
Systematic Review of Dementia Support Programs with Multicultural and Multilingual Populations

Abstract
:1. Introduction
2. Methods
2.1. Data Sources
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Abstraction
2.5. Quality Appraisal
3. Results
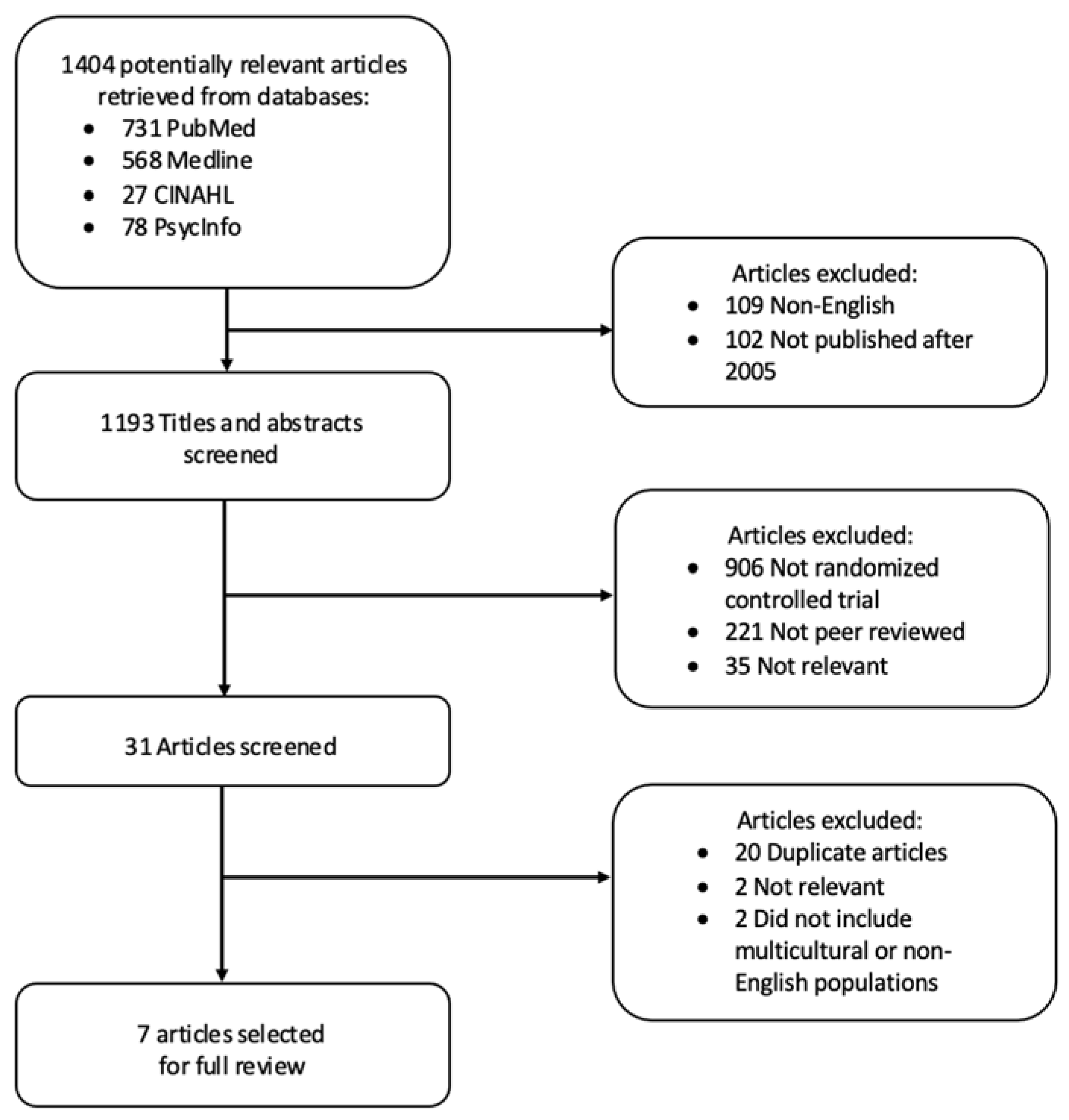
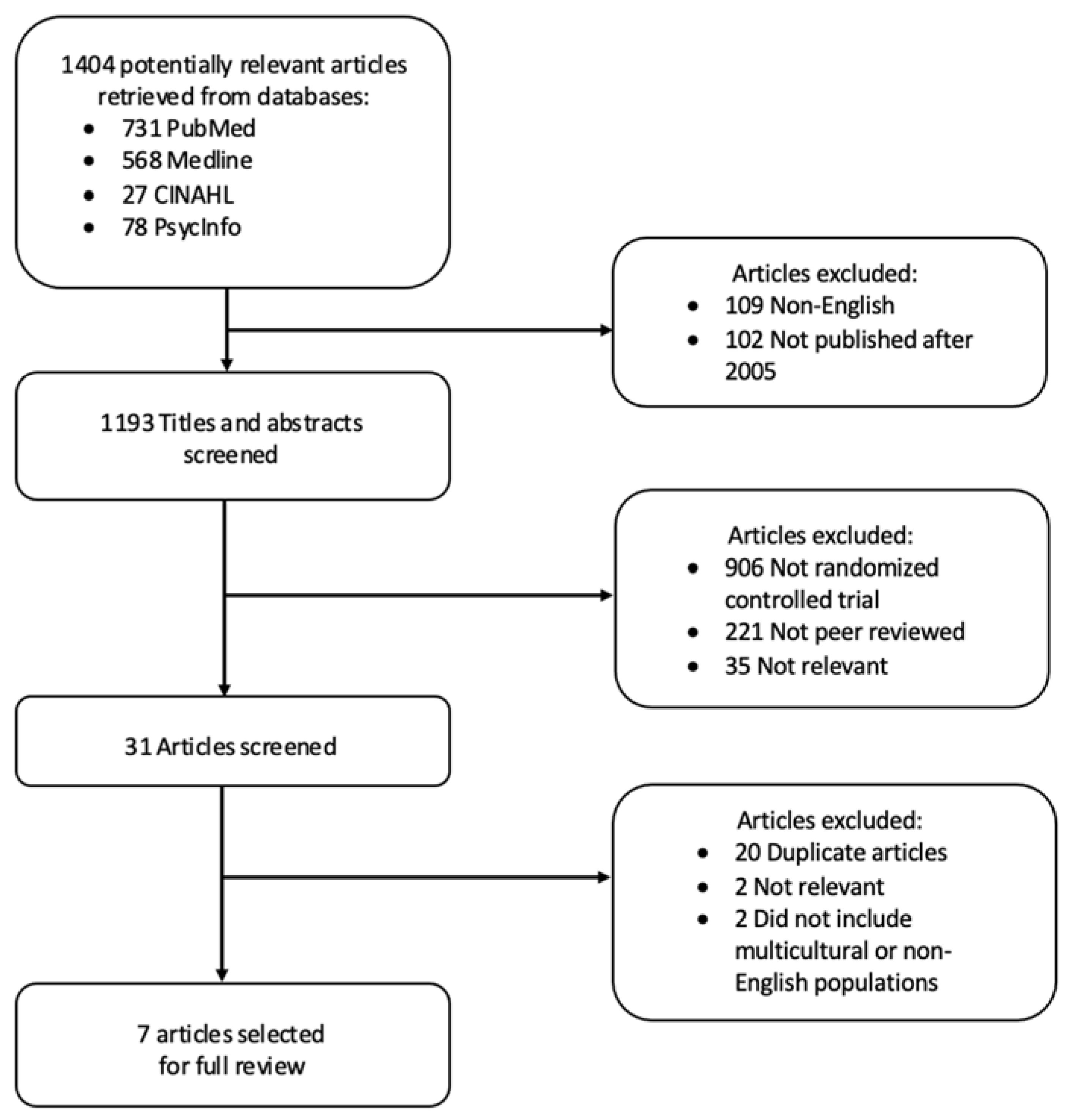
3.1. Article Selection
3.2. Type of Studies
3.2.1. Study Design
3.2.2. Setting
3.2.3. Study Population
3.2.4. Outcomes
4. Identification of Key Themes
4.1. Care Team Members
4.2. Health Care Utilization
4.3. Clinical Outcomes
4.4. Type of Educational Materials
4.5. Multicultural or Non-English Speaking Participants
4.6. Quality of Studies
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Prince, M.J.; Wimo, A.; Guerchet, M.M.; Ali, G.C.; Wu, Y.T.; Prina, M. The Global Impact of Dementia: An Analysis of Prevalence, Incidence, Cost and Trends; Alzheimer’s Disease International: London, UK, 2015; p. 1. [Google Scholar]
- Hunt, L.J.; Coombs, L.A.; Stephens, C.E. Emergency Department Use by Community-Dwelling Individuals with Dementia in the United States: An Integrative Review. J. Gerontol. Nurs. 2018, 44, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.W.; Cosentino, S.; Ornstein, K.; Gu, Y.; Andrews, H.; Stern, Y. Use and Cost of Hospitalization in Dementia: Longitudinal Results from a Community-Based Study: Use and Cost of Hospitalization in Dementia. Int. J. Geriatr. Psychiatry 2015, 30, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Etters, L.; Goodall, D.; Harrison, B.E. Caregiver Burden among Dementia Patient Caregivers: A Review of the Literature. J. Am. Acad. Nurse Pract. 2008, 20, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, R.; Regan, C.; Katona, C.; Livingston, G. Anxiety and Depression in Family Caregivers of People with Alzheimer Disease: The LASER-AD Study. Am. J. Geriatr. Psychiatry 2005, 13, 795–801. [Google Scholar] [CrossRef]
- Possin, K.L.; Merrilees, J.J.; Dulaney, S.; Bonasera, S.J.; Chiong, W.; Lee, K.; Hooper, S.M.; Allen, I.E.; Braley, T.; Bernstein, A.; et al. Effect of Collaborative Dementia Care via Telephone and Internet on Quality of Life, Caregiver Well-Being, and Health Care Use: The Care Ecosystem Randomized Clinical Trial. JAMA Intern. Med. 2019, 179, 1658. [Google Scholar] [CrossRef]
- Papastavrou, E.; Kalokerinou, A.; Papacostas, S.S.; Tsangari, H.; Sourtzi, P. Caring for a Relative with Dementia: Family Caregiver Burden. J. Adv. Nurs. 2007, 58, 446–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagán-Ortiz, M.E.; Cortés, D.E.; Rudloff, N.; Weitzman, P.; Levkoff, S. Use of an Online Community to Provide Support to Caregivers of People With Dementia. J. Gerontol. Soc. Work 2014, 57, 694–709. [Google Scholar] [CrossRef] [Green Version]
- Callahan, C.M. Alzheimer’s Disease: Individuals, Dyads, Communities, and Costs. J. Am. Geriatr. Soc. 2017, 65, 892–895. [Google Scholar] [CrossRef]
- Biegel, D.E.; Sales, E.; Schulz, R. Family Caregiving in Chronic Illness: Alzheimer’s Disease, Cancer, Heart Disease, Mental Illness, and Stroke; Sage Publications: Newbury Park, CA, USA, 1991. [Google Scholar]
- Llanque, S.M.; Enriquez, M. Interventions for Hispanic Caregivers of Patients with Dementia: A Review of the Literature. Am. J. Alzheimers Dis. Dement. 2012, 27, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Buckley, J.S.; Salpeter, S.R. A Risk-Benefit Assessment of Dementia Medications: Systematic Review of the Evidence. Drugs Aging 2015, 32, 453–467. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The Feasibility of Creating a Checklist for the Assessment of the Methodological Quality Both of Randomised and Non-Randomised Studies of Health Care Interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Silva, M.D.; Genoff, M.; Zaballa, A.; Jewell, S.; Stabler, S.; Gany, F.M.; Diamond, L.C. Interpreting at the End of Life: A Systematic Review of the Impact of Interpreters on the Delivery of Palliative Care Services to Cancer Patients with Limited English Proficiency. J. Pain Symptom Manag. 2016, 51, 569–580. [Google Scholar] [CrossRef] [Green Version]
- Callahan, C.M.; Boustani, M.A.; Unverzagt, F.W.; Austrom, M.G.; Damush, T.M.; Perkins, A.J.; Fultz, B.A.; Hui, S.L.; Counsell, S.R.; Hendrie, H.C. Effectiveness of Collaborative Care for Older Adults with Alzheimer Disease in Primary Care: A Randomized Controlled Trial. JAMA 2006, 295, 2148. [Google Scholar] [CrossRef] [PubMed]
- Bass, D.M.; Judge, K.S.; Maslow, K.; Wilson, N.L.; Morgan, R.O.; McCarthy, C.A.; Looman, W.J.; Snow, A.L.; Kunik, M.E. Impact of the Care Coordination Program “Partners in Dementia Care” on Veterans’ Hospital Admissions and Emergency Department Visits. Alzheimers Dement. Transl. Res. Clin. Interv. 2015, 1, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Xiao, L.D.; De Bellis, A.; Kyriazopoulos, H.; Draper, B.; Ullah, S. The Effect of a Personalized Dementia Care Intervention for Caregivers From Australian Minority Groups. Am. J. Alzheimers Dis. Dement. 2016, 31, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Amjad, H.; Wong, S.K.; Roth, D.L.; Huang, J.; Willink, A.; Black, B.S.; Johnston, D.; Rabins, P.V.; Gitlin, L.N.; Lyketsos, C.G.; et al. Health Services Utilization in Older Adults with Dementia Receiving Care Coordination: The MIND at Home Trial. Health Serv. Res. 2018, 53, 556–579. [Google Scholar] [CrossRef]
- Czaja, S.J.; Loewenstein, D.; Schulz, R.; Nair, S.N.; Perdomo, D. A Videophone Psychosocial Intervention for Dementia Caregivers. Am. J. Geriatr. Psychiatry 2013, 21, 1071–1081. [Google Scholar] [CrossRef] [PubMed]
- Sink, K.M.; Holden, K.F.; Yaffe, K. Pharmacological Treatment of Neuropsychiatric Symptoms of Dementia: A Review of the Evidence. JAMA 2005, 293, 596. [Google Scholar] [CrossRef]
- Chodosh, J.; Colaiaco, B.A.; Connor, K.I.; Cope, D.W.; Liu, H.; Ganz, D.A.; Richman, M.J.; Cherry, D.L.; Blank, J.M.; Carbone, R.d.P.; et al. Dementia Care Management in an Underserved Community: The Comparative Effectiveness of Two Different Approaches. J. Aging Health 2015, 27, 864–893. [Google Scholar] [CrossRef] [PubMed]
- Bynum, J.P.W.; Rabins, P.V.; Weller, W.; Niefeld, M.; Anderson, G.F.; Wu, A.W. The Relationship Between a Dementia Diagnosis, Chronic Illness, Medicare Expenditures, and Hospital Use. J. Am. Geriatr. Soc. 2004, 52, 187–194. [Google Scholar] [CrossRef]
- Krishnan, L.L.; Petersen, N.J.; Snow, A.L.; Cully, J.A.; Schulz, P.E.; Graham, D.P.; Morgan, R.O.; Braun, U.; Moffett, M.L.; Yu, H.-J.; et al. Prevalence of Dementia among Veterans Affairs Medical Care System Users. Dement. Geriatr. Cogn. Disord. 2005, 20, 245–253. [Google Scholar] [CrossRef]
- Maslow, K.; Mezey, M. Recognition of Dementia in Hospitalized Older Adults. AJN Am. J. Nurs. 2008, 108, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Clevenger, C.K.; Chu, T.A.; Yang, Z.; Hepburn, K.W. Clinical Care of Persons with Dementia in the Emergency Department: A Review of the Literature and Agenda for Research. J. Am. Geriatr. Soc. 2012, 60, 1742–1748. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.; Rhodes, R.L.; Mitchell, S.L.; Mor, V.; Teno, J.M. Natural History of Feeding-Tube Use in Nursing Home Residents with Advanced Dementia. J. Am. Med. Dir. Assoc. 2009, 10, 264–270. [Google Scholar] [CrossRef] [Green Version]
- Sands, L.P.; Yaffe, K.; Covinsky, K.; Chren, M.-M.; Counsell, S.; Palmer, R.; Fortinsky, R.; Landefeld, C.S. Cognitive Screening Predicts Magnitude of Functional Recovery From Admission to 3 Months After Discharge in Hospitalized Elders. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, M37–M45. [Google Scholar] [CrossRef] [Green Version]
- Bejjani, C.; Rumph, G.; Kunik, M. Addressing Psychiatric Problems of Dementia in the Emergency Room. Internet J. Emerg. Med. 2017, 7, 1–2. [Google Scholar]
- Williams, K.N.; Perkhounkova, Y.; Shaw, C.A.; Hein, M.; Vidoni, E.D.; Coleman, C.K. Supporting Family Caregivers with Technology for Dementia Home Care: A Randomized Controlled Trial. Innov. Aging 2019, 3, igz037. [Google Scholar] [CrossRef] [Green Version]
- Talley, R.C.; Crews, J.E. Framing the Public Health of Caregiving. Am. J. Public Health 2007, 97, 224–228. [Google Scholar] [CrossRef]
- Hopwood, J.; Walker, N.; McDonagh, L.; Rait, G.; Walters, K.; Iliffe, S.; Ross, J.; Davies, N. Internet-Based Interventions Aimed at Supporting Family Caregivers of People With Dementia: Systematic Review. J. Med. Internet Res. 2018, 20, e216. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Article | Population | Clinical Setting | Sample Size | Intervention and Comparison Group | Measured Outcomes | Major Findings | Black and Downs Score |
|---|---|---|---|---|---|---|---|
| Bass et al., 2015 | Community-dwelling, veterans ≥ 60 yo with dementia and their caregivers located in 5 major US cities (Boston, MA, Houston, TX, Providence, RI, Oklahoma City, OK, Beaumont, TX) * multicultural populations included | Virtual (e.g., telephone, mail and email) | n = 508 (total) n = 299 (intervention) n = 187 (control) * 19% identified as member of multicultural group, however n not specified | Bachelor or Masters level SW or RN Veterans Affairs (VA) coordinator and Alzheimer’s Association (AA) coordinator collaborated to provide guidance for veterans and caregivers using standardized protocols via at least monthly phone calls. VA coordinator addressed medical-related concerns. AA coordinator addressed caregiver’s nonmedical concerns. Comparison group: no assistance from care-coordination program. Received educational materials. | Number of veterans’ hospital admissions and emergency department (ED) visits in persons with dementia over 12 months. | Veterans with dementia who received assistance from care coordinators had fewer hospital admissions and ED visits than comparison-group veterans. There were no differences in the likelihood of hospital admission or ED use. | 16 |
| Xiao et al., 2016 | Caregivers ≥ 18 yo from minority groups who cared for a community-dwelling person with dementia (PWD) from the same multicultural group located in Metropolitan Adelaide, South Australia. * Non-English speaking participants included | Home visits and virtual (e.g., telephone) | n = 61 (total) n = 31 (intervention) n = 30 (control) * n = 53 (non-English speaking) | Care-coordinator with varied backgrounds (RN, SW, Community Home Care Certificate holders) who have cultural and linguistic concordance with caregivers provided support by screening for caregiver needs through home visits and phone calls, referring caregivers to services, and education programs. Caregivers also kept diary of unmet needs. Comparison group: no assistance from care coordinator. | Questionnaires addressing caregiver’s competence, quality of life (physical vs. mental), dependence level of care recipients, and satisfaction with care support. | The intervention group showed a significant increase in the caregivers’ sense of competence and mental components of quality of life. There were no significant differences in the caregivers’ physical components of quality of life. | 20 |
| Amjad et al., 2018 | Community-dwelling adults ≥ 70 yo with cognitive impairment residing in North West Baltimore * multicultural populations included | In-home visits (at baseline and 18 months) and at least one monthly contact (e.g., telephone or in-person) | n = 303 (total) n = 110 (intervention) n = 193 (control) * n = 87 (Black/African American or other race) | 18-month care coordination intervention provided by community-based, nonclinical care coordinators that were supported by interdisciplinary clinical team. Care coordination with nonclinical memory care coordinator + RN + geriatrician + psychiatrist (no PMD involvement) who provide education, skill building, linkage to services, informal counseling and care monitoring for 18 months. Comparison group: no assistance from care-coordinator. | In-person, self reported interviews administered at baseline, 9 months, and 18 months to assess utilization of acute care/inpatient, outpatient, and home-and community-based services. | No significant group differences in acute care/inpatient or total outpatient services use. Intervention group had significantly increased outpatient dementia/mental health visits from 9 to 18 months compared to controls. Intervention group had more home and community-based support service use from baseline to 18 months. | 20 |
| Possin et al., 2019 | Community-dwelling persons with dementia-caregiver dyads ≥ 45 yo located in 3 US states (California, Iowa, and Nebraska). * Non-English speaking, multicultural, and rural participants included | Virtual (e.g., telephone and internet-based supportive care) | n = 780 (total PWD and caregiver dyads) n = 512 (intervention) n = 268 (control) PWD: * n = 31 (Spanish) * n = 16 (Cantonese) * n = 82 (Hispanic or Latino) * n = 31 (African American) Caregivers: * n = 43 (Spanish) * n = 16 (Cantonese) * n = 83 (Hispanic or Latino) * n = 32 (African American) * n not included for rural populations | Unlicensed care team navigator with 40 h of training provided telephone-based screening, support, education, and care coordination. Nurse, social worker and pharmacist provided support to care team navigator. Comparison group: no assistance from team navigator. They were offered contact info for Family Caregiver Alliance, Alzheimer’s association and area agencies on aging. | Primary outcome measure: Quality of Life in Alzheimer’s Disease based on caregiver survey of person with dementia. Secondary outcomes: frequencies of PWDs’ use of emergency department, hospitalization, ambulance services, caregiver depression, and caregiver burden. | Compared with usual care, intervention group showed improved quality of life for persons with dementia, reduced emergency department visits, and reduced caregiver depression and caregiver burden. | 21 |
| Pagán-Ortiz et al., 2014 | Community-based Hispanic caregivers of PWD located in Puerto Rico, Mexico, or Massachusetts. * Non-English and multicultural populations included | Virtual (e.g., web-based) | n = 72 (total) n = 15 (intervention group that completed both pre-and post-test) n = 17 (control group that completed both pre-and post-test) * n = 72 (Spanish) * n = 72 (Hispanic) | Intervention group participated in 4 group sessions devoted to teaching them about features of a website that provides online education and support for Hispanic families, and professional caregivers of people with dementia. Comparison group: participated in 2 group sessions where they received printed Spanish educational materials on Alzheimer’s caregiving. | Caregivers were surveyed using pre- and post-test and assessed for sense of self-mastery, social support, burden, and depression symptomatology. | No outcomes were statistically significant | 10 |
| Callahan et al., 2006 | Community-dwelling adults from two primary care practices in Indianapolis that met diagnostic criteria for Alzheimer’s disease and their caregiver. * multicultural population included | Primary care clinic, virtual (e.g., telephone-based) | n = 153 (total) n = 84 (intervention) n = 69 (control) * n = 75 (Black/African American) | Intervention group received 1 year of care management by an interdisciplinary team led by an advanced NP integrated within primary care setting who provided education on communication skills, caregiver coping skills, legal and financial advice, and implementation of behavior protocols when behaviors became an issue. Comparison group: augmented usual care without assistance from interdisciplinary team. | Neuropsychiatric Inventory (NPI) measured at baseline and at 6, 12, and 18 months. Secondary outcomes included the Cornell Scale for Depression in Dementia (CSDD), cognition, activities of daily living, resource use, and caregiver’s depression severity, and healthcare use. | Collaborative care group showed significant improvement in behavioral NPI scores and caregiver stress. There was no impact on depression scales, cognitive of functional status. Augmented usual care showed fewer cumulative physician and nurse visits. Rates of nursing home placement did not differ between groups. | 23 |
| Czaja et al., 2013 | African American caregivers ≥ 21 yo of community-dwelling PWD located in Miami, FL * Non-English (Spanish) and multicultural populations included | Virtual (e.g., videophone-based) | n = 110 (total) n = 38 (intervention) n = 36 (attention control) n = 36 (control) * n = 56 (Hispanic) * n = 54 (Black/African American) * n not reported for Spanish speaking participants | Caregivers were randomized to three groups: 1. Intervention: certified interventionists taught problem solving strategies to deal with behaviors, stress management, healthy behaviors, and communication conducted through in-home visits. 2. Attention control: In-home and videophone visits focusing on nutrition 3. Information only control: Education material about dementia, caregiving, safety, and resources were mailed to participants followed by brief phone call. | Measurements of depression, caregiver burden, social support, and the caregivers’ perception of the caregiver’s experience were administered at baseline and 5 months post- randomization. | Caregivers in the intervention group compared to controls experienced decrease caregiver burden, increased appreciation of positive aspects of caregiving, and greater satisfaction with social support. | 16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demanes, A.; Ward, K.T.; Wang, A.T.; Hess, M. Systematic Review of Dementia Support Programs with Multicultural and Multilingual Populations. Geriatrics 2022, 7, 8. https://doi.org/10.3390/geriatrics7010008
Demanes A, Ward KT, Wang AT, Hess M. Systematic Review of Dementia Support Programs with Multicultural and Multilingual Populations. Geriatrics. 2022; 7(1):8. https://doi.org/10.3390/geriatrics7010008
Chicago/Turabian StyleDemanes, Abriella, Katherine T. Ward, Amy Tu Wang, and Mailee Hess. 2022. "Systematic Review of Dementia Support Programs with Multicultural and Multilingual Populations" Geriatrics 7, no. 1: 8. https://doi.org/10.3390/geriatrics7010008
APA StyleDemanes, A., Ward, K. T., Wang, A. T., & Hess, M. (2022). Systematic Review of Dementia Support Programs with Multicultural and Multilingual Populations. Geriatrics, 7(1), 8. https://doi.org/10.3390/geriatrics7010008