
Use of Contrast-Enhanced Ultrasonography and Shear-Wave Elastography in the Diagnosis of Granulomatous Colitis in a French Bulldog

 and
and 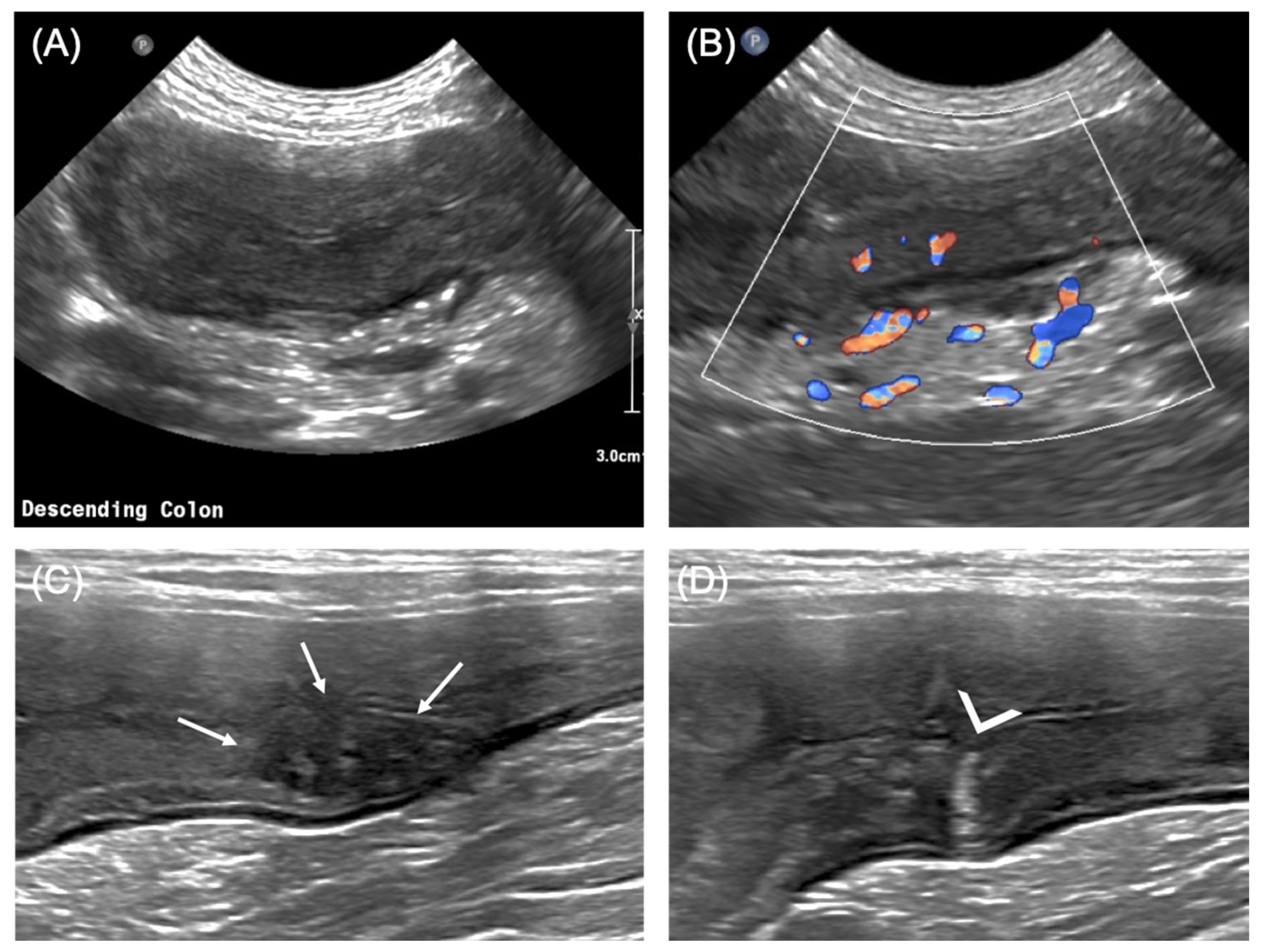{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials, Methods, and Results
2.1. Case Description and Clinical Investigations
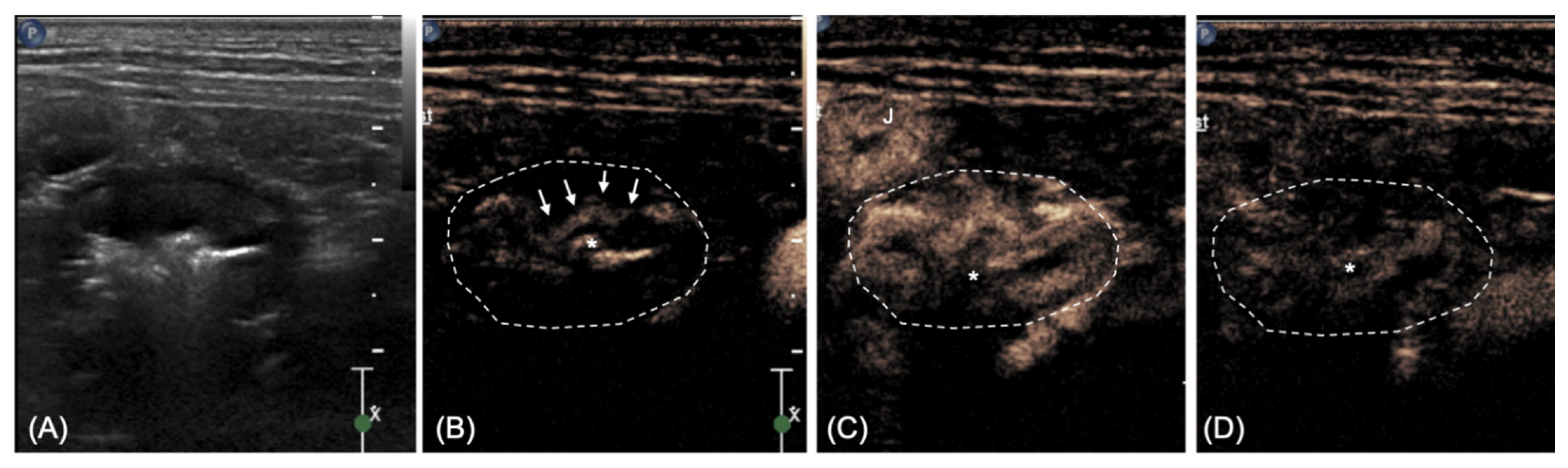
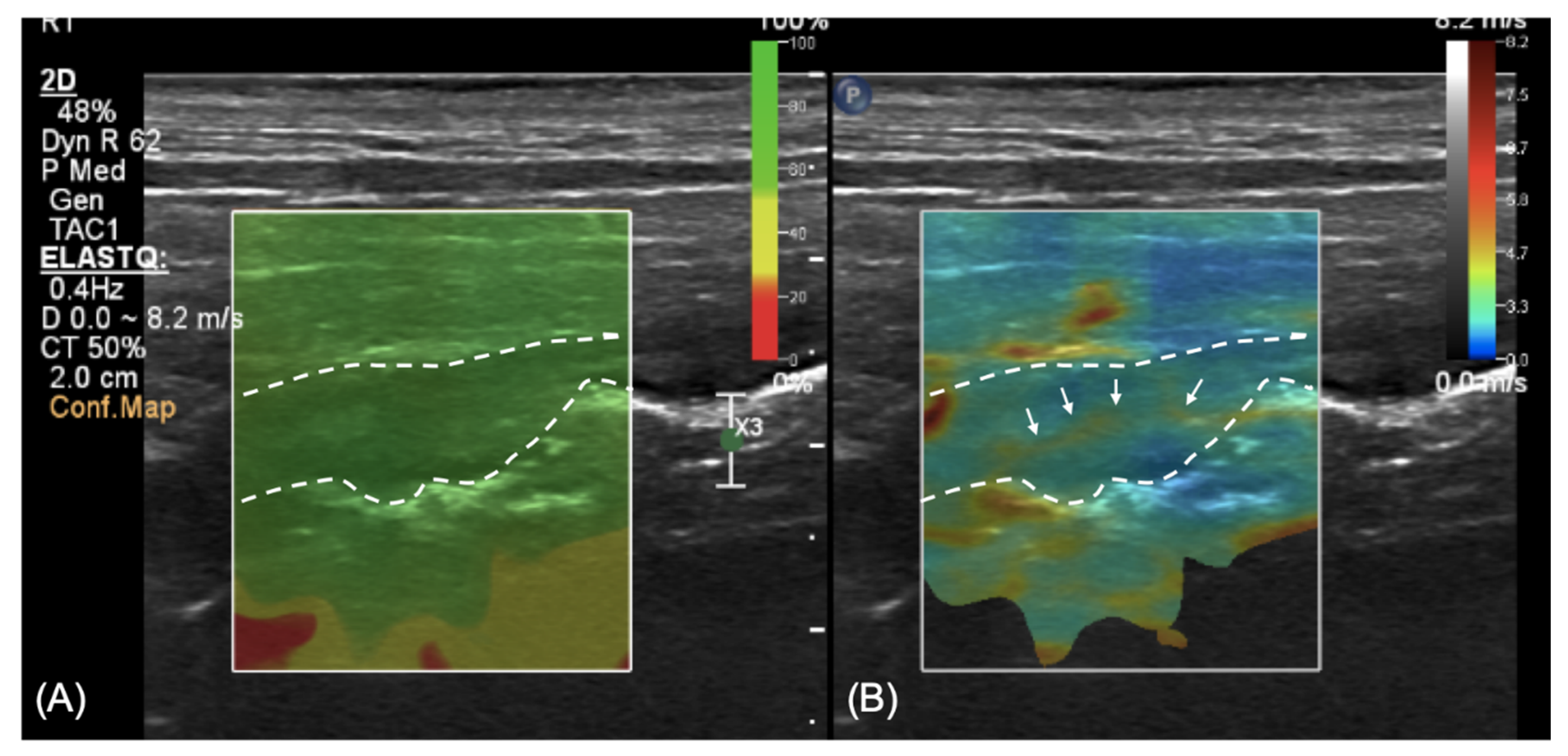
2.2. Imaging Diagnosis
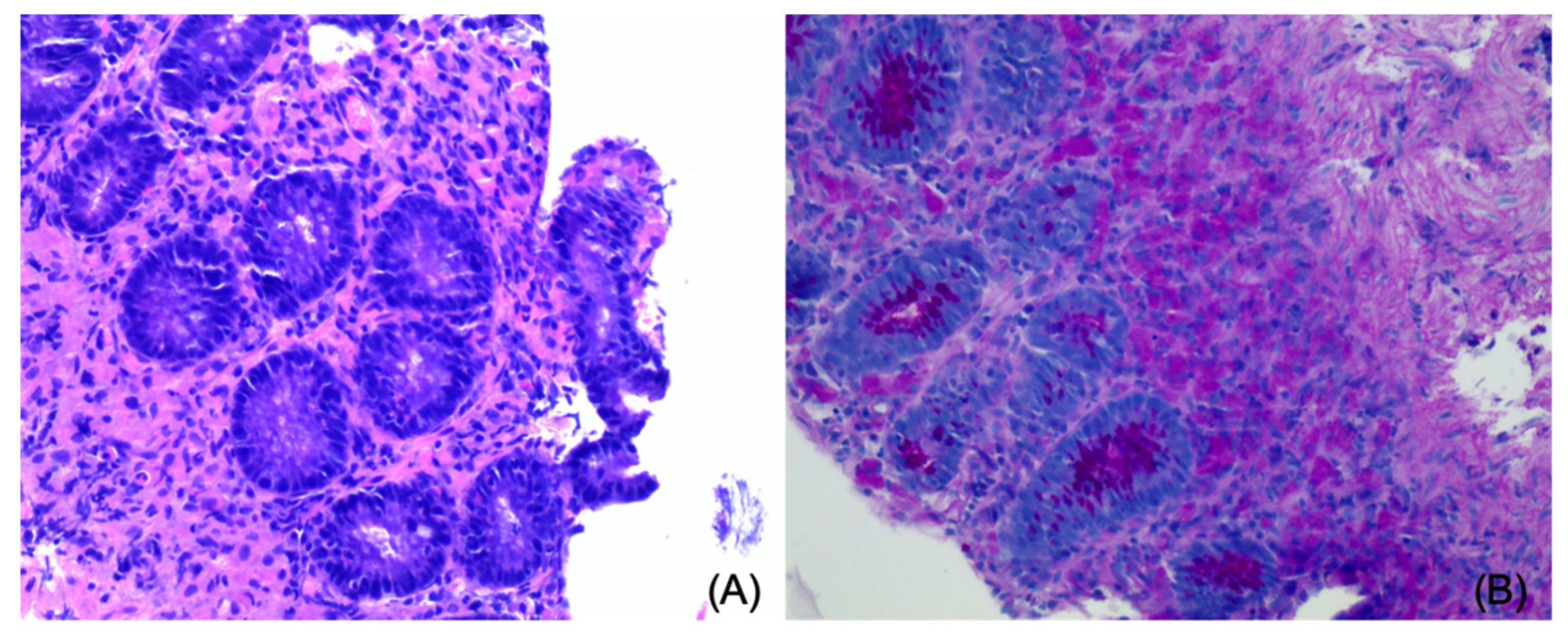
2.3. Endoscopy, Histopathology, Treatment, and Outcome
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Craven, M.; Mansfield, C.S.; Simpson, K.W. Granulomatous Colitis of Boxer Dogs. Vet. Clin. N. Am. Small Anim. Pr. 2011, 41, 433–445. [Google Scholar] [CrossRef] [PubMed]
- Manchester, A.; Hill, S.; Sabatino, B.; Armentano, R.; Carroll, M.; Kessler, B.; Miller, M.; Dogan, B.; McDonough, S.; Simpson, K. Association between granulomatous colitis in French bulldogs and invasive Escherichia coli and response to fluoroquinolone antimicrobials. J. Vet. Intern. Med. 2013, 27, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Hostutler, R.A.; Luria, B.J.; Johnson, S.E.; Weisbrode, S.E.; Sherding, R.G.; Jaeger, J.Q.; Guilford, W.G. Antibiotic-responsive histiocytic ulcerative colitis in 9 dogs. J. Vet. Intern. Med. 2004, 18, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Craven, M.; Dogan, B.; Schukken, A.; Volkman, M.; Chandler, A.; McDonough, P.; Simpson, K. Antimicrobial resistance impacts clinical outcome of granulomatous colitis in boxer dogs. J. Vet. Intern. Med. 2010, 24, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Churcher, R.K.; Watson, A. Canine histiocytic ulcerative colitis. Aust. Vet. J. 1997, 75, 710–713. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Nakayama, M.; Takase, K. Histiocytic ulcerative colitis in a French bulldog. J. Vet. Med. Sci. 2003, 65, 431–433. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Van der Gaag, I.; Van Toorenburg, J.V.; Voorhout, G.; Happe, R.P.; Aalfs, R.H.G. Histiocytic ulcerative colitis in a French Bulldog. J. Small Anim. Pract. 1978, 19, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Simpson, K.W.; Dogan, B.; Rishniw, M.; Goldstein, R.E.; Klaessig, S.; McDonough, P.L.; German, A.J.; Yates, R.M.; Russell, D.; Johnson, S.E.; et al. Adherent and invasive Escherichia coli is associated with granulomatous colitis in boxer dogs. Infect. Immun. 2006, 74, 4778–4792. [Google Scholar] [CrossRef] [PubMed]
- Leib, M.; Larson, M.; Grant, D.; Monroe, W.; Troy, G.; Panciera, D.; Rossmeisl, J.; Werre, S. Diagnostic utility of abdominal ultrasonography in dogs with chronic diarrhea. J. Vet. Intern. Med. 2012, 26, 1288–1294. [Google Scholar] [CrossRef]
- Mapletoft, E.K.; Allenspach, K.; Lamb, C.R. How useful is abdominal ultrasonography in dogs with diarrhoea? J. Small Anim. Pr. 2018, 59, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Penninck, D.; d’Anjou, M.A. Gastrointestinal tract. In Atlas of Small Animal Ultrasonography, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 251–300. [Google Scholar]
- Girlich, C.; Schacherer, D.; Jung, E.M.; Klebl, F.; Huber, E. Comparison between quantitative assessment of bowel wall vascularization by contrast-enhanced ultrasound and results of histopathological scoring in ulcerative colitis. Int. J. Color. Dis. 2011, 27, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Miao, L.-Y.; Ge, H.-Y.; Tan, S.; Li, Z.-Q.; Zhao, B. Usefulness of contrast-enhanced ultrasound in differentiating inflammatory bowel disease from colon cancer. Ultrasound Med. Biol. 2018, 44, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Fufezan, O.; Asavoaie, C.; Tamas, A.; Farcau, D.; Serban, E.D. Bowel elastography—A pilot study for developing an elastographic scoring system to evaluate disease activity in pediatric Crohn’s disease. Med. Ultrason. 2015, 17, 422–430. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stokes, J.; Kruger, J.M.; Mullaney, T.; Holan, K.; Schall, W. Histiocytic ulcerative colitis in three non-boxer dogs. J. Am. Anim. Hosp. Assoc. 2001, 37, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Citi, S.; Chimenti, T.; Marchetti, V.; Millanta, F.; Mannucci, T. Micronodular ultrasound lesions in the colonic submucosa of 42 dogs and 14 cats. Vet. Radiol. Ultrasound 2013, 54, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Nisa, K.; Lim, S.Y.; Shinohara, M.; Osuga, T.; Yokoyama, N.; Tamura, M.; Nagata, N.; Sasaoka, K.; Dermlim, A.; Leela-Arporn, R.; et al. Evaluation of duodenal perfusion by contrast-enhanced ultrasonography in dogs with chronic inflammatory enteropathy and intestinal lymphoma. J. Vet. Intern. Med. 2018, 33, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Spużak, J.; Kubiak, K.; Glińska-Suchocka, K.; Jankowski, M.; Borusewicz, P.; Kubiak-Nowak, D. Accuracy of real-time shear wave elastography in the assessment of normal small intestine mucosa in dogs. Pol. J. Vet. Sci. 2019, 22, 457–461. [Google Scholar] [PubMed]
- Mansfield, C.; James, F.; Craven, M.; Davies, D.; O’Hara, A.; Nicholls, P.; Dogan, B.; MacDonough, S.; Simpson, K. Remission of histiocytic ulcerative colitis in boxer dogs correlates with eradication of invasive intramucosal Escherichia coli. J. Vet. Intern. Med. 2009, 23, 964–969. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordella, A.; Stock, E.; Van de Maele, I.; Willems, A.; Saunders, J. Use of Contrast-Enhanced Ultrasonography and Shear-Wave Elastography in the Diagnosis of Granulomatous Colitis in a French Bulldog. Vet. Sci. 2021, 8, 133. https://doi.org/10.3390/vetsci8070133
Cordella A, Stock E, Van de Maele I, Willems A, Saunders J. Use of Contrast-Enhanced Ultrasonography and Shear-Wave Elastography in the Diagnosis of Granulomatous Colitis in a French Bulldog. Veterinary Sciences. 2021; 8(7):133. https://doi.org/10.3390/vetsci8070133
Chicago/Turabian StyleCordella, Alessia, Emmelie Stock, Isabel Van de Maele, Annelies Willems, and Jimmy Saunders. 2021. "Use of Contrast-Enhanced Ultrasonography and Shear-Wave Elastography in the Diagnosis of Granulomatous Colitis in a French Bulldog" Veterinary Sciences 8, no. 7: 133. https://doi.org/10.3390/vetsci8070133
APA StyleCordella, A., Stock, E., Van de Maele, I., Willems, A., & Saunders, J. (2021). Use of Contrast-Enhanced Ultrasonography and Shear-Wave Elastography in the Diagnosis of Granulomatous Colitis in a French Bulldog. Veterinary Sciences, 8(7), 133. https://doi.org/10.3390/vetsci8070133