
Non-Vitamin K Oral Anticoagulants Assessment in High Risk of Bleeding Patients with Non-Valvular Atrial Fibrillation

Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
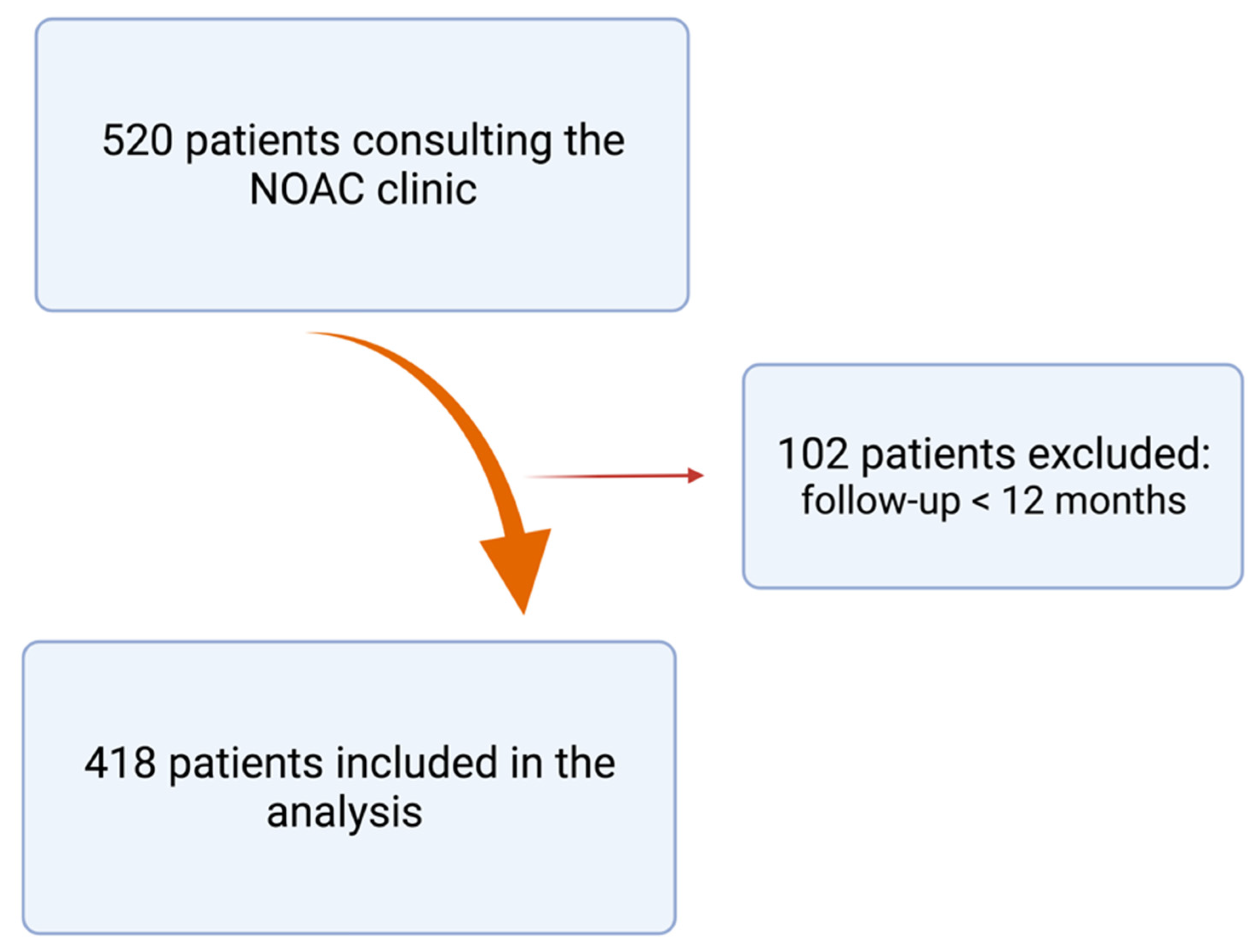
3.1. Study Population
3.2. Follow-Up
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, H.V.; Fischer, G.W. Atrial fibrillation: Pathophysiology and therapeutic options. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Zimetbaum, P. Atrial fibrillation. Ann. Intern. Med. 2017, 166, 920. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Lane, D.A. Stroke prevention in atrial fibrillation: A systematic review. JAMA 2015, 313, 1950–1962. [Google Scholar] [CrossRef] [PubMed]
- Killu, A.M.; Granger, C.B.; Gersh, B.J. Risk stratification for stroke in atrial fibrillation: A critique. Eur. Heart J. 2019, 40, 1294–1302. [Google Scholar] [CrossRef]
- Man-Son-Hing, M.; Laupacis, A. Anticoagulant-related bleeding in older persons with atrial fibrillation: Physicians’ fears often unfounded. Arch. Intern. Med. 2003, 163, 1580–1586. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Lip, G.Y.; Apostolakis, S. Bleeding risk assessment and management in atrial fibrillation patients. Key messages for clinical practice from the European Heart Rhythm Association position statement. Pol. Arch. Med. Wewn. 2012, 122, 235–242. [Google Scholar] [CrossRef] [Green Version]
- Shoeb, M.; Fang, M.C. Assessing bleeding risk in patients taking anticoagulants. J. Thromb. Thrombolysis 2013, 35, 312–319. [Google Scholar] [CrossRef] [Green Version]
- Induruwa, I.; Evans, N.R.; Aziz, A.; Reddy, S.; Khadjooi, K.; Romero-Ortuno, R. Clinical frailty is independently associated with non-prescription of anticoagulants in older patients with atrial fibrillation. Geriatr. Gerontol. Int. 2017, 17, 2178–2183. [Google Scholar] [CrossRef]
- Guo, Q.; Du, X.; Ma, C.S. Atrial fibrillation and frailty. J. Geriatr. Cardiol. 2020, 17, 105–109. [Google Scholar] [CrossRef]
- Go, A.S.; Hylek, E.M.; Borowsky, L.H.; Phillips, K.A.; Selby, J.V.; Singer, D.E. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: The anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Ann. Intern. Med. 1999, 131, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Pawar, A.; Gagne, J.J.; Bessette, L.G.; Lee, H.; Glynn, R.J.; Schneeweiss, S. Frailty and clinical outcomes of direct oral anticoagulants versus warfarin in older adults with atrial fibrillation: A cohort study. Ann. Intern. Med. 2021, 174, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Perera, V.; Bajorek, B.V.; Matthews, S.; Hilmer, S.N. The impact of frailty on the utilisation of antithrombotic therapy in older patients with atrial fibrillation. Age Ageing 2009, 38, 156–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prins, M.H.; Lensing, A.W.; Bauersachs, R.; van Bellen, B.; Bounameaux, H.; Brighton, T.A.; Cohen, A.T.; Davidson, B.L.; Decousus, H.; Raskob, G.E. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: A pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb. J. 2013, 11, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, S.S.; McDuffie, J.R.; Ortel, T.L.; Williams, J.W., Jr. Comparative effectiveness of warfarin and new oral anticoagulants for the management of atrial fibrillation and venous thromboembolism: A systematic review. Ann. Intern. Med. 2012, 157, 796–807. [Google Scholar] [CrossRef] [PubMed]
- Zappulla, P.; Calvi, V. Gastrointestinal bleeding and direct oral anticoagulants among patients with atrial fibrillation: Risk, prevention, management, and quality of life. TH Open 2021, 5, e200–e210. [Google Scholar] [CrossRef]
- Sinnaeve, P.R.; Brueckmann, M.; Clemens, A.; Oldgren, J.; Eikelboom, J.; Healey, J.S. Stroke prevention in elderly patients with atrial fibrillation: Challenges for anticoagulation. J. Intern. Med. 2012, 271, 15–24. [Google Scholar] [CrossRef]
- Steffel, J.; Verhamme, P.; Potpara, T.S.; Albaladejo, P.; Antz, M.; Desteghe, L.; Haeusler, K.G.; Oldgren, J.; Reinecke, H.; Roldan-Schilling, V. The 2018 European Heart Rhythm Association Practical Guide on the use of non-Vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur. Heart J. 2018, 39, 1330–1393. [Google Scholar] [CrossRef] [Green Version]
- Jame, S.; Barnes, G. Stroke and thromboembolism prevention in atrial fibrillation. Heart 2020, 106, 10–17. [Google Scholar] [CrossRef]
- Sharma, M.; Cornelius, V.R.; Patel, J.P.; Davies, J.G.; Molokhia, M. Efficacy and harms of direct oral anticoagulants in the elderly for stroke prevention in atrial fibrillation and secondary prevention of venous thromboembolism: Systematic review and meta-analysis. Circulation 2015, 132, 194–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.; Guo, S.D.; Deng, H.; Shantsila, A.; Fauchier, L.; Ma, C.S.; Lip, G.Y. Effectiveness and safety of oral anticoagulants in older patients with atrial fibrillation: A systematic review and meta-regression analysis. Age Ageing 2018, 47, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulman, S.; Kearon, C.; Subcommittee on control of anticoagulation of the scientific and standardization committee of the international society on thrombosis and haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S.; Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.G.M.; Lip, G.Y.H. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef] [Green Version]
- Basaran, O.; Filiz Basaran, N.; Cekic, E.G.; Altun, I.; Dogan, V.; Mert, G.O.; Mert, K.U.; Akin, F.; Soylu, M.O.; Memic Sancar, K. Prescription patterns of oral anticoagulants in nonvalvular atrial fibrillation (PROPER study). Clin. Appl. Thromb. 2017, 23, 384–391. [Google Scholar] [CrossRef] [Green Version]
- Heidbuchel, H.; Berti, D.; Campos, M.; Desteghe, L.; Freixo, A.P.; Nunes, A.R.; Roldán, V.; Toschi, V.; Lassila, R. Implementation of non-vitamin K antagonist oral anticoagulants in daily practice: The need for comprehensive education for professionals and patients. Thromb. J. 2015, 13, 22. [Google Scholar] [CrossRef]
- Henrard, S.; Vandenabeele, C.; Marien, S.; Boland, B.; Dalleur, O. Underuse of anticoagulation in older patients with atrial fibrillation and CHADS2 score ≥ 2, are we doing better since the marketing of direct oral anticoagulants? Drugs Aging 2017, 34, 841–850. [Google Scholar] [CrossRef]
- Patti, G.; Lucerna, M.; Pecen, L.; Siller-Matula, J.M.; Cavallari, I.; Kirchhof, P.; de Caterina, R. Thromboembolic risk, bleeding outcomes and effect of different antithrombotic strategies in very elderly patients with atrial fibrillation: A sub-analysis from the PREFER in AF (prevention of thromboembolic events-European registry in atrial fibrillation). J. Am. Heart Assoc. 2017, 23, 6. [Google Scholar]
- Kooiman, J.; van de Peppel, W.R.; van der Meer, F.J.; Huisman, M.V. Incidence of chronic kidney disease in patients with atrial fibrillation and its relevance for prescribing new oral antithrombotic drugs. J. Thromb. Haemost. 2011, 9, 1652–1653. [Google Scholar] [CrossRef]
- Jönsson, K.M.; Wieloch, M.; Sterner, G.; Nyman, U.; Elmståhl, S.; Engström, G.; Svensson, P.J. Glomerular filtration rate in patients with atrial fibrillation on warfarin treatment: A subgroup analysis from the AURICULA registry in Sweden. Thromb. Res. 2011, 128, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Roldán, V.; Marín, F.; Fernández, H.; Manzano-Fernández, S.; Gallego, P.; Valdés, M.; Vicente, V.; Lip, G.Y. Renal impairment in a “real-life” cohort of anticoagulated patients with atrial fibrillation (implications for thromboembolism and bleeding). Am. J. Cardiol. 2013, 111, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.F.; Liu, C.J.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Hu, Y.F.; Tuan, T.C.; Liao, J.N.; Chung, F.P.; Chen, T.J. Oral anticoagulation in very elderly patients with atrial fibrillation: A nationwide cohort study. Circulation 2018, 138, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Martinez, B.K.; Sood, N.A.; Bunz, T.J.; Coleman, C.I. Effectiveness and safety of apixaban, dabigatran, and rivaroxaban versus warfarin in frail patients with nonvalvular atrial fibrillation. J. Am. Heart Assoc. 2018, 7, e008643. [Google Scholar] [CrossRef] [PubMed]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Connolly, S.; Ezekowitz, M.; Salim Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, M.; Mahaffey, K.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.; Alexander, J.; McMurray, J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [Green Version]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [Green Version]
- Maura, G.; Billionnet, C.; Drouin, J.; Weill, A.; Neumann, A.; Pariente, A. Oral anticoagulation therapy use in patients with atrial fibrillation after the introduction of non-vitamin K antagonist oral anticoagulants: Findings from the French healthcare databases, 2011–2016. BMJ Open 2019, 9, e026645. [Google Scholar] [CrossRef]
- Rohla, M.; Weiss, T.W.; Pecen, L.; Patti, G.; Siller-Matula, J.M.; Schnabel, R.B.; Schilling, R.; Kotecha, D.; Lucerna, M.; Huber, K. Risk factors for thromboembolic and bleeding events in anticoagulated patients with atrial fibrillation: The prospective, multicentre observational PREvention of thromboembolic events—European Registry in Atrial Fibrillation (PREFER in AF). BMJ Open 2019, 9, e022478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Veer, A.J.W.M.; Bennaghmouch, N.; Wijffels, M.C.E.F.; Ten Berg, J.M. Management and outcomes of real-world use of non-vitamin-K oral anticoagulants (NOACs) in patients with atrial fibrillation: Experience of a dedicated NOAC clinic. Neth. Heart J. 2019, 27, 605–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caro Martínez, C.; Andreu Cayuelas, J.M.; Flores Blanco, P.J.; Valdés, M.; Bailén Lorenzo, J.L.; Manzano Fernández, S. Comparison of bleeding risk scores in patients with nonvalvular atrial fibrillation starting direct oral anticoagulants. Rev. Esp. Cardiol. 2017, 70, 878–880. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Rutherford, O.W.; Jonasson, C.; Ghanima, W.; Söderdahl, F.; Halvorsen, S. Effectiveness and safety of oral anticoagulants in elderly patients with atrial fibrillation. Heart 2022, 108, 345–352. [Google Scholar] [CrossRef]
- Lee, K.N.; Choi, J.I.; Boo, K.Y.; Kim, D.Y.; Kim, Y.G.; Oh, S.K.; Baek, Y.S.; Lee, D.I.; Roh, S.Y.; Shim, J. Effectiveness and safety of off-label dosing of non–vitamin K antagonist anticoagulant for atrial fibrillation in Asian patients. Sci. Rep. 2020, 10, 1801. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total Number of Patients | 418 | |
| Age, y (mean ± SD) | 77.88 ± 10.3 | |
| Age groups, n (%) | <65 years | 38 (9) |
| 65–74 years | 89 (21.2) | |
| ≥75 years | 289 (69.1) | |
| Weight, Kg (mean ± SD) | 73 ± 13.7 | |
| Male, n (%) | 228 (54.5) | |
| Comorbidities | ||
| Hypertension | 250 (55) | |
| Diabetes mellitus | 74 (17.7) | |
| Heart failure | 39 (9.3) | |
| Prior stroke/TIA | 65 (15.5) | |
| Myocardial Infarction | 8 (1.9) | |
| COPD | 60 (14.3) | |
| Congenital heart disease | 2 (4.1) | |
| Previous pulmonary embolism | 17 (4) | |
| Use of NSAIDs, n (%) | 16 (3.8) | |
| Alcohol excess/abuse, n (%) | 3 (0.7) | |
| GFR (mL/min/1.73 m2), mean ± SD | 59.7 ± 20.1 | |
| CHA2DS2-VASc score, mean ± SD | 3.85 ± 1.4 | |
| CHA2DS2-VASc score, n (%) | ≤1 | 18 (4.3) |
| 2 | 40 (9.5) | |
| ≥3 | 359 (86) | |
| HAS-BLED score, mean ± SD | 1.85 ± 1.0 |
| Type of NOAC | Dosage (mg) | n (%) |
|---|---|---|
| Apixaban (twice daily) | 2.5 | 95 (22.6%) |
| 5 | 87 (20.8%) | |
| Edoxaban (once daily) | 15 | 1 (0.2%) |
| 30 | 57 (13.6%) | |
| 60 | 79 (18.8%) | |
| Dabigatran (twice daily) | 75 | 3 (0.7%) |
| 110 | 9 (2.1%) | |
| 150 | 4 (0.9%) | |
| Rivaroxaban (once daily) | 10 | 5 (1.1%) |
| 15 | 26 (6.2%) | |
| 20 | 51(12.2%) |
| Variable | Events no. (%) | Event Rate no./100 Patient-yrs. |
|---|---|---|
| Total Bleeding events (Major and Clinically Relevant Non-Major bleeding) * | 50 (11.9) | 7 |
| Major Bleeding | ||
| Total (any) | 16 (3.8) | 2.2 |
| Transfusion | 4 (0.95) | 0.56 |
| Decrease in hemoglobin > 2 g/dL | 2 (0.47) | 0.2 |
| Critical Bleeding | 10 (2.4) | 1.4 |
| Fatal Bleeding | 0 (0) | 0 (0) |
| Clinically Relevant Non-Major Bleeding | 34 (8.1) | 4.8 |
| Stroke/TIA, n (%) | 12 (2.6) | 1.6 |
| Venous Thromboembolic complications | 2 (0.47) | 0.28 |
| Systemic arterial embolism | 0 (0) | 0 (0) |
| Hospital Admissions | 59 (14.1) | 8.3 |
| All-cause Mortality, n (%) | 36 (8.6) | 5 |
| Reason for Discontinuation | n (%) |
|---|---|
| Biopsy | 5 (1.1) |
| Surgery | 50 (11.96) |
| Endoscopy | 20 (4.7) |
| Trauma | 5 (1.1) |
| Dental Extraction | 7 (1.6) |
| Total | 87 (20.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva Cunha, P.; Viveiros Monteiro, A.; Coutinho Cruz, M.; Malveiro, P.; Reis, J.P.; Portugal, G.; Dias, A.; Ferreira, R.C.; Oliveira, M.M. Non-Vitamin K Oral Anticoagulants Assessment in High Risk of Bleeding Patients with Non-Valvular Atrial Fibrillation. Geriatrics 2022, 7, 20. https://doi.org/10.3390/geriatrics7010020
Silva Cunha P, Viveiros Monteiro A, Coutinho Cruz M, Malveiro P, Reis JP, Portugal G, Dias A, Ferreira RC, Oliveira MM. Non-Vitamin K Oral Anticoagulants Assessment in High Risk of Bleeding Patients with Non-Valvular Atrial Fibrillation. Geriatrics. 2022; 7(1):20. https://doi.org/10.3390/geriatrics7010020
Chicago/Turabian StyleSilva Cunha, Pedro, André Viveiros Monteiro, Madalena Coutinho Cruz, Paula Malveiro, João Pedro Reis, Guilherme Portugal, Ana Dias, Rui Cruz Ferreira, and Mário Martins Oliveira. 2022. "Non-Vitamin K Oral Anticoagulants Assessment in High Risk of Bleeding Patients with Non-Valvular Atrial Fibrillation" Geriatrics 7, no. 1: 20. https://doi.org/10.3390/geriatrics7010020
APA StyleSilva Cunha, P., Viveiros Monteiro, A., Coutinho Cruz, M., Malveiro, P., Reis, J. P., Portugal, G., Dias, A., Ferreira, R. C., & Oliveira, M. M. (2022). Non-Vitamin K Oral Anticoagulants Assessment in High Risk of Bleeding Patients with Non-Valvular Atrial Fibrillation. Geriatrics, 7(1), 20. https://doi.org/10.3390/geriatrics7010020