
Non Epitheliotropic B-Cell Lymphoma with Plasmablastic Differentiation vs. Cutaneous Plasmacytosis in a 12-Years-Old Beagle: Case Presentation and Clinical Review

 ,
,
Abstract
:1. Introduction
2. Case Report
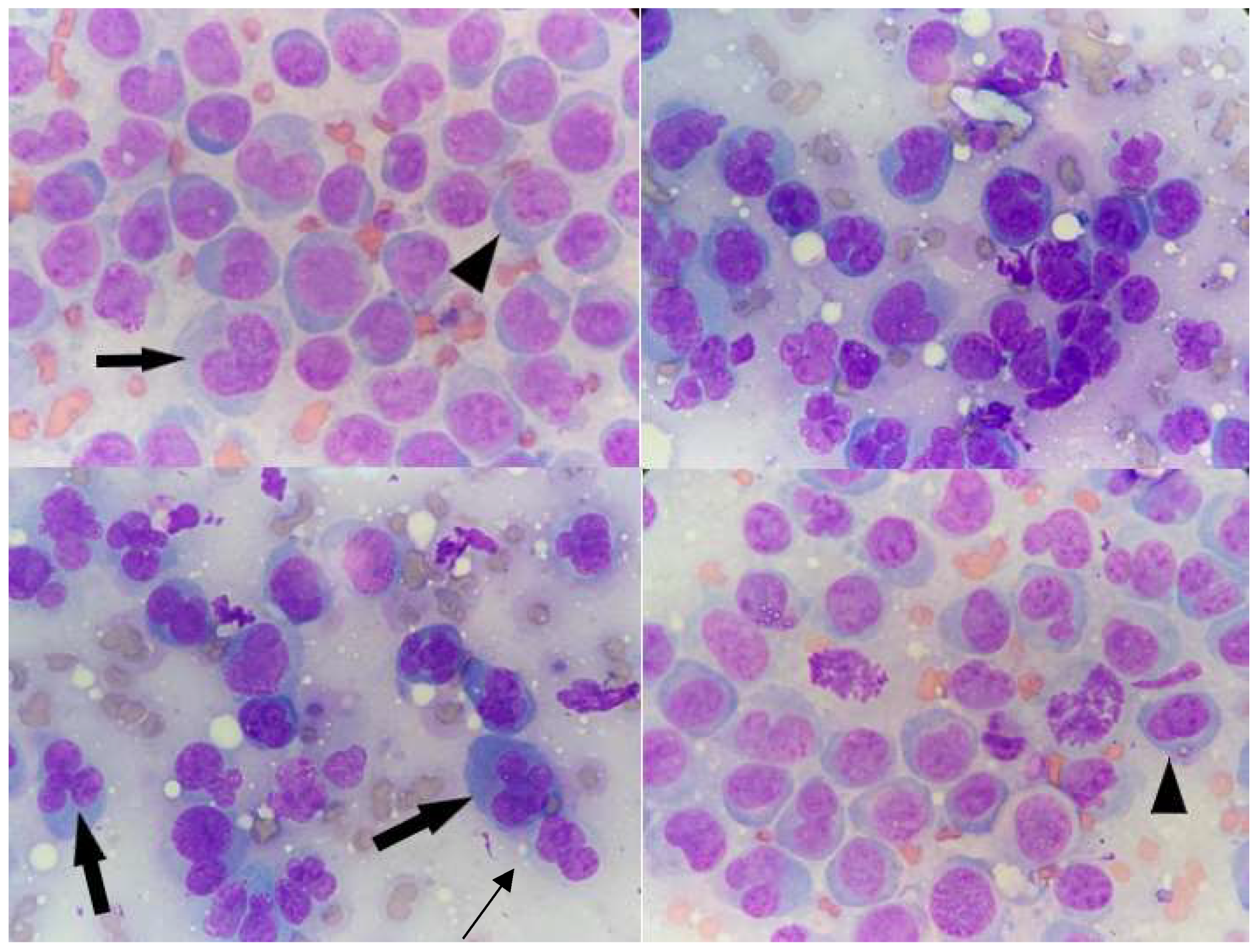
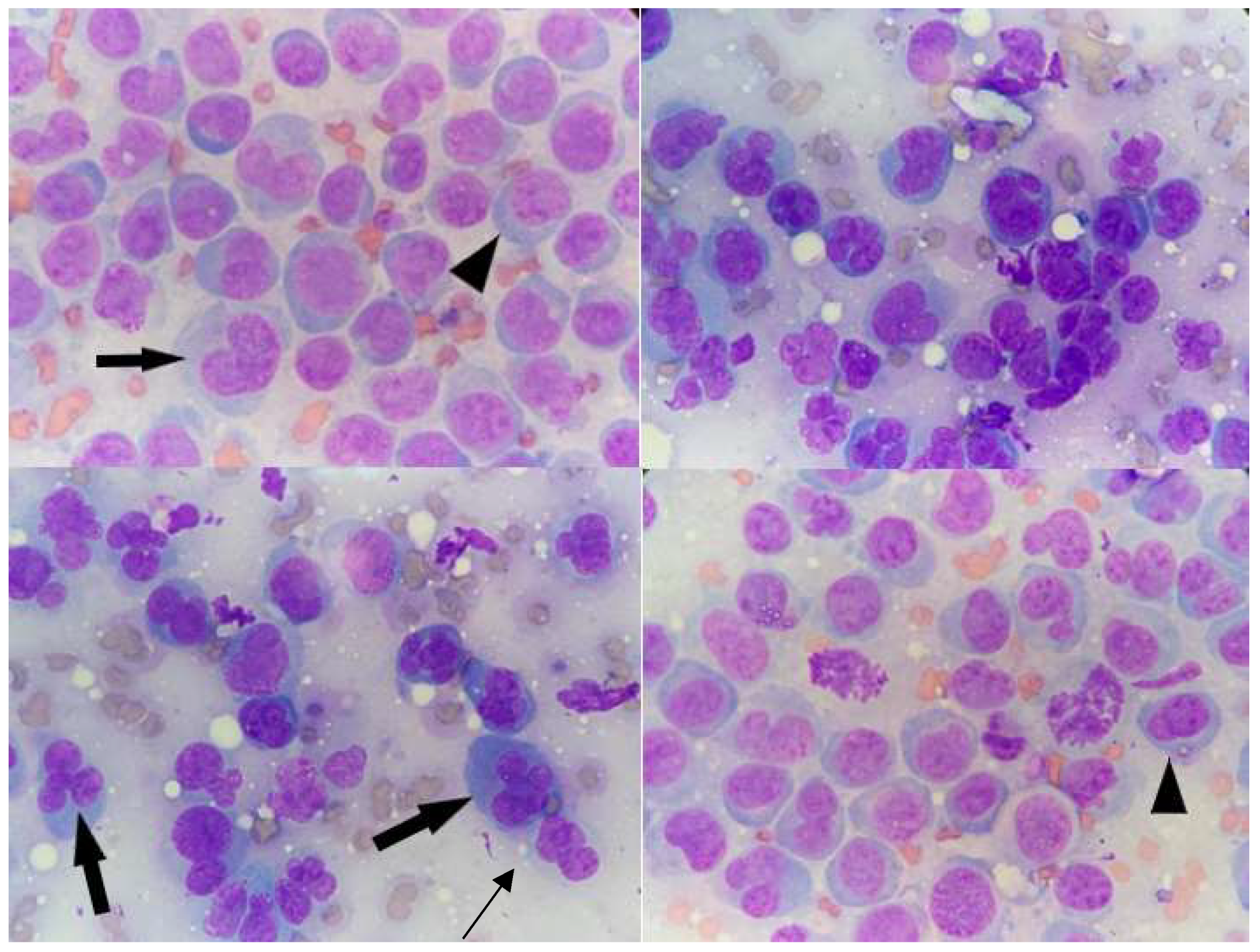
3. Cytology
4. Histopathology
5. Flow Cytometry
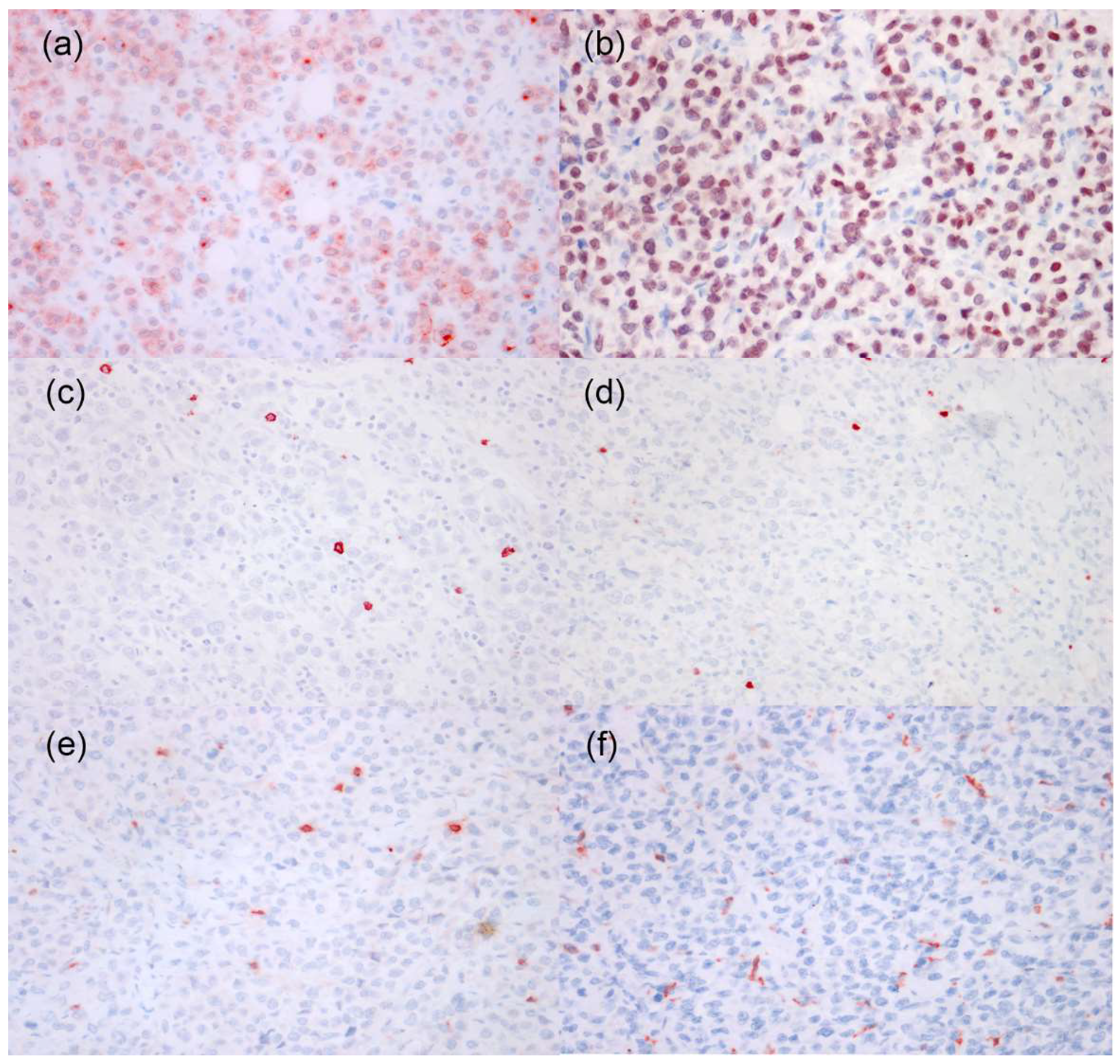
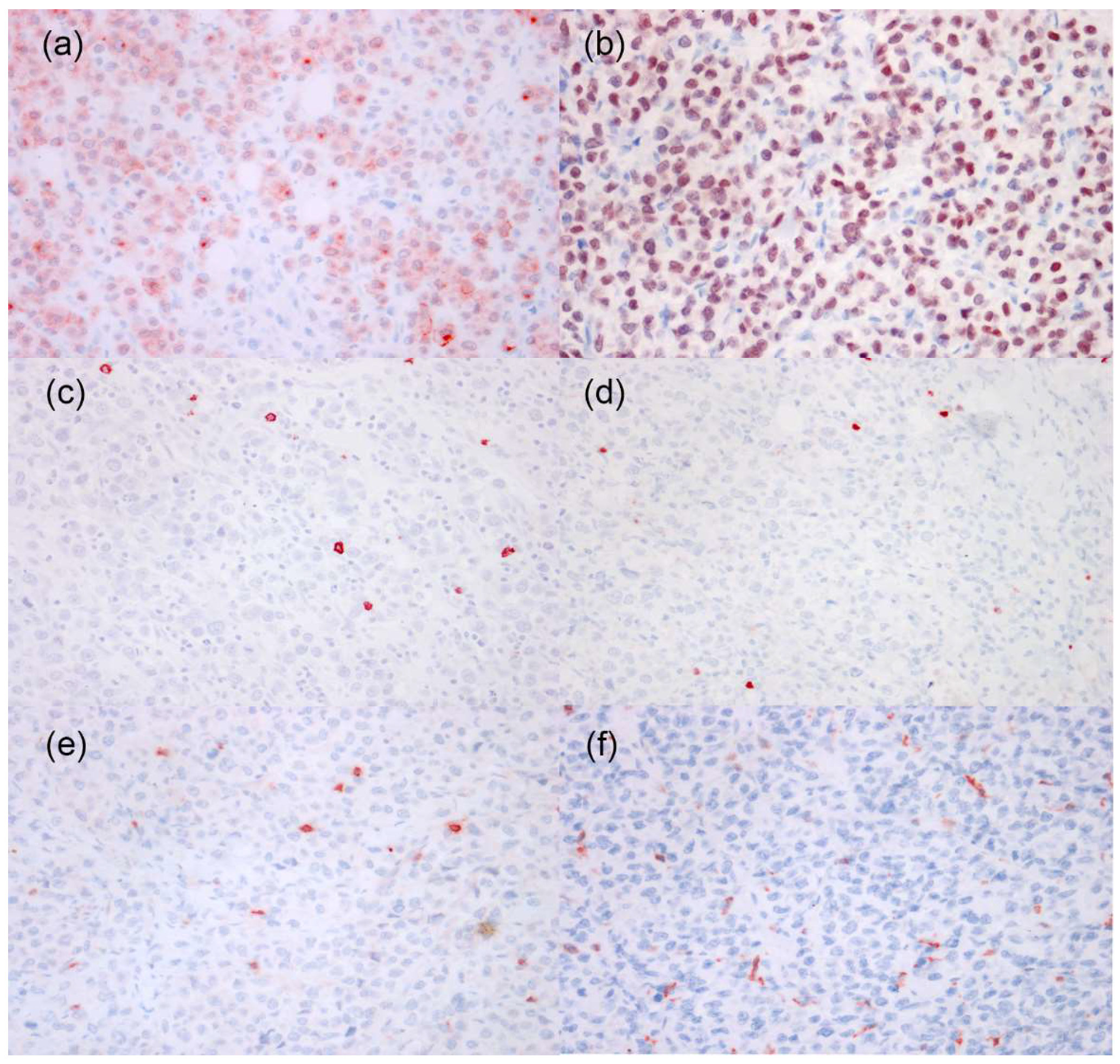
6. Immunohistochemistry
7. Chemotherapy
8. Follow-Up
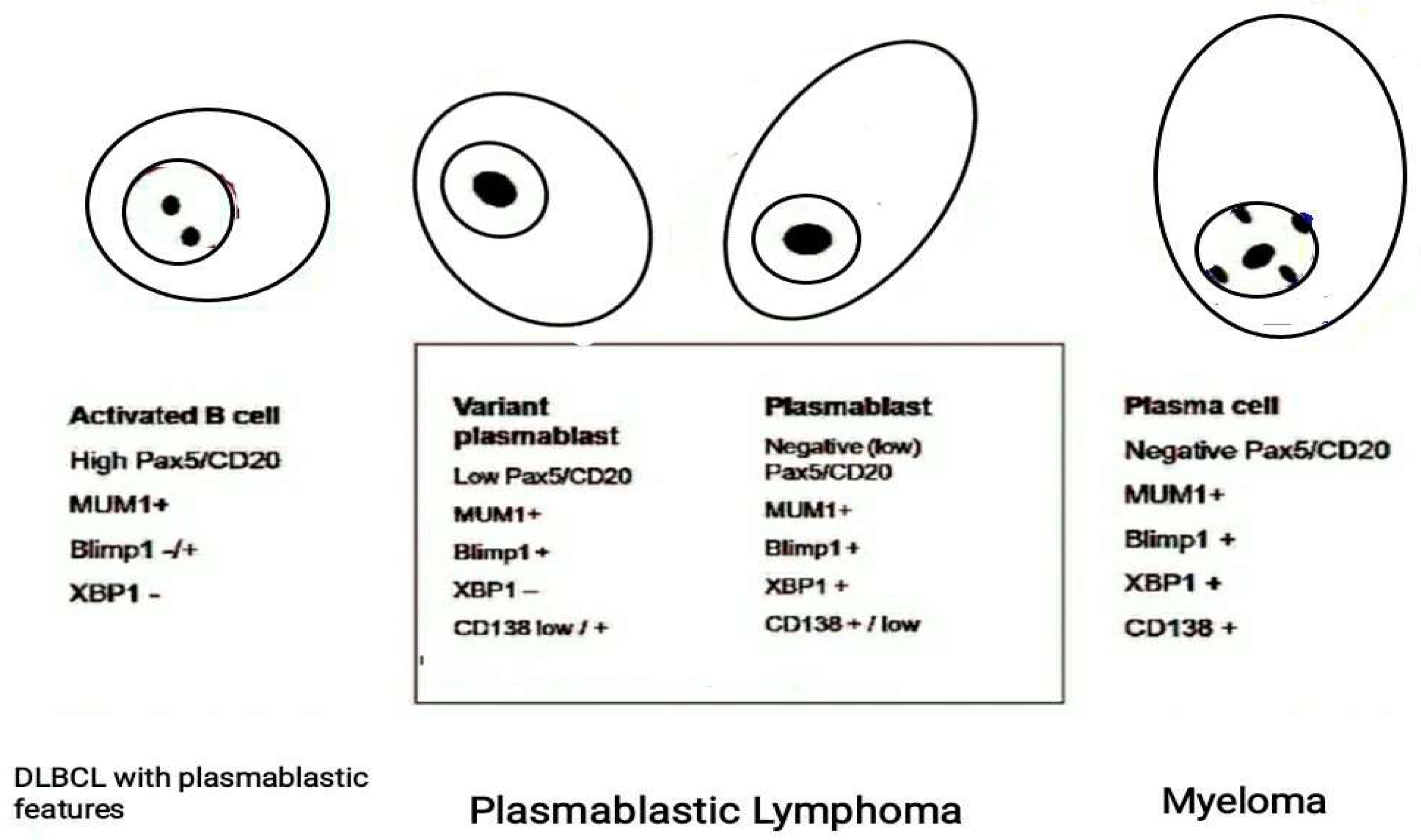
9. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cangul, I.T.; Wijnen, M.; Van Garderen, E.; van den Ingh, T.S.G.A.M. Clinico-Pathological Aspects of Canine Cutaneous and Mucocutaneous Plasmacytomas. J. Vet. Med. A Physiol. Pathol. Clin. Med. 2002, 49, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Pazdzior-Czapula, K.; Mikiewicz, M.; Gesek, M.; Zwolinski, C.; Otrocka-Domagala, I. Diagnostic Immunohistochemistry for Canine Cutaneous Round Cell Tumours—Retrospective Analysis of 60 Cases. Folia Histochem. Cytobiol. 2019, 57, 146–154. [Google Scholar] [CrossRef]
- Erich, S.A.; Constantino-Casas, F.; Dobson, J.M.; Teske, E. Morphological Distinction of Histiocytic Sarcoma from Other Tumor Types in Bernese Mountain Dogs and Flatcoated Retrievers. In Vivo 2018, 32, 7–17. [Google Scholar] [CrossRef] [Green Version]
- Fontaine, J.; Bovens, C.; Bettenay, S.; Mueller, R.S. Canine Cutaneous Epitheliotropic T-Cell Lymphoma: A Review. Vet. Comp. Oncol. 2009, 7, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Skin Tumors of the Dog and Cat. Available online: https://www.cabdirect.org/cabdirect/abstract/19932278375 (accessed on 21 September 2021).
- Rook, K.A. Canine and Feline Cutaneous Epitheliotropic Lymphoma and Cutaneous Lymphocytosis. Vet. Clin. N. Am. Small Anim. Pract. 2019, 49, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Gross, T.L.; Ihrke, P.J.; Walder, E.J.; Affolter, V.K. Skin Diseases of the Dog and Cat: Clinical and Histopathologic Diagnosis; John Wiley & Sons: Oxford, UK, 2008; ISBN 978-0-470-75247-0. [Google Scholar]
- Muller and Kirk’s Small Animal Dermatology—6th Edition. Available online: https://www.elsevier.com/books/muller-and-kirks-small-animal-dermatology/scott/978-0-7216-7618-0 (accessed on 18 May 2021).
- Small Animal Dermatology Secrets—1st Edition. Available online: https://www.elsevier.com/books/small-animal-dermatology-secrets/campbell/978-1-56053-626-0 (accessed on 18 May 2021).
- Moore, P.F.; Olivry, T.; Naydan, D. Canine Cutaneous Epitheliotropic Lymphoma (Mycosis Fungoides) Is a Proliferative Disorder of CD8+ T Cells. Am. J. Pathol. 1994, 144, 421–429. [Google Scholar]
- Moore, P.F.; Affolter, V.K.; Olivry, T.; Schrenzel, M.D. The Use of Immunological Reagents in Defining the Pathogenesis of Canine Skin Diseases Involving Proliferation of Leukocytes; Butterworth-Heinemann Ltd.: Oxford, UK, 1998. [Google Scholar]
- Bosschere, H.D.; Declercq, J. Cutaneous Nonepitheliotropic B-Cell Lymphoma in a Golden Retriever. Vlaams Diergeneeskundig Tijdschrift 2008, 77, 315–318. [Google Scholar]
- Day, M.J. Immunophenotypic Characterization of Cutaneous Lymphoid Neoplasia in the Dog and Cat. J. Comp. Pathol. 1995, 112, 79–96. [Google Scholar] [CrossRef]
- Witt, S.; Willeke, K.; Köhler, K.; Bauer, N. Non-epitheliotropic B-cell lymphoma with atypical spindle cell morphology in a Weimaraner dog. Tierarztl. Prax. Ausg. K Kleintiere Heimtiere 2018, 46, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Cortina, B.; Guenthner, E.; Sypniewski, L. Subcutaneous B Cell Lymphoma in a Dog from the West Indies. Case Rep. Vet. Med. 2020, 2020, 3695130. [Google Scholar] [CrossRef] [Green Version]
- Quintavalla, F.; Di Lecce, R.; Carlini, D.; Zanfabro, M.; Cantoni, A.M. Multifocal Cutaneous Non-Epitheliotropic B-Cell Lymphoma in a Cat. JFMS Open Rep. 2020, 6, 2055116920972077. [Google Scholar] [CrossRef] [PubMed]
- Kodama, A.; Tani, M.; Hori, K.; Tozuka, T.; Matsui, T.; Ito, M.; Nakao, S.; Fujita, T.; Kobayashi, H. Systemic and Cutaneous Plasmacytosis with Multiple Skin Lesions and Polyclonal Hypergammaglobulinaemia: Significant Serum Interleukin-6 Levels. Br. J. Dermatol. 1992, 127, 49–53. [Google Scholar] [CrossRef]
- Boostrom, B.O.; Moore, A.S.; DeRegis, C.J.; Robat, C.; Freeman, K.; Thamm, D.H. Canine Cutaneous Plasmacytosis: 21 Cases (2005–2015). J. Vet. Intern. Med. 2017, 31, 1074–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Lee, J.K.; Kim, J.; Choi, U.S.; Seo, K.W. Multiple Cutaneous Plasmacytosis with Multilobated (Clover-Leaf Shaped) Nuclei Cells in a Dog. Vet. Med. Sci. 2020, 6, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Honda, R.; Cerroni, L.; Tanikawa, A.; Ebihara, T.; Amagai, M.; Ishiko, A. Cutaneous Plasmacytosis: Report of 6 Cases with or without Systemic Involvement. J. Am. Acad. Dermatol. 2013, 68, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.; Hou, J.S.; Hisamichi, K.; Tamada, K.; Cusack, C.A.; Abdelmalek, M.; Brown, R.E.; Vonderheid, E.C. Cutaneous and Systemic Plasmacytosis vs. Cutaneous Plasmacytic Castleman Disease: Review and Speculations about Pathogenesis. Clin. Lymphoma Myeloma Leuk. 2011, 11, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Hahn, K.A.; Richardson, R.C.; Teclaw, R.F.; Cline, J.M.; Carlton, W.W.; DeNicola, D.B.; Bonney, P.L. Is Maintenance Chemotherapy Appropriate for the Management of Canine Malignant Lymphoma? J. Vet. Intern. Med. 1992, 6, 3–10. [Google Scholar] [CrossRef]
- Fritz, D.; Freeman, K.P.; Hopfner, C.; Fontaine, O.D.; Seroka, M.; Simon, F.; Musch, D.; Rabeyrin, M. Multilobulated “Flower” Cells in a Subcutaneous Mass Aspirate from a Cat. Vet. Clin. Pathol. 2005, 34, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Sokołowska, J.; Micuń, J.; Zabielska, K.; Malicka, E.; Lechowski, R. Immunohistochemical Study of Expression of Immunoglobulins in Canine B-Cell Lymphomas. Pol. J. Vet. Sci. 2010, 13, 623–628. [Google Scholar] [CrossRef] [Green Version]
- Kol, A.; Christopher, M.M.; Skorupski, K.A.; Tokarz, D.; Vernau, W. B-Cell Lymphoma with Plasmacytoid Differentiation, Atypical Cytoplasmic Inclusions, and Secondary Leukemia in a Dog. Vet. Clin. Pathol. 2013, 42, 40–46. [Google Scholar] [CrossRef]
- Gualco, G.; Weiss, L.M.; Bacchi, C.E. MUM1/IRF4: A Review. Appl. Immunohistochem. Mol. Morphol. 2010, 18, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Vara, J.A.; Miller, M.A.; Valli, V.E.O. Immunohistochemical Detection of Multiple Myeloma 1/Interferon Regulatory Factor 4 (MUM1/IRF-4) in Canine Plasmacytoma: Comparison with CD79a and CD20. Vet. Pathol. 2007, 44, 875–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seelig, D.M.; Perry, J.A.; Zaks, K.; Avery, A.C.; Avery, P.R. Monoclonal Immunoglobulin Protein Production in Two Dogs with Secretory B-Cell Lymphoma with Mott Cell Differentiation. J. Am. Vet. Med. Assoc. 2011, 239, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gumber, S.; Schnellbacher, R.; Bauer, R.W.; Gaunt, S.D. Malignant B-Cell Lymphoma with Mott Cell Differentiation in a Ferret (Mustela Putorius Furo). J. Vet. Diagn. Investig. 2010, 22, 469–473. [Google Scholar] [CrossRef] [Green Version]
- Snyman, H.N.; Fromstein, J.M.; Vince, A.R. A Rare Variant of Multicentric Large B-Cell Lymphoma with Plasmacytoid and Mott Cell Differentiation in a Dog. J. Comp. Pathol. 2013, 148, 329–334. [Google Scholar] [CrossRef]
- Kodama, A.; Sakai, H.; Kobayashi, K.; Mori, T.; Maruo, K.; Kudo, T.; Yanai, T.; Masegi, T. B-Cell Intestinal Lymphoma with Mott Cell Differentiation in a 1-Year-Old Miniature Dachshund. Vet. Clin. Pathol. 2008, 37, 409–415. [Google Scholar] [CrossRef]
- Stacy, N.I.; Nabity, M.B.; Hackendahl, N.; Buote, M.; Ward, J.; Ginn, P.E.; Vernau, W.; Clapp, W.L.; Harvey, J.W. B-Cell Lymphoma with Mott Cell Differentiation in Two Young Adult Dogs. Vet. Clin. Pathol. 2009, 38, 113–120. [Google Scholar] [CrossRef]
- De Zan, G.; Zappulli, V.; Cavicchioli, L.; Di Martino, L.; Ros, E.; Conforto, G.; Castagnaro, M. Gastric B-Cell Lymphoma with Mott Cell Differentiation in a Dog. J. Vet. Diagn. Investig. 2009, 21, 715–719. [Google Scholar] [CrossRef]
- Lopez, A.; Abrisqueta, P. Plasmablastic Lymphoma: Current Perspectives. Blood Lymphat. Cancer 2018, 8, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Montes-Moreno, S.; Montalbán, C.; Piris, M.A. Large B-Cell Lymphomas with Plasmablastic Differentiation: A Biological and Therapeutic Challenge. Leuk Lymphoma 2012, 53, 185–194. [Google Scholar] [CrossRef]
- Montes-Moreno, S.; Gonzalez-Medina, A.-R.; Rodriguez-Pinilla, S.-M.; Maestre, L.; Sanchez-Verde, L.; Roncador, G.; Mollejo, M.; García, J.F.; Menarguez, J.; Montalbán, C.; et al. Aggressive Large B-Cell Lymphoma with Plasma Cell Differentiation: Immunohistochemical Characterization of Plasmablastic Lymphoma and Diffuse Large B-Cell Lymphoma with Partial Plasmablastic Phenotype. Haematologica 2010, 95, 1342–1349. [Google Scholar] [CrossRef] [Green Version]
- Harmon, C.M.; Smith, L.B. Plasmablastic Lymphoma: A Review of Clinicopathologic Features and Differential Diagnosis. Arch. Pathol. Lab. Med. 2016, 140, 1074–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega, F.; Chang, C.C.; Medeiros, L.J.; Udden, M.M.; Cho-Vega, J.H.; Lau, C.C.; Finch, C.J.; Vilchez, R.A.; McGregor, D.; Jorgensen, J.L. Plasmablastic Lymphomas and Plasmablastic Plasma Cell Myelomas Have Nearly Identical Immunophenotypic Profiles. Mod. Pathol. 2005, 18, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; LeBlanc, R.E.; Carter, J.B. Cutaneous B-Cell Lymphoma. Hematol./Oncol. Clin. N. Am. 2019, 33, 149–161. [Google Scholar] [CrossRef]
- Zinzani, P.L.; Quaglino, P.; Pimpinelli, N.; Berti, E.; Baliva, G.; Rupoli, S.; Martelli, M.; Alaibac, M.; Borroni, G.; Chimenti, S.; et al. Prognostic Factors in Primary Cutaneous B-Cell Lymphoma: The Italian Study Group for Cutaneous Lymphomas. J. Clin. Oncol. 2006, 24, 1376–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olszewska-Szopa, M.; Sobas, M.; Laribi, K.; Bao Perez, L.; Drozd-Sokołowska, J.; Subocz, E.; Joks, M.; Zduniak, K.; Gajewska, M.; de Nalecz, A.K.; et al. Primary Cutaneous Indolent B-Cell Lymphomas—A Retrospective Multicenter Analysis and a Review of Literature. Acta Oncol. 2021, 60, 1361–1368. [Google Scholar] [CrossRef]
- Miglio, A.; Morelli, C.; Gialletti, R.; Lauteri, E.; Sforna, M.; Marenzoni, M.L.; Antognoni, M.T. Clinical and Immunophenotypic Findings in 4 Forms of Equine Lymphoma. Can. Vet. J. 2019, 60, 33–40. [Google Scholar]
- Antognoni, M.T.; Birettoni, F.; Miglio, A.; Lalli, P.; Porciello, F.; Mangili Pecci, V. Monoclonal Gammopathy Associated with Multiple Myeloma and Visceral Leishmaniasis in the Dog: A Comparison of Two Cases. Vet. Res. Commun. 2010, 34 (Suppl. 1), S97–S101. [Google Scholar] [CrossRef] [Green Version]
- Miglio, A.; Antognoni, M.T.; Maresca, C.; Moncada, C.; Riondato, F.; Scoccia, E.; Mangili, V. Serum Protein Concentration and Protein Fractions in Clinically Healthy Lacaune and Sarda Sheep Using Agarose Gel Electrophoresis. Vet. Clin. Pathol. 2015, 44, 564–569. [Google Scholar] [CrossRef]
- Miglio, A.; Antognoni, M.T.; Morelli, C.; Gialletti, R. Third Eyelid T-Cell-Rich Large B-Cell Lymphoma Positive to EHV-5 in a Mare—A Case Report. J. Equine Vet. Sci. 2018, 70, 52–56. [Google Scholar] [CrossRef]
- Marenzoni, M.L.; Antognoni, M.T.; Baldelli, F.; Miglio, A.; Stefanetti, V.; Desario, C.; Di Summa, A.; Buonavoglia, C.; Decaro, N. Detection of Parvovirus and Herpesvirus DNA in the Blood of Feline and Canine Blood Donors. Vet. Microbiol. 2018, 224, 66–69. [Google Scholar] [CrossRef]
- Wagner, G.; Rose, C.; Klapper, W.; Sachse, M.M. Cutaneous and Systemic Plasmocytosis. J. Dtsch. Dermatol. Ges. 2013, 11, 1161–1167. [Google Scholar] [CrossRef] [Green Version]
- Uhara, H.; Saida, T.; Ikegawa, S.; Yamazaki, Y.; Mikoshiba, H.; Nijoh, S.; Kitano, K.; Koh, C.S. Primary Cutaneous Plasmacytosis: Report of Three Cases and Review of the Literature. Dermatology 1994, 189, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Leonard, A.L.; Meehan, S.A.; Ramsey, D.; Brown, L.; Sen, F. Cutaneous and Systemic Plasmacytosis. J. Am. Acad. Dermatol. 2007, 56, S38–S40. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.-H.; Shih, L.-Y.; Yang, C.-H.; Kuo, T.-T. Cutaneous Plasmacytosis: A Clinicopathologic Study of 12 Cases in Taiwan Revealing Heterogeneous Underlying Causes. Int. J. Dermatol. 2015, 54, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Han, X.D.; Lee, S.S.J.; Tan, S.H.; Chong, W.-S.; Ng, S.K.; Ooi, M.G.M.; Goh, C.L. Cutaneous Plasmacytosis: A Clinicopathologic Study of a Series of Cases and Their Treatment Outcomes. Am. J. Dermatopathol. 2018, 40, 36–42. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Matsumura, M. Cutaneous Plasmacytosis: A Rare Initial Presentation of Idiopathic Multicentric Castleman’s Disease. Clin. Case Rep. 2021, 9, e04109. [Google Scholar] [CrossRef]
- Hristov, A.C.; Comfere, N.I.; Vidal, C.I.; Sundram, U. Kappa and Lambda Immunohistochemistry and in Situ Hybridization in the Evaluation of Atypical Cutaneous Lymphoid Infiltrates. J. Cutan. Pathol. 2020, 47, 1103–1110. [Google Scholar] [CrossRef]
- Miglio, A.; Antognoni, M.T.; Miniscalco, B.; Caivano, D.; Lepri, E.; Birettoni, F.; Mangili, V. Acute Undifferentiated Leukaemia in a Dog. Aust. Vet. J. 2014, 92, 499–503. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MoAb | Result | Ab Source | Cell Type Expression |
|---|---|---|---|
| CD3 | − | Serotec, Oxford, UK | T cells |
| CD4 | − | Serotec, Oxford, UK | T cells, hystiocitic |
| CD5 | − | Serotec, Oxford, UK | T cells |
| CD8 | − | Serotec, Oxford, UK | T cells |
| CD11b | + | PF Moore, UC Davis, Davis, CA, USA | granulocytes, monocytes, macrophages |
| CD11d | − | Santa Cruz Biotechnology, Santa Cruz, CA, USA | lymphoid and histiocytic tumor |
| CD14 | − | VMRD, Pullman, WA, USA | Monocytes, macrophages |
| CD18 | + | PF Moore, UC Davis, USA | Leukocyte tumors |
| CD21 | − | Serotec, Oxford, UK | B cells |
| CD34 | − | Santa Cruz Biotechnology, CA, USA | pluripotent haematopoietic progenitor cells |
| CD44 | + | PF Moore, UC Davis, USA | panleucocytic |
| CD45 | + | Serotec, Oxford, UK | panleucocytic |
| CD79b | + | Serotec, Oxford, UK | B lymphocytes |
| CD117 | − | Santa Cruz Biotechnology, CA, USA | Mast cells, melanocytes, GIST tumor |
| IgE | + | Serotec, Oxford, UK | B cells, plasma cells |
| Antibody | Producer | Code/Clone | Dilution | AR Method | Results |
|---|---|---|---|---|---|
| CD79a (HM75) | Santa Cruz, Oregon, USA | Sc-53208 | 1:200 | Tris-EDTA pH 9.0 | +++ |
| MUM1 | Agilent Dako, Glostrup, Denmark | M7259 | 1:50 | Tris-EDTA pH 9.0 | +++ |
| CD20 | Thermo Scientific, Fremont, CA, USA | RB-9013-P1 | 1:200 | NOAR | −(+) |
| PAX5 | BD Bioscience, San Jose, CA, USA | 610863 | 1:20 | Tris-EDTA pH 9.0 | −(+) |
| CD3 | Agilent Dako, Glostrup, Denmark | A0452 | 1:200 | Tris-EDTA pH 9.0 | −(+) |
| Iba1 | Abcam, San Jose, CA, USA | Ab107159 | 1:250 | Tris-EDTA pH 9.0 | −(+) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antognoni, M.T.; Misia, A.L.; Brachelente, C.; Mechelli, L.; Paolini, A.; Miglio, A. Non Epitheliotropic B-Cell Lymphoma with Plasmablastic Differentiation vs. Cutaneous Plasmacytosis in a 12-Years-Old Beagle: Case Presentation and Clinical Review. Vet. Sci. 2021, 8, 317. https://doi.org/10.3390/vetsci8120317
Antognoni MT, Misia AL, Brachelente C, Mechelli L, Paolini A, Miglio A. Non Epitheliotropic B-Cell Lymphoma with Plasmablastic Differentiation vs. Cutaneous Plasmacytosis in a 12-Years-Old Beagle: Case Presentation and Clinical Review. Veterinary Sciences. 2021; 8(12):317. https://doi.org/10.3390/vetsci8120317
Chicago/Turabian StyleAntognoni, Maria Teresa, Ambra Lisa Misia, Chiara Brachelente, Luca Mechelli, Andrea Paolini, and Arianna Miglio. 2021. "Non Epitheliotropic B-Cell Lymphoma with Plasmablastic Differentiation vs. Cutaneous Plasmacytosis in a 12-Years-Old Beagle: Case Presentation and Clinical Review" Veterinary Sciences 8, no. 12: 317. https://doi.org/10.3390/vetsci8120317
APA StyleAntognoni, M. T., Misia, A. L., Brachelente, C., Mechelli, L., Paolini, A., & Miglio, A. (2021). Non Epitheliotropic B-Cell Lymphoma with Plasmablastic Differentiation vs. Cutaneous Plasmacytosis in a 12-Years-Old Beagle: Case Presentation and Clinical Review. Veterinary Sciences, 8(12), 317. https://doi.org/10.3390/vetsci8120317