
A Hybrid Minimally Invasive Atrial Fibrillation Ablation Procedure Using Unilateral Thoracoscopy and Endocardial Pulsed Field Ablation: An Early Feasibility Study
 , ,
, , 
Abstract

1. Introduction
2. Materials and Methods
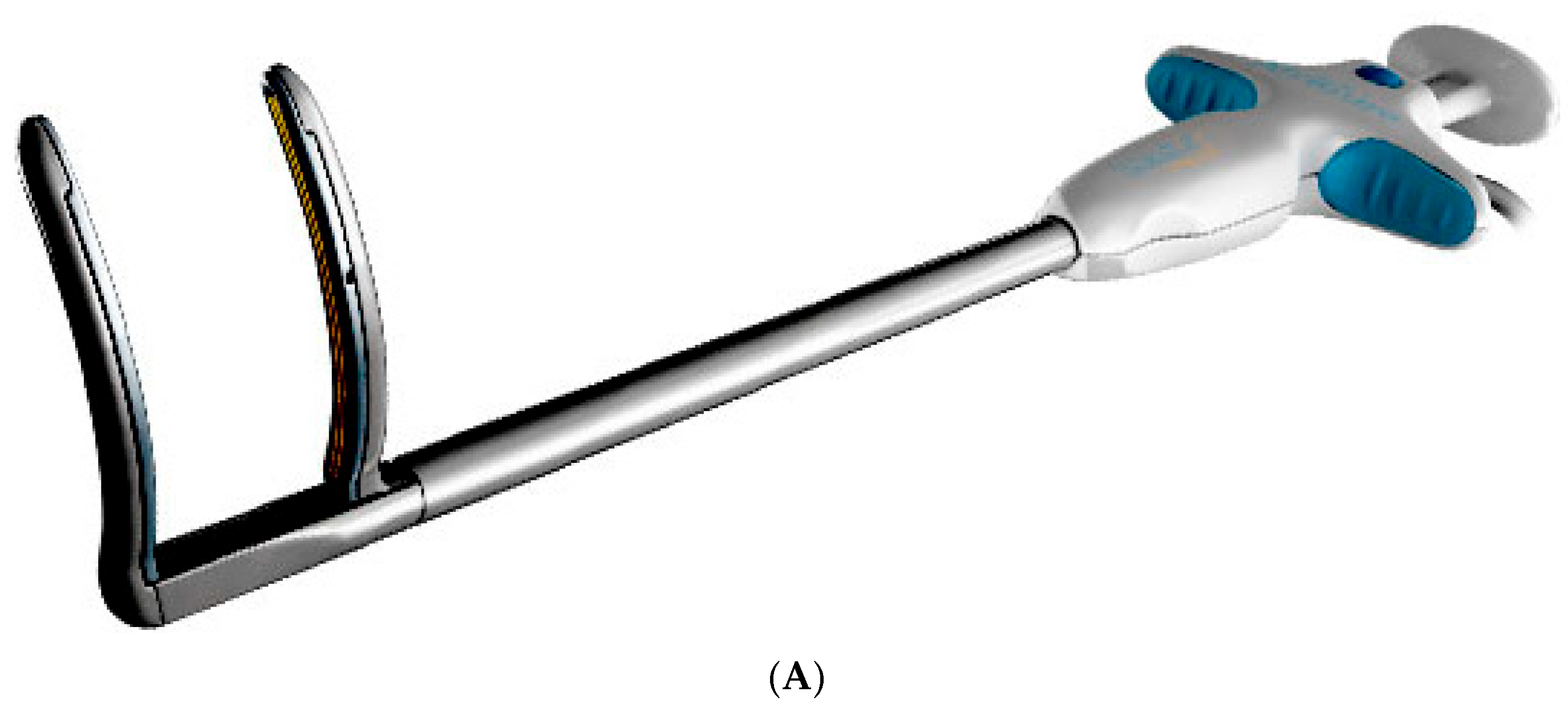
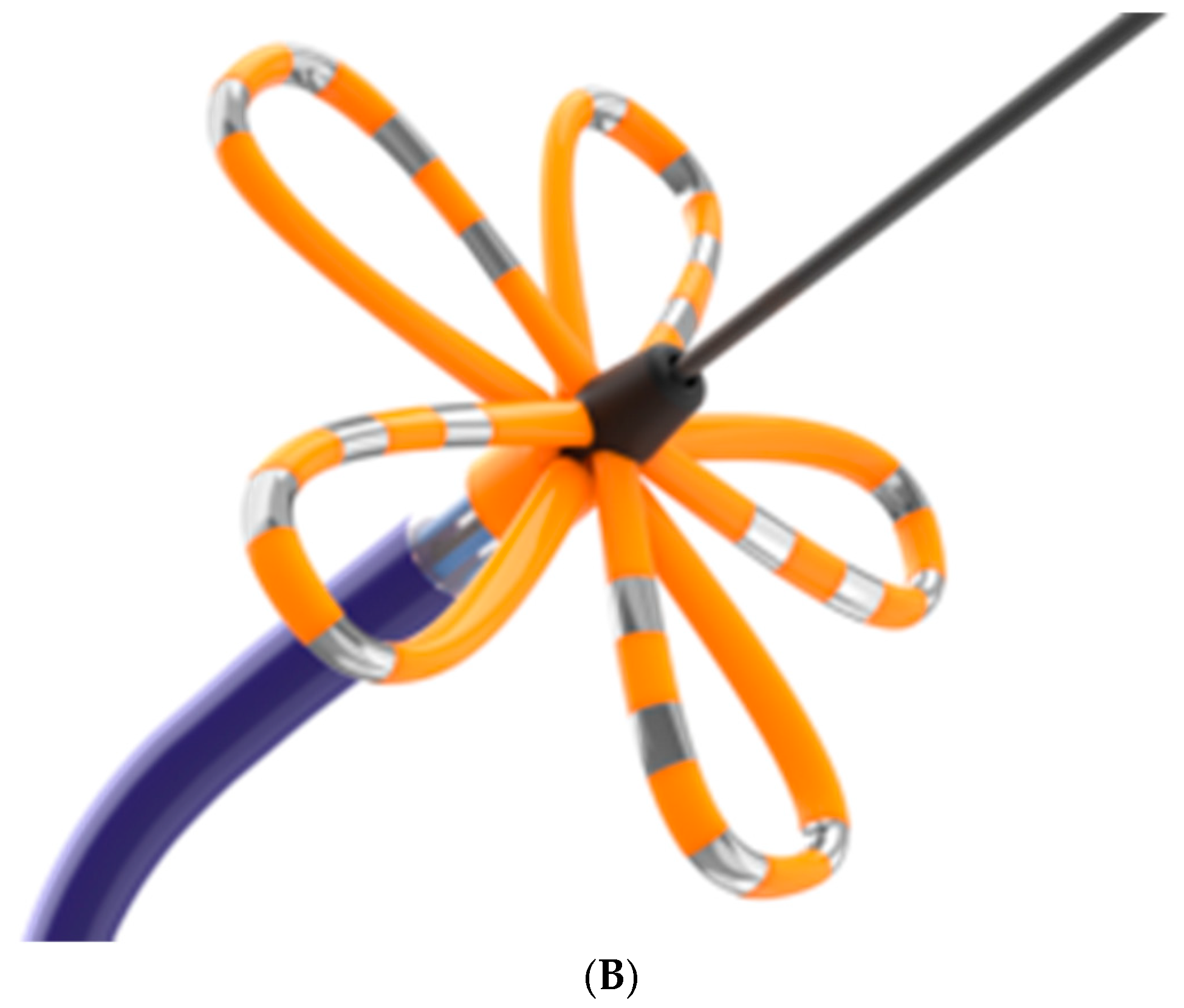
2.1. Devices
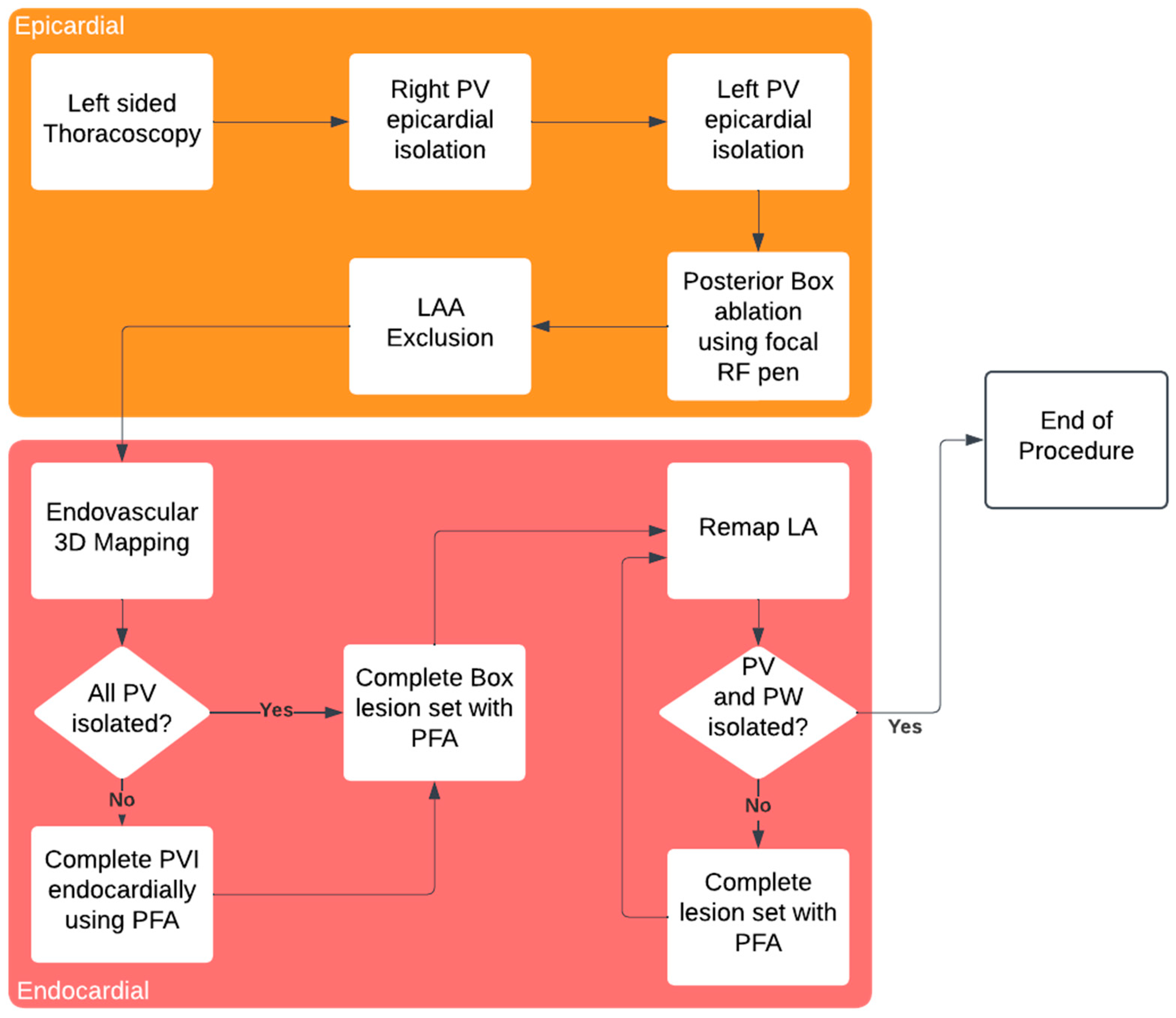
2.2. Surgical Procedure
2.3. Endovascular Procedure
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Study Population Characteristics
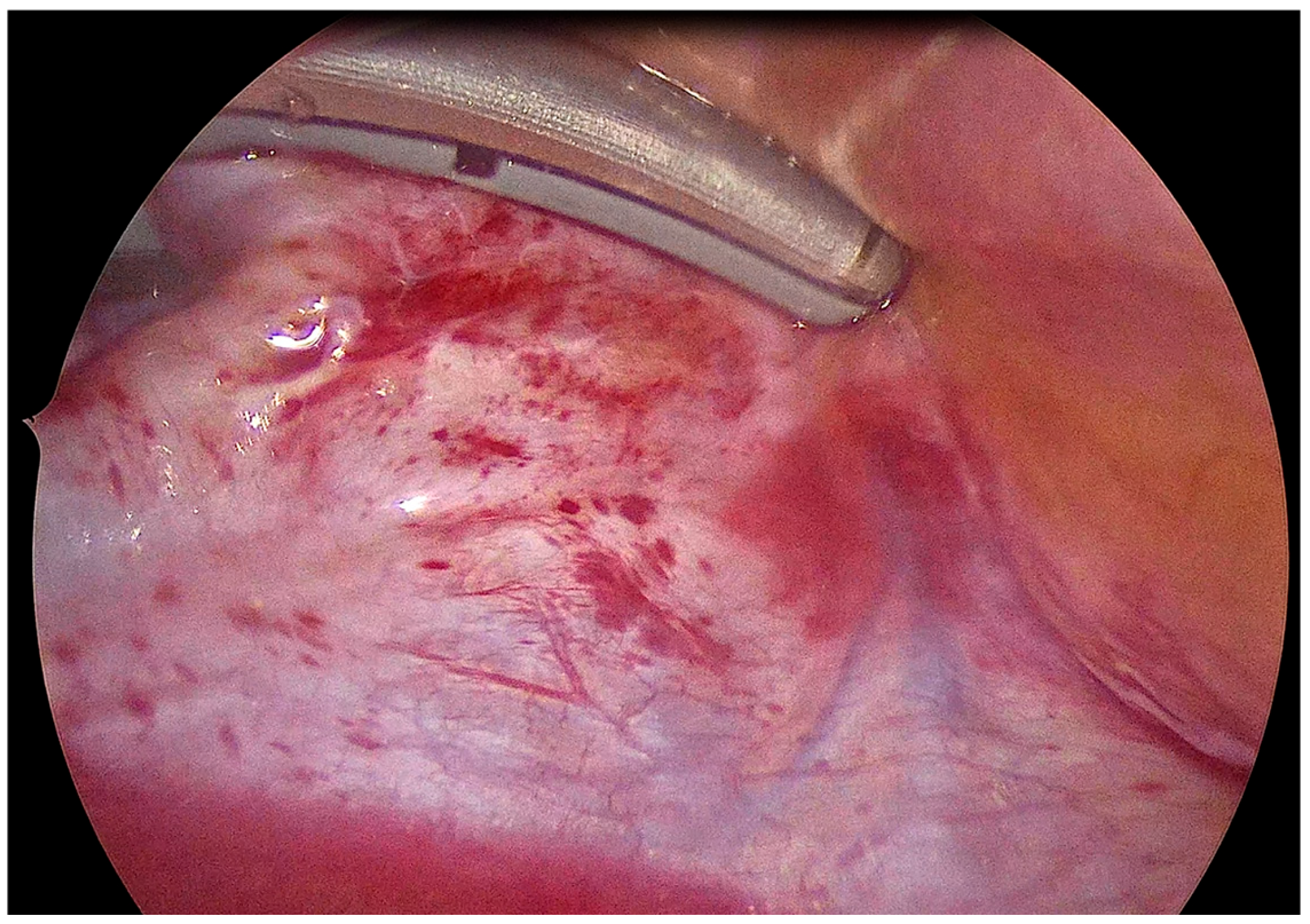
3.2. Intraprocedural Assessment of Epicardial Lesion Set
3.3. Acute Procedure Results
3.4. Safety
3.5. Follow-Up Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AF | Atrial Fibrillation |
| PFA | Pulsed Field Ablation |
| EAM | Electro Pulsed Field Anatomical Mapping |
| RF | Radio Frequency |
| VATS | Video-Assisted Thoracoscopy |
| CMP | Cox-Maze Procedure |
| LPV | Left Pulmonary Veins |
| LSPV | Left Superior Pulmonary Vein |
| LIPV | Left Inferior Pulmonary Vein |
| RPV | Right Pulmonary Veins |
| RSPV | Right Superior Pulmonary Vein |
| RIPV | Right Inferior Pulmonary Vein |
| LAA | Left Atrial Appendage |
| LAAC | Left Atrial Appendage Occlusion |
| LAPW | Left Atrial Posterior Wall |
| PML | Posterior Mitral Line |
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2021 update: A report from the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Wang, T.J.; Leip, E.P.; Larson, M.G.; Levy, D.; Vasan, R.S.; D’agostino, R.B.; Massaro, J.M.; Beiser, A.; Wolf, P.A.; et al. Life time risk ford development of atrial fibrillation: The Framingham Heart Study. Circulation 2004, 110, 1042–1046. [Google Scholar] [CrossRef]
- Yu, J.; Yi, J.; Nikolaisen, G.; Wilson, L.D.; Schill, M.R.; Damiano, R.J.; Zemlin, C.W. Efficacy of a surgical cardiac ablation clamp using nanosecond pulsed electric fields: An acute porcine model. J. Thorac. Cardiovasc. Surg. 2024. online ahead of print. [Google Scholar] [CrossRef]
- Chander, M.P.; Kartick, J.C.; Gangadhar, P. Pulsed field ablation of paroxysmal atrial fibrillation. JACC Clin. Electrophysiol. 2021, 7, 614–627. [Google Scholar] [CrossRef]
- Khiabani, A.J.; MacGregor, R.M.; Bakir, N.H.; Manghelli, J.L.; Sinn, L.A.; Maniar, H.S.; Moon, M.R.; Schuessler, R.B.; Melby, S.J.; Damiano, R.J. The long-term outcomes and durability of the Cox-Maze IV procedure for atrial fibrillation. J. Thorac. Cardiovasc. Surg. 2022, 163, 629–641.e7. [Google Scholar] [CrossRef]
- Badhwar, V.; Rankin, J.S.; Damiano, R.J.; Gillinov, A.M.; Bakaeen, F.G.; Edgerton, J.R.; Philpott, J.M.; McCarthy, P.M.; Bolling, S.F.; Roberts, H.G.; et al. The Society of Thoracic Surgeons 2017 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann. Thorac. Surg. 2017, 103, 329–341. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- von Ballmoos, M.C.W.; Hui, D.S.; Mehaffey, J.H.; Malaisrie, S.C.; Vardas, P.N.; Gillinov, A.M.; Badhwar, V. The Society of Thoracic Surgeons 2023 clinical practice guidelines for the surgical treatment of atrial fibrillation. Ann. Thorac. Surg. 2024, 118, 291–310. [Google Scholar] [CrossRef]
- Tzeis, S.; Gerstenfeld, E.P.; Kalman, J.; Saad, E.; Shamloo, A.S.; Andrade, J.G.; Barbhaiya, C.R.; Baykaner, T.; Boveda, S.; Calkins, H.; et al. 2024 European Heart Rhythm Association/Heart Rhythm Society/Asia Pacific Heart Rhythm Society/Latin American Heart Rhythm Society expert consensus statement on catheter and surgical ablation of atrial fibrillation. J. Interv. Card Electrophysiol. 2024, 67, 921–1072. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, P.M.; Davidson, C.J.; Kruse, J.; Lerner, D.J.; Braid-Forbes, M.J.; McCrea, M.M.; Elmouelhi, A.M.; Ferguson, M.A. Prevalence of atrial fibrillation before cardiac surgery and factors associated with concomitant ablation. J. Thorac. Cardiovasc. Surg. 2020, 159, 2245–2253.e15. [Google Scholar] [CrossRef]
- Marini, M.; Pannone, L.; Della Rocca, D.G.; Branzoli, S.; Bisignani, A.; Mouram, S.; Del Monte, A.; Monaco, C.; Gauthey, A.; Eltsov, I.; et al. Hybrid Ablation of Atrial Fibrillation: A Contemporary Overview. J. Cardiovasc. Dev. Dis. 2022, 9, 302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- DeLurgio, D.B. The hybrid convergent procedure for persistent and long-standing persistent atrial fibrillation from an electrophysiologist’s perspective. J. Cardiovasc. Electrophysiol. 2022, 33, 1954–1960. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Qing, H.; Zhang, Y.; Liu, J.; Chen, Z.; Cao, Z.; Xu, J.; Huang, H.; Xue, Y.; Zhan, X.; et al. Stand-alone surgical ablation for atrial fibrillation: A novel bilateral double-port approach. J. Thorac. Dis. 2019, 11, 1989–1995. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van der Heijden, C.A.J.; Weberndörfer, V.; Luermans, J.G.L.M.; Chaldoupi, S.; van Kuijk, S.M.J.; Vroomen, M.; Bidar, E.; Maessen, J.G.; Pison, L.; La Meir, M.; et al. Hybrid ablation of atrial fibrillation: A unilateral left-sided thoracoscopic approach. J. Card. Surg. 2022, 37, 4630–4638. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schmidt, B.; Bordignon, S.; Neven, K.; Reichlin, T.; Blaauw, Y.; Hansen, J.; Adelino, R.; Ouss, A.; Füting, A.; Roten, L.; et al. European real-world outcomes with Pulsed field ablation in patients with symptomatic atrial fibrillation: Lessons from the multi-centre EUPORIA registry. Europace 2023, 25, euad185. [Google Scholar] [CrossRef]
- Urbanek, L.; Bordignon, S.; Schaack, D.; Chen, S.; Tohoku, S.; Efe, T.H.; Ebrahimi, R.; Pansera, F.; Hirokami, J.; Plank, K.; et al. Pulsed field versus cryoballoon pulmonary vein isolation for atrial fibrillation: Efficacy, safety, and long-term follow-up in a 400-patient cohort. Circ. Arrhythm. Electrophysiol. 2023, 16, 389–398. [Google Scholar] [CrossRef]
- Chen, G.; Gao, M.; Lai, Y.; Huang, L.; Xia, S.; Zuo, S.; Guo, X.; Liu, N.; Long, D.; Dong, J.; et al. Feasibility and Safety of Pulsed-Field Ablation for Persistent Atrial Fibrillation: A Prospective Study. Pacing Clin. Electrophysiol. 2025, 48, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Gelsomino, S.; Van Breugel, H.N.; Pison, L.; Parise, O.; Crijns, H.J.; Wellens, F.; Maessen, J.G.; La Meir, M. Hybrid thoracoscopic and transvenous catheter ablation of atrial fibrillation. Eur. J. Cardiothorac. Surg. 2014, 45, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Pannone, L.; Mouram, S.; Della Rocca, D.G.; Sorgente, A.; Monaco, C.; Del Monte, A.; Gauthey, A.; Bisignani, A.; Kronenberger, R.; Paparella, G.; et al. Hybrid atrial fibrillation ablation: Long-term outcomes from a single-centre 10-year experience. Europace 2023, 25, euad114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dan, G.A.; Martinez-Rubio, A.; Agewall, S.; Boriani, G.; Borggrefe, M.; Gaita, F.; van Gelder, I.; Gorenek, B.; Carlos Kaski, J.; Kjeldsen, K.; et al. Antiarrhythmic drugs-clinical use and clinical decision making: A consensus document from the European Heart Rhythm Association (EHRA) and European Society of Cardiology (ESC) working group on cardiovascular pharmacology, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and International Society of Cardiovascular Pharmacotherapy (ISCP). Europace 2018, 20, 731–732an. [Google Scholar]
- Della Rocca, D.G.; Marcon, L.; Magnocavallo, M.; Menè, R.; Pannone, L.; Mohanty, S.; Sousonis, V.; Sorgente, A.; Almorad, A.; Bisignani, A.; et al. HRMC Investigators. Pulsed electric field, cryoballoon, and radiofrequency for paroxysmal atrial fibrillation ablation: A propensity score-matched comparison. Europace 2023, 26, euae016. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eltsov, I.; Pannone, L.; Ramak, R.; Monaco, C.; Della Rocca, D.G.; Bala, G.; Kronenberger, R.; Overeinder, I.; Almorad, A.; Stroker, E.; et al. 3D mapping challenges in hybrid video-assisted thoracoscopic surgical ablation of Brugada syndrome. Interdiscip. Cardiovasc. Thorac. Surg. 2023, 37, ivad160. [Google Scholar] [CrossRef]
- Ekanem, E.; Neuzil, P.; Reichlin, T.; Kautzner, J.; van der Voort, P.; Jais, P.; Chierchia, G.-B.; Bulava, A.; Blaauw, Y.; Skala, T.; et al. Safety of pulsed field ablation in more than 17,000 patients with atrial fibrillation in the MANIFEST-17K study. Nat. Med. 2024, 30, 2020–2029. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Menè, R.; Boveda, S.; Della Rocca, D.G.; Sousonis, V.; Vetta, G.; Zeriouh, S.; Doundoulakis, I.; Betancur, A.; Benadel, M.; Combes, N.; et al. Efficacy of Intravenous Nitrates for the Prevention of Coronary Artery Spasm During Pulsed Field Ablation of the Mitral Isthmus. Circ. Arrhythm. Electrophysiol. 2024, 17, e012426. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 11) | Normal Epicardial Stage (N = 7) | Anatomical Difficulties Incomplete VATS Stage (N = 4) | p-Value | |
|---|---|---|---|---|
| Age (years) | 65.3 ± 9.3 | 64.6 ± 10.3 | 70.3 ± 9.2 | 0.81 |
| Sex (male) | 10 (90%) | 6 (85.7%) | 4 (100%) | 0.9 |
| BMI (Kg/m2) | 29.6 ± 4.2 | 28.7 ± 3.8 | 31.3 ± 5.1 | 0.56 |
| Cordarone | 3 | 0 (0%) | 2 (50%) | 0.048 |
| Beta Blockers | 4 | 3 (42.8%) | 1 (25%) | 0.1 |
| IC AAD | 3 | 2 (28.6%) | 1 (25%) | 0.9 |
| Index Procedure | 0 (0%) | 0 (0%) | 0 (0%) | N/A |
| Number ReDO | 2.8 | 3 (42.8%) | 2.75 (68.7%) | 0.71 |
| Epicardial first | 11 (100%) | 7 (100%) | 4 (100%) | 1.0 |
| Total (N = 11) | Epicardial Ablation Complete (N = 7) | Anatomical Difficulties Incomplete VATS Stage (N = 4) | p-Value | |
|---|---|---|---|---|
| LPV performed | 11 (100%) | 7 (100%) | 4 (100%) | N/A |
| Nr of LPV epi applications | 4.2 ± 0.7 | 4 ± 1.0 | 4 ± 0.0 | 0.292 |
| RPV performed | 8 (72.7%) | 7 (100%) | 1 (25%) | N/A |
| Nr of RPV epi applications | 4.6 ± 0.7 | 4.8 ± 0 | 4 ± 1.0 | 0.008 |
| PW epi performed | 8 (72.7%) | 7 (100%) | 1 (25%) | N/A |
| Nr of PW epi applications | 12.8 ± 8.0 | 11.8 ± 1.1 | 24 ± 8.0 | 0.31 |
| LAAC performed | 9 (81.8%) | 7 (100%) | 4 (100%) | 1 |
| LSPV isolated | 11 (100%) | 7 (100%) | 1 (25%) | 1 |
| LIPV isolated | 11 (100%) | 7 (100%) | 1 (25%) | 1 |
| RSPV isolated | 8 (72.7%) | 7 (100%) | 3 (75%) | 0.87 |
| RIPV isolated | 8 (72.7%) | 7 (100%) | 3 (75%) | 0.87 |
| PW isolated | 5 (40%) | 6 (85.7%) | 3 (75%) | 0.8 |
| Total (N = 11) | Epicardial Ablation Complete (N = 7) | Anatomical Difficulties Incomplete VATS Stage (N = 4) | p-Value | |
|---|---|---|---|---|
| Nr FP applications LSPV | 11 ± 3.1 | 10.5 ± 3.4 | 12.5 ± 3.0 | 0.69 |
| Nr FP applications LIPV | 10.6 ± 3.6 | 10.6 ± 2.8 | 10.7 ± 4.9 | 0.95 |
| Nr FP applications RSPV | 10.2 ± 3.7 | 10.8 ± 2.7 | 11.2 ± 5.3 | 0.87 |
| Nr FP applications RIPV | 11 ± 2.5 | 10 ± 2.5 | 10.4 ± 4.9 | 0.83 |
| Nr FP applications PW | 39.7 ± 16.5 | 37.8 ± 20.2 | 42.25 ± 13.1 | 0.72 |
| Nr FP applications MI | 21 ± 12.4 | 11 ± 12.7 | 10 ± 13.9 | 0.95 |
| Total (N = 11) | Epicardial Ablation Complete (N = 7) | Anatomical Difficulties Incomplete VATS Stage (N = 4) | p-Value | |
|---|---|---|---|---|
| Procedure duration | 206 ± 46.3 | 217 ± 52.7 | 193 ± 39.6 | 0.458 |
| Surgery duration | 55 ± 21.2 | 65.6 ± 17.7 | 42.5 ± 19.7 | 0.106 |
| Endo duration | 61.3 ± 29.0 | 62.2 ± 22.9 | 60.2 ± 35.8 | 0.928 |
| Fluoro time | 23.8 ± 6.5 | 26.9 ± 7.1 | 19.9 ± 2.8 | 0.109 |
| Dosage | 157.5 ± 77.0 | 181.4 ± 94.9 | 127.5 ± 40.7 | 0.329 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eltsov, I.; Pannone, L.; Della Rocca, D.G.; Marini, M.; Talevi, G.; Paparella, A.M.; Vergara, P.; Ströker, E.; Sieira, J.; Chierchia, G.-B.; et al. A Hybrid Minimally Invasive Atrial Fibrillation Ablation Procedure Using Unilateral Thoracoscopy and Endocardial Pulsed Field Ablation: An Early Feasibility Study. J. Cardiovasc. Dev. Dis. 2025, 12, 145. https://doi.org/10.3390/jcdd12040145
Eltsov I, Pannone L, Della Rocca DG, Marini M, Talevi G, Paparella AM, Vergara P, Ströker E, Sieira J, Chierchia G-B, et al. A Hybrid Minimally Invasive Atrial Fibrillation Ablation Procedure Using Unilateral Thoracoscopy and Endocardial Pulsed Field Ablation: An Early Feasibility Study. Journal of Cardiovascular Development and Disease. 2025; 12(4):145. https://doi.org/10.3390/jcdd12040145
Chicago/Turabian StyleEltsov, Ivan, Luigi Pannone, Domenico Giovanni Della Rocca, Massimiliano Marini, Giacomo Talevi, Andrea Maria Paparella, Pasquale Vergara, Erwin Ströker, Juan Sieira, Gian-Battista Chierchia, and et al. 2025. "A Hybrid Minimally Invasive Atrial Fibrillation Ablation Procedure Using Unilateral Thoracoscopy and Endocardial Pulsed Field Ablation: An Early Feasibility Study" Journal of Cardiovascular Development and Disease 12, no. 4: 145. https://doi.org/10.3390/jcdd12040145
APA StyleEltsov, I., Pannone, L., Della Rocca, D. G., Marini, M., Talevi, G., Paparella, A. M., Vergara, P., Ströker, E., Sieira, J., Chierchia, G.-B., de Asmundis, C., & La Meir, M. (2025). A Hybrid Minimally Invasive Atrial Fibrillation Ablation Procedure Using Unilateral Thoracoscopy and Endocardial Pulsed Field Ablation: An Early Feasibility Study. Journal of Cardiovascular Development and Disease, 12(4), 145. https://doi.org/10.3390/jcdd12040145