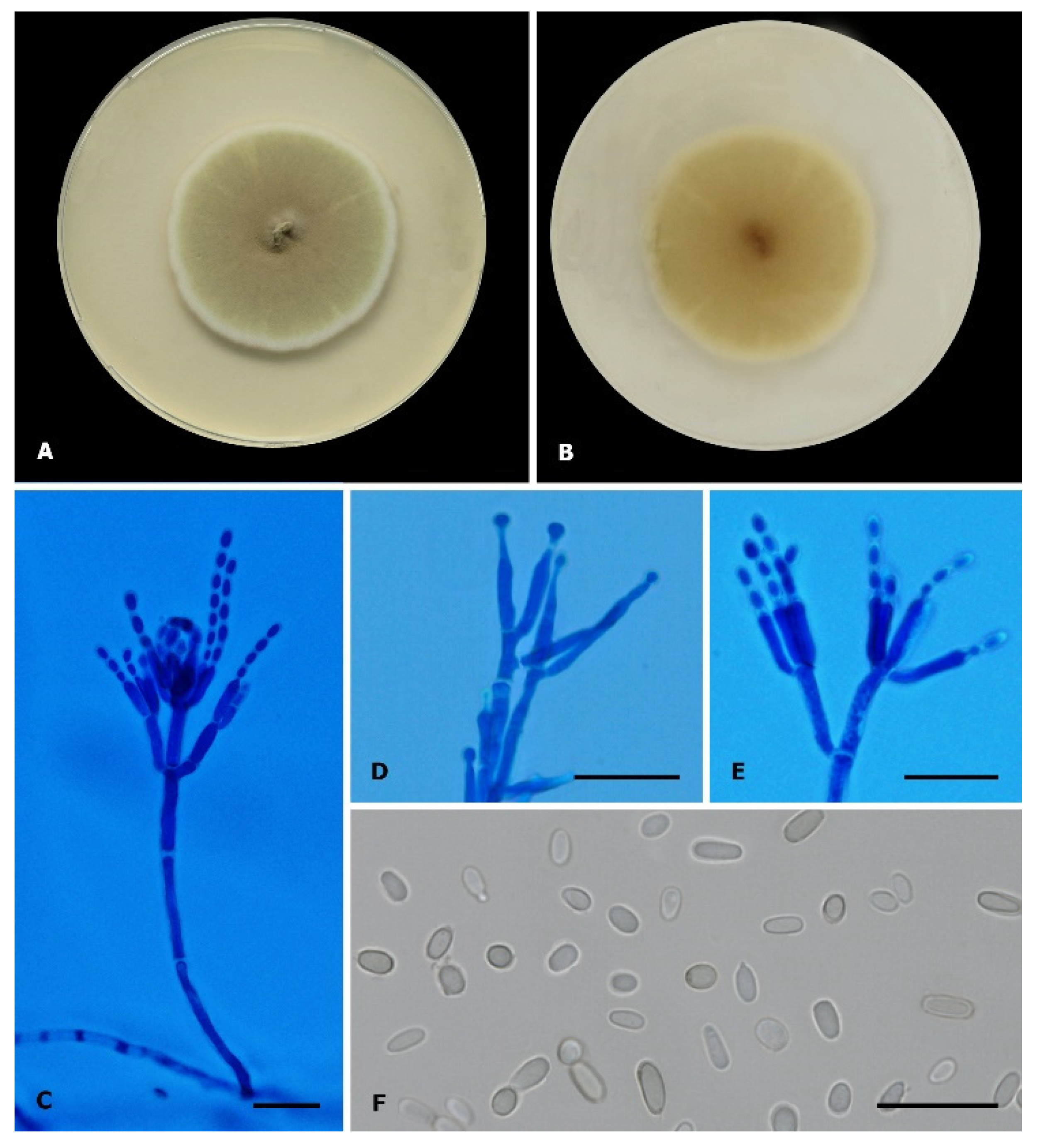
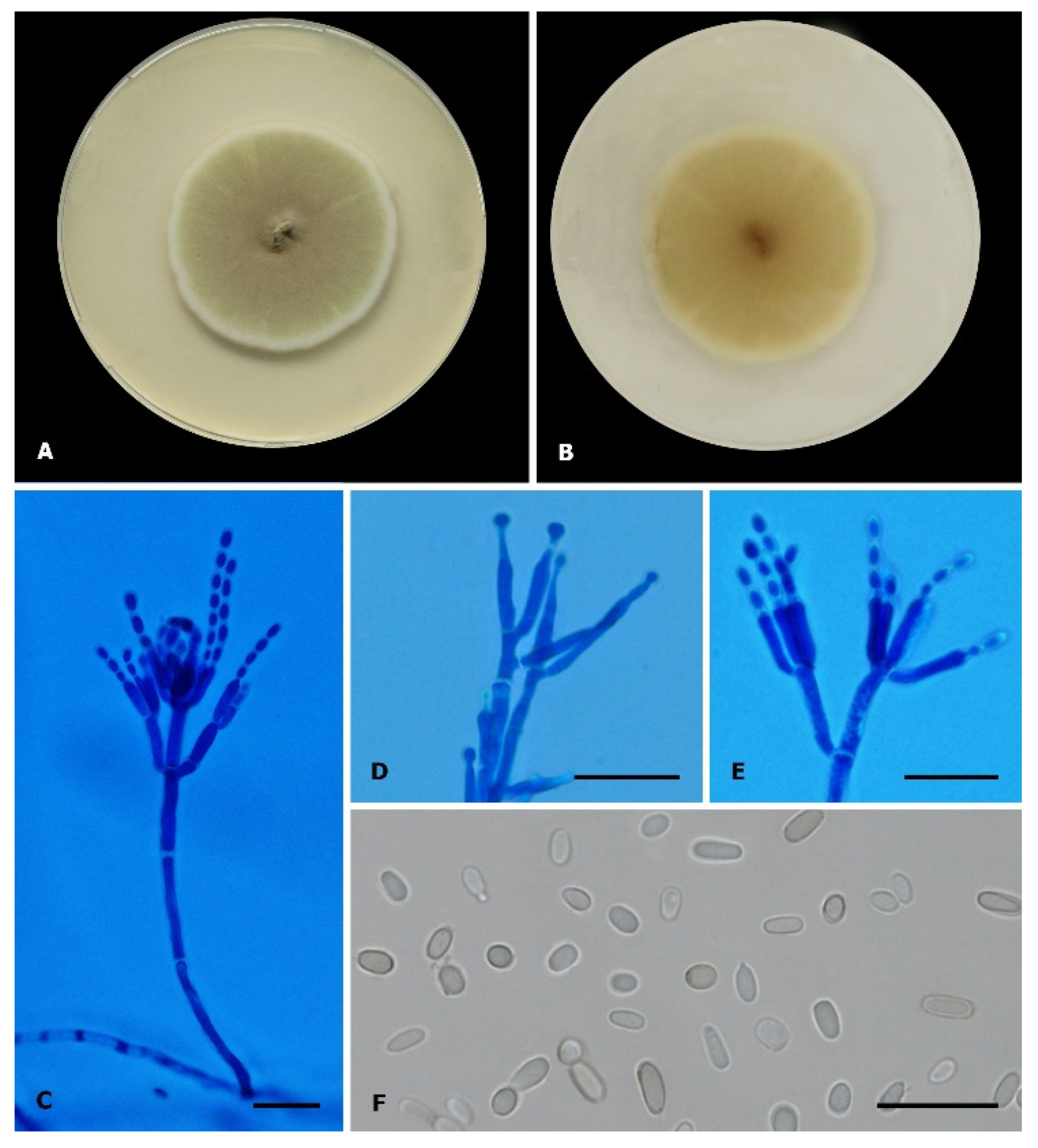
3.1. Phenotypic Study and Preliminary Identification
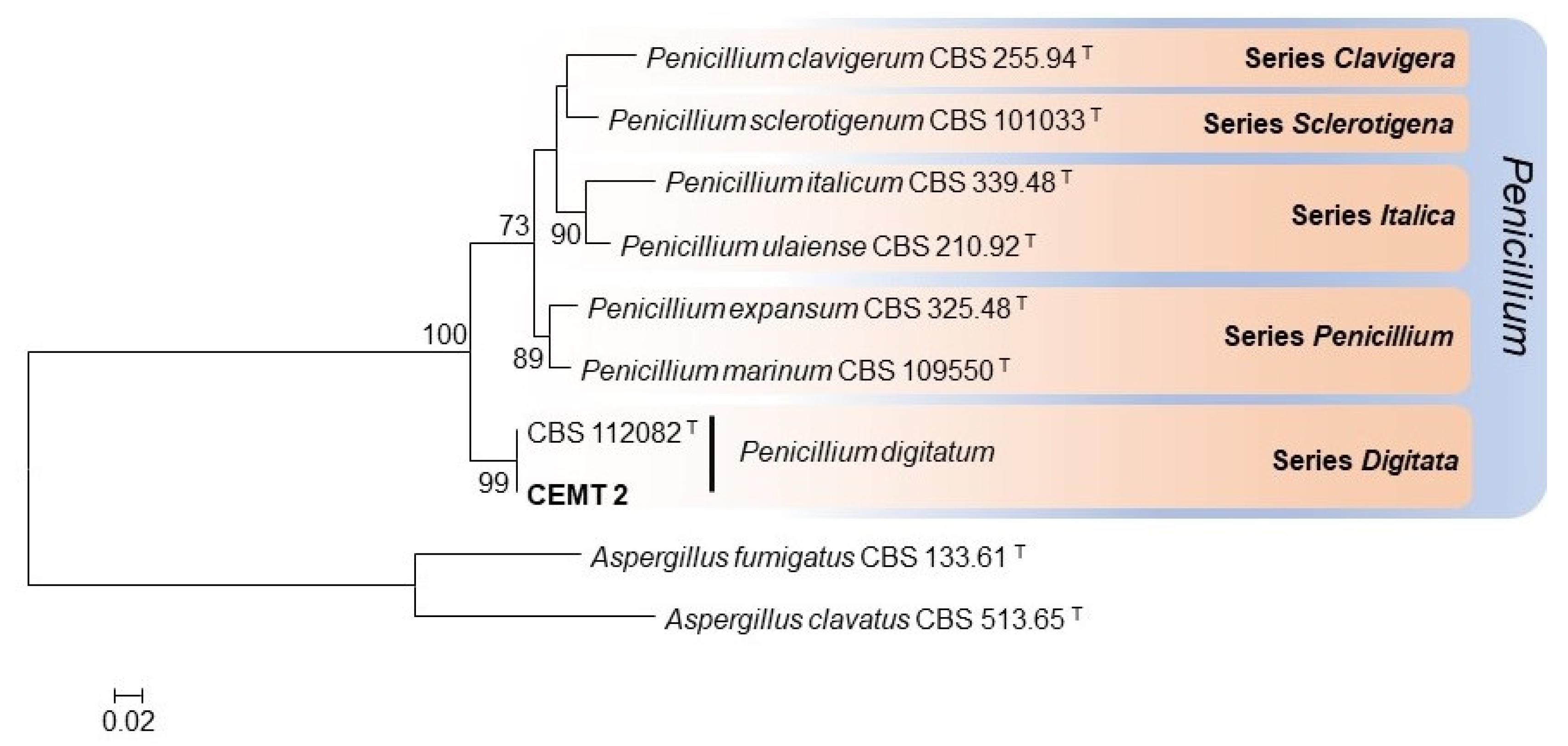
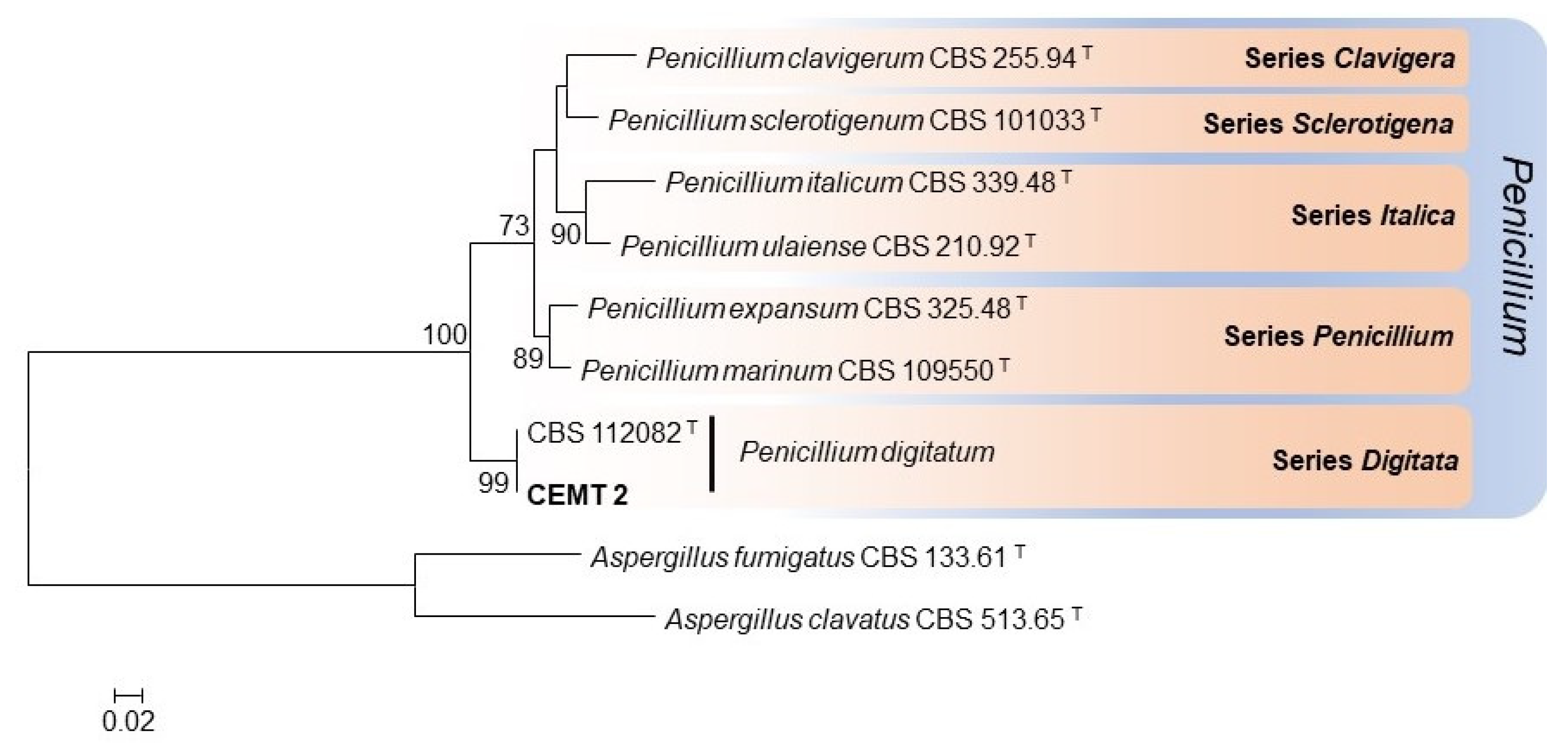
3.2. Molecular Identification and Phylogenetic Analysis
3.3. Results of In Vitro Antifungal Susceptibility Test
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Vilanova, L.; Viñas, I.; Torres, R.; Usall, J.; Jauset, A.; Teixidó, N. Infection capacities in the orange-pathogen relationship: Compatible (Penicillium digitatum) and incompatible (Penicillium expansum) interactions. Food Microbiol. 2012, 29, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Qian, X.; Dhanasekaran, S.; Boateng, N.A.S.; Yan, X.; Zhu, H.; He, F.; Zhang, H. Study on the Infection Mechanism of Penicillium digitatum on Postharvest Citrus (Citrus Reticulata Blanco) Based on Transcriptomics. Microorganisms 2019, 7, 672. [Google Scholar] [CrossRef] [PubMed]
- Ballester, A.R.; González-Candelas, L. EFE-Mediated Ethylene Synthesis Is the Major Pathway in the Citrus Postharvest Pathogen Penicillium digitatum during Fruit Infection. J. Fungi 2020, 6, 175. [Google Scholar] [CrossRef]
- Costa, J.H.; Bazioli, J.M.; Barbosa, L.D.; Júnior, P.L.T.D.S.; Reis, F.C.G.; Klimeck, T.; Crnkovic, C.M.; Berlinck, R.G.S.; Sussulini, A.; Rodrigues, M.L.; et al. Phytotoxic Tryptoquialanines Produced In Vivo by Penicillium digitatum Are Exported in Extracellular Vesicles. mBio 2021, 12, e03393-20. [Google Scholar] [CrossRef] [PubMed]
- Arai, M.; Hibino, T. Tumorigenicity of citrinin in male F344 rats. Cancer Lett. 1983, 17, 281–287. [Google Scholar] [CrossRef]
- Flajs, D.; Peraica, M. Toxicological properties of citrinin. Arh. Hig. Rada Toksikol. 2009, 60, 457–464. [Google Scholar] [CrossRef]
- Singh, N.D.; Sharma, A.K.; Patil, R.D.; Rahman, S.; Leishangthem, G.D.; Kumar, M. Effect of feeding graded doses of Citrinin on clinical and teratology in female Wistar rats. Indian J. Exp. Biol. 2014, 52, 159–167. [Google Scholar]
- Oshikata, C.; Tsurikisawa, N.; Saito, A.; Watanabe, M.; Kamata, Y.; Tanaka, M.; Tsuburai, T.; Mitomi, H.; Takatori, K.; Yasueda, H.; et al. Fatal Pneumonia Caused by Penicillium digitatum: A Case Report. BMC Pulm. Med. 2013, 13, 16. Available online: http://www.biomedcentral.com/1471-2466/13/16 (accessed on 23 March 2013). [CrossRef]
- Visagie, C.; Houbraken, J.; Frisvad, J.; Hong, S.-B.; Klaassen, C.; Perrone, G.; Seifert, K.; Varga, J.; Yaguchi, T.; Samson, R. Identification and nomenclature of the genus Penicillium. Stud. Mycol. 2014, 78, 343–371. [Google Scholar] [CrossRef]
- Houbraken, J.; Kocsubé, S.; Visagie, C.M.; Yilmaz, N.; Wang, X.-C.; Meijer, M.; Kraak, B.; Hubka, V.; Bensch, K.; Samson, R.A.; et al. Classification of Aspergillus, Penicillium, Talaromyces and related genera (Eurotiales): An overview of families, genera, subgenera, sections, series and species. Stud. Mycol. 2020, 95, 5–169. [Google Scholar] [CrossRef]
- Tamura, K.; Stecher, G.; Peterson, D.; Filipski, A.; Kumar, S. MEGA6: Molecular evolutionary genetics analysis version 6.0. Mol. Biol. Evol. 2013, 30, 2725–2729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, J.D.; Higgins, D.G.; Gibson, T.J. CLUSTAL W: Improving the sensitivity of progressive multiple sequence alignment through sequence weighting, position-specific gap penalties and weight matrix choice. Nucleic Acids Res. 1994, 22, 4673–4680. [Google Scholar] [CrossRef] [PubMed]
- Edgar, R.C. MUSCLE: Multiple sequence alignment with high accuracy and high throughput. Nucleic Acids Res. 2004, 32, 1792–1797. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi; Approved Standard-Second Edition, CLSI document M38-A2; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Low, C.Y.; Rotstein, C. Emerging fungal infections in immunocompromised patients. F1000 Med. Rep. 2011, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Enoch, D.A.; Yang, H.; Aliyu, S.H.; Micallef, C. The Changing Epidemiology of Invasive Fungal Infections. Methods Mol. Biol. 2017, 1508, 17–65. [Google Scholar] [PubMed]
- Denning, D.W.; Chakrabarti, A. Pulmonary and sinus fungal diseases in non-immunocompromised patients. Lancet Infect. Dis. 2017, 17, e357–e366. [Google Scholar] [CrossRef]
- Adulkar, N.G.; Radhakrishnan, S.; Vidhya, N.; Kim, U. Invasive sino-orbital fungal infections in immunocompetent patients: A clinico-pathological study. Eye 2019, 33, 988–994. [Google Scholar] [CrossRef]
- Rudramurthy, S.M.; Singh, S. Candida Infections in Immunocompetent Hosts: Pathogenesis and Diagnosis. Curr. Fungal Infect. Rep. 2020, 14, 233–245. [Google Scholar] [CrossRef]
- Cao, X.-G.; Yu, C.-W.; Zhou, S.-S.; Huang, Y.; Wang, C.-Y. Case Report: A Candida Meningitis in an Immunocompetent Patient Detected Through the Next-Generation Sequencing. Front. Med. 2021, 22, 656066. [Google Scholar] [CrossRef]
- He, J.; Sheng, G.; Yue, H.; Zhang, F.; Zhang, H.-L. Isolated pulmonary mucormycosis in an immunocompetent patient: A case report and systematic review of the literature. BMC Pulm. Med. 2021, 21, 138. [Google Scholar] [CrossRef]
- Kumar, S.; Muthu, V.; Bansal, Y.S.; Mehta, N.; Arora, V. Invasive pulmonary aspergillosis with brain dissemination in an immunocompetent host. Autops. Case Rep. 2021, 11, e2021280. [Google Scholar] [CrossRef] [PubMed]
- Arastehfar, A.; Carvalho, A.; Van De Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; Perlin, D.S.; Lass-Flörl, C.; Hoenigl, M. COVID-19 Associated Pulmonary Aspergillosis (CAPA)–From Immunology to Treatment. J. Fungi 2020, 6, 91. [Google Scholar] [CrossRef] [PubMed]
- Salmanton-García, J.; Sprute, R.; Stemler, J.; Bartoletti, M.; Dupont, D.; Valerio, M.; Garcia-Vidal, C.; Falces-Romero, I.; Machado, M.; de la Villa, S.; et al. COVID-19-Associated Pulmonary Aspergillosis, March-August 2020. Emerg. Infect. Dis. 2021, 27, 1077–1086. [Google Scholar] [CrossRef] [PubMed]
- Chaharom, F.E.; Pourafkari, L.; Chaharom, A.A.E.; Nader, N.D. Effects of corticosteroids on Covid-19 patients: A systematic review and meta-analysis on clinical outcomes. Pulm. Pharmacol. Ther. 2022, 72, 102107. [Google Scholar] [CrossRef]
- Närhi, F.; Moonesinghe, S.R.; Shenkin, S.D.; Drake, T.M.; Mulholland, R.H.; Donegan, C.; Dunning, J.; Fairfield, C.J.; Girvan, M.; Hardwick, H.E.; et al. Implementation of corticosteroids in treatment of COVID-19 in the ISARIC WHO Clinical Characterisation Protocol UK: Prospective, cohort study. Lancet Digit. Health 2022, 4, e220–e234. [Google Scholar] [CrossRef]
- Tan, Y.P.; Crous, P.W.; Shivas, R.G. Cryptic species of Curvularia in the culture collection of the Queensland Plant Pathology Herbarium. MycoKeys 2018, 35, 1–25. [Google Scholar] [CrossRef]
- Lyratzopoulos, G.; Ellis, M.; Nerringer, R.; Denning, D. Invasive infection due to Penicillium species other than P. marneffei. J. Infect. 2002, 45, 184–195. [Google Scholar] [CrossRef]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef]
- Baskaran, V.; Lawrence, H.; Lansbury, L.E.; Webb, K.; Safavi, S.; Zainuddin, N.I.; Huq, T.; Eggleston, C.; Ellis, J.; Thakker, C.; et al. Co-infection in critically ill patients with COVID-19: An observational cohort study from England. J. Med. Microbiol. 2021, 70, 001350. [Google Scholar] [CrossRef]
- Peng, J.; Wang, Q.; Mei, H.; Zheng, H.; Liang, G.; She, X.; Liu, W. Fungal co-infection in COVID-19 patients: Evidence from a systematic review and meta-analysis. Aging 2021, 13, 7745–7757. [Google Scholar] [CrossRef]
- Yang, S.; Hua, M.; Liu, X.; Du, C.; Pu, L.; Xiang, P.; Wang, L.; Liu, J. Bacterial and fungal co-infections among COVID-19 patients in intensive care unit. Microbes Infect. 2021, 23, 104806. [Google Scholar] [CrossRef] [PubMed]
- Shafiekhani, M.; Shekari, Z.; Boorboor, A.; Zare, Z.; Arabsheybani, S.; Azadeh, N. Bacterial and fungal co-infections with SARS-CoV-2 in solid organ recipients: A retrospective study. Virol. J. 2022, 19, 35. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Cornely, O.A.; Böttiger, B.W.; Dusse, F.; Eichenauer, D.A.; Fuchs, F.; Hallek, M.; Jung, N.; Klein, F.; Persigehl, T.; et al. COVID-19 associated pulmonary aspergillosis. Mycoses 2020, 63, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Nasir, N.; Farooqi, J.; Mahmood, S.F.; Jabeen, K. COVID-19-associated pulmonary aspergillosis (CAPA) in patients admitted with severe COVID-19 pneumonia: An observational study from Pakistan. Mycoses 2020, 63, 766–770. [Google Scholar] [CrossRef]
- van Arkel, A.L.; Rijpstra, T.A.; Belderbos, H.N.; Van Wijngaarden, P.; Verweij, P.E.; Bentvelsen, R.G. COVID-19-associated Pulmonary Aspergillosis. Am. J. Respir. Crit. Care Med. 2020, 202, 132–135. [Google Scholar] [CrossRef]
- Latgé, J.P.; Kobayashi, H.; Debeaupuis, J.P.; Diaquin, M.; Sarfati, J.; Wieruszeski, J.M.; Parra, E.; Bouchara, J.P.; Fournet, B. Chemical and immunological characterization of the extracellular galactomannan of Aspergillus fumigatus. Infect. Immun. 1994, 62, 5424–5433. [Google Scholar] [CrossRef]
- Mercier, T.; Guldentops, E.; Lagrou, K.; Maertens, J. Galactomannan, a Surrogate Marker for Outcome in Invasive Aspergillosis: Finally Coming of Age. Front. Microbiol. 2018, 9, 661. [Google Scholar] [CrossRef]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Species | Strain | Substrate | Locality | β-tubulin GenBank Accession Numbers |
|---|---|---|---|---|
| Aspergillus fumigatus | CBS 133.61 T | Chicken, lung | USA | KF314730 |
| A. clavatus | CBS 513.65 T | Unknown | Unknown | EU076340 |
| Penicillium clavigerum | CBS 255.94 T | Man | Canada | AY674427 |
| P. expansum | CBS 325.48 T | Malus sylvestris, fruit | USA | AY674400 |
| P. digitatum | CBS 112082 T | Citrus limon | Italy | KJ834447 |
| CEMT 2 | Human Bronchoalveolar Lavage | Chile | OP046418 | |
| P. italicum | CBS 339.48 T | Citrus sp., fruit | USA | AY674398 |
| P. marinum | CBS 109550 T | Sandy soil | Japan | AY674392 |
| P. sclerotigenum | CBS 101033 T | Dioscorea batatas, rotting tuber | Japan | AY674393 |
| P. ulaiense | CBS 210.92 T | skin of decaying orange | Taiwan | AY674408 |
| Fungal Strain | Antifungal | MIC (µg/mL) |
|---|---|---|
| Penicillium digitatum CEMT-2 | Amphotericin B | 2 |
| Voriconazole | 2 | |
| Itraconazole | 4 | |
| Fusarium oxysporum ATCC 36031 | Amphotericin B | 2 |
| Voriconazole | 16 | |
| Itraconazole | >32 | |
| Fusarium keratoplasticum ATCC 48112 | Amphotericin B | 4 |
| Voriconazole | 32 | |
| Itraconazole | >32 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iturrieta-González, I.; Giacaman, A.; Godoy-Martínez, P.; Vega, F.; Sepúlveda, M.; Santos, C.; Toledo, V.; Rivera, G.; Ortega, L.; San Martín, A.; et al. Penicillium digitatum, First Clinical Report in Chile: Fungal Co-Infection in COVID-19 Patient. J. Fungi 2022, 8, 961. https://doi.org/10.3390/jof8090961
Iturrieta-González I, Giacaman A, Godoy-Martínez P, Vega F, Sepúlveda M, Santos C, Toledo V, Rivera G, Ortega L, San Martín A, et al. Penicillium digitatum, First Clinical Report in Chile: Fungal Co-Infection in COVID-19 Patient. Journal of Fungi. 2022; 8(9):961. https://doi.org/10.3390/jof8090961
Chicago/Turabian StyleIturrieta-González, Isabel, Annesi Giacaman, Patricio Godoy-Martínez, Fernando Vega, Marcela Sepúlveda, Cledir Santos, Valentina Toledo, Gonzalo Rivera, Leandro Ortega, Andrés San Martín, and et al. 2022. "Penicillium digitatum, First Clinical Report in Chile: Fungal Co-Infection in COVID-19 Patient" Journal of Fungi 8, no. 9: 961. https://doi.org/10.3390/jof8090961
APA StyleIturrieta-González, I., Giacaman, A., Godoy-Martínez, P., Vega, F., Sepúlveda, M., Santos, C., Toledo, V., Rivera, G., Ortega, L., San Martín, A., Bahamondes, V., Collao, F., Sánchez, R., & Fonseca-Salamanca, F. (2022). Penicillium digitatum, First Clinical Report in Chile: Fungal Co-Infection in COVID-19 Patient. Journal of Fungi, 8(9), 961. https://doi.org/10.3390/jof8090961