
Performance of LDBio Aspergillus WB and ICT Antibody Detection in Chronic Pulmonary Aspergillosis

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patients and Clinical Characteristics
3.2. Culture Results
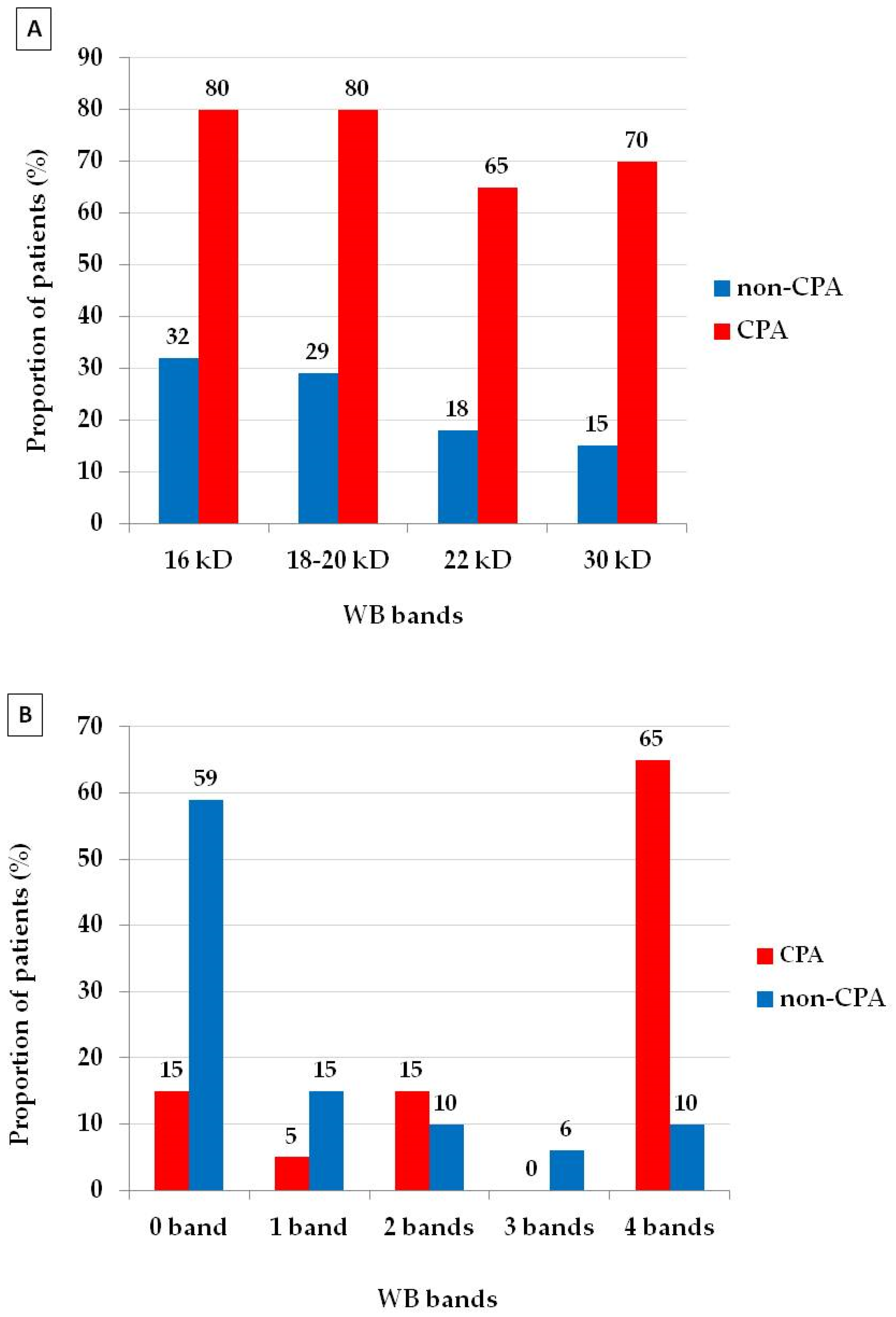
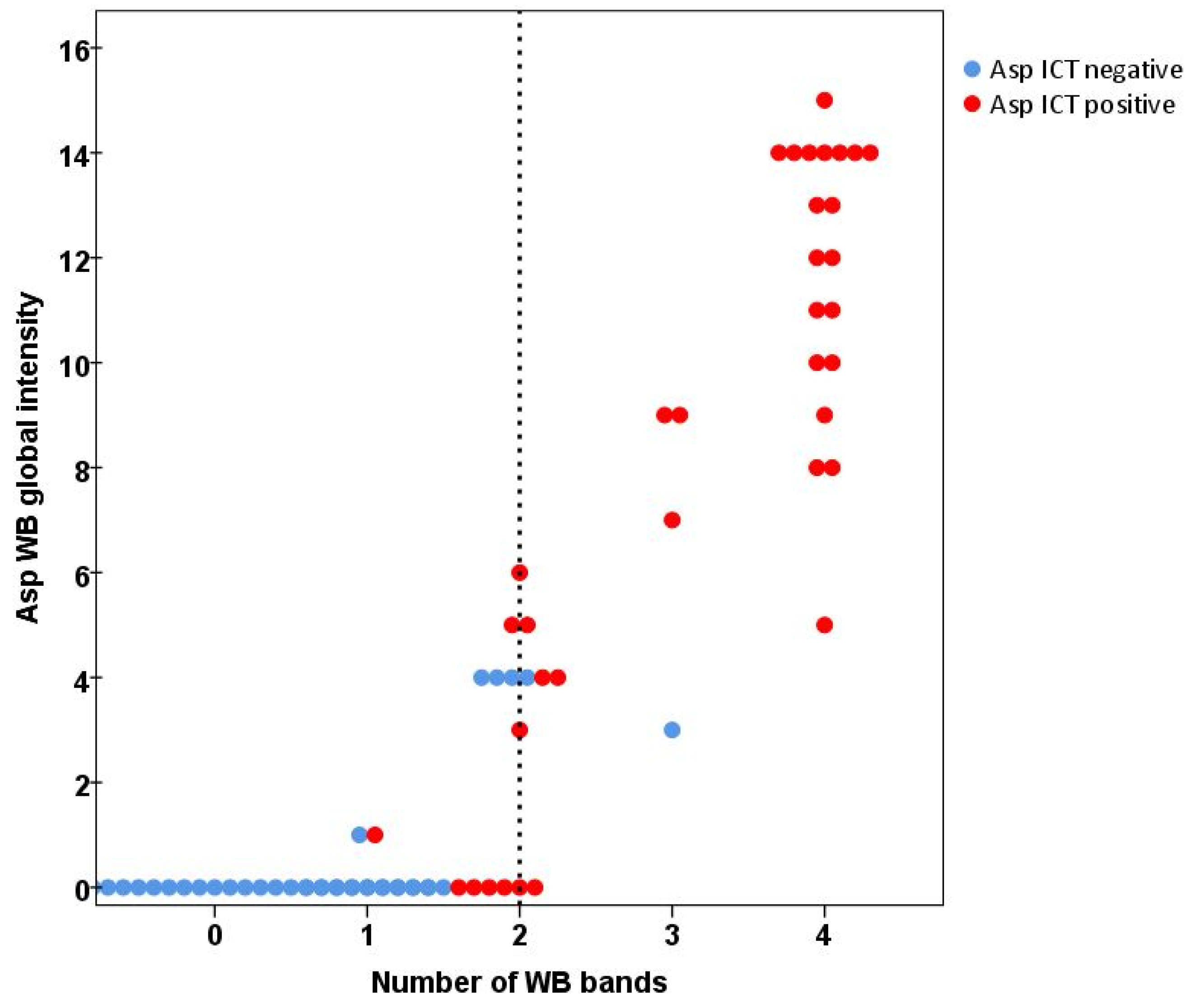
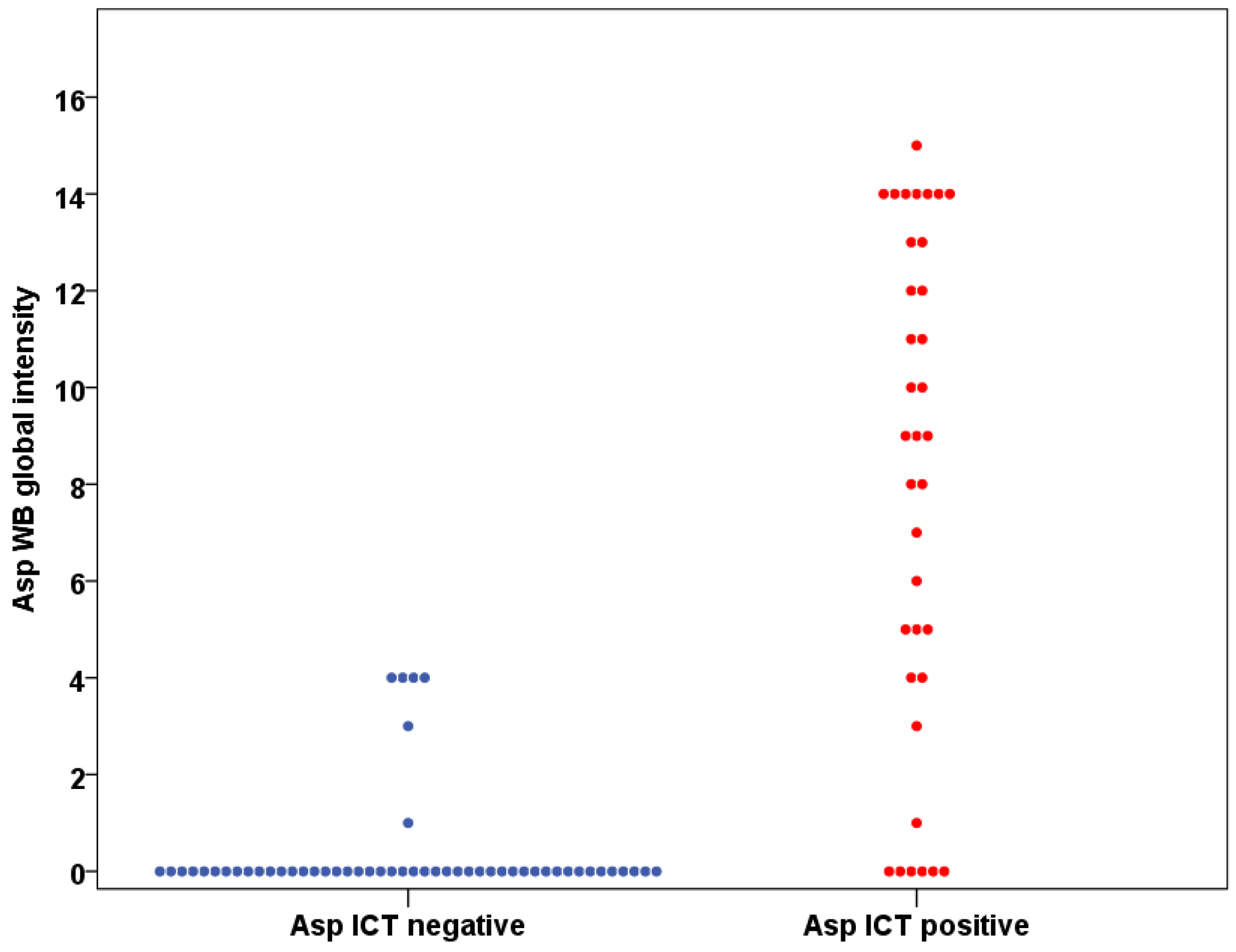
3.3. Western Blot and ICT Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Denning, D.W.; Pleuvry, A.; Cole, D.C. Global Burden of Chronic Pulmonary Aspergillosis as a Sequel to Pulmonary Tuberculosis. Bull. World Health Organ. 2011, 89, 864–872. [Google Scholar] [CrossRef]
- Kosmidis, C.; Denning, D.W. The Clinical Spectrum of Pulmonary Aspergillosis. Thorax 2015, 70, 270–277. [Google Scholar] [CrossRef]
- Lowes, D.; Al-Shair, K.; Newton, P.J.; Morris, J.; Harris, C.; Rautemaa-Richardson, R.; Denning, D.W. Predictors of Mortality in Chronic Pulmonary Aspergillosis. Eur. Respir. J. 2017, 49, 1–10. [Google Scholar] [CrossRef]
- Setianingrum, F.; Rozaliyani, A.; Syam, R.; Adawiyah, R.; Tugiran, M.; Sari, C.Y.I.; Burhan, E.; Wahyuningsih, R.; Rauteema-Richradson, R.; Denning, D.W. Evaluation and Comparison of Automated and Manual ELISA for Diagnosis of Chronic Pulmonary Aspergillosis (CPA) in Indonesia. Diagnostic Microbiol. Infect. Dis. 2020, 98, 1–6. [Google Scholar] [CrossRef]
- Denning, D.W.; Page, I.; Chakaya, J.; Jabeen, K.; Jude, C.M.; Cornet, M.; Alastruey-Izquierdo, A.; Bongomin, F.; Bowyer, P.; Chakrabarti, A.; et al. Case Definition of Chronic Pulmonary Aspergillosis in Resource-Limited Settings: Catalysing Research and Clinical Care. Emerg. Infect. Dis. 2018, 24, e171312. [Google Scholar] [CrossRef]
- Denning, D.W.; Cadranel, J.; Beigelman-Aubry, C.; Ader, F.; Chakrabarti, A.; Blot, S.; Ullmann, A.J.; Dimopoulos, G.; Lange, C. Chronic Pulmonary Aspergillosis: Rationale and Clinical Guidelines for Diagnosis and Management. Eur. Respir. J. 2016, 47, 45–68. [Google Scholar] [CrossRef]
- Richardson, M.; Page, I. Role of Serological Tests in the Diagnosis of Mold Infections. Curr. Fungal Infect. Rep. 2018, 12, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Oliva, A.; Flori, P.; Hennequin, C.; Dubus, J.C.; Reynaud-Gaubert, M.; Charpin, D.; Vergnon, J.M.; Gay, P.; Colly, A.; Piarroux, R.; et al. Evaluation of the Aspergillus Western Blot IgG Kit for Diagnosis of Chronic Aspergillosis. J. Clin. Microbiol. 2015, 53, 248–254. [Google Scholar] [CrossRef]
- Stucky Hunter, E.; Richardson, M.D.; Denning, D.W. Evaluation of LDBio Aspergillus ICT Lateral Flow Assay for IgG and IgM Antibody Detection in Chronic Pulmonary Aspergillosis. J. Clin. Microbiol. 2019, 57, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rozaliyani, A.; Rosianawati, H.; Handayani, D.; Agustin, H.; Zaini, J.; Syam, R.; Adawiyah, R.; Tugiran, M.; Setianingrum, F.; Burhan, E.; et al. Chronic Pulmonary Aspergillosis in Post Tuberculosis Patients in Indonesia and the Role of Ldbio Aspergillus Ict as Part of the Diagnosis Scheme. J. Fungi 2020, 6, 318. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Otu, A.; Harris, C.; Foden, P.; Kosmidis, C.; Denning, D.W. Risk Factors for Relapse of Chronic Pulmonary Aspergillosis after Discontinuation of Antifungal Therapy. Clin. Infect. Pract. 2020, 5, 100015. [Google Scholar] [CrossRef]
- Setianingrum, F.; Rautemaa-Richardson, R.; Shah, R.; Denning, D.W. Clinical Outcomes of Patients with Chronic Pulmonary Aspergillosis Managed Surgically. Eur. J. Cardio Thorac. Surg. 2020, 58, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Bongomin, F.; Harris, C.; Hayes, G.; Kosmidis, C.; Denning, D.W. Twelve-Month Clinical Outcomes of 206 Patients with Chronic Pulmonary Aspergillosis. PLoS ONE 2018, 13, 1–17. [Google Scholar] [CrossRef]
- Vergidis, P.; Moore, C.B.; Novak-Frazer, L.; Rautemaa-Richardson, R.; Walker, A.; Denning, D.W.; Richardson, M.D. High-Volume Culture and Quantitative Real-Time PCR for the Detection of Aspergillus in Sputum. Clin. Microbiol. Infect. 2020, 26, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Lee, W. Does McNemar’s Test Compare the Sensitivities and Specificities of Two Diagnostic Tests? Stat. Methods Med. Res. 2017, 26, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Viera, A.J.; Garrett, J.M. Understanding Interobserver Agreement: The Kappa Statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar]
- Hunter, E.S.; Wilopo, B.; Richardson, M.D.; Kosmidis, C.; Denning, D.W. Effect of Patient Immunodeficiencies on the Diagnostic Performance of Serological Assays to Detect Aspergillus -Specific Antibodies in Chronic Pulmonary Aspergillosis. Respir. Med. 2021, 178, 106290. [Google Scholar] [CrossRef]
- Kauffman, H.; van der Heide, S.; Beaumont, F.; Blok, H.; de Vries, K. Class-Specific Antibody Determintaion against Aspergillus Fumigatus by Means of the Enzyme-Linked Immunosorbent Assay. Int. Archs Allergy appl. Immun. 1986, 80, 300–306. [Google Scholar] [CrossRef]
- Kostiala, A.I.; Stenius-aarniala, B.; Alanko, K. Analysis of Antibodies to Aspergillus Fumigatus Antigens by Class-Specific Enzyme-Linked Immunosorbent Assay in Patients with Pulmonary Aspergillosis. Diagn. Microbiol. Infect. Dis. 1984, 2, 37–49. [Google Scholar] [CrossRef]
- Weig, M.; Frosch, M.; Tintelnot, K.; Haas, A.; Groß, U.; Linsmeier, B.; Heesemann, J. Use of Recombinant Mitogillin for Improved Serodiagnosis of Aspergillus Fumigatus-Associated Diseases. J. Clin. Microbiol. 2001, 39, 1721–1730. [Google Scholar] [CrossRef]
- Bozza, S.; Clavaud, C.; Giovannini, G.; Beauvais, A.; Sarfati, J.; Angelo, D.; Perruccio, K.; Bonifazi, P.; Moretti, S.; Bistoni, F.; et al. Immune Sensing of Aspergillus Fumigatus Proteins, Glycolipids, and Polysaccharides and the Impact on Th Immunity and Vaccination. J. Immunol. 2009, 183, 2407–2414. [Google Scholar] [CrossRef]
- Page, I.D.; Richardson, M.; Denning, D.W. Antibody Testing in Aspergillosis--Quo Vadis? Med. Mycol. 2015, 53, 417–439. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Bai, Y.; Yang, C.; Gu, L. Evaluation of Aspergillus IgG, IgM Antibody for Diagnosing in Chronic Pulmonary Aspergillosis: A Prospective Study from a Single Center in China. Medicine 2019, 98, e15021. [Google Scholar] [CrossRef]
- Iqbal, N.; Irfan, M.; Bin, A.; Zubairi, S.; Jabeen, K.; Awan, S.; Khan, J.A. Clinical Manifestations and Outcomes of Pulmonary Aspergillosis: Experience from Pakistan. BMJ Open Respir. Res. 2016, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bekele, A.; Ali, A.; Biluts, H. Surgically Treated Pulmonary Tuberculosis: Report on Cases from Tikur Anbess Hospital, Addis Ababa, Ethiopia. Ethiop. Med. J. 2008, 46, 261–266. [Google Scholar] [PubMed]
- Setianingrum, F.; Rozaliyani, A.; Adawiyah, R.; Syam, R.; Tugiran, M.; Sari, C.Y.I.; Nandipinto, F.; Ramnath, J.; Arifin, A.R.; Handayani, D.; et al. A Prospective Longitudinal Study of Chronic Pulmonary Aspergillosis in Pulmonary Tuberculosis in Indonesia (APICAL). Thorax. Manuscript Submitted.
- Kuwabara, K.; Hirose, M.; Kato, K.; Yokoi, T.; Shiga, M.; Kondo, R.; Nakamura, M.; Matsunaga, K. Serological Analysis of Sensitization in Allergic Bronchopulmonary Aspergillosis: A Study on Allergen Components and Interspecies Relationships. J. Asthma 2020, 57, 610–617. [Google Scholar] [CrossRef]
- Lee, M.; Huang, H.; Chen, L.; Yang, H.; Ko, J.; Cheng, M.; Chong, I.; Lee, L.; Wang, J.; Dimopoulos, G. Seroprevalence of Aspergillus IgG and Disease Prevalence of Chronic Pulmonary Aspergillosis in a Country with Intermediate Burden of Tuberculosis: A Prospective Observational Study. Clin. Microbiol. Infect. 2019, 26, 1091.e1–1091.e7. [Google Scholar] [CrossRef]
- Severo, L.; Londero, A.; Geyer, G.; Picon, P. Oxalosis Associated with An Aspergillus Niger Fungus Ball. Report of A Case. Mycopathologia 1981, 73, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Severo, L.C.; Geyer, G.R.; Porto, N.S.; Micologia, S.D.; Bioldgicas, I.D.P.; Domingos, R. Pulmonary Aspergillus Intracavitary Colonization (PAIC). Mycopathologia 1990, 112, 93–104. [Google Scholar] [CrossRef]
- Severo, L.; Geyer, G.; Porto, N.; Wagner, M.; Londero, A. Pulmonary Aspergillus Niger Intracavitary Colonization. Report of 23 Cases and a Review of the Literature. Rev. Iberoam. Micol. 1997, 14, 104–110. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All (n = 88) | CPA (n = 20) | Non CPA(n = 68) | p-Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 61 (69%) | 14 (70%) | 47 (69%) | |
| Female | 27 (31%) | 6 (30%) | 21 (31%) | 0.940 |
| Age, mean (range) | 49 (18–79) | 50 (28–66) | 49 (18–79) | 0.919 |
| Chronic diseases | ||||
| Diabetes mellitus | 11 (13%) | 7 (39%) | 4 (6%) | 0.002 |
| Hypertension | 8 (9%) | 1 (6%) | 7 (10%) | 0.676 |
| Asthma | 6 (7%) | 1 (6%) | 5 (7%) | 1 |
| Chronic obstructive pulmonary disease | 9 (10%) | 2 (11%) | 7 (10%) | 1 |
| Duration of TB therapy (range), months | 9 (2–26) | 13 (9–17) | 8 (7–9) | <0.001 |
| TB therapy >6 months | 34 (39%) | 13 (65%) | 21 (31%) | 0.007 |
| Time from end of TB therapy to recruitment (months), median (range) | 8.5 (1–244) | 5 (1–56) | 9 (1–244) | 0.245 |
| Smoking history | 50 (57%) | 14 (70%) | 36 (53%) | 0.176 |
| Test | % Sensitivity (95% CI) | % Specificity (95% CI) | AUC ROC |
|---|---|---|---|
| Western blot | 80 (56.3–94.3) | 73.5 (61.4–83.5) | 0.768 |
| ICT | 85 (62.1–96.8) | 72.1 (59.9–82.3) | 0.785 |
| Western blot + ICT | 80 (56.3–94.3) | 80.9 (69.5–89.4) | 0.804 |
| All (n = 88) | CPA (n = 20) | Non-CPA (n = 68) | p-Value | |
|---|---|---|---|---|
| WB Global intensity | ||||
| Median | 0 | 10.5 | 0 | <0.001 |
| Mean (95% CI) | 3.5 (2.4–4.6) | 8.75 (6.1–11.4) | 2 (1.1–2.8) | |
| Interquartile range | 0–6.75 | 3.25–14 | 0–3.75 | |
| Maximum | 0 | 0 | 0 | |
| Minimum | 15 | 15 | 15 | |
| Number of symptoms | ||||
| Median | 1.5 | 2 | 1 | 0.005 |
| Mean | 1.6 (1.3–1.9) | 2.3 (1.8–2.8) | 1.4 (1.1–1.7) | |
| Interquartile range | 0–3 | 2–3 | 0–2 | |
| Maximum | 0 | 0 | 0 | |
| Minimum | 5 | 5 | 4 | |
| WB global intensity & number of symptoms correlation (p) | 0.010 | 0.001 | 0.752 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rozaliyani, A.; Setianingrum, F.; Azahra, S.; Abdullah, A.; Fatril, A.E.; Rosianawati, H.; Burhan, E.; Handayani, D.; Arifin, A.R.; Zaini, J.; et al. Performance of LDBio Aspergillus WB and ICT Antibody Detection in Chronic Pulmonary Aspergillosis. J. Fungi 2021, 7, 311. https://doi.org/10.3390/jof7040311
Rozaliyani A, Setianingrum F, Azahra S, Abdullah A, Fatril AE, Rosianawati H, Burhan E, Handayani D, Arifin AR, Zaini J, et al. Performance of LDBio Aspergillus WB and ICT Antibody Detection in Chronic Pulmonary Aspergillosis. Journal of Fungi. 2021; 7(4):311. https://doi.org/10.3390/jof7040311
Chicago/Turabian StyleRozaliyani, Anna, Findra Setianingrum, Sresta Azahra, Asriyani Abdullah, Ayu Eka Fatril, Harmi Rosianawati, Erlina Burhan, Diah Handayani, Arief Riadi Arifin, Jamal Zaini, and et al. 2021. "Performance of LDBio Aspergillus WB and ICT Antibody Detection in Chronic Pulmonary Aspergillosis" Journal of Fungi 7, no. 4: 311. https://doi.org/10.3390/jof7040311
APA StyleRozaliyani, A., Setianingrum, F., Azahra, S., Abdullah, A., Fatril, A. E., Rosianawati, H., Burhan, E., Handayani, D., Arifin, A. R., Zaini, J., Tugiran, M., Adawiyah, R., Syam, R., Wibowo, H., Wahyuningsih, R., Kosmidis, C., & Denning, D. W. (2021). Performance of LDBio Aspergillus WB and ICT Antibody Detection in Chronic Pulmonary Aspergillosis. Journal of Fungi, 7(4), 311. https://doi.org/10.3390/jof7040311