
Malnutrition–Sarcopenia Syndrome and Self-Management Behaviors in Continuing-Care Retirement Community Residents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurement
2.2. Malnutrition Assessment
2.3. Sarcopenia Assessment
2.4. Sedentary and Physical Activity Behavior Assessment
2.5. Protein and Caloric Intake Assessment
2.6. Self-Efficacy for Physical Activity Assessment
2.7. Aging Expectations Assessment
2.8. Other Measures
2.9. Statistical Analysis
3. Results
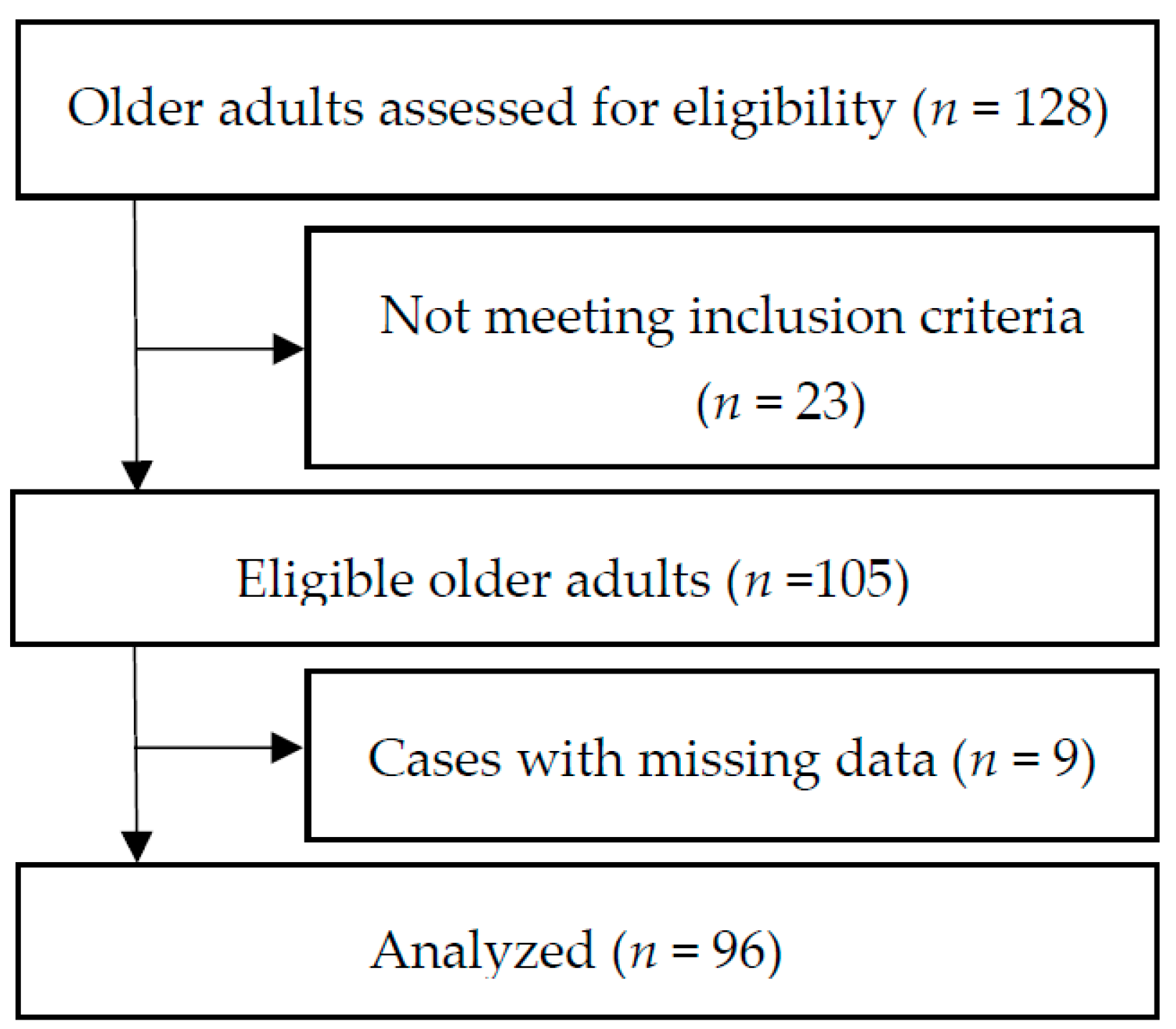
3.1. Characteristics of Study Sample
3.2. Sarcopenia, Malnutrition, and MMS
3.3. Comparison of Characteristics between with MSS and without MSS
3.4. Factors Associated with MMS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruyère, O.; Beaudart, C.; Locquet, M.; Buckinx, F.; Petermans, J.; Reginster, J.Y. Sarcopenia as a public health problem. Eur. Geriatr. Med. 2016, 7, 272–275. [Google Scholar] [CrossRef]
- Plotkin, A.; Taani, M.H. Factors associated with food intake, nutritional status, and function among nursing home residents with dementia. Geriatr. Nurs. 2020, 41, 559–563. [Google Scholar] [CrossRef]
- Papadopoulou, S.; Tsintavis, P.; Potsaki, G.; Papandreou, D. Differences in the Prevalence of Sarcopenia in Community-Dwelling, Nursing Home and Hospitalized Individuals. A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2020, 24, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Leij-Halfwerk, S.; Verwijs, M.; van Houdt, S.; Borkent, J.; Guaitoli, P.R.; Pelgrim, T.; Heymans, M.; Power, L.; Visser, M.; Corish, C.; et al. Prevalence of protein-energy malnutrition risk in European older adults in community, residential and hospital settings, according to 22 malnutrition screening tools validated for use in adults ≥65 years: A systematic review and meta-analysis. Maturitas 2019, 126, 80–89. [Google Scholar] [CrossRef]
- Vandewoude, M.F.J.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-Sarcopenia Syndrome: Is This the Future of Nutrition Screening and Assessment for Older Adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef]
- Taani, M.H.; Siglinsky, E.; Kovach, C.R.; Buehring, B. Psychosocial Factors Associated With Reduced Muscle Mass, Strength, and Function in Residential Care Apartment Complex Residents. Res. Gerontol. Nurs. 2018, 11, 238–248. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Liang, C.-K.; Hsu, Y.-H.; Peng, L.-N.; Chu, C.-S.; Liao, M.-C.; Shen, H.-C.; Chou, M.-Y.; Lin, Y.-T. Synergistic effect of low handgrip strength and malnutrition on 4-year all-cause mortality in older males: A prospective longitudinal cohort study. Arch. Gerontol. Geriatr. 2019, 83, 217–222. [Google Scholar] [CrossRef]
- Lardiés-Sánchez, B.; Sanz-París, A.; Pérez-Nogueras, J.; Serrano-Oliver, A.; Torres-Anoro, M.E.; Cruz-Jentoft, A.J. Influence of nutritional status in the diagnosis of sarcopenia in nursing home residents. Nutrition 2017, 41, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Freire, A.N.; Guerra, R.; Alvarado, B.; Guralnik, J.M.; Zunzunegui, M.-V. Validity and Reliability of the Short Physical Performance Battery in Two Diverse Older Adult Populations in Quebec and Brazil. J. Aging Health 2012, 24, 863–878. [Google Scholar] [CrossRef]
- Ryan, P.; Sawin, K.J. The Individual and Family Self-Management Theory: Background and perspectives on context, process, and outcomes. Nurs. Outlook 2009, 57, 217–225.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Sheikh, J.I.; Yesavage, J.A. 9/Geriatric Depression Scale (GDS) recent evidence and development of a shorter version. Clin. Gerontol. J. Aging Ment. Health 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Villars, H.; Soto, M.; Morley, J.E. Over view of the MNA-Its history and challenges. J. Nutr. Health Aging 2005, 10, 456–465. [Google Scholar]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment Short-Form (MNA®-SF): A practical tool for identification of nutritional status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Isautier, J.M.; Bosnić, M.; Yeung, S.S.; Trappenburg, M.C.; Meskers, C.; Whittaker, A.C.; Maier, A.B. Validity of Nutritional Screening Tools for Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2019, 20, 1351.e13–1351.e25. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Watanabe, Y.; Ikenaga, M.; Yokoyama, K.; Yoshida, T.; Morimoto, T.; Kimura, M. Comparison of single- or multifrequency bioelectrical impedance analysis and spectroscopy for assessment of appendicular skeletal muscle in the elderly. J. Appl. Physiol. 2013, 115, 812–818. [Google Scholar] [CrossRef] [Green Version]
- Sergi, G.; De Rui, M.; Veronese, N.; Bolzetta, F.; Berton, L.; Carraro, S.; Bano, G.; Coin, A.; Manzato, E.; Perissinotto, E. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin. Nutr. 2015, 34, 667–673. [Google Scholar] [CrossRef]
- Mathiowetz, V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup. Ther. Int. 2002, 9, 201–209. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: As-Sociation with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Matthews, C.E. Calibration of accelerometer output for adults. Med. Sci. Sports Exerc. 2005, 37 (Suppl. 11), S512–S522. [Google Scholar] [CrossRef] [PubMed]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Block, G.; Hartman, A.M.; Naughton, D. A Reduced Dietary Questionnaire: Development and Validation. Epidemiology 1990, 1, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Boucher, B.; Cotterchio, M.; Kreiger, N.; Nadalin, V.; Block, T.; Block, G. Validity and reliability of the Block98 food-frequency questionnaire in a sample of Canadian women. Public Health Nutr. 2006, 9, 84–93. [Google Scholar] [CrossRef]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.C.; Stehle, P.; Teta, D.; et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People: A Position Paper From the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids; National Academies: Washington, DC, USA, 2005. [Google Scholar]
- Haas, B.K.; Northam, S. Measuring self-efficacy: Development of the Physical Activity Assessment Inventory. South. Online J. Nurs. Res. 2010, 10, 35–51. [Google Scholar]
- Im, E.-O.; Chee, W.; Lim, H.-J.; Liu, Y.; Kim, H.K. Midlife Women’s Attitudes Toward Physical Activity. J. Obstet. Gynecol. Neonatal Nurs. 2008, 37, 203–213. [Google Scholar] [CrossRef]
- Sarkisian, C.A.; Hays, R.D.; Berry, S.; Mangione, C.M. Development, reliability, and validity of the expectations regarding aging (ERA-38) survey. Gerontologist 2002, 42, 534–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ware, J. SF-36 Physical and Mental Health Summary Scales: A User’s Manual; Health Institute New England Medical Center: Boston, MA, USA, 1994. [Google Scholar]
- Richardson, S. The Timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Nishioka, S.; Matsushita, T.; Yamanouchi, A.; Okazaki, Y.; Oishi, K.; Nishioka, E.; Mori, N.; Tokunaga, Y.; Onizuka, S. Prevalence and associated factors of coexistence of malnutrition and sarco-penia in geriatric rehabilitation. Nutrition 2021, 13, 3745. [Google Scholar]
- Gümüşsoy, M.; Atmış, V.; Yalçın, A.; Bahşi, R.; Yiğit, S.; Arı, S.; Dokuyan, H.C.; Gözükara, M.G.; Silay, K. Malnutrition-sarcopenia syndrome and all-cause mortality in hospitalized older people. Clin. Nutr. 2021, 40, 5475–5481. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, L.; Wang, H.; Hao, Q.; Dong, B.; Yang, M. Malnutrition-Sarcopenia syndrome predicts mortality in hospitalized older patients. Sci. Rep. 2017, 7, 3171. [Google Scholar] [CrossRef] [Green Version]
- Faxén-Irving, G.; Luiking, Y.; Grönstedt, H.; Franzén, E.; Seiger, Å.; Vikström, S.; Wimo, A.; Boström, A.-M.; Cederholm, T. Do Malnutrition, Sarcopenia and Frailty Overlap in Nursing-Home Residents? J. Frailty Aging 2021, 10, 17–21. [Google Scholar] [CrossRef]
- Bosaeus, I.; Rothenberg, E. Nutrition and physical activity for the prevention and treatment of age-related sarcopenia. Proc. Nutr. Soc. 2015, 75, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; The IOF-ESCEO Sarcopenia Working Group; Dawson, A.; Shaw, S.C.; Harvey, N.; Kanis, J.A.; Binkley, N.; Reginster, J.Y.; Chapurlat, R.; Chan, D.C.; et al. Nutrition and physical activity in the prevention and treatment of sarcopenia: Systematic review. Osteoporos. Int. 2017, 28, 1817–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martone, A.M.; Marzetti, E.; Calvani, R.; Picca, A.; Tosato, M.; Santoro, L.; Di Giorgio, A.; Nesci, A.; Sisto, A.; Santoliquido, A.; et al. Exercise and Protein Intake: A Synergistic Approach against Sarcopenia. BioMed. Res. Int. 2017, 2017, 2672435. [Google Scholar] [CrossRef] [PubMed]
- Thivel, D.; Tremblay, A.; Genin, P.M.; Panahi, S.; Riviere, D.; Duclos, M. Physical Activity, Inactivity, and Sedentary Behaviors: Definitions and Implications in Occupational Health. Front. Public Health 2018, 6, 288. [Google Scholar] [CrossRef]
- Leung, P.-M.; Ejupi, A.; Van Schooten, K.S.; Aziz, O.; Feldman, F.; Mackey, D.C.; Ashe, M.C.; Robinovitch, S.N. Association between Sedentary Behaviour and Physical, Cognitive, and Psychosocial Status among Older Adults in Assisted Living. BioMed Res. Int. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Smith, L.; Thomas, E.L.; Bell, J.D.; Hamer, M. The association between objectively measured sitting and standing with body composi-tion: A pilot study using MRI. BMJ Open 2014, 4, e005476. [Google Scholar] [CrossRef]
- Smith, L.; Tully, M.; Jacob, L.; Blackburn, N.; Adlakha, D.; Caserotti, P.; Soysal, P.; Veronese, N.; Sánchez, G.F.L.; Vancampfort, D.; et al. The Association Between Sedentary Behavior and Sarcopenia Among Adults Aged ≥65 Years in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2020, 17, 1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levy, B.R.; Slade, M.D.; Kunkel, S.R.; Kasl, S.V. Longevity increased by positive self-perceptions of aging. J. Pers. Soc. Psychol. 2002, 83, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Meisner, B.A.; Baker, J. An exploratory analysis of aging expectations and health care behavior among aging adults. Psychol. Aging 2013, 28, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Locher, J.L.; Burgio, K.L.; Goode, P.S.; Roth, D.L.; Rodriguez, E. Effects of Age and Causal Attribution to Aging on Health-Related Behaviors Associated With Urinary Incontinence in Older Women. Gerontologist 2002, 42, 515–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, T.L.; Chipperfield, J.; Perry, R.P.; Weiner, B. Attributing illness to ‘old age’: Consequences of a self-directed stereotype for health and mortality. Psychol. Health 2012, 27, 881–897. [Google Scholar] [CrossRef]
- Stewart, T.L.; Chipperfield, J.; Perry, R.P.; Hamm, J.M. Attributing heart attack and stroke to “Old Age”: Implications for subsequent health outcomes among older adults. J. Health Psychol. 2016, 21, 40–49. [Google Scholar] [CrossRef]
- Sarkisian, C.A.; Prohaska, T.R.; Wong, M.D.; Hirsch, S.; Mangione, C.M. The relationship between expectations for aging and physical activity among older adults. J. Gen. Intern. Med. 2005, 20, 911–915. [Google Scholar] [CrossRef] [Green Version]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Russo, A.; Bernabei, R.; Onder, G. Prevalence and Risk Factors of Sarcopenia Among Nursing Home Older Residents. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2012, 67, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Keller, K.; Engelhardt, M. Strength and muscle mass loss with aging process. Age and strength loss. Muscle Ligaments Tendons J. 2019, 3, 346–350. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Total Sample (n = 96, 100%) | No MSS (n = 84, 87.5%) | MSS (n = 12, 12.5%) | p-Value (No MSS vs. MSS) |
|---|---|---|---|---|
| Age (years) | 82.5 ± 7.4 | 81.9 ± 7.2 | 86.1 ± 8.4 | 0.074 |
| BMI | 26.1 ± 6.1 | 27.12 ± 5.8 | 20.26 ± 1.2 | <0.001 |
| Gender | 0.686 | |||
| Female | 79 (82.3) | 68 (81.0) | 11 (91.7) | |
| Male | 17 (17.7) | 16 (19) | 1 (8.3) | |
| Race | 0.207 | |||
| White or Caucasian | 78 (81.3) | 68 (81.0) | 10 (83.3) | |
| Black or African American | 16 (16.7) | 15 (17.9) | 1 (8.3) | |
| American Indian/Alaska Native | 2 (2.1) | 1 (1.2) | 1 (8.3) | |
| Marital Status | 0.298 | |||
| Never married or single | 4 (4.2) | 3 (3.6) | 1 (8.3) | |
| Married | 18 (18.8) | 18 (21.4) | 0 (0) | |
| Divorced or separated | 17 (17.7) | 14 (16.7) | 3 (25.0) | |
| Widowed | 57 (59.4) | 49 (58.3) | 8 (66.7) | |
| Education Level | 0.742 | |||
| High school or below | 28 (29.2) | 24 (28.6) | 4 (33.3) | |
| College and above | 68 (70.8) | 60 (71.4) | 8 (66.7) | |
| Falls | 0.313 | |||
| Yes | 43 (44.8) | 36 (42.9) | 7 (58.3) | |
| No | 53 (55.2) | 48 (57.1) | 5 (41.7) | |
| Smoking Status | 0.624 | |||
| Current smokers | 11 (11.5) | 9 (10.7) | 2 (16.7) | |
| Non-current smokers | 85 (88.5) | 75 (89.3) | 10 (83.3) | |
| Nutrition Status | <0.001 | |||
| Normal | 62 (64.6) | 62 (73.8) | 0 (0) | |
| Malnutrition risk | 21 (21.9) | 21 (25.0) | 0 (0) | |
| Malnutrition | 13 (13.4) | 1 (1.2) | 12 (100) | |
| Sarcopenia Status | 0.004 | |||
| No | 60 (62.5) | 60 (71.4) | 0 (0) | |
| Yes | 36 (37.5) | 24 (28.6) | 12 (100) | |
| Protein Intake | 0.437 | |||
| Yes | 42 (43.8) | 38 (45.2) | 4 (33.3) | |
| No | 54 (56.3) | 46 (54.8) | 8 (66.7) | |
| Caloric Intake | 0.167 | |||
| Yes | 33 (34.4) | 31 (36.9) | 2 (16.7) | |
| No | 63 (65.6) | 53 (63.1) | 10 (83.3) | |
| Number of chronic conditions | 4.8 ± 5.4 | 4.6 ± 5.4 | 5.6 ± 5.3 | 0.598 |
| Handgrip strength (kg) | 19.0 ± 6.9 | 19.9 ± 6.7 | 11.9 ± 3.7 | <0.001 |
| Body fat % | 37.5 ± 7.2 | 39.1 ± 5.5 | 37.26 ± 7.4 | 0.403 |
| ASMM (kg) | 16.0 ± 3.6 | 16.4 ± 3.7 | 13.2 ± 2.1 | <0.001 |
| Gait speed (m/s) | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.57 ± 0.2 | 0.016 |
| SPPB | 7.9 ± 2.6 | 8.2 ± 2.5 | 5.83 ± 2.7 | 0.003 |
| TUG | 14.9 ± 5.4 | 14.2 ± 4.4 | 19.8 ± 8.4 | 0.001 |
| Sedentary time | 519.1 ± 77.8 | 506.7 ± 73.5 | 608.5 ± 41.5 | <0.001 |
| LPA | 151.6 ± 54.6 | 153.6 ± 55.8 | 137.2 ± 43.9 | 0.353 |
| MVPA | 4.6 ± 10.2 | 5.1 ± 10.9 | 2.1 ± 2.0 | 0.369 |
| Self-efficacy | 919.9 ± 256.9 | 928.7 ± 251.3 | 858.6 ± 298.1 | 0.379 |
| ERA | 40.1 ± 14.9 | 40.8 ± 15.3 | 35.4 ± 10.8 | 0.146 |
| HRQoL | ||||
| Physical | 23.3 ± 0.3 | 23.3 ± 0.3 | 23.2 ± 0.3 | 0.170 |
| Mental | 12.6 ± 0.3 | 12.7 ± 0.4 | 12.4 ± 0.3 | 0.069 |
| Coefficient | SE | Wald | p-Value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Protein intake | −0.140 | 0.685 | 0.42 | 0.838 | 0.869 | 0.227–3.327 |
| Caloric intake | −0.980 | 0.825 | 1.411 | 0.235 | 0.375 | 0.074–1.891 |
| Sedentary time | 0.024 | 0.007 | 10.878 | 0.001 | 1.024 | 1.010–1.039 |
| LPA | −0.003 | 0.007 | 0.269 | 0.604 | 0.997 | 0.984–1.009 |
| MVPA | −0.089 | 0.111 | 0.651 | 0.420 | 0.915 | 0.736–1.136 |
| Self-efficacy | −0.002 | 0.001 | 2.012 | 0.156 | 0.998 | 0.995–1.001 |
| ERA | −0.030 | 0.024 | 1.560 | 0.212 | 0.970 | 0.925–1.017 |
| Coefficient | SE | Wald | p-Value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Protein intake | −2.115 | 1.513 | 1.954 | 0.162 | 0.121 | 0.006–2.341 |
| Caloric intake | −1.642 | 1.421 | 1.335 | 0.248 | 0.194 | 0.012–3.137 |
| Sedentary time | 0.040 | 0.015 | 7.409 | 0.006 | 1.041 | 1.011–1.071 |
| LPA | −0.021 | 0.013 | 2.697 | 0.101 | 0.980 | 0.956–1.004 |
| MVPA | −0.015 | 0.126 | 0.013 | 0.908 | 0.986 | 0.770–1.262 |
| Self-efficacy | −0.006 | 0.004 | 2.173 | 0.140 | 1.006 | 0.998–1.013 |
| ERA | −0.110 | 0.054 | 4.085 | 0.043 | 0.896 | 0.806–0.997 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taani, M.H.; Apchemengich, I.; Sima, C.D. Malnutrition–Sarcopenia Syndrome and Self-Management Behaviors in Continuing-Care Retirement Community Residents. Geriatrics 2022, 7, 9. https://doi.org/10.3390/geriatrics7010009
Taani MH, Apchemengich I, Sima CD. Malnutrition–Sarcopenia Syndrome and Self-Management Behaviors in Continuing-Care Retirement Community Residents. Geriatrics. 2022; 7(1):9. https://doi.org/10.3390/geriatrics7010009
Chicago/Turabian StyleTaani, Murad H., Immaculate Apchemengich, and Christina Diane Sima. 2022. "Malnutrition–Sarcopenia Syndrome and Self-Management Behaviors in Continuing-Care Retirement Community Residents" Geriatrics 7, no. 1: 9. https://doi.org/10.3390/geriatrics7010009
APA StyleTaani, M. H., Apchemengich, I., & Sima, C. D. (2022). Malnutrition–Sarcopenia Syndrome and Self-Management Behaviors in Continuing-Care Retirement Community Residents. Geriatrics, 7(1), 9. https://doi.org/10.3390/geriatrics7010009