
A Study about a New Standardized Method of Home-Based Exercise in Elderly People Aged 65 and Older to Improve Motor Abilities and Well-Being: Feasibility, Functional Abilities and Strength Improvements

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcome Measures
2.2.1. Strength and Functional Abilities Tests
30-s Chair-Stand Test
Hand Grip Test (HAND GRIP)
Timed Up-and-Go Test
Sit-and-Reach Test
Standing Stork Balance Test
2.2.2. Well-Being Tests
Perceived Physical Exertion
Evaluation of Pain
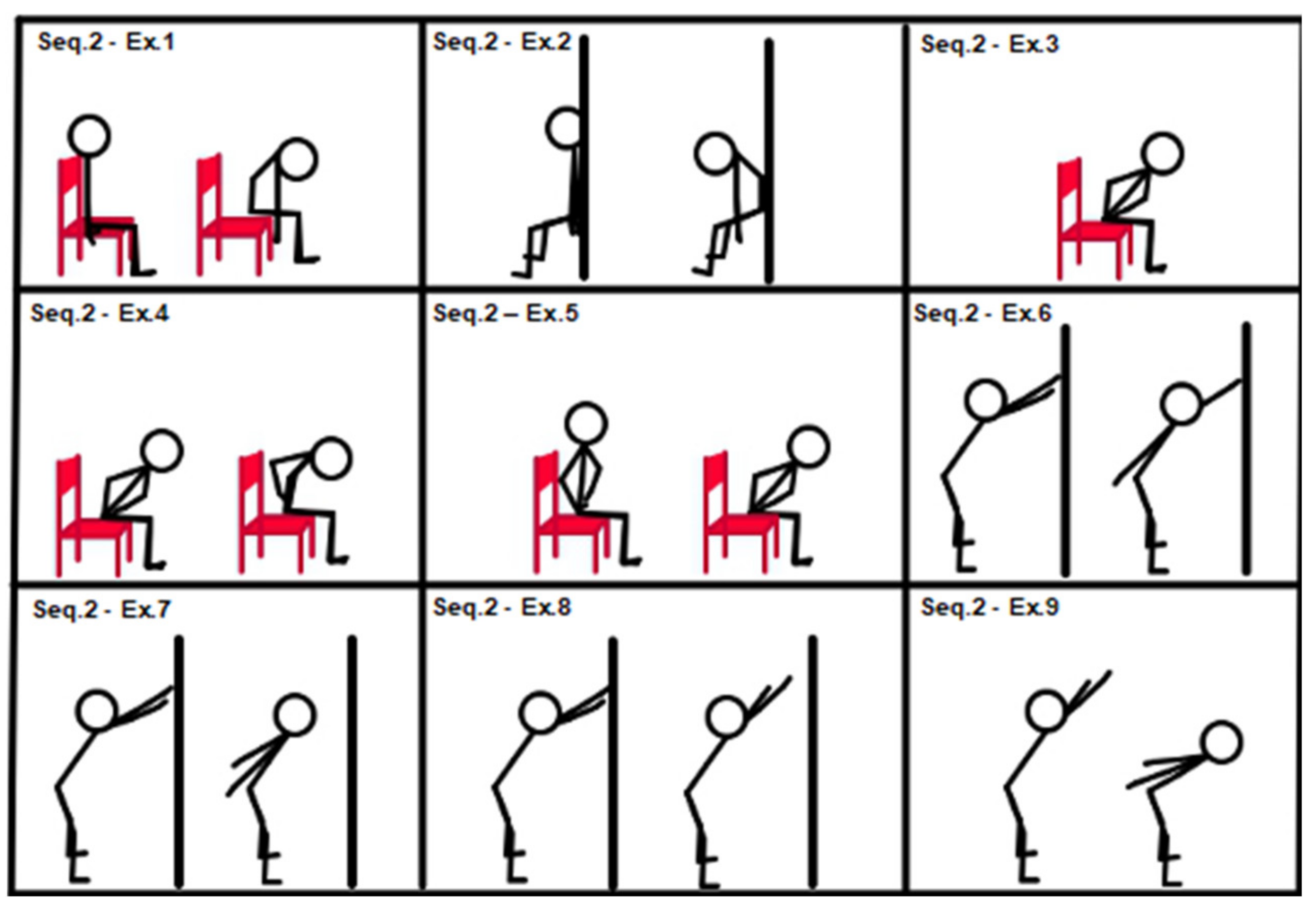
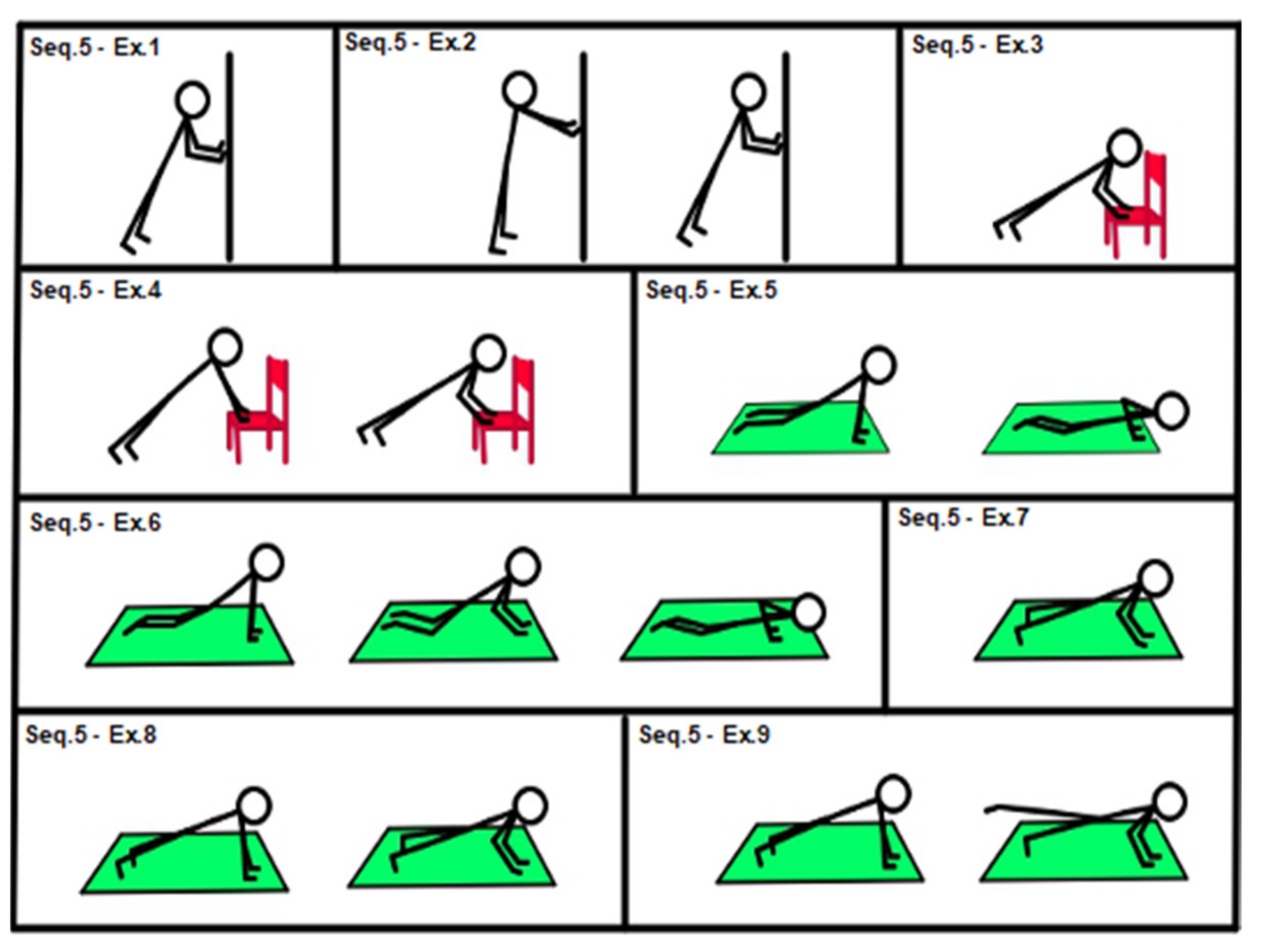
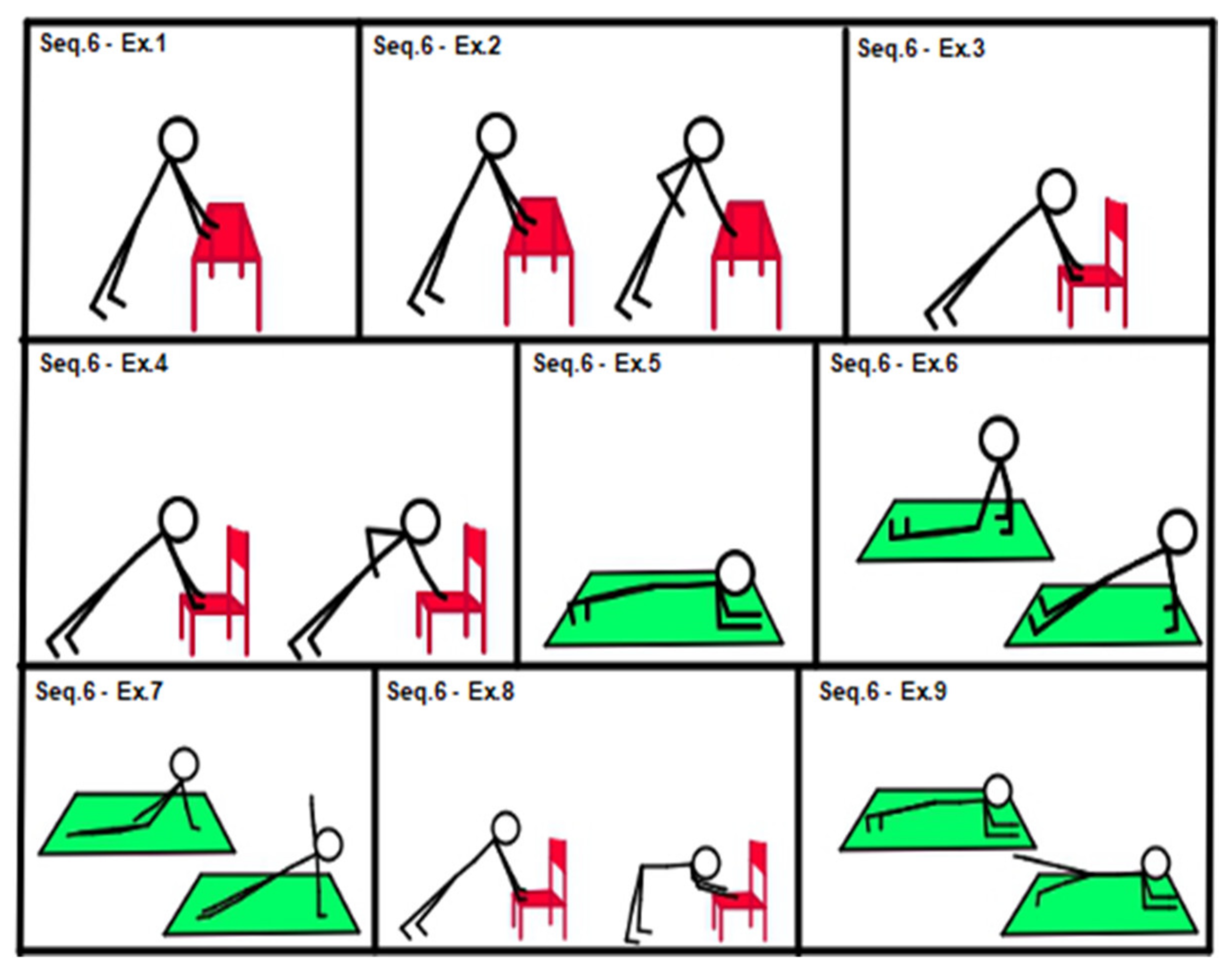
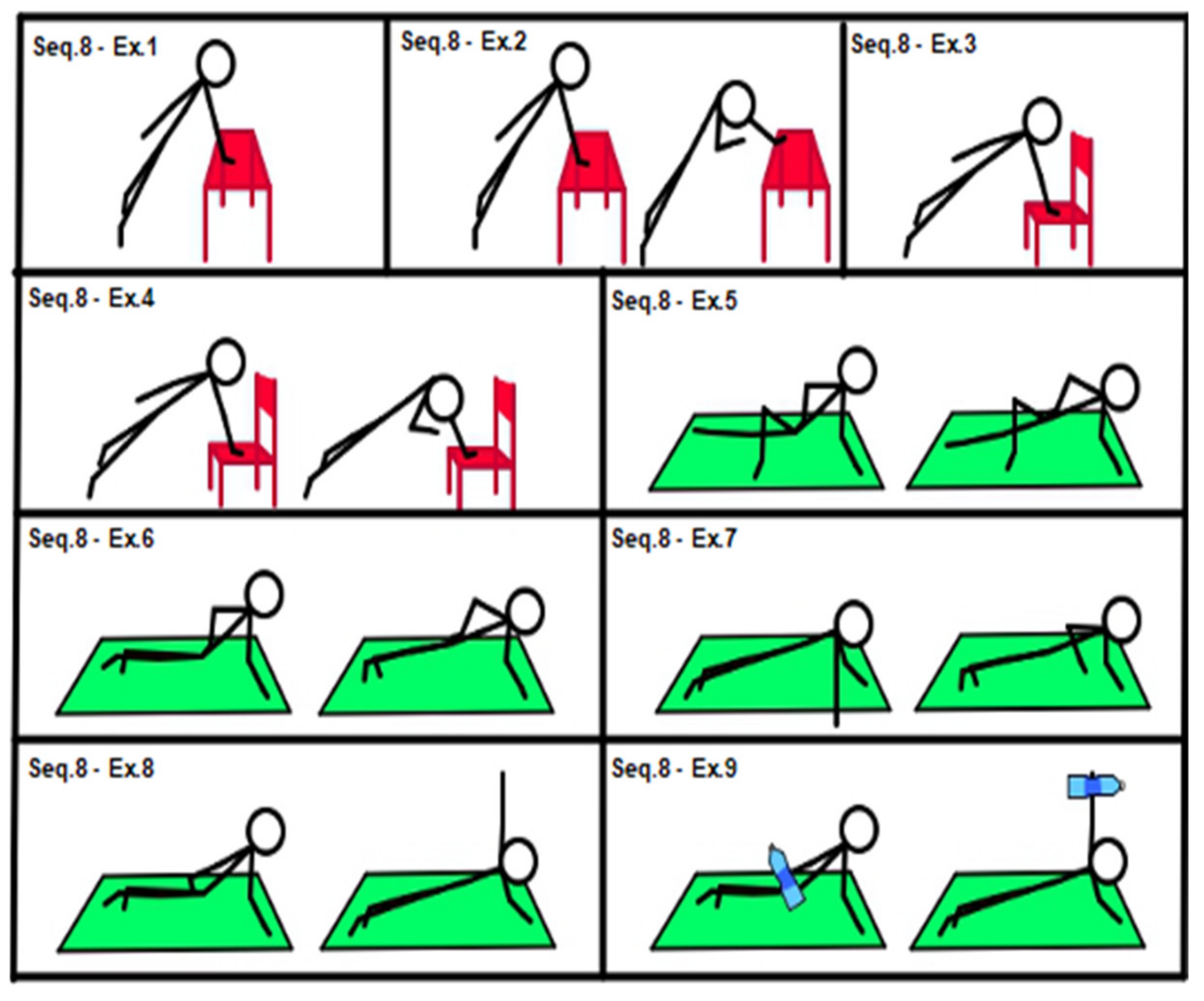
2.3. Intervention
Exercises and Sequences
2.4. Experimental Procedure
2.4.1. Study Protocol
2.4.2. Tests
2.4.3. Training Progression
2.4.4. Statistical Analysis
3. Results
4. Discussion
4.1. Feasibility
4.2. Strength, Functional Ability and Well-Being Effects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thiebaud, R.S.; Funk, M.D.; Abe, T. Home-based resistance training for older adults: A systematic review. Geriatr. Gerontol. Int. 2014, 14, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Campo, G.; Tonet, E.; Chiaranda, G.; Sella, G.; Maietti, E.; Bugani, G.; Vitali, F.; Serenelli, M.; Mazzoni, G.; Ruggiero, R.; et al. Exercise intervention improves quality of life in oldera dults after myocardial infarction: Randomised clinical trial. Heart 2020, 106, 1658–1664. [Google Scholar] [CrossRef] [PubMed]
- McCarty, N.P.; Craighead, D.H.; Freeberg, K.A. Overcoming exercise barriers: Home-based HIT for reducing cardiovascular disease risk in obese individuals. J. Physiol. 2020, 598, 13–14. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Xu, L.; Tian, X.; Wang, S.; Liu, X.; Dai, Y.; Kang, L.; Chen, L.; Jin, L.; Li, Q.; et al. The comparative efficacy of supervised versus home-based exercise programs in patients with ankylosing spondylitis: A meta-analysis. Medicine 2020, 99, e19229. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Pan, J.; Qian, Y. Home-Based Physical Therapy for Older Adults after Hip Fracture. JAMA 2020, 323, 378–379. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, T.L.; Jakobsen, M.D.; Andersen, L.L.; Husted, H.; Kehlet, H.; Bandholm, T. Quadriceps muscle activity during commonly used strength training exercises shortly after total knee arthroplasty: Implications for home-based exercise-selection. J. Exp. Orthop. 2019, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Flynn, A.; Allen, N.E.; Dennis, S.; Canning, C.G.; Preston, E. Home-based prescribed exercise improves balance-related activities in people with Parkinson’s disease and has benefits similar to centre-based exercise: A systematic review. J. Physiother. 2019, 65, 189–199. [Google Scholar] [CrossRef]
- Perrochon, A.; Borel, B.; Istrate, D.; Compagnat, M.; Daviet, J.C. Exercise-based games interventions at home in individuals with a neurological disease: A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2019, 62, 366–378. [Google Scholar] [CrossRef]
- Mahmood, A.; Solomon, J.M.; English, C.; Bhaskaran, U.; Menon, G.; Manikandan, N. Measurement of adherence to home-based exercises among community-dwelling stroke survivors in India. Physiother. Res. Int. 2019, 25, e1827. [Google Scholar] [CrossRef]
- Weller, S.; Oliffe, J.L.; Campbell, K.L. Factors associated with exercise preferences, barriers and facilitators of prostate cancer survivors. Eur. J. Cancer Care 2019, 28, e13135. [Google Scholar] [CrossRef]
- Parker, N.H.; Lee, R.E.; O’Connor, D.P.; Ngo-Huang, A.; Petzel MQ, B.; Schadler, K.; Wang, X.; Xiao, L.; Fogelman, D.; Simpson, R.; et al. Supports and Barriers to Home-Based Physical Activity During Preoperative Treatment of Pancreatic Cancer: A Mixed-Methods Study. J. Phys. Act. Health 2019, 16, 1113–1122. [Google Scholar] [CrossRef]
- Larsen, R.F.; Jarden, M.; Minet, L.R.; Frølund, U.C.; Abildgaard, N. Supervised and home-based physical exercise in patients newly diagnosed with multiple myeloma-a randomized controlled feasibility study. Pilot Feasibility Stud. 2019, 5, 130. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Caplan, L.; Stone, R.; Stewart, J. A review of home-based physical activity interventions for breast cancer survivors. Curr. Cancer Rep. 2019, 1, 6–12. [Google Scholar] [CrossRef]
- Liu, X.; Li, P.; Li, J.; Xiao, L.; Li, N.; Lu, Y.; Wang, Z.; Su, J.; Wang, Z.; Shan, C.; et al. Home-Based Prescribed Pulmonary Exercise in Patients with Stable Chronic Obstructive Pulmonary Disease. J. Vis. Exp. 2019, 24, 150. [Google Scholar] [CrossRef] [PubMed]
- Rolving, N.; Brocki, B.C.; Bloch-Nielsen, J.R.; Larsen, T.B.; Jensen, F.L.; Mikkelsen, H.R.; Ravn, P.; Frost, L. Effect of a Physiotherapist-Guided Home-Based Exercise Intervention on Physical Capacity and Patient-Reported Outcomes Among Patients With Acute Pulmonary Embolism: A Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200064. [Google Scholar] [CrossRef]
- Scott, S.N.; Shepherd, S.O.; Strauss, J.A.; Wagenmakers AJ, M.; Cocks, M. Home-based high-intensity interval training reduces barriers to exercise in people with type 1 diabetes. Exp. Physiol. 2020, 105, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Frimpong, E.; Dafkin, C.; Donaldson, J.; Millen AM, E.; Meiring, R.M. The effect of home-based low-volume, high-intensity interval training on cardiorespiratory fitness, body composition and cardiometabolic health in women of normal body mass and those with overweight or obesity: Protocol for a randomized controlled trial. BMC Sports Sci. Med. Rehabil. 2019, 30, 11–39. [Google Scholar] [CrossRef]
- Kelly, L.; Holmberg, P.M.; Schroeder, E.T.; Loza, A.; Lin, X.; Moody, A.; Hughes, A.; Gibson, A.; Kirk, A. Effect of home-based strength training program on IGF-I, IGFBP-1 and IGFBP-3 in obese Latino boys participating in a 16-week randomized controlled trial. J. Pediatr. Endocrinol. Metab 2019, 32, 1121–1129. [Google Scholar] [CrossRef]
- Pepera, G.; Mpea, C.; Krinta, K.; Peristeropoulos, A.; Antoniou, V. Effects of multicomponent exercise training intervention on hemodynamic and physical function in older residents of long-term care facilities: A multicenter randomized clinical controlled trial. J. Bodyw. Mov. Ther. 2021, 28, 231–237. [Google Scholar] [CrossRef]
- Pepera, G.; Krinta, K.; Mpea, C.; Antoniou, V.; Peristeropoulos, A.; Dimitriadis, Z. Randomized Controlled Trial of Group Exercise Intervention for Fall Risk Factors Reduction in Nursing Home Residents. Can J. Aging 2022, 11, 1–9. [Google Scholar] [CrossRef]
- Bernocchi, P.; Giordano, A.; Pintavalle, G.; Galli, T.; Ballini Spoglia, E.; Baratti, D.; Scalvini, S. Feasibility and clinical efficacy of a multidisciplinary hometelehealth program to prevent falls in older adults: A randomized controlled trial. J. Am. Med. Dir. Assoc. 2019, 20, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Cederbom, S.; Bjerk, M.; Bergland, A. A qualitative study exploring physical therapists’ views on the Otago Exercise Programme for fall prevention: A stepping stone to “age in place” and to give faith in the future. Physiother. Theory Pract. 2020, 24, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Turunen, K.M.; Aaltonen-Määttä, L.; Törmäkangas, T.; Rantalainen, T.; Portegijs, E.; Keikkala, S.; Kinnunen, M.; Finni, T.; Sipilä, S.; Nikander, R. Effects of an individually targeted multicomponent counseling and home-based rehabilitation program on physical activity and mobility in community-dwelling older people after discharge from hospital: A randomized controlled trial. Clin. Rehabil. 2020, 34, 491–503. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, T.J.; Su, S.C.; Chen, C.W.; Kang, Y.W.; Hu, M.H.; Hsu, L.L.; Wu, S.Y.; Chen, L.; Chang, H.Y.; Chuang, S.Y.; et al. Individualized home-based exercise and nutrition interventions improve frailty in older adults: A randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 119. [Google Scholar] [CrossRef]
- Miller, K.L.; Magel, J.R.; Hayes, J.G. The effects of a home-based exercise program on balance confidence, balance performance, and gait in debilitated, ambulatory community-dwelling older adults: A pilot study. J. Geriatr. Phys. Ther. 2010, 33, 85–91. [Google Scholar]
- Lockwood, K.J.; Harding, K.E.; Boyd, J.N.; Taylor, N.F. Home visits by occupational therapists improve adherence to recommendations: Process evaluation of a randomised controlled trial. Aust. Occup. Ther. J. 2020, 67, 287–296. [Google Scholar] [CrossRef]
- Winser, S.J.; Chan HT, F.; Ho, L.; Chung, L.S.; Ching, L.T.; Felix TK, L.; Kannan, P. Dosage for cost-effective exercise-based falls prevention programs for older people: A systematic review of economic evaluations. Ann. Phys. Rehabil. Med. 2020, 63, 69–80. [Google Scholar] [CrossRef]
- Frei, A.; Radtke, T.; Dalla Lana, K.; Braun, J.; Müller, R.M.; Puhan, M.A. Effects of a long-term home-based exercise training programme using minimal equipment vs. usual care in COPD patients: A study protocol for two multicenter randomised controlled trials (HOMEX-1 and HOMEX-2 trials). BMC Pulm. Med. 2019, 19, 57. [Google Scholar] [CrossRef]
- Jones, C.J.; Rikli, R.E.; Beam, W.C. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res. Q. Exerc. Sport 1999, 70, 113–119. [Google Scholar] [CrossRef]
- Bohannon, R.W. Muscle Strength: Clinical and Prognostic Value of Hand-Grip Dynamometry. Curr. Opin. Clin. Nutr. Metab Care 2015, 18, 465–470. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The “Up and go”: A test of basic functional mobility for frail elderly persons. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Lemmink KA, P.M.; Kemper HC, G.; de Greef MH, G.; Rispens, P.; Stevens, M. The Validity of the Sit-And-Reach Test and the Modified Sit-And-Reach Test in Middle-Aged to Older Men and Women. Res. Q. Exerc. Sport 2003, 74, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.P.; Chapman, L.J.; Allen, J.J. The measurement of foot preference. Neuropsychologia 1987, 25, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Seco, J.; Abecia, L.C.; Echevarría, E.; Barbero, I.; Torres-Unda, J.; Rodriguez, V.; Calvo, J.I. A long-term physical activity training program increases strength and flexibility, and improves balance in older adults. Rehabil. Nurs. 2013, 38, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Burgel, B.J.; Elshatarat, R.A. Psychosocial Work Factors and Low Back Pain in Taxi Drivers. Am. J. Ind. Med. 2017, 60, 734–746. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Tsubaki, A.; Nakamura, M.; Nashimoto, S.; Fu, J.B.; Onishi, H. Rating of perceived exertion on resistance training in elderly subjects. Rev. Expert Rev. Cardiovasc. 2019, 17, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Voutilainen, A.; Pitkäaho, T.; Kvist, T.; Vehviläinen-Julkunen, K. How to ask about patient satisfaction? The visual analogue scale is less vulnerable to confounding factors and ceiling effect than a symmetric Likert scale. J. Adv. Nurs. 2016, 72, 946–957. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Spring, B.; Berger, J.S.; Treat-Jacobson, D.; Conte, M.S.; Creager, M.A.; Criqui, M.H.; Ferrucci, L.; Gornik, H.L.; Guralnik, J.M.; et al. Effect of a Home-Based Exercise Intervention of Wearable Technology and Telephone Coaching on Walking Performance in Peripheral Artery Disease. JAMA 2018, 319, 1665–1676. [Google Scholar] [CrossRef]
- Echeverria, I.; Amasene, M.; Urquiza, M.; Labayen, I.; Anaut, P.; Rodriguez-Larrad, A.; Irazusta, J.; Besga, A. Multicomponent Physical Exercise in Older Adults after Hospitalization: A Randomized Controlled Trial Comparing Short- vs. Long-Term Group-Based Interventions. Int. J. Environ. Res. Public Health 2020, 17, 666. [Google Scholar] [CrossRef]
- Chen, B.; Hu, N.; Tan, J.H. Efficacy of home-based exercise programme on physical function after hip fracture: A systematic review and meta-analysis of randomised controlled trials. Int. Wound J. 2020, 17, 45–54. [Google Scholar] [CrossRef]
- Mendes, J.; Amaral, T.F.; Borges, N.; Santos, A.; Padrão, P.; Moreira, P.; Afonso, C.; Negrão, R. Handgrip Strength Values of Portuguese Older Adults: A Population Based Study. BMC Geriatr. 2017, 17, 191. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Billis, E.; Tsepis, E.; Dimitriadis, Z.; Matzaroglou, C.; Tyllianakis, M.; Panagiotopoulos, E.; Gliatis, J. The Effects of Group and Home-Based Exercise Programs in Elderly With Sarcopenia: A Randomized Controlled Trial. J. Clin. Med. 2018, 7, 480. [Google Scholar] [CrossRef] [PubMed]
- Jeeyoung, H.; Jeongeun Ki Suk Wha, K.; Hyoun-Joong, K. Effects of Home-Based Tele-Exercise on Sarcopenia Among Community-Dwelling Elderly Adults: Body Composition and Functional Fitness. Exp. Gerontol. 2017, 87, 33–39. [Google Scholar]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise Prescription for Patients With Multiple Sclerosis; Potential Benefits and Practical Recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef]
- Rodríguez, A.C.; Chinchilla-Minguet, J.L. Cardiovascular Program to Improve Physical Fitness in Those Over 60 Years Old—Pilot Study. Clin. Interv. Aging 2014, 9, 1269–1275. [Google Scholar]
- Cummings, S.R.; Studenski, S.; Ferrucci, L. A Diagnosis of Dismobility-Giving Mobility Clinical Visibility: A Mobility Working Group Recommendation. JAMA 2014, 311, 2061–2062. [Google Scholar] [CrossRef]
- Rodríguez-Lozano, C.; Juanola, X.; Cruz-Martínez, J.; Peña-Arrébola, A.; Mulero, J.; Gratacós, J.; Collantes, E.; Spondyloarthropathies Study Group of the Spanish Society of Rheumatologyet. Outcome of an Education and Home-Based Exercise Programme for Patients With Ankylosing Spondylitis: A Nationwide Randomized Study. Clin. Exp. Rheumatol. 2013, 31, 739–748. [Google Scholar]
- Domb, B.G.; Sgroi, T.A.; VanDevender, J.C. Physical Therapy Protocol After Hip Arthroscopy: Clinical Guidelines Supported by 2-Year Outcomes. Sports Health 2016, 8, 347–354. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TOT n = 69 | FEMALE n = 44 | MALE n = 25 | MEAN |
|---|---|---|---|
| NATIONALITY | ITALIAN | ITALIAN | |
| EMPLOYMENT STATUS | RETIRED | RETIRED | ----- |
| AGE (years) | 71.8 ± 0.9 | 74.5 ± 1.2 | 72.5 ± 5.1 |
| HEIGHT (cm) | 159.1 ± 7.0 | 169.3 ± 8.3 | 163.3 ± 11.5 |
| BODY MASS (kg) | 68.9 ± 12.2 | 78.8 ± 11.5 | 73.6 ± 13.1 |
| BMI | 27.3 ± 5.0 | 27.5 ± 3.8 | 27.3 ± 4.4 |
| I.G. (n 67) | Comments | |
|---|---|---|
| Adherence to HT exercise session | ||
| Patients who completed (n (%)) | 48 (72%) | Private reasons, slightly seasonal illnesses |
| Sessions completed (n (%)) | 1543 (96%) | |
| Adjustments of the exercise program | ||
| Progression of exercise program (n (%)) | 65 (97%) | |
| Regression of exercise program (n (%)) | 0 | |
| No progression or regression (n (%)) | 0 | |
| Both progression and regression (n (%)) | 2 (3%) | |
| Diary registration (n (%)) | ||
| All weeks | 59 (88%) | |
| Some weeks | 8 (12%) | |
| No weeks | 0 | |
| Adverse events (n) | 8 | Low back pain: 4; knee pain: 3; shoulder pain: 1 |
| Consequences of the adverse events | ||
| None | 7 | |
| Discontinuation of the supervised exercise session (n) | 1 |
| CHAIR TEST (reps) | HAND GRIP (kg) | TUG (sec) | SIT and REACH (cm) | STORK TEST (sec) | PPE (A.U. 0–10) | VAS (A.U. 1–10) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | |
| mean | 12.7 | 16.6 | 21.2 | 22.4 | 7.7 | 6.4 | −6.9 | −3.1 | 20.7 | 34.2 | 4.2 | 1.3 | 5.3 | 3.5 |
| sd | 3.7 | 4.6 | 6.8 | 7.8 | 2.3 | 1.7 | 2.5 | 1.8 | 9.1 | 11.3 | 1.1 | 0.5 | 2.3 | 2.4 |
| effect size | −0.9 | −0,2 | 0.7 | −1.8 | −1.3 | 3.4 | 0.8 | |||||||
| percentage | 31 | 6 | −17 | 55 | 65 | −69 | −34 | |||||||
| p value | 0.001 * | 0.001 * | 0.001 * | 0.001 * | 0.001 * | 0.001 * | 0.001 * | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melchiorri, G.; Triossi, T.; Viero, V.; Marroni, S.; D’Arcangelo, G.; Tancredi, V. A Study about a New Standardized Method of Home-Based Exercise in Elderly People Aged 65 and Older to Improve Motor Abilities and Well-Being: Feasibility, Functional Abilities and Strength Improvements. Geriatrics 2022, 7, 134. https://doi.org/10.3390/geriatrics7060134
Melchiorri G, Triossi T, Viero V, Marroni S, D’Arcangelo G, Tancredi V. A Study about a New Standardized Method of Home-Based Exercise in Elderly People Aged 65 and Older to Improve Motor Abilities and Well-Being: Feasibility, Functional Abilities and Strength Improvements. Geriatrics. 2022; 7(6):134. https://doi.org/10.3390/geriatrics7060134
Chicago/Turabian StyleMelchiorri, Giovanni, Tamara Triossi, Valerio Viero, Silvia Marroni, Giovanna D’Arcangelo, and Virginia Tancredi. 2022. "A Study about a New Standardized Method of Home-Based Exercise in Elderly People Aged 65 and Older to Improve Motor Abilities and Well-Being: Feasibility, Functional Abilities and Strength Improvements" Geriatrics 7, no. 6: 134. https://doi.org/10.3390/geriatrics7060134
APA StyleMelchiorri, G., Triossi, T., Viero, V., Marroni, S., D’Arcangelo, G., & Tancredi, V. (2022). A Study about a New Standardized Method of Home-Based Exercise in Elderly People Aged 65 and Older to Improve Motor Abilities and Well-Being: Feasibility, Functional Abilities and Strength Improvements. Geriatrics, 7(6), 134. https://doi.org/10.3390/geriatrics7060134