Breakthrough Bloodstream Infections Caused by Echinocandin-Resistant Candida tropicalis: An Emerging Threat to Immunocompromised Patients with Hematological Malignancies


Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Review
2.2. Organisms
2.3. In Vitro Antifungal Susceptibility Testing
2.4. FKS Sequencing
3. Results
3.1. Index Case 1
3.2. Index Case 2
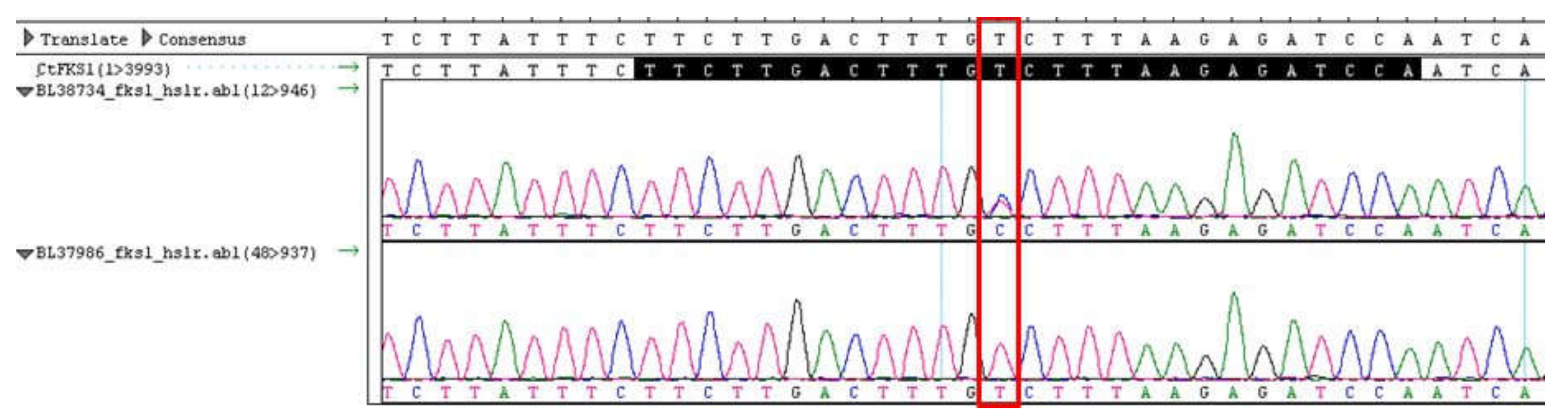
3.3. Molecular Mechanisms of Resistance
3.4. Review of Cases
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Pfaller, M.A.; Diekema, D.J. Epidemiology of Invasive Candidiasis: A Persistent Public Health Problem. Clin. Microbiol. Rev. 2007, 20, 133–163. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Executive Summary: Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Messer, S.A.; Jones, R.N.; Castanheira, M. Antifungal Susceptibilities of Candida, Cryptococcus Neoformans and Aspergillus Fumigatus from the Asia and Western Pacific Region: Data from the SENTRY Antifungal Surveillance Program (2010-2012). J. Antibiot. 2015, 68, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Zuza-Alves, D.L.; Silva-Rocha, W.P.; Chaves, G.M. An Update on Candida Tropicalis Based on Basic and Clinical Approaches. Front. Microbiol. 2017, 8, 1927. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-F.; Liu, W.-L.; Hsieh, M.-H.; Hii, I.-M.; Lee, Y.-L.; Lin, Y.-T.; Ho, M.-W.; Liu, C.-E.; Chen, Y.-H.; Wang, F.-D. Epidemiology and Antifungal Susceptibility of Candidemia Isolates of Non-Albicans Candida Species from Cancer Patients. Emerg. Microbes. Infect. 2017, 6, e87. [Google Scholar] [CrossRef] [PubMed]
- Wingard, J.R.; Merz, W.G.; Saral, R. Candida Tropicalis: A Major Pathogen in Immunocompromised Patients. Ann. Intern. Med. 1979, 91, 539–543. [Google Scholar] [CrossRef]
- Wingard, J.R.; Dick, J.D.; Merz, W.G.; Sandford, G.R.; Saral, R.; Burns, W.H. Pathogenicity of Candida Tropicalis and Candida Albicans after Gastrointestinal Inoculation in Mice. Infect. Immun. 1980, 29, 808–813. [Google Scholar]
- Sanitá, P.V.; Zago, C.E.; de Oliveira Mima, E.G.; Pavarina, C.E.; Jorge, J.H.; Machado, A.L.; Vergani, C.E. In Vitro Evaluation of the Enzymatic Activity Profile of Non-Albicans Candida Species Isolated from Patients with Oral Candidiasis with or without Diabetes. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2014, 118, 84–91. [Google Scholar] [CrossRef]
- Kothavade, R.J.; Kura, M.M.; Valand, A.G.; Panthaki, M.H. Candida Tropicalis: Its Prevalence, Pathogenicity and Increasing Resistance to Fluconazole. J. Med. Microbiol. 2010, 59, 873–880. [Google Scholar] [CrossRef]
- Andes, D.R.; Safdar, N.; Baddley, J.W.; Alexander, B.; Brumble, L.; Freifeld, A.; Hadley, S.; Herwaldt, L.; Kauffman, C.; Lyon, G.M.; et al. The Epidemiology and Outcomes of Invasive Candida Infections among Organ Transplant Recipients in the United States: Results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Transpl. Infect. Dis. 2016, 18, 921–931. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Lewis, R.E. Antifungal Drug Resistance of Pathogenic Fungi. Lancet 2002, 359, 1135–1144. [Google Scholar] [CrossRef]
- Desnos-Ollivier, M.; Bretagne, S.; Raoux, D.; Hoinard, D.; Dromer, F.; Dannaoui, E.; European Committee on Antibiotic Susceptibility Testing. Mutations in the Fks1 Gene in Candida Albicans, C. Tropicalis, and C. Krusei Correlate with Elevated Caspofungin MICs Uncovered in AM3 Medium Using the Method of the European Committee on Antibiotic Susceptibility Testing. Antimicrob. Agents Chemother. 2008, 52, 3092–3098. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Effron, G.; Kontoyiannis, D.P.; Lewis, R.E.; Perlin, D.S. Caspofungin-Resistant Candida Tropicalis Strains Causing Breakthrough Fungemia in Patients at High Risk for Hematologic Malignancies. Antimicrob. Agents Chemother. 2008, 52, 4181–4183. [Google Scholar] [CrossRef] [PubMed]
- Jensen, R.H.; Johansen, H.K.; Arendrup, M.C. Stepwise Development of a Homozygous S80P Substitution in Fks1p, Conferring Echinocandin Resistance in Candida Tropicalis. Antimicrob. Agents Chemother. 2013, 57, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Kofteridis, D.P.; Lewis, R.E.; Kontoyiannis, D.P. Caspofungin-Non-Susceptible Candida Isolates in Cancer Patients. J. Antimicrob. Chemother. 2010, 65, 293–295. [Google Scholar] [CrossRef][Green Version]
- Pfeiffer, C.D.; Garcia-Effron, G.; Zaas, A.K.; Perfect, J.R.; Perlin, D.S.; Alexander, B.D. Breakthrough Invasive Candidiasis in Patients on Micafungin. J. Clin. Microbiol. 2010, 48, 2373–2380. [Google Scholar] [CrossRef]
- Grosset, M.; Desnos-Ollivier, M.; Godet, C.; Kauffmann-Lacroix, C.; Cazenave-Roblot, F. Recurrent Episodes of Candidemia Due to Candida Glabrata, Candida Tropicalis and Candida Albicans with Acquired Echinocandin Resistance. Med. Mycol. Case Rep. 2016, 14, 20–23. [Google Scholar] [CrossRef]
- Xiao, M.; Fan, X.; Hou, X.; Chen, S.C.; Wang, H.; Kong, F.; Sun, Z.-Y.; Chu, Y.-Z.; Xu, Y.-C. Clinical Characteristics of the First Cases of Invasive Candidiasis in China Due to Pan-Echinocandin-Resistant Candida Tropicalis and Candida Glabrata Isolates with Delineation of Their Resistance Mechanisms. Infect. Drug. Resist. 2018, 11, 155–161. [Google Scholar] [CrossRef]
- Khan, Z.; Ahmad, S.; Mokaddas, E.; Meis, J.F.; Joseph, L.; Abdullah, A.; Vayalil, S. Development of Echinocandin Resistance in Candida Tropicalis Following Short-Term Exposure to Caspofungin for Empiric Therapy. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef]
- Muñoz, P.; Giannella, M.; Fanciulli, C.; Guinea, J.; Valerio, M.; Rojas, L.; Rodríguez-Créixems, M.; Bouza, E. Candida Tropicalis Fungaemia: Incidence, Risk Factors and Mortality in a General Hospital. Clin. Microbiol. Infect. 2011, 17, 1538–1545. [Google Scholar] [CrossRef]
- Alexander, B.D.; Johnson, M.D.; Pfeiffer, C.D.; Jiménez-Ortigosa, C.; Catania, J.; Booker, R.; Castanheira, M.; Messer, S.A.; Perlin, D.S.; Pfaller, M.A. Increasing Echinocandin Resistance in Candida Glabrata: Clinical Failure Correlates with Presence of FKS Mutations and Elevated Minimum Inhibitory Concentrations. Clin. Infect. Dis. 2013, 56, 1724–1732. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Merz, W.G. Pathologic Features in the Human Alimentary Tract Associated with Invasiveness of Candida Tropicalis. Am. J. Clin. Pathol. 1986, 85, 498–502. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Diekema, D.J.; Andes, D.; Arendrup, M.C.; Brown, S.D.; Lockhart, S.R.; Motyl, M.; Perlin, D.S.; CLSI Subcommittee for Antifungal Testing. Clinical Breakpoints for the Echinocandins and Candida Revisited: Integration of Molecular, Clinical, and Microbiological Data to Arrive at Species-Specific Interpretive Criteria. Drug Resist. Updat. 2011, 14, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.J.; Finberg, R.W.; Arndt, C.; Hiemenz, J.; Schwartz, C.; Bodensteiner, D.; Pappas, P.; Seibel, N.; Greenberg, R.N.; Dummer, S.; et al. Liposomal Amphotericin B for Empirical Therapy in Patients with Persistent Fever and Neutropenia. National Institute of Allergy and Infectious Diseases Mycoses Study Group. N. Engl. J. Med. 1999, 340, 764–771. [Google Scholar] [CrossRef]
- CLSI. M27-S4 Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts: 4th Informational Supplement; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2012. [Google Scholar]
- CLSI. Performance Standards for Antifungal Susceptibility Testing of Yeasts, 1st ed.; CLSI Supplement M60; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017. [Google Scholar]



{kind=link}
{kind=link}
| Organism | Hot Spot 1 Forward Primer (5’-3’) | Hot Spot 1 Reverse Primer (5’–3’) * | Hot Spot 2 Forward Primer (5’–3’) * | Hot Spot 2 Forward Primer (5’–3’) |
|---|---|---|---|---|
| C. tropicalis | AATGGGCTGGTGCTCAACAT | CCTTCAATTTCAGATGGAACTTGATG | AAGATTGGTGCTGGTATGGG | TAATGGTGCTTGCCAATGAG |
| Published Case, Year of Publication | Age | Sex | Underlying Condition | Source | Antifungal Treatment in the Previous 3 Months | ANF MIC | CAS MIC | MCF MIC | FLU MIC | ITR MIC | VOR MIC | POS MIC | AMP MIC | 5FC MIC | FKS1 Hot Spot Sequence Analysis | Antifungal Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grosset M. et al., Med Mycol Case Rep. 2016 | 37 | M | Tuberculosis | blood | caspofungin then voriconazole | 0.5 | 4 | 0.5 | 0.5 | NA | 0.06 | 0.06 | 0.06 | 0.124 | FKS1-S645P | liposomal amphotericin B and flucytosine then voriconazole | survived |
| Jensen R. et al., Antimicrob Agents Chemother. 2013 | 51 | F | ALL | blood | voriconazole then caspofungin | 0.25 | >32 | 1 | 0.5 | ≤0.03 | ≤0.03 | ≤0.03 | 0.5 | NA | FKS1-S80S/P | amphotericin B | survived |
| Garcia-Effron G. et al., Antimicrob Agents Chemother. 2008 | 84 | M | ALL | blood | caspofungin | 2 | 4 | 2 | 8 | 0.5 | 1 | 0.25 | NA | NA | FKS1- S645P | voriconazole | survived |
| Garcia-Effron G. et al., Antimicrob Agents Chemother. 2008 | 59 | M | Large-cell lymphoma-allo-HSCT | blood | caspofungin | 1 | 4 | 2 | 32 | 1 | 2 | 1 | NA | NA | FKS1- F641L | liposomal amphotericin B | survived |
| Garcia-Effron G. et al., Antimicrob Agents Chemother. 2008 | 45 | M | Hodgkin lymphoma, renal cell carcinoma, esophageal cancer | blood | caspofungin | 0.5 | 1 | 0.5 | 0.5 | 0.125 | 0.03 | 0.06 | NA | NA | FKS1- S645P | fluconazole | died |
| Garcia-Effron G. et al., Antimicrob Agents Chemother. 2010 | 28 | F | AML | blood | caspofungin | 1 | 4 | 1 | 1 | NA | NA | NA | NA | NA | FKS1-F641S | fluconazole | survived |
| Pfeiffer CD et al., J Clin Microbiol. 2010 | 65 | F | Bilateral lung transplant recipient | blood | micafungin | 4, 2 | 8, 4 | 2,2 | NA | NA | NA | NA | NA | NA | FKS1- S80S/P | amphotericin B lipid complex | died |
| Pfeiffer CD et al., J Clin Microbiol. 2010 | 45 | F | Ventral hernia | blood, pleural fluid | micafungin | 0.12 | 0.25 | 0.06 | NA | NA | NA | NA | NA | NA | None | amphotericin B lipid complex | died |
| Kofteridids D. et al., J Antimicrob Chemother.2010 | 60 | M | Large B cell lymphoma-HSCT | blood | voriconazole | NA | 8 | NA | 32 | NA | 1 | 2 | 0.5 | NA | NA | liposomal amphotericin + voriconazole | survived |
| Kofteridids D. et al., J Antimicrob Chemother. 2010 | 66 | F | AML- HSCT | blood | voriconazole | NA | 16 | NA | 1 | NA | 0.2 | 0.06 | 0.5 | NA | NA | voriconazole | survived |
| Kofteridids D. et al., J Antimicrob Chemother. 2010 | 84 | M | ALL, prostate cancer | blood | caspofungin | NA | 8 | NA | 8 | NA | 0.25 | 0.2 | 0.5 | NA | NA | caspofungin + voriconazole | survived |
| Khan Z. et al., Antimicrob Agents Chemother. 2018 | 34 | F | Multiple sclerosis on natalizumab | endotracheal secretions (two C. tropicalis isolates) | caspofungin | 1; 1 * | 16; 32 * | 0.5; 075 * | 1; 0.5* | 0.031; 0.063 * | 0.063; 0.125 * | 0.063; 0.016 * | 0.25; 0.25* | NA; NA* | FKS1-S654P (homozygous) | caspofungin | died |
| Xiao M. et al., Inf Drug Resis. 2018 | 69 | F | Asthma, pulmonary infection, coronary artery disease, multiple organ dysfunction | chest drainage | micafungin x18 days | 2 | 4 | 2 | 2 | 0.25 | 0.125 | 0.25 | 0.5 | ≤0.06 | FKS1-S80P | voriconazole | died |
| Index case #1 | 87 | M | Urothelial carcinoma | blood | micafungin | 1 | 4 | 2 | 128 | NA | 8 | 0.5 | 1 | 0.12 | FKS1-S654P | liposomal amphotericin B | survived |
| Index case #2. | 41 | F | AML | blood | micafungin | 2 | 16 | 4 | 1 | NA | 0.12 | 0.12 | 0.5 | 0.12 | FKS1-S654P | voriconazole | died |
| Characteristic | n = 15 (%) |
|---|---|
| Age, years, median ± SD | 59.5 ± 18.7 |
| Gender | |
| Male | 7 (47) |
| Female | 8 (53) |
| Comorbidities | |
| ALL * | 3 (20) |
| AML | 2 (13) |
| Lymphoma * | 3 (20) |
| Urothelial cancer | 1 (7) |
| Multiple sclerosis | 1 (7) |
| COPD/Candida lung infection | 1 (7) |
| Prior exposure to echinocandins | 13 (87) |
| Echinocandin resistance occurrence | |
| Breakthrough resistance while on echinocandin | 12 (80) |
| De novo resistance (nil exposure to echinocandins) | 2 (13) |
| Outcome | |
| Recovery | 9 (60) |
| Death | 6 (40) |
| Candida tropicalis Isolate | DNA Sequence | Protein |
|---|---|---|
| ATCC 750 Ref strain | TTCTTGACTTTGTCTTTAAGAGATCCA | FLTLSLRDP |
| BL37986 | TTCTTGACTTTGTCTTTAAGAGATCCA | FLTLSLRDP |
| BL38734 | TTCTTGACTTTGCCTTTAAGAGATCCAA | FLTLS/PLRDP |
| Isolate 2 | TTCTTGACTTTGCCTTTAAGAGATCCAA | FLTLPLRDP |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sfeir, M.M.; Jiménez-Ortigosa, C.; Gamaletsou, M.N.; Schuetz, A.N.; Soave, R.; Van Besien, K.; Small, C.B.; Perlin, D.S.; Walsh, T.J. Breakthrough Bloodstream Infections Caused by Echinocandin-Resistant Candida tropicalis: An Emerging Threat to Immunocompromised Patients with Hematological Malignancies. J. Fungi 2020, 6, 20. https://doi.org/10.3390/jof6010020
Sfeir MM, Jiménez-Ortigosa C, Gamaletsou MN, Schuetz AN, Soave R, Van Besien K, Small CB, Perlin DS, Walsh TJ. Breakthrough Bloodstream Infections Caused by Echinocandin-Resistant Candida tropicalis: An Emerging Threat to Immunocompromised Patients with Hematological Malignancies. Journal of Fungi. 2020; 6(1):20. https://doi.org/10.3390/jof6010020
Chicago/Turabian StyleSfeir, Maroun M., Cristina Jiménez-Ortigosa, Maria N. Gamaletsou, Audrey N. Schuetz, Rosemary Soave, Koen Van Besien, Catherine B. Small, David S. Perlin, and Thomas J. Walsh. 2020. "Breakthrough Bloodstream Infections Caused by Echinocandin-Resistant Candida tropicalis: An Emerging Threat to Immunocompromised Patients with Hematological Malignancies" Journal of Fungi 6, no. 1: 20. https://doi.org/10.3390/jof6010020
APA StyleSfeir, M. M., Jiménez-Ortigosa, C., Gamaletsou, M. N., Schuetz, A. N., Soave, R., Van Besien, K., Small, C. B., Perlin, D. S., & Walsh, T. J. (2020). Breakthrough Bloodstream Infections Caused by Echinocandin-Resistant Candida tropicalis: An Emerging Threat to Immunocompromised Patients with Hematological Malignancies. Journal of Fungi, 6(1), 20. https://doi.org/10.3390/jof6010020