
Ten-Year Results of a Single-Center Trial Investigating Heart Rate Control with Ivabradine or Metoprolol Succinate in Patients After Heart Transplantation

 ,
,  ,
,
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Follow-Up
2.3. Post-Transplant Medications
2.4. Statistical Analysis
3. Results
3.1. Demographics and Post-Transplant Medications
3.2. Drug Dosage and Side Effects
3.3. Post-Transplant Heart Rates
3.4. QT/QTc Intervals
3.5. Blood Pressure Values
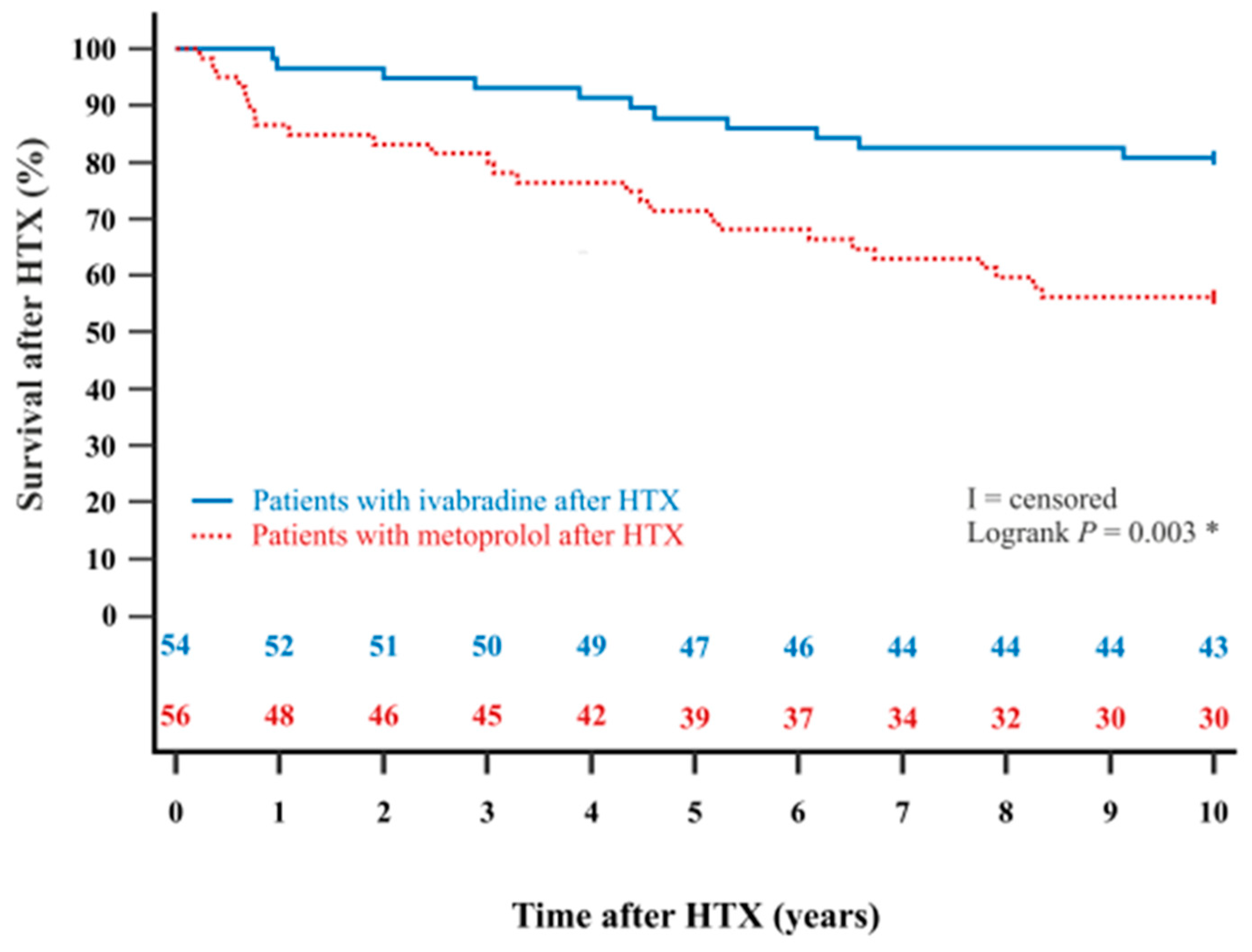
3.6. Post-Transplant Mortality and Causes of Death
3.7. Post-Transplant Echocardiographic Features
3.8. Post-Transplant Cardiac Catheterization Data and Cardiac Biomarkers
4. Discussion
4.1. Long-Term Management of Resting Heart Rates After Heart Transplantation
4.2. Long-Term Results of Side Effects, Blood Pressure, and QT/QTc Interval
4.3. Long-Term Survival After Heart Transplantation
4.4. Long-Term Effects of Heart Rate Control After Heart Transplantation
4.5. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, R.; Haverich, A.; Strüber, M.; Simon, A.; Pichlmaier, M.; Bara, C. Effects of Ivabradine on Allograft Function and Exercise Performance in Heart Transplant Recipients with Permanent Sinus Tachycardia. Clin. Res. Cardiol. 2008, 97, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Bobylev, D.; Stiefel, P.; Haverich, A.; Bara, C. Lasting Reduction of Heart Transplant Tachycardia with Ivabradine is Effective and Well Tolerated: Results of 48-Month Study. Clin. Res. Cardiol. 2012, 101, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Doesch, A.O.; Celik, S.; Ehlermann, P.; Frankenstein, L.; Zehelein, J.; Koch, A.; Katus, H.A.; Dengler, T.J. Heart Rate Reduction after Heart Transplantation with Beta-Blocker Versus the Selective If Channel Antagonist Ivabradine. Transplantation 2007, 84, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Doesch, A.O.; Ammon, K.; Konstandin, M.; Celik, S.; Kristen, A.; Frankenstein, L.; Buss, S.; Hardt, S.; Sack, F.U.; Katus, H.A.; et al. Heart Rate Reduction for 12 Months with Ivabradine Reduces Left Ventricular Mass in Cardiac Allograft Recipients. Transplantation 2009, 88, 835–841. [Google Scholar] [CrossRef]
- Doesch, A.O.; Mueller, S.; Erbel, C.; Gleissner, C.A.; Frankenstein, L.; Hardt, S.; Ruhparwar, A.; Ehlermann, P.; Dengler, T.; Katus, H.A. Heart Rate Reduction for 36 Months with Ivabradine Reduces Left Ventricular Mass in Cardiac Allograft Recipients: A Long-Term Follow-Up Study. Drug Des. Devel. Ther. 2013, 7, 1323–1328. [Google Scholar] [CrossRef]
- Rivinius, R.; Helmschrott, M.; Ruhparwar, A.; Rahm, A.K.; Darche, F.F.; Thomas, D.; Bruckner, T.; Ehlermann, P.; Katus, H.A.; Doesch, A.O. Control of Cardiac Chronotropic Function in Patients after Heart Transplantation: Effects of Ivabradine and Metoprolol Succinate on Resting Heart Rate in the Denervated Heart. Clin. Res. Cardiol. 2018, 107, 138–147. [Google Scholar] [CrossRef]
- Rivinius, R.; Helmschrott, M.; Rahm, A.K.; Darche, F.F.; Thomas, D.; Bruckner, T.; Doesch, A.O.; Katus, H.A.; Ehlermann, P. Five-Year Results of Heart Rate Control with Ivabradine or Metoprolol Succinate in Patients after Heart Transplantation. Clin. Res. Cardiol. 2022, 111, 141–153. [Google Scholar] [CrossRef]
- Custodis, F.; Roggenbuck, U.; Lehmann, N.; Moebus, S.; Laufs, U.; Mahabadi, A.A.; Heusch, G.; Mann, K.; Jöckel, K.H.; Erbel, R.; et al. Resting Heart Rate is an Independent Predictor of All-Cause Mortality in the Middle Aged General Population. Clin. Res. Cardiol. 2016, 105, 601–612. [Google Scholar] [CrossRef]
- Swedberg, K.; Komajda, M.; Böhm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L.; SHIFT Investigators. Ivabradine and Outcomes in Chronic Heart Failure (SHIFT): A Randomised Placebo-Controlled Study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- Böhm, M.; Swedberg, K.; Komajda, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L.; SHIFT Investigators. Heart Rate as a Risk Factor in Chronic Heart Failure (SHIFT): The Association Between Heart Rate and Outcomes in a Randomised Placebo-Controlled Trial. Lancet 2010, 376, 886–894. [Google Scholar] [CrossRef]
- Münzel, T.; Hahad, O.; Gori, T.; Hollmann, S.; Arnold, N.; Prochaska, J.H.; Schulz, A.; Beutel, M.; Pfeiffer, N.; Schmidtmann, I.; et al. Heart Rate, Mortality, and the Relation with Clinical and Subclinical Cardiovascular Diseases: Results from the Gutenberg Health Study. Clin. Res. Cardiol. 2019, 108, 1313–1323. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.D.; McComb, J.M.; Dark, J.H. Heart Rate and Late Mortality in Cardiac Transplant Recipients. Eur. Heart J. 1993, 14, 530–533. [Google Scholar] [CrossRef] [PubMed]
- Dobre, D.; Borer, J.S.; Fox, K.; Swedberg, K.; Adams, K.F.; Cleland, J.G.; Cohen-Solal, A.; Gheorghiade, M.; Gueyffier, F.; O’Connor, C.M.; et al. Heart Rate: A Prognostic Factor and Therapeutic Target in Chronic Heart Failure. The Distinct Roles of Drugs with Heart Rate-Lowering Properties. Eur. J. Heart Fail. 2014, 16, 76–85. [Google Scholar] [CrossRef]
- Tardif, J.C.; Ford, I.; Tendera, M.; Bourassa, M.G.; Fox, K.; INITIATIVE Investigators. Efficacy of Ivabradine, a New Selective I(f) Inhibitor, Compared with Atenolol in Patients with Chronic Stable Angina. Eur. Heart J. 2005, 26, 2529–2536. [Google Scholar] [CrossRef]
- DiFrancesco, D. Characterization of Single Pacemaker Channels in Cardiac Sino-Atrial Node Cells. Nature 1986, 324, 470–473. [Google Scholar] [CrossRef]
- DiFrancesco, D. The Contribution of the ‘Pacemaker’ Current (if) to Generation of Spontaneous Activity in Rabbit Sino-Atrial Node Myocytes. J. Physiol. 1991, 434, 23–40. [Google Scholar] [CrossRef]
- DiFrancesco, D.; Camm, J.A. Heart Rate Lowering by Specific and Selective I(f) Current Inhibition with Ivabradine: A New Therapeutic Perspective in Cardiovascular Disease. Drugs 2004, 64, 1757–1765. [Google Scholar] [CrossRef]
- Thollon, C.; Bedut, S.; Villeneuve, N.; Cogé, F.; Piffard, L.; Guillaumin, J.P.; Brunel-Jacquemin, C.; Chomarat, P.; Boutin, J.A.; Peglion, J.L.; et al. Use-Dependent Inhibition of hHCN4 by Ivabradine and Relationship with Reduction in Pacemaker Activity. Br. J. Pharmacol. 2007, 150, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Haechl, N.; Ebner, J.; Hilber, K.; Todt, H.; Koenig, X. Pharmacological Profile of the Bradycardic Agent Ivabradine on Human Cardiac Ion Channels. Cell. Physiol. Biochem. 2019, 53, 36–48. [Google Scholar] [CrossRef]
- Hancox, J.C.; Melgari, D.; Dempsey, C.E.; Brack, K.E.; Mitcheson, J.; Ng, G.A. hERG Potassium Channel Inhibition by Ivabradine May Contribute to QT Prolongation and Risk of Torsades De Pointes. Ther. Adv. Drug Saf. 2015, 6, 177–179. [Google Scholar] [CrossRef]
- Melgari, D.; Brack, K.E.; Zhang, C.; Zhang, Y.; El Harchi, A.; Mitcheson, J.S.; Dempsey, C.E.; Ng, G.A.; Hancox, J.C. hERG Potassium Channel Blockade by the HCN Channel Inhibitor Bradycardic Agent Ivabradine. J. Am. Heart Assoc. 2015, 4, e001813. [Google Scholar] [CrossRef]
- Savelieva, I.; Camm, A.J. Novel If Current Inhibitor Ivabradine: Safety Considerations. Adv. Cardiol. 2006, 43, 79–96. [Google Scholar]
- Ozkanlar, Y.; Nishijima, Y.; da Cunha, D.; Hamlin, R.L. Acute Effects of Tacrolimus (FK506) on Left Ventricular Mechanics. Pharmacol. Res. 2005, 52, 307–312. [Google Scholar]
- Darche, F.F.; Helmschrott, M.; Rahm, A.K.; Thomas, D.; Schweizer, P.A.; Bruckner, T.; Ehlermann, P.; Kreusser, M.M.; Warnecke, G.; Frey, N.; et al. Atrial Fibrillation before Heart Transplantation is a Risk Factor for Post-Transplant Atrial Fibrillation and Mortality. ESC Heart Fail. 2021, 8, 4265–4277. [Google Scholar] [CrossRef] [PubMed]
- Darche, F.F.; Fabricius, L.C.; Helmschrott, M.; Rahm, A.K.; Ehlermann, P.; Bruckner, T.; Sommer, W.; Warnecke, G.; Frey, N.; Rivinius, R. Oral Anticoagulants after Heart Transplantation-Comparison between Vitamin K Antagonists and Direct Oral Anticoagulants. J. Clin. Med. 2023, 12, 4334. [Google Scholar] [CrossRef] [PubMed]
- Darche, F.F.; Heil, K.M.; Rivinius, R.; Helmschrott, M.; Ehlermann, P.; Frey, N.; Rahm, A.K. Early Pacemaker Dependency after Heart Transplantation is Associated with Permanent Pacemaker Implantation, Graft Failure and Mortality. J. Cardiovasc. Dev. Dis. 2024, 11, 394. [Google Scholar] [CrossRef]
- Vandenberk, B.; Vandael, E.; Robyns, T.; Vandenberghe, J.; Garweg, C.; Foulon, V.; Ector, J.; Willems, R. Which QT Correction Formulae to Use for QT Monitoring? J. Am. Heart Assoc. 2016, 5, e003264. [Google Scholar] [CrossRef] [PubMed]
- Boeken, U.; Albert, A.; Mehdiani, A.; Sowinski, B.; Westenfeld, R.; Aubin, H.; Saeed, D.; Akhyari, P.; Lichtenberg, A. Efficacy and Safety of Ivabradine Application in the Early Period after Heart Transplantation. J. Heart Lung Transplant. 2019, 38, S292. [Google Scholar] [CrossRef]
- Dos Santos, C.C.; Rossi Neto, J.M.; Finger, M.A.; Timerman, A.; Contreras, C.; Chaccur, P. Ivabradine plus Conventional Treatment vs Conventional Treatment Alone in Reducing the Mean Heart Rate in Heart Transplant Recipients: A Randomized Clinical Trial. Clin. Transplant. 2021, 35, e14227. [Google Scholar] [CrossRef]
- Halpert, I.; Goldberg, A.D.; Levine, A.B.; Levine, T.B.; Kornberg, R.; Kelly, C.; Lesch, M. Reinnervation of the Transplanted Human Heart as Evidenced from Heart Rate Variability Studies. Am. J. Cardiol. 1996, 77, 180–183. [Google Scholar] [CrossRef]
- Lage-Gallé, E.; Romero-Rodríguez, N.; Nevado-Portero, J.; Guisado-Rasco, A.; Sobrino-Márquez, M.; Machuca, M.G.; Fernández-Quero, M.; Campos-Pareja, A.; Ballesteros-Pradas, S.; Martínez-Martínez, A. Safety and Effectiveness of Ivabradine after Cardiac Transplantation. Transplant. Proc. 2010, 42, 3191–3192. [Google Scholar] [CrossRef]
- Minematsu, T.; Ohtani, H.; Sato, H.; Iga, T. Sustained QT Prolongation Induced by Tacrolimus in Guinea Pigs. Life Sci. 1999, 65, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.C.; So, S.; Marsh, J.W.; Murphy, A.M. QT Prolongation and Torsades de Pointes after Administration of FK506. Transplantation 1992, 53, 929–930. [Google Scholar] [CrossRef]
- Kröller-Schön, S.; Schulz, E.; Wenzel, P.; Kleschyov, A.L.; Hortmann, M.; Torzewski, M.; Oelze, M.; Renné, T.; Daiber, A.; Münzel, T. Differential Effects of Heart Rate Reduction with Ivabradine in Two Models of Endothelial Dysfunction and Oxidative Stress. Basic Res. Cardiol. 2011, 106, 1147–1158. [Google Scholar] [CrossRef]
- Mangiacapra, F.; Colaiori, I.; Ricottini, E.; Balducci, F.; Creta, A.; Demartini, C.; Minotti, G.; Di Sciascio, G. Heart Rate Reduction by IVabradine for Improvement of ENDothELial Function in Patients with Coronary Artery Disease: The RIVENDEL study. Clin. Res. Cardiol. 2017, 106, 69–75. [Google Scholar] [CrossRef]
- Sabbah, H.N.; Gupta, R.C.; Kohli, S.; Wang, M.; Zhang, K.; Rastogi, S. Heart Rate Reduction with Ivabradine Improves Left Ventricular Function and Reverses Multiple Pathological Maladaptations in Dogs with Chronic Heart Failure. ESC Heart Fail. 2014, 1, 94–102. [Google Scholar] [CrossRef]
- Fischer-Rasokat, U.; Honold, J.; Lochmann, D.; Wolter, S.; Liebetrau, C.; Fichtlscherer, S.; Möllmann, H.; Spyridopoulos, I.; Hamm, C.W. β-Blockers and Ivabradine Differentially Affect Cardiopulmonary Function and Left Ventricular Filling Index. Clin. Res. Cardiol. 2016, 105, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Mulder, P.; Barbier, S.; Chagraoui, A.; Richard, V.; Henry, J.P.; Lallemand, F.; Renet, S.; Lerebours, G.; Mahlberg-Gaudin, F.; Thuillez, C. Long-term Heart Rate Reduction Induced by the Selective I(f) Current Inhibitor Ivabradine Improves Left Ventricular Function and Intrinsic Myocardial Structure in Congestive Heart Failure. Circulation 2004, 109, 1674–1679. [Google Scholar] [CrossRef]
- Monnet, X.; Colin, P.; Ghaleh, B.; Hittinger, L.; Giudicelli, J.F.; Berdeaux, A. Heart Rate Reduction During Exercise-Induced Myocardial Ischaemia and Stunning. Eur. Heart J. 2004, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Yang, M.; Wang, H.; Shen, C.; Wu, M.; Xu, H.; Wu, Y.; Li, Y.; Li, X.; Huang, T.; et al. Moderate Heart Rate Reduction Promotes Cardiac Regeneration through Stimulation of the Metabolic Pattern Switch. Cell Rep. 2022, 38, 110468. [Google Scholar] [CrossRef]
- Chih, S.; Chong, A.Y.; Mielniczuk, L.M.; Bhatt, D.L.; Beanlands, R.S. Allograft Vasculopathy: The Achilles’ Heel of Heart Transplantation. J. Am. Coll. Cardiol. 2016, 68, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Minton, D.; Lee, D.C.; Sui, X.; Fayad, R.; Lavie, C.J.; Blair, S.N. Protective Role of Resting Heart Rate on All-Cause and Cardiovascular Disease Mortality. Mayo Clin. Proc. 2013, 88, 1420–1426. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Recipient data | ||||||
| Age (years), mean ± SD | 51.3 ± 10.8 | 49.9 ± 11.4 | 52.7 ± 10.2 | 2.8 | −1.2–6.8 | 0.165 |
| Male sex, n (%) | 82 (74.5%) | 40 (74.1%) | 42 (75.0%) | 0.9% | −15.4–17.2% | 0.911 |
| BMI (kg/m2), mean ± SD | 25.3 ± 4.7 | 24.8 ± 4.9 | 25.8 ± 4.4 | 1.0 | −0.7–2.7 | 0.226 |
| Arterial hypertension, n (%) | 65 (59.1%) | 28 (51.9%) | 37 (66.1%) | 14.2% | −4.0–32.4% | 0.129 |
| Dyslipidemia, n (%) | 66 (60.0%) | 32 (59.2%) | 34 (60.7%) | 1.5% | −16.8–19.8% | 0.876 |
| Diabetes mellitus, n (%) | 36 (32.7%) | 16 (29.6%) | 20 (35.7%) | 6.1% | −11.4–23.6% | 0.497 |
| Peripheral artery disease, n (%) | 11 (10.0%) | 3 (5.6%) | 8 (14.3%) | 8.7% | −2.3–19.7% | 0.127 |
| COPD, n (%) | 26 (23.6%) | 9 (16.7%) | 17 (30.4%) | 13.7% | −1.9–29.3% | 0.091 |
| History of smoking, n (%) | 65 (59.1%) | 29 (53.7%) | 36 (64.3%) | 10.6% | −7.7–28.9% | 0.259 |
| Chronic kidney disease ^, n (%) | 59 (53.6%) | 27 (50.0%) | 32 (57.1%) | 7.1% | −11.5–25.7% | 0.453 |
| eGFR (ml/min/1.73 m2), mean ± SD | 59.7 ± 22.6 | 61.6 ± 25.0 | 57.8 ± 20.1 | 3.8 | −4.7–12.3 | 0.391 |
| Previous open-heart surgery | ||||||
| Overall open-heart surgery, n (%) | 21 (19.1%) | 11 (20.4%) | 10 (17.9%) | 2.5% | −12.2–17.2% | 0.737 |
| CABG surgery, n (%) | 8 (7.3%) | 3 (5.6%) | 5 (8.9%) | 3.3% | −6.4–13.0% | 0.496 |
| Other surgery °, n (%) | 8 (7.3%) | 4 (7.4%) | 4 (7.1%) | 0.3% | −9.4–10.0% | 0.957 |
| VAD surgery, n (%) | 8 (7.3%) | 5 (9.3%) | 3 (5.4%) | 3.9% | −5.9–13.7% | 0.431 |
| Principal diagnosis for HTX | ||||||
| Ischemic CMP, n (%) | 38 (34.5%) | 15 (27.8%) | 23 (41.1%) | 13.3% | −4.3–30.9% | 0.143 |
| Non-ischemic CMP, n (%) | 53 (48.2%) | 30 (55.5%) | 23 (41.1%) | 14.4% | −4.1–32.9% | 0.129 |
| Valvular heart disease, n (%) | 3 (2.7%) | 2 (3.7%) | 1 (1.8%) | 1.9% | −4.2–8.0% | 0.537 |
| Cardiac amyloidosis, n (%) | 16 (14.6%) | 7 (13.0%) | 9 (16.0%) | 3.0% | −10.1–16.1% | 0.644 |
| Donor data | ||||||
| Age (years), mean ± SD | 45.2 ± 13.5 | 42.9 ± 14.6 | 47.4 ± 12.1 | 4.5 | −0.5–9.5 | 0.083 |
| Male sex, n (%) | 31 (28.2%) | 13 (24.1%) | 18 (32.1%) | 8.0% | −8.7–24.7% | 0.347 |
| BMI (kg/m2), mean ± SD | 25.3 ± 5.2 | 24.5 ± 5.2 | 26.1 ± 5.1 | 1.6 | −0.3–3.5 | 0.099 |
| Transplant sex mismatch | ||||||
| Mismatch, n (%) | 58 (52.7%) | 32 (59.2%) | 26 (46.4%) | 12.8% | −5.7–31.3% | 0.178 |
| Donor (m) to recipient (f), n (%) | 3 (2.7%) | 2 (3.7%) | 1 (1.8%) | 1.9% | −4.2–8.0% | 0.537 |
| Donor (f) to recipient (m), n (%) | 55 (50.7%) | 30 (55.5%) | 25 (44.6%) | 10.9% | −7.7–29.5% | 0.252 |
| Perioperative data | ||||||
| Ischemic time (min), mean ± SD | 262.4 ± 56.6 | 268.9 ± 52.7 | 256.1 ± 59.8 | 12.8 | −8.3–33.9 | 0.236 |
| Biatrial anastomosis, n (%) | 1 (0.9%) | 0 (0.0%) | 1 (1.8%) | 1.8% | −1.7–5.3% | 0.324 |
| Bicaval anastomosis, n (%) | 47 (42.7%) | 27 (50.0%) | 20 (35.7%) | 14.3% | −4.0–32.6% | 0.130 |
| Total orthotopic anastomosis, n (%) | 62 (56.4%) | 27 (50.0%) | 35 (62.5%) | 12.5% | −5.9–30.9% | 0.186 |
| LOS (days), mean ± SD | 45.4 ± 19.4 | 44.8 ± 20.0 | 46.1 ± 18.9 | 1.3 | −6.0–8.6 | 0.721 |
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Immunosuppressive drug therapy | ||||||
| Cyclosporine A, n (%) | 9 (8.2%) | 4 (7.4%) | 5 (8.9%) | 1.5% | −8.7–11.7% | 0.771 |
| Tacrolimus, n (%) | 101 (91.8%) | 50 (92.6%) | 51 (91.1%) | 1.5% | −8.7–11.7% | 0.771 |
| Azathioprine, n (%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.0% | n. a. | n. a. |
| Mycophenolic acid, n (%) | 110 (100.0%) | 54 (100.0%) | 56 (100.0%) | 0.0% | n. a. | n. a. |
| Steroids, n (%) | 110 (100.0%) | 54 (100.0%) | 56 (100.0%) | 0.0% | n. a. | n. a. |
| Concomitant medications | ||||||
| ASA, n (%) | 21 (19.1%) | 8 (14.8%) | 13 (23.2%) | 8.4% | −6.2–23.0% | 0.262 |
| Amiodarone, n (%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.0% | n. a. | n. a. |
| Digitalis, n (%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.0% | n. a. | n. a. |
| Beta blocker, n (%) | 56 (50.9%) | 0 (0.0%) | 56 (100.0%) | 100.0% | n. a. | <0.001 * |
| Ivabradine, n (%) | 54 (49.1%) | 54 (100.0%) | 0 (0.0%) | 100.0% | n. a. | <0.001 * |
| Calcium channel blocker ^, n (%) | 25 (22.7%) | 12 (22.2%) | 13 (23.2%) | 1.0% | −14.7–16.7% | 0.901 |
| ACE inhibitor/ARB, n (%) | 46 (41.8%) | 23 (42.6%) | 23 (41.1%) | 1.5% | −16.9–19.9% | 0.872 |
| Diuretic, n (%) | 110 (100.0%) | 54 (100.0%) | 56 (100.0%) | 0.0% | n. a. | n. a. |
| Statin, n (%) | 80 (72.7%) | 37 (68.5%) | 43 (76.8%) | 8.3% | −8.3–24.9% | 0.330 |
| Gastric protection drug †, n (%) | 110 (100.0%) | 54 (100.0%) | 56 (100.0%) | 0.0% | n. a. | n. a. |
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Average heart rate (bpm) (resting ECG), mean ± SD | ||||||
| Baseline after HTX | 87.8 ± 8.6 | 88.8 ± 7.6 | 86.9 ± 9.5 | 1.9 | −1.3–5.1 | 0.257 |
| At 5-year FU after HTX | 76.7 ± 10.2 | 73.4 ± 9.0 | 80.7 ± 10.3 | 7.3 | 3.2–11.4 | <0.001 * |
| At 10-year FU after HTX | 75.7 ± 9.0 | 72.7 ± 8.5 | 80.1 ± 8.1 | 7.4 | 3.6–11.2 | <0.001 * |
| p-value: baseline vs. 5-year FU | <0.001 * | <0.001 * | 0.004 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | 0.001 * | |||
| Average heart rate (bpm) (24 h-Holter monitor), mean ± SD | ||||||
| Baseline after HTX | 85.9 ± 9.4 | 86.2 ± 9.8 | 85.6 ± 9.0 | 0.6 | −2.9–4.1 | 0.756 |
| At 5-year FU after HTX | 75.9 ± 8.4 | 72.5 ± 7.1 | 79.9 ± 8.1 | 7.4 | 4.1–10.7 | <0.001 * |
| At 10-year FU after HTX | 74.2 ± 8.6 | 70.9 ± 7.0 | 79.1 ± 8.4 | 8.2 | 4.5–11.9 | <0.001 * |
| p-value: baseline vs. 5-year FU | <0.001 * | <0.001 * | 0.002 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | 0.001 * | |||
| QT interval (ms), mean ± SD | ||||||
| Baseline after HTX | 367.5 ± 21.2 | 365.5 ± 21.1 | 369.4 ± 21.2 | 3.9 | −4.0–11.8 | 0.337 |
| At 5-year FU after HTX | 388.0 ± 23.8 | 391.9 ± 23.4 | 383.5 ± 23.8 | 8.4 | −1.6–18.4 | 0.105 |
| At 10-year FU after HTX | 391.6 ± 24.3 | 392.8 ± 26.4 | 389.9 ± 21.3 | 2.9 | −8.1–13.9 | 0.603 |
| p-value: baseline vs. 5-year FU | <0.001 * | <0.001 * | 0.004 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | <0.001 * | |||
| QTc interval (ms), mean ± SD | ||||||
| Baseline after HTX | 416.0 ± 19.4 | 415.2 ± 21.2 | 416.8 ± 17.6 | 1.6 | −5.7–8.9 | 0.672 |
| At 5-year FU after HTX | 419.4 ± 16.4 | 417.3 ± 14.9 | 422.0 ± 18.0 | 4.7 | −2.4–11.8 | 0.199 |
| At 10-year FU after HTX | 420.3 ± 16.9 | 419.0 ± 17.8 | 422.2 ± 15.5 | 3.2 | −4.5–10.9 | 0.423 |
| p-value: baseline vs. 5-year FU | 0.182 | 0.560 | 0.165 | |||
| p-value: baseline vs. 10-year FU | 0.115 | 0.341 | 0.148 | |||
| Systolic BP (mmHg), mean ± SD | ||||||
| Baseline after HTX | 125.8 ± 15.4 | 126.1 ± 13.9 | 125.4 ± 16.8 | 0.7 | −5.1–6.5 | 0.821 |
| At 5-year FU after HTX | 125.5 ± 11.7 | 125.2 ± 13.3 | 125.9 ± 9.5 | 0.7 | −4.1–5.5 | 0.782 |
| At 10-year FU after HTX | 124.6 ± 12.2 | 124.5 ± 12.8 | 124.7 ± 11.5 | 0.2 | −5.4–5.8 | 0.963 |
| p-value: baseline vs. 5-year FU | 0.897 | 0.741 | 0.869 | |||
| p-value: baseline vs. 10-year FU | 0.564 | 0.562 | 0.801 | |||
| Diastolic BP (mmHg), mean ± SD | ||||||
| Baseline after HTX | 77.3 ± 9.1 | 78.0 ± 9.3 | 76.7 ± 9.0 | 1.3 | −2.1–4.7 | 0.469 |
| At 5-year FU after HTX | 76.9 ± 8.9 | 76.7 ± 7.5 | 77.2 ± 8.8 | 0.5 | −3.0–4.0 | 0.790 |
| At 10-year FU after HTX | 76.2 ± 8.7 | 76.2 ± 9.7 | 76.3 ± 7.3 | 0.1 | −3.8–4.0 | 0.932 |
| p-value: baseline vs. 5-year FU | 0.746 | 0.454 | 0.794 | |||
| p-value: baseline vs. 10-year FU | 0.419 | 0.357 | 0.840 |
| (a) Within 5 Years After HTX. | ||||||
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
| Graft failure, n (%) | 9 (8.2%) | 0 (0.0%) | 9 (16.0%) | 16.0% | 6.4–25.6% | 0.002 * |
| Acute rejection, n (%) | 2 (1.8%) | 1 (1.9%) | 1 (1.8%) | 0.1% | −4.9–5.1% | 0.979 |
| Infection/sepsis, n (%) | 11 (10.0%) | 5 (9.2%) | 6 (10.7%) | 1.5% | −9.7–12.7% | 0.799 |
| Malignancy, n (%) | 1 (0.9%) | 1 (1.9%) | 0 (0.0%) | 1.9% | −1.7–5.5% | 0.306 |
| Thromboembolic event/bleeding, n (%) | 1 (0.9%) | 0 (0.0%) | 1 (1.8%) | 1.8% | −1.7–5.3% | 0.324 |
| All causes, n (%) | 24 (21.8%) | 7 (13.0%) | 17 (30.3%) | 17.3% | 2.3–32.3% | 0.027 * |
| (b) Within 10 Years After HTX. | ||||||
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
| Graft failure, n (%) | 13 (11.8%) | 1 (1.9%) | 12 (21.4%) | 19.5% | 8.2–30.8% | 0.001 * |
| Acute rejection, n (%) | 3 (2.7%) | 1 (1.9%) | 2 (3.6%) | 1.7% | −4.4–7.8% | 0.580 |
| Infection/sepsis, n (%) | 15 (13.6%) | 7 (13.0%) | 8 (14.3%) | 1.3% | −11.5–14.1% | 0.840 |
| Malignancy, n (%) | 4 (3.6%) | 2 (3.7%) | 2 (3.6%) | 0.1% | −6.9–7.1% | 0.970 |
| Thromboembolic event/bleeding, n (%) | 2 (1.8%) | 0 (0.0%) | 2 (3.6%) | 3.6% | −1.3–8.5% | 0.161 |
| All causes, n (%) | 37 (33.6%) | 11 (20.4%) | 26 (46.4%) | 26.0% | 9.1–42.9% | 0.004 * |
| (a) Within 5 Years After HTX. | |||
| Parameter | Hazard Ratio | 95% CI | p-Value |
| Recipient age (years) | 0.989 | 0.947–1.034 | 0.631 |
| Recipient BMI (kg/m2) | 1.050 | 0.961–1.147 | 0.278 |
| Recipient eGFR (mL/min/1.73 m2) | 1.003 | 0.984–1.022 | 0.791 |
| Donor age (years) | 0.996 | 0.962–1.031 | 0.805 |
| Donor BMI (kg/m2) | 1.072 | 0.991–1.159 | 0.082 |
| Transplant sex mismatch (in total) | 0.943 | 0.412–2.161 | 0.890 |
| Total ischemic time (min) | 1.001 | 0.994–1.008 | 0.841 |
| Administration of ivabradine after HTX (in total) | 0.388 | 0.159–0.949 | 0.038 * |
| (b) Within 10 Years After HTX. | |||
| Parameter | Hazard Ratio | 95% CI | p-Value |
| Recipient age (years) | 0.982 | 0.949–1.017 | 0.314 |
| Recipient BMI (kg/m2) | 1.036 | 0.963–1.115 | 0.341 |
| Recipient eGFR (mL/min/1.73 m2) | 1.003 | 0.987–1.020 | 0.687 |
| Donor age (years) | 1.008 | 0.980–1.037 | 0.566 |
| Donor BMI (kg/m2) | 1.038 | 0.971–1.110 | 0.278 |
| Transplant sex mismatch (in total) | 0.940 | 0.480–1.839 | 0.856 |
| Total ischemic time (min) | 1.001 | 0.995–1.006 | 0.769 |
| Administration of ivabradine after HTX (in total) | 0.374 | 0.182–0.770 | 0.008 * |
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| LV mass (g), mean ± SD | ||||||
| Baseline after HTX | 178.6 ± 40.4 | 178.5 ± 41.9 | 178.6 ± 39.3 | 0.1 | −15.0–15.2 | 0.993 |
| At 5-year FU after HTX | 165.0 ± 28.6 | 153.7 ± 23.7 | 178.2 ± 28.4 | 24.5 | 13.4–35.6 | <0.001 * |
| At 10-year FU after HTX | 165.8 ± 34.6 | 155.9 ± 32.4 | 179.9 ± 33.2 | 24.0 | 8.6–39.4 | 0.003 * |
| p-value: baseline vs. 5-year FU | 0.006 * | <0.001 * | 0.949 | |||
| p-value: baseline vs. 10-year FU | 0.023 * | 0.004 * | 0.874 | |||
| LV mass index (g/m2), mean ± SD | ||||||
| Baseline after HTX | 94.3 ± 20.9 | 96.1 ± 21.4 | 92.5 ± 20.4 | 3.6 | −4.2–11.4 | 0.363 |
| At 5-year FU after HTX | 87.2 ± 17.1 | 81.7 ± 12.9 | 93.8 ± 19.2 | 12.1 | 5.1–19.1 | 0.001 * |
| At 10-year FU after HTX | 86.8 ± 17.1 | 83.1 ± 15.8 | 92.0 ± 17.7 | 8.9 | 1.0–16.8 | 0.031 * |
| p-value: baseline vs. 5-year FU | 0.010 * | <0.001 * | 0.756 | |||
| p-value: baseline vs. 10-year FU | 0.009 * | 0.001 * | 0.916 | |||
| LVEF (%), mean ± SD | ||||||
| Baseline after HTX | 62.1 ± 4.2 | 61.6 ± 4.2 | 62.6 ± 4.2 | 1.0 | −0.6–2.6 | 0.198 |
| At 5-year FU after HTX | 59.1 ± 6.2 | 61.5 ± 6.1 | 56.3 ± 5.0 | 5.2 | 2.9–7.5 | <0.001 * |
| At 10-year FU after HTX | 58.2 ± 5.8 | 60.7 ± 4.5 | 54.6 ± 5.8 | 6.1 | 3.7–8.5 | <0.001 * |
| p-value: baseline vs. 5-year FU | <0.001 * | 0.954 | <0.001 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | 0.314 | <0.001 * | |||
| MAPSE (mm), mean ± SD | ||||||
| Baseline after HTX | 17.7 ± 1.7 | 17.4 ± 1.8 | 17.9 ± 1.6 | 0.5 | −0.2–1.2 | 0.168 |
| At 5-year FU after HTX | 16.6 ± 2.8 | 17.5 ± 2.5 | 15.4 ± 2.8 | 2.1 | 1.0–3.2 | <0.001 * |
| At 10-year FU after HTX | 16.3 ± 2.5 | 17.1 ± 2.4 | 15.1 ± 2.2 | 2.0 | 0.9–3.1 | <0.001 * |
| p-value: baseline vs. 5-year FU | 0.002 * | 0.808 | <0.001 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | 0.515 | <0.001 * | |||
| E/A ratio, mean ± SD | ||||||
| Baseline after HTX | 1.5 ± 0.4 | 1.5 ± 0.3 | 1.6 ± 0.4 | 0.1 | −0.1–0.3 | 0.817 |
| At 5-year FU after HTX | 1.5 ± 0.5 | 1.6 ± 0.4 | 1.3 ± 0.5 | 0.3 | 0.1–0.5 | <0.001 * |
| At 10-year FU after HTX | 1.5 ± 0.4 | 1.6 ± 0.4 | 1.3 ± 0.4 | 0.3 | 0.1–0.5 | <0.001 * |
| p-value: baseline vs. 5-year FU | 0.236 | 0.175 | 0.003 * | |||
| p-value: baseline vs. 10-year FU | 0.473 | 0.169 | 0.005 * | |||
| E/e′ ratio, mean ± SD | ||||||
| Baseline after HTX | 7.5 ± 2.7 | 7.4 ± 2.6 | 7.6 ± 2.8 | 0.2 | −0.8–1.2 | 0.805 |
| At 5-year FU after HTX | 8.4 ± 3.4 | 7.2 ± 2.6 | 9.9 ± 3.8 | 2.7 | 1.3–4.1 | <0.001 * |
| At 10-year FU after HTX | 8.4 ± 2.7 | 7.4 ± 1.8 | 9.8 ± 3.1 | 2.4 | 1.2–3.6 | <0.001 * |
| p-value: baseline vs. 5-year FU | 0.040 * | 0.683 | 0.002 * | |||
| p-value: baseline vs. 10-year FU | 0.027 * | 0.987 | 0.002 * | |||
| DT-E (ms), mean ± SD | ||||||
| Baseline after HTX | 211.1 ± 24.0 | 211.8 ± 22.5 | 210.4 ± 25.6 | 1.4 | −7.6–10.4 | 0.766 |
| At 5-year FU after HTX | 192.2 ± 25.9 | 180.6 ± 21.1 | 205.8 ± 24.6 | 25.2 | 15.5–34.9 | <0.001 * |
| At 10-year FU after HTX | 190.2 ± 27.8 | 181.9 ± 28.8 | 202.2 ± 21.5 | 20.3 | 8.8–31.8 | <0.001 * |
| p-value: baseline vs. 5-year FU | <0.001 * | <0.001 * | 0.369 | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | 0.117 | |||
| LA diameter (mm), mean ± SD | ||||||
| Baseline after HTX | 38.8 ± 5.5 | 38.4 ± 5.8 | 39.1 ± 5.3 | 0.7 | −1.4–2.8 | 0.458 |
| At 5-year FU after HTX | 40.6 ± 5.0 | 39.3 ± 4.9 | 42.2 ± 4.6 | 2.9 | 0.9–4.9 | 0.006 * |
| At 10-year FU after HTX | 41.4 ± 4.5 | 40.2 ± 4.5 | 43.1 ± 3.9 | 2.9 | 1.0–4.8 | 0.005 * |
| p-value: baseline vs. 5-year FU | 0.015 * | 0.389 | 0.004 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | 0.076 | <0.001 * | |||
| Systolic PAP (mmHg), mean ± SD | ||||||
| Baseline after HTX | 30.6 ± 7.5 | 30.5 ± 7.5 | 30.6 ± 7.7 | 0.1 | −2.7–2.9 | 0.901 |
| At 5-year FU after HTX | 27.9 ± 7.0 | 25.8 ± 7.1 | 30.4 ± 6.0 | 4.6 | 1.8–7.4 | 0.002 * |
| At 10-year FU after HTX | 28.1 ± 6.4 | 26.5 ± 5.4 | 30.5 ± 7.1 | 4.0 | 1.0–7.0 | 0.012 * |
| p-value: baseline vs. 5-year FU | 0.011 * | 0.002 * | 0.835 | |||
| p-value: baseline vs. 10-year FU | 0.020 * | 0.003 * | 0.915 |
| Parameter | All Patients (n = 110) | Ivabradine (n = 54) | Metoprolol (n = 56) | Difference | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| CAD (stenosis ≥ 50%), n (%) | ||||||
| Baseline after HTX | 5 (4.5%) | 3 (5.6%) | 2 (3.6%) | 2.0% | −5.8–9.8% | 0.617 |
| Within 5 years after HTX | 27 (24.5%) | 14 (25.9%) | 13 (23.2%) | 2.7% | −13.4–18.8% | 0.741 |
| Within 10 years after HTX | 42 38.2%) | 22 (40.7%) | 20 (35.7%) | 5.0% | −13.1–23.1% | 0.587 |
| p-value: baseline vs. within 5 years | <0.001 * | 0.004 * | 0.002 * | |||
| p-value: baseline vs. within 10 years | <0.001 * | <0.001 * | <0.001 * | |||
| Coronary stenting, n (%) | ||||||
| Baseline after HTX | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0.0% | n. a. | n. a. |
| Within 5 years after HTX | 12 (10.9%) | 6 (11.1%) | 6 (10.7%) | 0.4% | −11.3–12.1% | 0.947 |
| Within 10 years after HTX | 27 (24.5%) | 15 (27.8%) | 12 (21.4%) | 6.4% | −9.7–22.5% | 0.439 |
| p-value: baseline vs. within 5 years | <0.001 * | 0.012 * | 0.012 * | |||
| p-value: baseline vs. within 10 years | <0.001 * | <0.001 * | <0.001 * | |||
| LVEDP (mmHg), mean ± SD | ||||||
| Baseline after HTX | 15.3 ± 2.4 | 15.4 ± 2.7 | 15.2 ± 2.0 | 0.2 | −0.7–1.1 | 0.620 |
| At 5-year FU after HTX | 14.3 ± 4.1 | 12.0 ± 3.7 | 17.1 ± 2.6 | 5.1 | 3.7–6.5 | <0.001 * |
| At 10-year FU after HTX | 13.3 ± 4.4 | 10.4 ± 3.4 | 16.7 ± 2.5 | 6.3 | 5.1–7.5 | <0.001* |
| p-value: baseline vs. 5-year FU | 0.053 | <0.001 * | <0.001 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | 0.002 * | |||
| hs-cTnT (pg/mL), mean ± SD | ||||||
| Baseline after HTX | 167.8 ± 74.4 | 168.7 ± 68.3 | 166.8 ± 80.4 | 1.9 | −26.1–29.9 | 0.892 |
| At 5-year FU after HTX | 16.1 ± 11.3 | 14.6 ± 11.5 | 17.8 ± 11.0 | 3.2 | −1.5–7.9 | 0.191 |
| At 10-year FU after HTX | 19.5 ± 14.7 | 18.8 ± 15.0 | 20.6 ± 14.3 | 1.8 | −5.0–8.6 | 0.598 |
| p-value: baseline vs. 5-year FU | <0.001 * | <0.001 * | <0.001 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | <0.001 * | |||
| NT-proBNP (pg/mL), mean ± SD | ||||||
| Baseline after HTX | 3853.9 ± 1842.9 | 3849.7 ± 1960.0 | 3858.0 ± 1740.3 | 8.3 | −683.8–700.4 | 0.982 |
| At 5-year FU after HTX | 769.5 ± 741.0 | 555.4 ± 541.9 | 1021.0 ± 862.8 | 465.6 | 156.6–774.6 | 0.004 * |
| At 10-year FU after HTX | 851.6 ± 843.2 | 588.4 ± 461.4 | 1229.0 ± 1098.6 | 640.6 | 224.0–1057.2 | 0.005 * |
| p-value: baseline vs. 5-year FU | <0.001 * | <0.001 * | <0.001 * | |||
| p-value: baseline vs. 10-year FU | <0.001 * | <0.001 * | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darche, F.F.; Alt, A.C.; Rivinius, R.; Helmschrott, M.; Ehlermann, P.; Frey, N.; Rahm, A.-K. Ten-Year Results of a Single-Center Trial Investigating Heart Rate Control with Ivabradine or Metoprolol Succinate in Patients After Heart Transplantation. J. Cardiovasc. Dev. Dis. 2025, 12, 297. https://doi.org/10.3390/jcdd12080297
Darche FF, Alt AC, Rivinius R, Helmschrott M, Ehlermann P, Frey N, Rahm A-K. Ten-Year Results of a Single-Center Trial Investigating Heart Rate Control with Ivabradine or Metoprolol Succinate in Patients After Heart Transplantation. Journal of Cardiovascular Development and Disease. 2025; 12(8):297. https://doi.org/10.3390/jcdd12080297
Chicago/Turabian StyleDarche, Fabrice F., Alexandra C. Alt, Rasmus Rivinius, Matthias Helmschrott, Philipp Ehlermann, Norbert Frey, and Ann-Kathrin Rahm. 2025. "Ten-Year Results of a Single-Center Trial Investigating Heart Rate Control with Ivabradine or Metoprolol Succinate in Patients After Heart Transplantation" Journal of Cardiovascular Development and Disease 12, no. 8: 297. https://doi.org/10.3390/jcdd12080297
APA StyleDarche, F. F., Alt, A. C., Rivinius, R., Helmschrott, M., Ehlermann, P., Frey, N., & Rahm, A.-K. (2025). Ten-Year Results of a Single-Center Trial Investigating Heart Rate Control with Ivabradine or Metoprolol Succinate in Patients After Heart Transplantation. Journal of Cardiovascular Development and Disease, 12(8), 297. https://doi.org/10.3390/jcdd12080297