
Evaluation of the Use of Platelet-Rich Fibrin Xenologous Membranes Derived from Bubaline Blood in Canine Periodontal Defects

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. PRF Preparation
2.2. Clinical Study in Animals
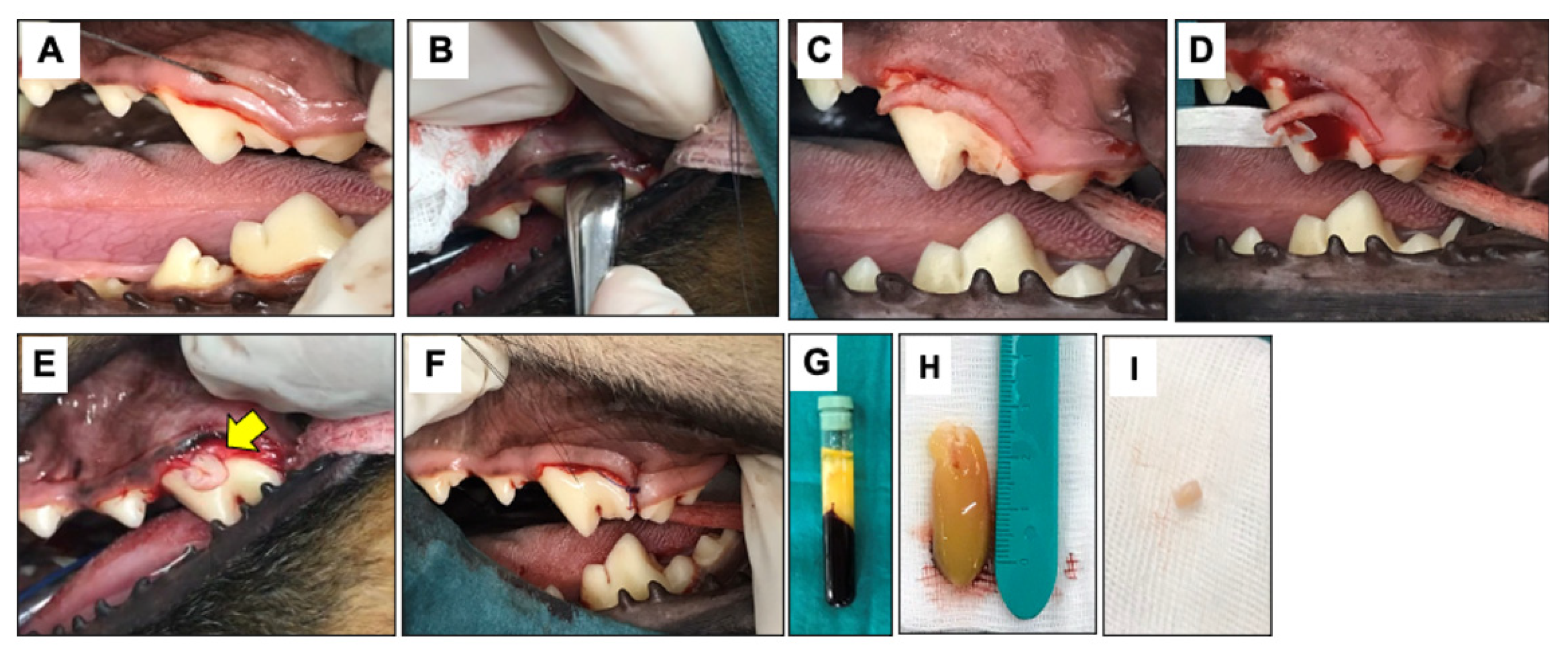
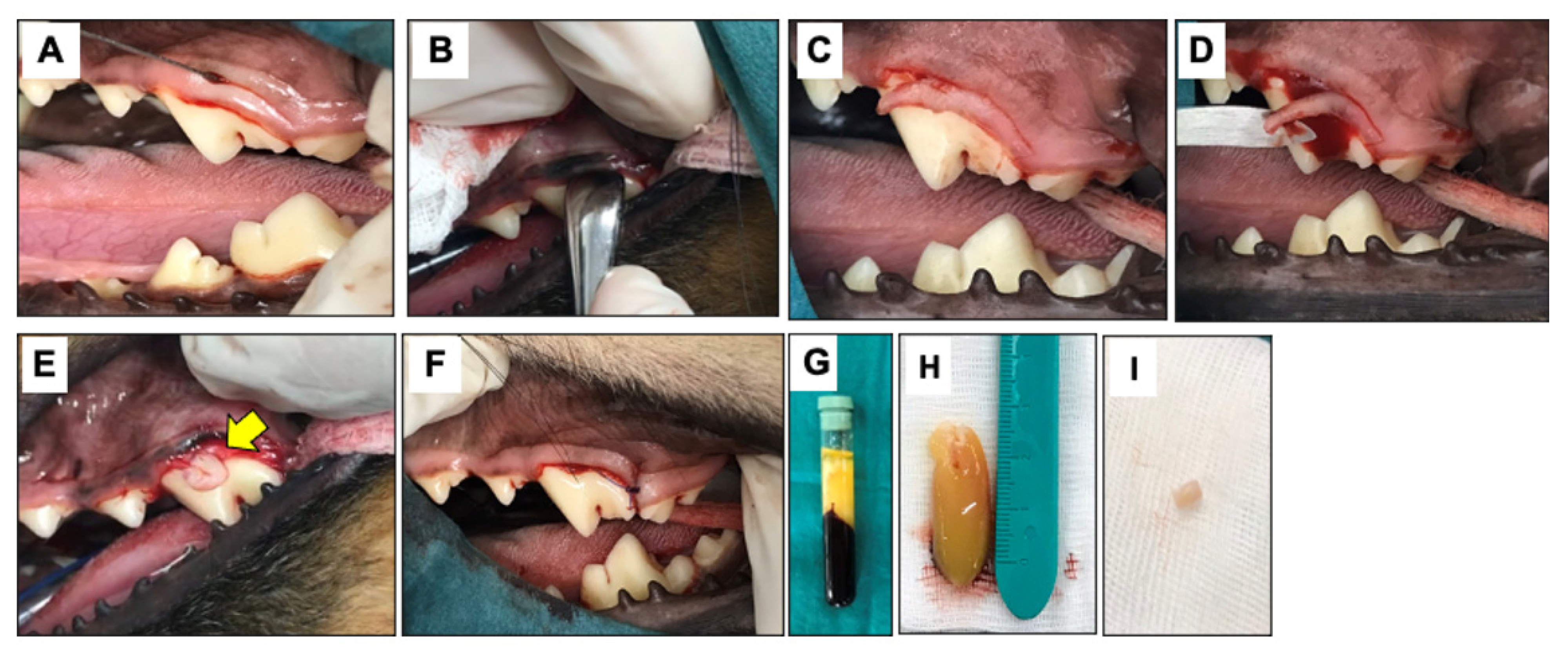
2.3. Surgical Procedure and PRF Administration
2.4. Clinical Examination
2.5. Radiographic Examination
2.6. Histopathological Analysis
2.7. Gene Expression Analysis
2.8. Statistical Analyses
3. Results
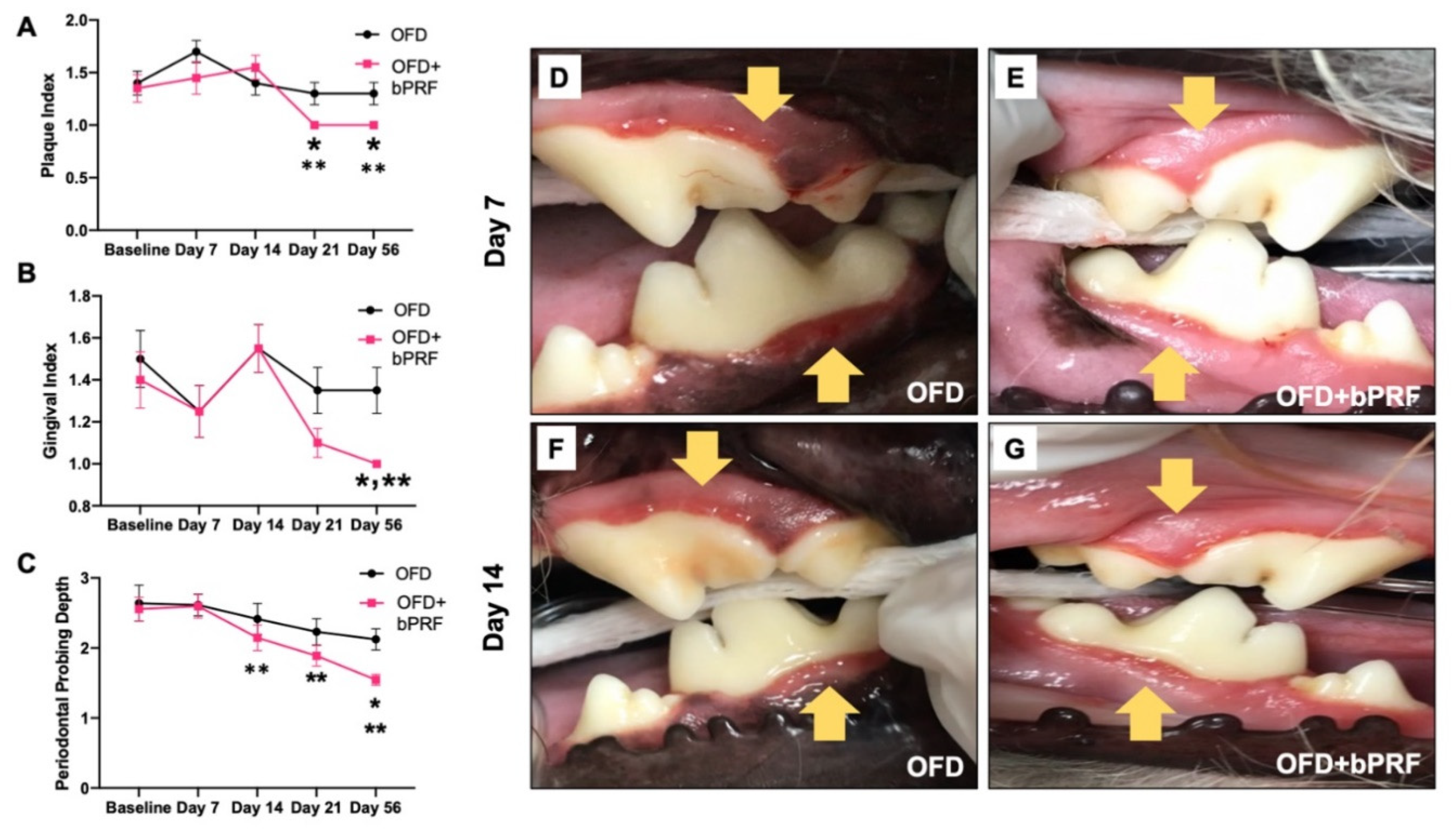
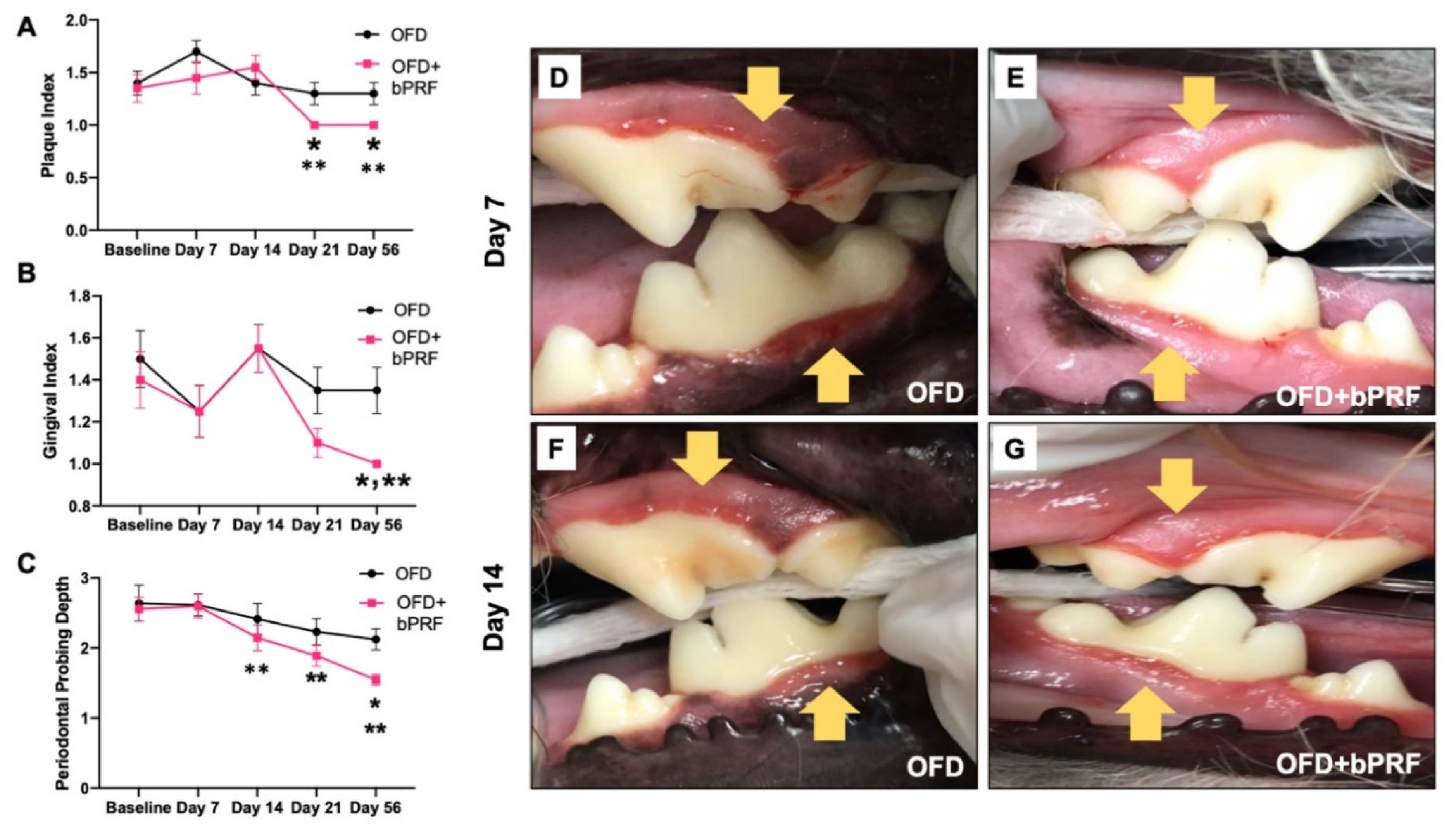
3.1. Clinical Examination
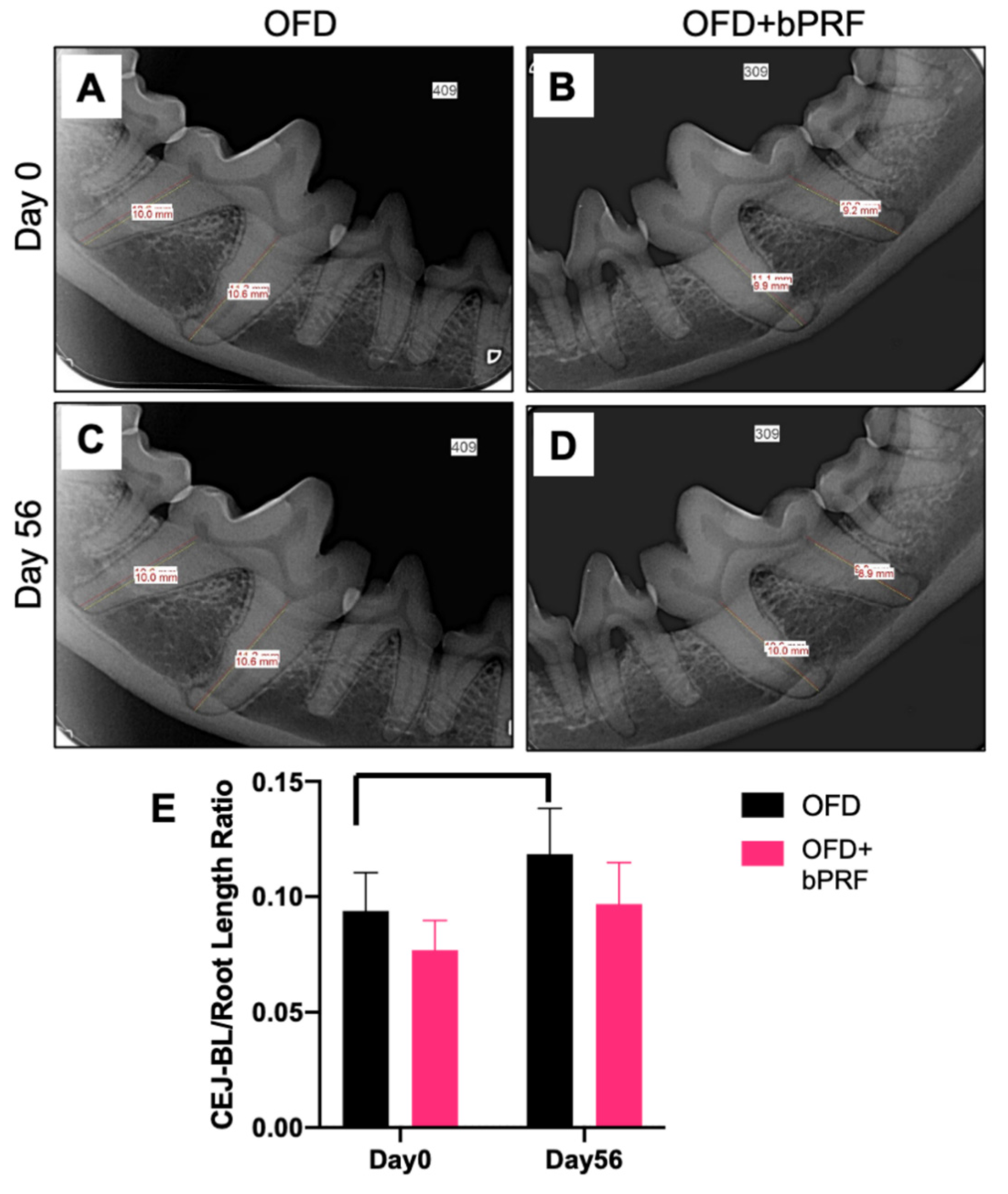
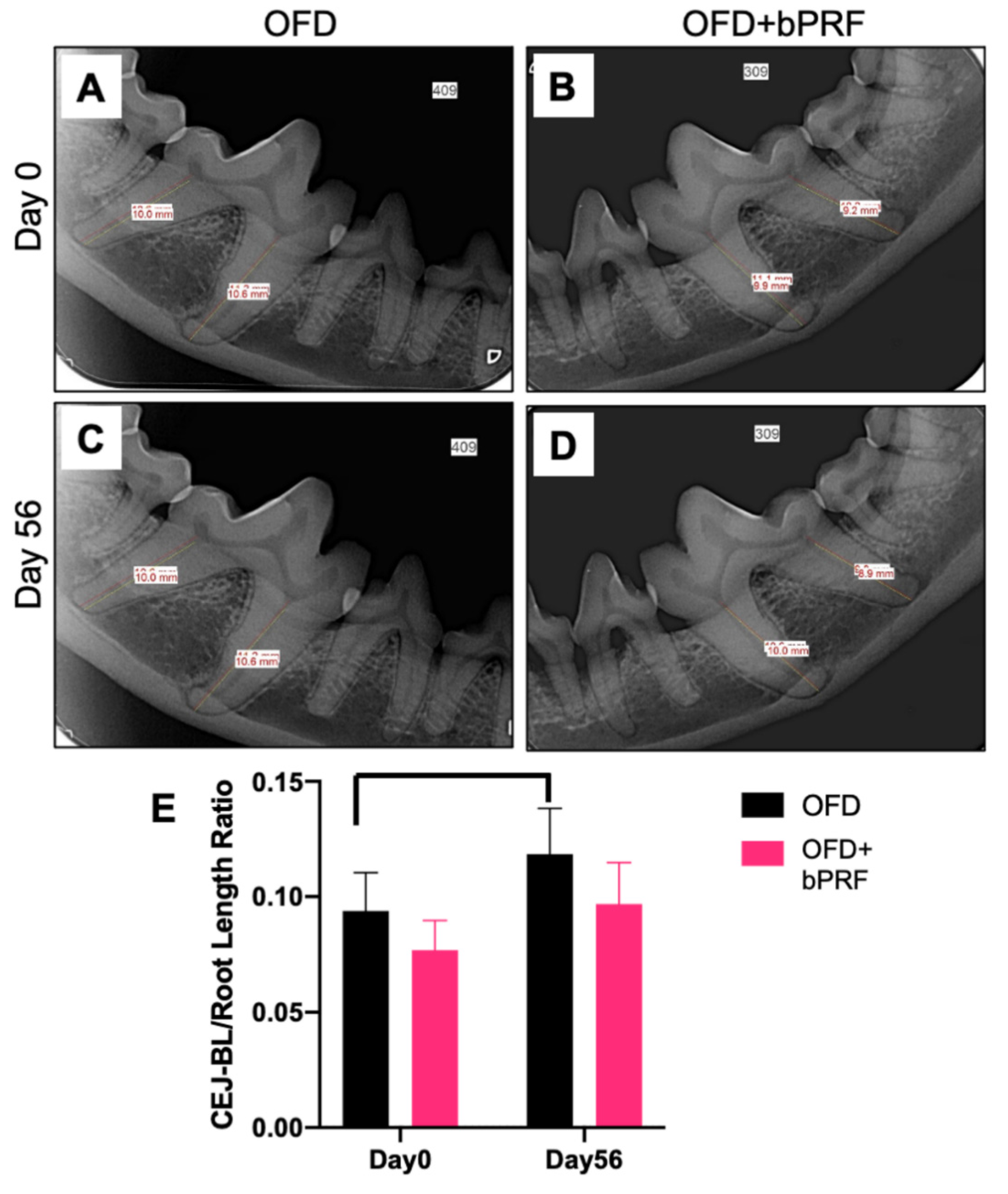
3.2. Radiographic Examination
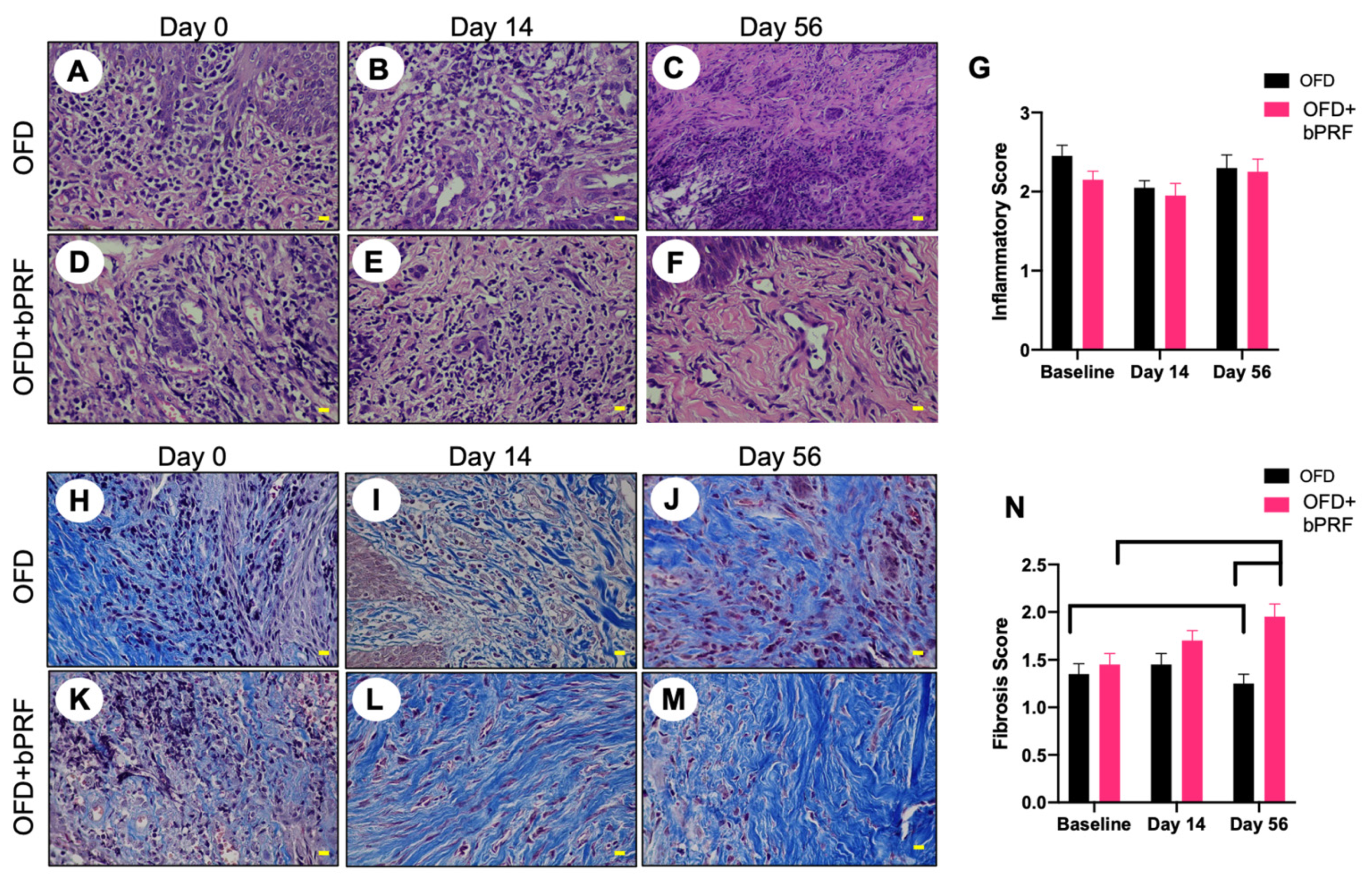
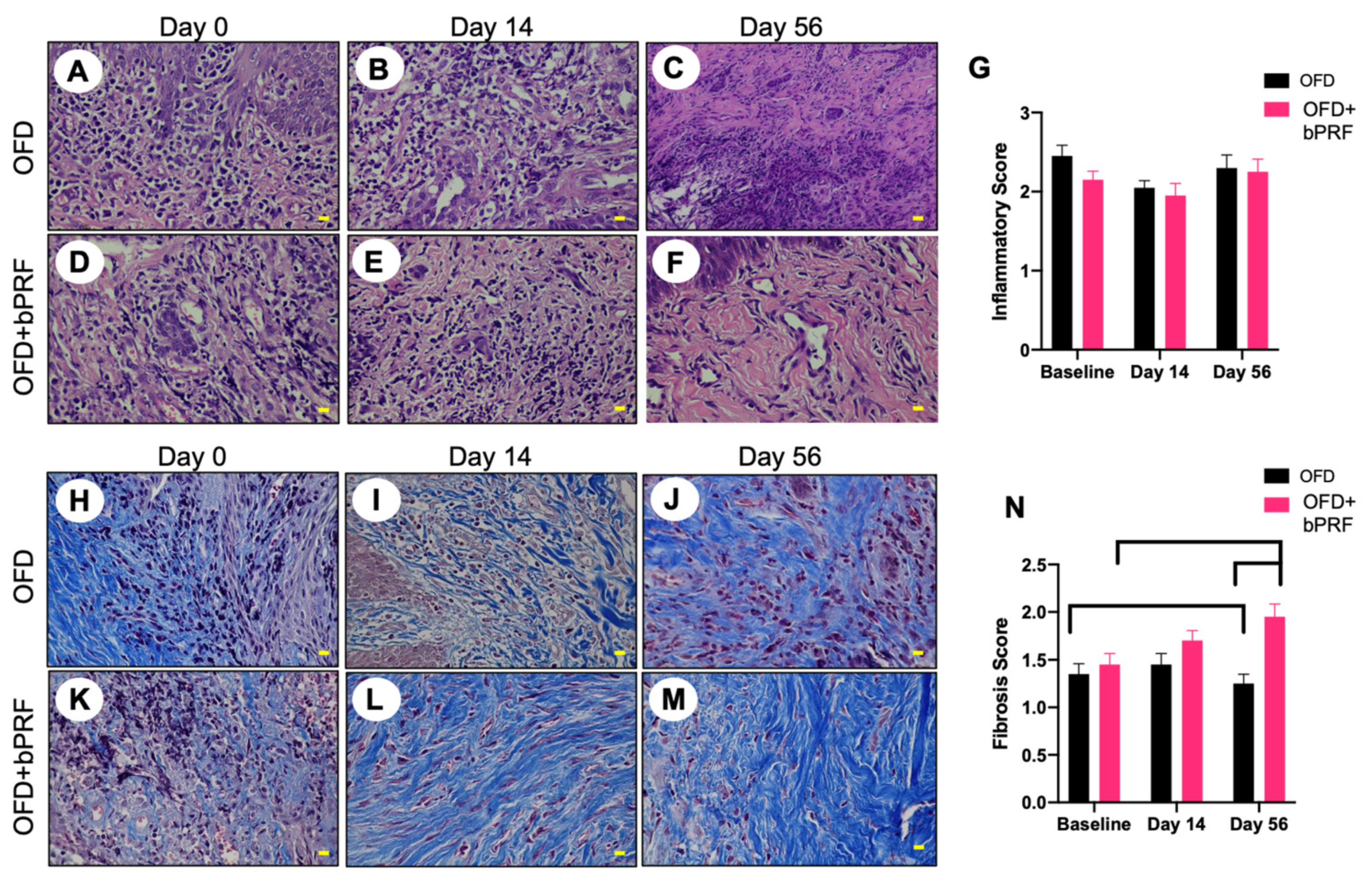
3.3. Histopathological Analyses
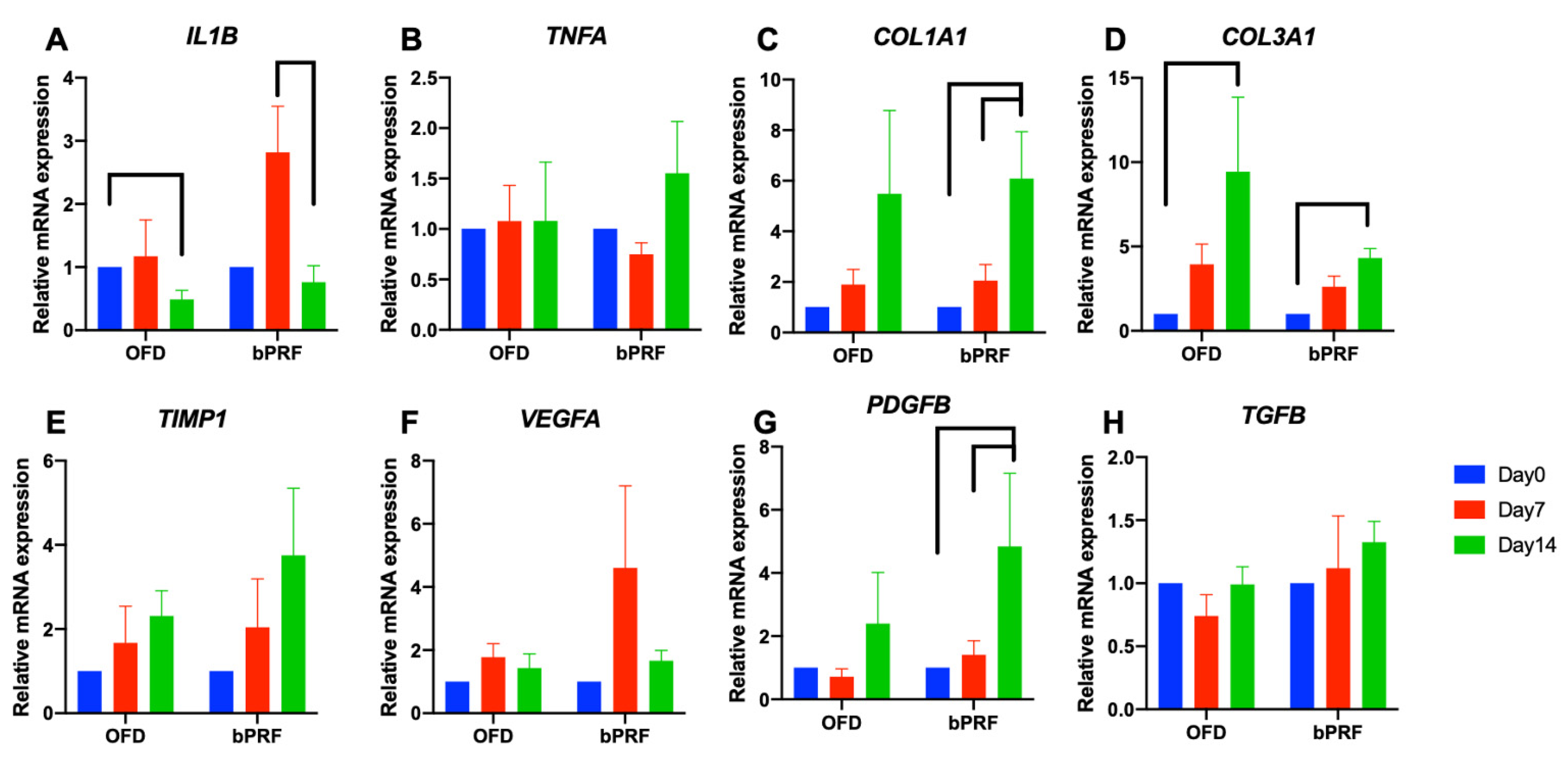
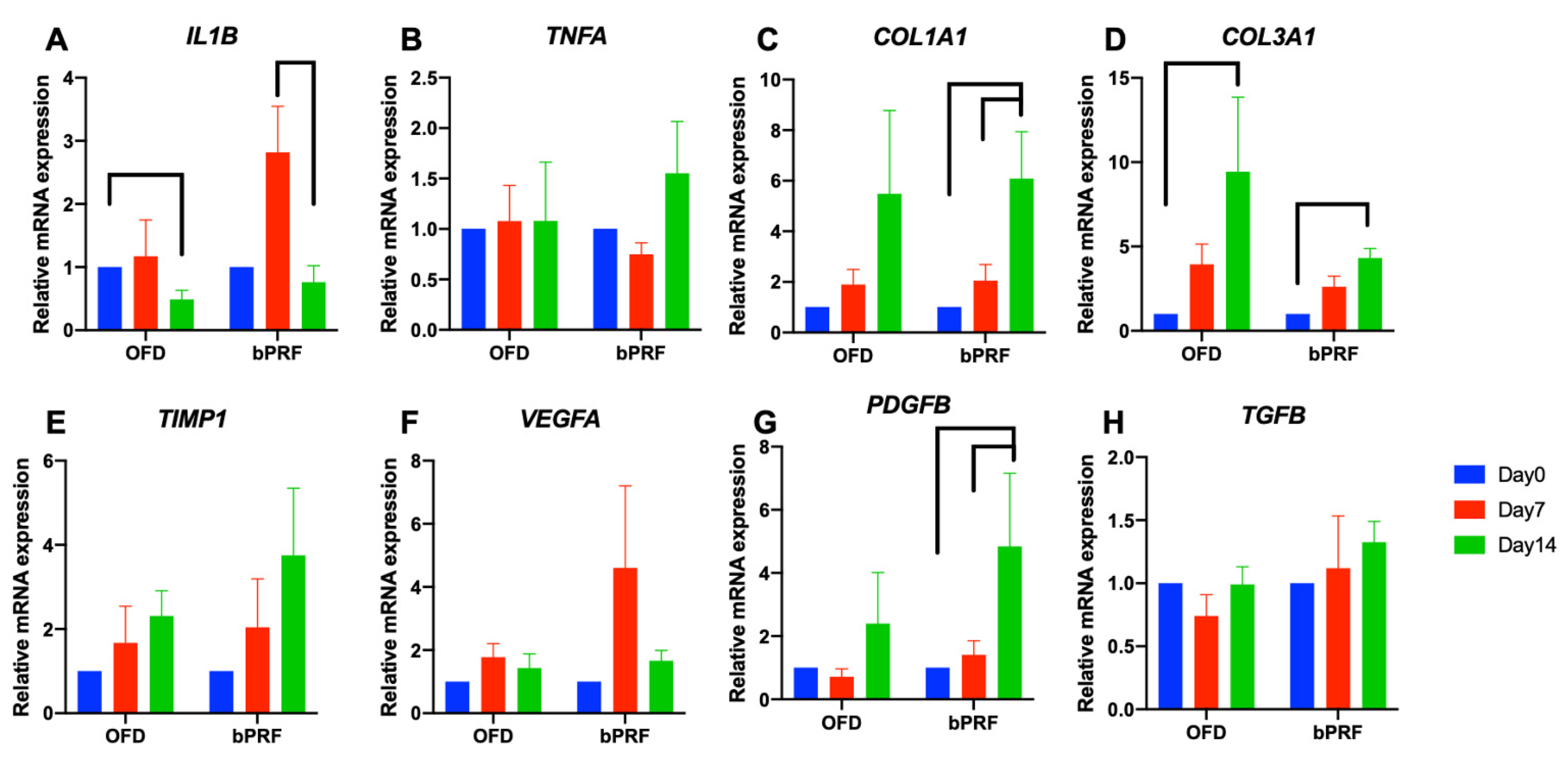
3.4. Gene Expression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kortegaard, H.E.; Eriksen, T.; Baelum, V. Periodontal disease in research beagle dogs—An epidemiological study. J. Small Anim. Pract. 2008, 49, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.; Gaengler, P. Epidemiology of periodontal disease in poodles. J. Small Anim. Pract. 1996, 37, 309–316. [Google Scholar] [CrossRef] [PubMed]
- AlJehani, Y.A. Risk factors of periodontal disease: Review of the literature. Int. J. Dent. 2014, 2014, 182513. [Google Scholar] [CrossRef] [Green Version]
- Susin, C.; Fiorini, T.; Lee, J.; De Stefano, J.A.; Dickinson, D.P.; Wikesjö, U.M. Wound healing following surgical and regenerative periodontal therapy. Periodontol. 2000 2015, 68, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Iviglia, G.; Kargozar, S.; Baino, F. Biomaterials, current strategies, and novel nano-technological approaches for periodontal regeneration. J. Funct. Biomater. 2019, 10, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas, M.A.; Marini, L.; Pilloni, A.; Sahrmann, P. Early wound healing outcomes after regenerative periodontal surgery with enamel matrix derivatives or guided tissue regeneration: A systematic review. BMC Oral Health 2019, 19, 76. [Google Scholar] [CrossRef]
- Schupbach, P.; Gaberthuel, T.; Lutz, F.; Guggenheim, B. Periodontal repair or regeneration: Structures of different types of new attachment. J. Periodontal Res. 1993, 28, 281–293. [Google Scholar] [CrossRef]
- Borie, E.; Olivi, D.G.; Orsi, I.A.; Garlet, K.; Weber, B.; Beltran, V.; Fuentes, R. Platelet-rich fibrin application in dentistry: A literature review. Int. J. Clin. Exp. Med. 2015, 8, 7922–7929. [Google Scholar]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Marchetti, E.; Mancini, L.; Bernardi, S.; Bianchi, S.; Cristiano, L.; Torge, D.; Marzo, G.; Macchiarelli, G. Evaluation of Different Autologous Platelet Concentrate Biomaterials: Morphological and Biological Comparisons and Considerations. Materials 2020, 13, 2282. [Google Scholar] [CrossRef]
- Muñoz, F.; Jiménez, C.; Espinoza, D.; Vervelle, A.; Beugnet, J.; Haidar, Z. Use of leukocyte and platelet-rich fibrin (L-PRF) in periodontally accelerated osteogenic orthodontics (PAOO): Clinical effects on edema and pain. J. Clin. Exp. Dent. 2016, 8, e119–e124. [Google Scholar] [PubMed] [Green Version]
- Ozgul, O.; Senses, F.; Er, N.; Tekin, U.; Tuz, H.H.; Alkan, A.; Kocyigit, I.D.; Atil, F. Efficacy of platelet rich fibrin in the reduction of the pain and swelling after impacted third molar surgery: Randomized multicenter split-mouth clinical trial. Head Face Med. 2015, 11, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatakeyama, I.; Marukawa, E.; Takahashi, Y.; Omura, K. Effects of platelet-poor plasma, platelet-rich plasma, and platelet-rich fibrin on healing of extraction sockets with buccal dehiscence in dogs. Tissue Eng. Part A 2014, 20, 874–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.M.; Lee, C.U.; Son, J.S.; Oh, J.H.; Fang, Y.; Choi, B.H. Simultaneous sinus lift and implantation using platelet-rich fibrin as sole grafting material. J. Craniomaxillofac. Surg. 2014, 42, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.B.; Lee, J.T.; Hwang, S.; Choi, J.Y.; Rhyu, I.C.; Yeo, I.L. Leukocyte-and platelet-rich fibrin is an effective membrane for lateral ridge augmentation: An in vivo study using a canine model with surgically created defects. J. Periodontol. 2020, 91, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Simon, B.I.; Zatcoff, A.L.; Kong, J.J.; O’Connell, S.M. Clinical and histological comparison of extraction socket healing following the use of autologous platelet-rich fibrin matrix (PRFM) to ridge preservation procedures employing demineralized freeze dried bone allograft material and membrane. Open Dent. J. 2009, 3, 92–99. [Google Scholar] [CrossRef] [Green Version]
- To, M.; Su, C.Y.; Hidaka, K.; Okudera, T.; Matsuo, M. Effect of advanced platelet-rich fibrin on accelerating alveolar bone formation in dogs: A histological and immunofluorescence evaluation. Anat. Sci. Int. 2019, 94, 238–244. [Google Scholar] [CrossRef]
- Tambella, A.M.; Bartocetti, F.; Rossi, G.; Galosi, L.; Catone, G.; Falcone, A.; Vullo, C. Effects of Autologous Platelet-Rich Fibrin in Post-Extraction Alveolar Sockets: A Randomized, Controlled Split-Mouth Trial in Dogs with Spontaneous Periodontal Disease. Animals 2020, 10, 1343. [Google Scholar] [CrossRef]
- Kornsuthisopon, C.; Pirarat, N.; Osathanon, T.; Kalpravidh, C. Autologous platelet-rich fibrin stimulates canine periodontal regeneration. Sci. Rep. 2020, 10, 1850. [Google Scholar] [CrossRef] [Green Version]
- Abdelmagid, S.E.; Shaaban, A.M.M.; Ragaa, H.; Nagui, D. Comparison between the Use of Platelet Rich Fibrin with/and Without Biphasic Calcium Phosphate for Osseointegration around Implants (Experimental Study). Int. J. Sci. Res. 2015, 6, E1803–E1807. [Google Scholar]
- Mancini, L.; Tarallo, F.; Quinzi, V.; Fratini, A.; Mummolo, S.; Marchetti, E. Platelet-Rich Fibrin in Single and Multiple Coronally Advanced Flap for Type 1 Recession: An Updated Systematic Review and Meta-Analysis. Medicina 2021, 57, 144. [Google Scholar] [CrossRef]
- Panda, S.; Satpathy, A.; Chandra Das, A.; Kumar, M.; Mishra, L.; Gupta, S.; Srivastava, G.; Lukomska-Szymanska, M.; Taschieri, S.; Del Fabbro, M. Additive Effect of Platelet Rich Fibrin with Coronally Advanced Flap Procedure in Root Coverage of Miller’s Class I and II Recession Defects-A PRISMA Compliant Systematic Review and Meta-Analysis. Materials 2020, 13, 4314. [Google Scholar] [CrossRef]
- Panda, S.; Karanxha, L.; Goker, F.; Satpathy, A.; Taschieri, S.; Francetti, L.; Das, A.C.; Kumar, M.; Panda, S.; Fabbro, M.D. Autologous Platelet Concentrates in Treatment of Furcation Defects-A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2019, 20, 1347. [Google Scholar] [CrossRef] [Green Version]
- Thomazini-Santos, I.A.; Giannini, M.J.S.M.; Toscano, E.; Machado, P.E.D.; Lima, C.R.G.; Barraviera, B. The evaluation of clotting time in bovine thrombin, Reptilase®, and thrombin-like fraction of Crotalus durissus terrificus venom using bovine, equine, ovine, bubaline and human cryoprecipitates. J. Venom. Anim. Toxins 1998, 4, 120–136. [Google Scholar] [CrossRef]
- Davis, I.J.; Jones, A.W.; Creese, A.J.; Staunton, R.; Atwal, J.; Chapple, I.L.; Harris, S.; Grant, M.M. Longitudinal quantification of the gingival crevicular fluid proteome during progression from gingivitis to periodontitis in a canine model. J. Clin. Periodontol. 2016, 43, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Wiggs, R.B.; Lobprise, H.B. Veterinary Dentistry: Principles and Practice; Lippincott-Raven Publishers: New York, NY, USA, 1997; pp. 93–95. [Google Scholar]
- Loe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Fischman, S.L. Current status of indices of plaque. J. Clin. Periodontol. 1986, 13, 371–374. [Google Scholar] [CrossRef]
- Persson, R.E.; Tzannetou, S.; Feloutzis, A.G.; Brägger, U.; Persson, G.R.; Lang, N.P. Comparison between panoramic and intra-oral radiographs for the assessment of alveolar bone levels in a periodontal maintenance population. J. Clin. Periodontol. 2003, 30, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Balci Yuce, H.; Toker, H.; Goze, F. The histopathological and morphometric investigation of the effects of systemically administered boric acid on alveolar bone loss in ligature-induced periodontitis in diabetic rats. Acta Odontol. Scand. 2014, 72, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Takashiba, S.; Nagai, A.; Takigawa, M.; Myoukai, F.; Kurihara, H.; Murayama, Y. Assessment of interleukin-6 in the pathogenesis of periodontal disease. J. Periodontol. 1994, 65, 147–153. [Google Scholar] [CrossRef]
- Yücel, E.A.; Oral, O.; Olgaç, V.; Oral, C.K. Effects of fibrin glue on wound healing in oral cavity. J. Dent. 2003, 31, 569–575. [Google Scholar] [CrossRef]
- Dejyong, K.; Kaewamatawong, T.; Brikshavana, P.; Durongphongtorn, S. Efficacy of bubaline fibrin glue on full-thickness pinch and punch skin grafting in a pig. J. Biomater. Appl. 2017, 31, 1215–1224. [Google Scholar] [CrossRef]
- Rosamma Joseph, V.; Raghunath, A.; Sharma, N. Clinical effectiveness of autologous platelet rich fibrin in the management of infrabony periodontal defects. Singap. Dent. J. 2012, 33, 5–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandradas, N.D.; Ravindra, S.; Rangaraju, V.M.; Jain, S.; Dasappa, S. Efficacy of platelet rich fibrin in the treatment of human intrabony defects with or without bone graft: A randomized controlled trial. J. Int. Soc. Prev. Community Dent. 2016, 6 (Suppl. 2), S153–S159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lekovic, V.; Milinkovic, I.; Aleksic, Z.; Jankovic, S.; Stankovic, P.; Kenney, E.B.; Camargo, P.M. Platelet-rich fibrin and bovine porous bone mineral vs. platelet-rich fibrin in the treatment of intrabony periodontal defects. J. Periodontal Res. 2012, 47, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; Huang, Y.M.; Chen, C.H.; Lin, F.H.; Yeh, Y.Y.; Bai, M.Y. Cytokine and Growth Factor Delivery from Implanted Platelet-Rich Fibrin Enhances Rabbit Achilles Tendon Healing. Int. J. Mol. Sci. 2020, 21, 3221. [Google Scholar] [CrossRef]
- Wu, C.L.; Lee, S.S.; Tsai, C.H.; Lu, K.H.; Zhao, J.H.; Chang, Y.C. Platelet-rich fibrin increases cell attachment, proliferation and collagen-related protein expression of human osteoblasts. Aust. Dent. J. 2012, 57, 207–212. [Google Scholar] [CrossRef]
- Alishahi, M.K.; Mofidpoor, H.; Alishahi, M.A.K. Histopathological evaluation of the effect of platelet-rich fibrin on canine cutaneous incisional wound healing. World Appl. Sci. J. 2014, 31, 676–680. [Google Scholar]
- Su, C.Y.; Kuo, Y.P.; Tseng, Y.H.; Su, C.H.; Burnouf, T. In vitro release of growth factors from platelet-rich fibrin (PRF): A proposal to optimize the clinical applications of PRF. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, 56–61. [Google Scholar] [CrossRef]
- Preeja, C.; Arun, S. Platelet-rich fibrin: Its role in periodontal regeneration. Saudi J. Dent. Res. 2014, 5, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.H.; Jeon, S.H.; Park, J.Y.; Chung, J.H.; Choung, Y.H.; Choung, H.W.; Kim, E.S.; Choung, P.H. Platelet-rich fibrin is a Bioscaffold and reservoir of growth factors for tissue regeneration. Tissue Eng. Part A 2011, 17, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; de Peppo, G.M.; Doglioli, P.; Sammartino, G. Slow release of growth factors and thrombospondin-1 in Choukroun’s platelet-rich fibrin (PRF): A gold standard to achieve for all surgical platelet concentrates technologies. Growth Factors 2009, 27, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Barrientos, S.; Stojadinovic, O.; Golinko, M.S.; Brem, H.; Tomic-Canic, M. Growth factors and cytokines in wound healing. Wound Repair. Regen. 2008, 16, 585–601. [Google Scholar] [CrossRef] [PubMed]
- Tavelli, L.; Ravida, A.; Barootchi, S.; Chambrone, L.; Giannobile, W.V. Recombinant Human Platelet-Derived Growth Factor: A Systematic Review of Clinical Findings in Oral Regenerative Procedures. JDR Clin. Trans. Res. 2021, 6, 161–173. [Google Scholar] [CrossRef]
- Mihaylova, Z.; Tsikandelova, R.; Sanimirov, P.; Gateva, N.; Mitev, V.; Ishkitiev, N. Role of PDGF-BB in proliferation, differentiation and maintaining stem cell properties of PDL cells in vitro. Arch. Oral Biol. 2018, 85, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chowdhary, K.Y.; George, J.P.; Gowda, P.; Rao, J.A. Human periodontal ligament fibroblast response to rhPDGF-BB application on periodontally diseased root surfaces-in vitro. Growth Factors 2013, 31, 130–138. [Google Scholar] [CrossRef]
- Banyatworakul, P.; Osathanon, T.; Chumprasert, S.; Pavasant, P.; Pirarat, N. Responses of canine periodontal ligament cells to bubaline blood derived platelet rich fibrin in vitro. Sci. Rep. 2021, 11, 11409. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plaque Index | |
| score 0 | no plaque |
| score 1 | less than 25% plaque accumulation on the free gingival margin and the surface of the tooth |
| score 2 | 25–50% plaque accumulation on the surface of the tooth and deposits in the periodontal pocket |
| score 3 | more than 50% plaque accumulation on the gingival margin and abundant plaque in the periodontal pocket |
| Gingival Index | |
| score 0 | no inflammation and healthy periodontium |
| score 1 | mild inflammation with slight change in the color of the gingiva (erythyma), rounding of the gingival edges, and no bleeding on probing |
| score 2 | moderate inflammation with a significant change in the color (redness), rounding of the gingival edges, as well as bleeding on probing |
| score 3 | severe inflammation with a significant change in the color (redness), the consistency (hypertrophy), and the density of the gingiva (ulceration), as well as spontaneous bleeding |
| Inflammatory Response Score | |
|---|---|
| Score 0 | no inflammatory cells |
| Score 1 | inflammatory cells found 1–35% of the field |
| Score 2 | inflammatory cells found in 36–70% of the fields |
| Score 3 | inflammatory cells found over 70% of the fields |
| Healing Response Score | |
| Score 0 | no fibroblasts, fibrocytes, or connective tissues |
| Score 1 | fibroblasts, fibrocytes, and connective tissues found 1–35% of the fields |
| Score 2 | fibroblasts, fibrocytes, and connective tissues found 36–70% of the fields |
| Score 3 | fibroblasts, fibrocytes, and connective tissues found over 70% of the fields |
| Primer | Accession Number | Forward Primer | Reverse Primer |
|---|---|---|---|
| ACTB | NM_001195845.2 | 5′-AGCTCCACGGAGAAGAACTG-3′ | 5′-GGCTCCAAATGTAGGGGCAG-3′ |
| TNFA | NM_001003244 | 5′-TCTCGAACCCCAAGTGACAAG-3′ | 5′-CAACCCATCTGACGGCACTA-3′ |
| PDGFB | NM_001003383.1 | 5′-ACCGGAAGTTCAAGCACACA-3′ | 5′-TGCCCTCAATCTCCTCCAGA-3′ |
| TGFB1 | NM_001003309.1 | 5′-GGACTTCGAGCAGGAGATGG-3′ | 5′-TTCCATGCCCAGGAAGGAAG-3′ |
| VEGFA | NM_001003175.2 | 5′-CCGGTATAAACCCTGGAGCG-3′ | 5′-GCAACGCGAGTCTGTGTTTT-3′ |
| IL1B | NM_001037971 | 5′-CAAGTCTCCCACCAGCTCTGTA-3′ | 5′-GGGCTTCTTCAGCTTCTCCAA-3′ |
| COL1A1 | AF153062.1 | 5′-GGCAGGAGGGTTCAGCTAAG-3′ | 5′-GCAACAAAGTCCGCGTATCC-3′ |
| COL3A1 | HM775210.1 | 5′-TTCCTGGGAGAAATGGCGAC-3′ | 5′-AGGACCAGTAGGGCAGGATT-3′ |
| TIMP1 | AF077817_1 | 5′-GATGTTCAAGGGTTTCAGCG-3′ | 5′-TGTCACTCTGCAGTTGCAG-3′ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banyatworakul, P.; Osathanon, T.; Kalpravidh, C.; Pavasant, P.; Pirarat, N. Evaluation of the Use of Platelet-Rich Fibrin Xenologous Membranes Derived from Bubaline Blood in Canine Periodontal Defects. Vet. Sci. 2021, 8, 210. https://doi.org/10.3390/vetsci8100210
Banyatworakul P, Osathanon T, Kalpravidh C, Pavasant P, Pirarat N. Evaluation of the Use of Platelet-Rich Fibrin Xenologous Membranes Derived from Bubaline Blood in Canine Periodontal Defects. Veterinary Sciences. 2021; 8(10):210. https://doi.org/10.3390/vetsci8100210
Chicago/Turabian StyleBanyatworakul, Poranee, Thanaphum Osathanon, Chanin Kalpravidh, Prasit Pavasant, and Nopadon Pirarat. 2021. "Evaluation of the Use of Platelet-Rich Fibrin Xenologous Membranes Derived from Bubaline Blood in Canine Periodontal Defects" Veterinary Sciences 8, no. 10: 210. https://doi.org/10.3390/vetsci8100210
APA StyleBanyatworakul, P., Osathanon, T., Kalpravidh, C., Pavasant, P., & Pirarat, N. (2021). Evaluation of the Use of Platelet-Rich Fibrin Xenologous Membranes Derived from Bubaline Blood in Canine Periodontal Defects. Veterinary Sciences, 8(10), 210. https://doi.org/10.3390/vetsci8100210