Effect of Different Doses of Atipamezole on Reversal of Medetomidine-Induced Tear-Flow Decrease in Rats

 , ,
, , {kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Drug Treatment
2.3. Measurement
2.4. Statistical Analysis
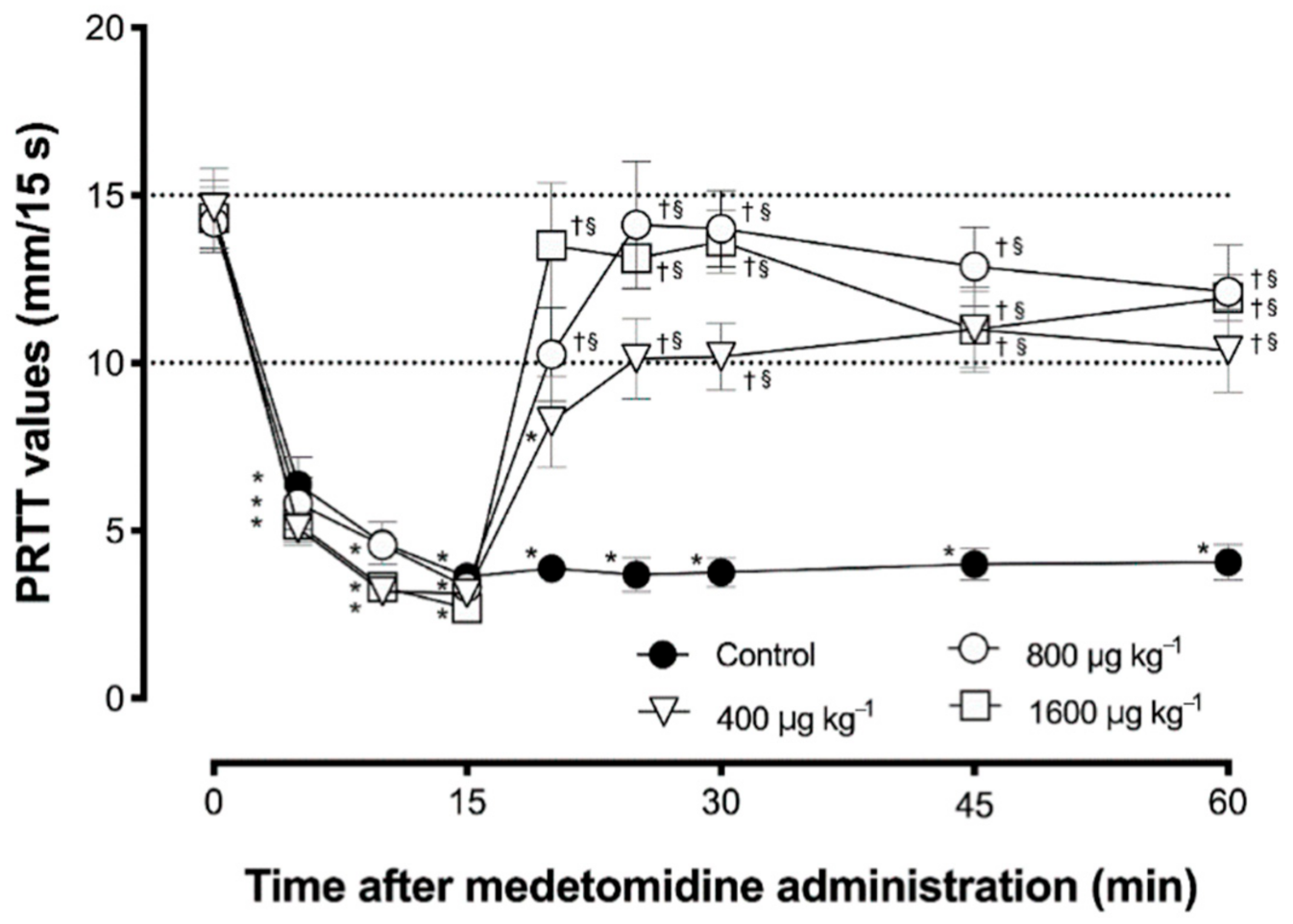
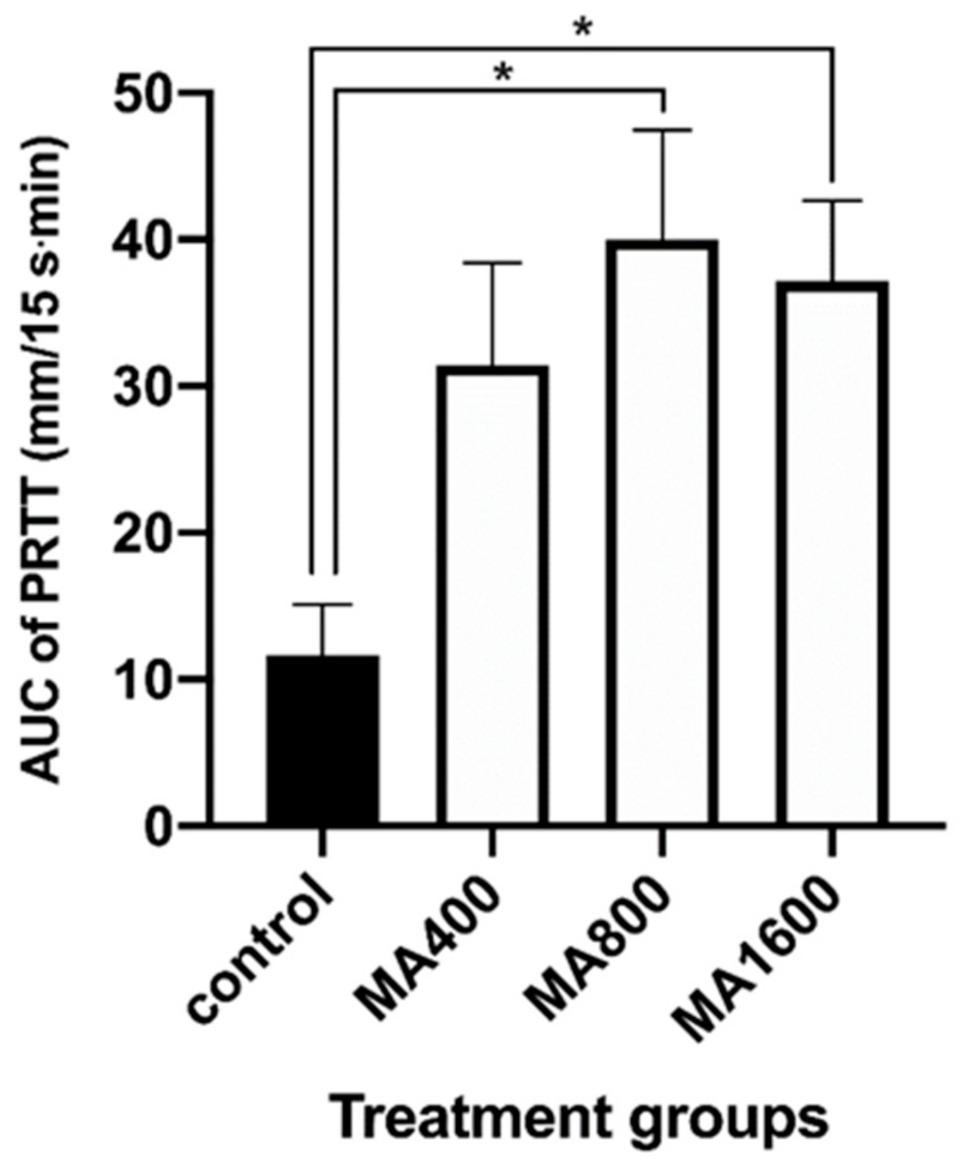
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sinclair, M.D. A review of the physiological effects of alpha2-agonists related to the clinical use of medetomidine in small animal practice. Can. Vet. J. 2003, 44, 885–897. [Google Scholar] [PubMed]
- Bryant, C.E.; England, G.C.; Clarke, K.W. Comparison of the sedative effects of medetomidine and xylazine in horses. Vet. Rec. 1991, 129, 421–423. [Google Scholar] [CrossRef] [PubMed]
- Pollock, C.G.; Schumacher, J.; Orosz, S.E.; Ramsay, E.C. Sedative Effects of Medetomidine in Pigeons (Columba livia). J. Avian Med. Surg. 2001, 15, 95–100. [Google Scholar] [CrossRef]
- Sakaguchi, M.; Nishimura, R.; Sasaki, N.; Ishiguro, T.; Tamura, H.; Takeuchi, A. Sedative effects of medetomidine in pigs. J. Vet. Med. Sci. 1992, 54, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Hikasa, Y. Neurohormonal and metabolic effects of medetomidine compared with xylazine in healthy cats. Can. J. Vet. Res. 2008, 72, 278–286. [Google Scholar]
- Ambrisko, T.D.; Hikasa, Y. Neurohormonal and metabolic effects of medetomidine compared with xylazine in beagle dogs. Can. J. Vet. Res. 2002, 66, 42–49. [Google Scholar]
- Vaisanen, M.; Raekallio, M.; Kuusela, E.; Huttunen, P.; Leppaluoto, J.; Kirves, P.; Vainio, O. Evaluation of the perioperative stress response in dogs administered medetomidine or acepromazine as part of the preanesthetic medication. Am. J. Vet. Res. 2002, 63, 969–975. [Google Scholar] [CrossRef]
- Lamont, L.; Burton, S.; Caines, D.; Masaoud, E.; Troncy, E. Effects of 2 different medetomidine infusion rates on selected neurohormonal and metabolic parameters in dogs. Can. J. Vet. Res. 2012, 76, 143–148. [Google Scholar]
- Sanchez, R.F.; Mellor, D.; Mould, J. Effects of medetomidine and medetomidine-butorphanol combination on Schirmer tear test 1 readings in dogs. Vet. Ophthalmol. 2006, 9, 33–37. [Google Scholar] [CrossRef]
- Abdelhakiem, M.A.H.; Elmeligy, E.; Al-lethie, A. Effect of Xylazine HCl and/or Ketamine HCl on the Tear Production in Clinically Healthy Dogs. Adv. Anim. Vet. Sci. 2019, 7, 1015–1020. [Google Scholar] [CrossRef]
- Kanda, T.; Ishihara, S.; Oka, M.; Sako, K.; Sato, Y.; Maeta, N.; Tamura, K.; Furumoto, K.; Furukawa, T. Temporal effects of intramuscular administration of medetomidine hydrochloride or xylazine hydrochloride to healthy dogs on tear flow measured by use of a schirmer tear test I. Am. J. Vet. Res. 2016, 77, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.S.; Malmasi, A.; Bokaie, S. Effect of acepromazine or xylazine on tear production as measured by Schirmer tear test in normal cats. Vet. Ophthalmol. 2010, 13, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Selk Ghaffari, M.; Brooks, D.E.; Sabzevari, A.; Ghamsari, S.M.; Mansoor Lakooraj, H.; Shad, H. Effects of Intravenous Detomidine on Schirmer Tear Test Results in Clinically Normal Horses. J. Equine Vet. Sci. 2017, 55, 97–99. [Google Scholar] [CrossRef]
- Leonardi, F.; Costa, G.L.; Dubau, M.; Sabbioni, A.; Simonazzi, B.; Angelone, M. Effects of intravenous romifidine, detomidine, detomidine combined with butorphanol, and xylazine on tear production in horses. Equine Vet. Educ. 2020, 32, 53–57. [Google Scholar] [CrossRef]
- Kanda, T.; Mizoguchi, Y.; Furumoto, K.; Shimizu, Y.; Maeta, N.; Furukawa, T. Effect of Intramuscular Medetomidine Administration on Tear Flow in Rats. Vet. Sci. 2020, 7, 42. [Google Scholar] [CrossRef]
- Weisse, I.; Hoefke, W.; Greenberg, S.; Gaida, W.; Stötzer, H.; Kreuzer, H. Ophthalmological and pharmacological studies after administration of clonidine in rats. Arch. Toxicol. 1978, 41, 89–98. [Google Scholar] [CrossRef]
- Kanda, T.; Kajiyama, A.; Morimitsu, W.; Nishino, Y.; Oishi, Y.; Shimizu, Y.; Maeta, N.; Furumoto, K.; Itoh, Y.; Furukawa, T. Effect of medetomidine on tear flow measured by Schirmer tear test I in normal pigs. J. Vet. Med. Sci. 2019, 81, 538–540. [Google Scholar] [CrossRef]
- Kanda, T.; Shimizu, Y.; Hanazono, C.; Maki, S.; Maeta, N.; Itoi, T.; Furumoto, K.; Okamura, Y.; Itoh, Y.; Furukawa, T. Effect of intramuscular administration of medetomidine and xylazine on tear flow measured by the Schirmer tear test I in healthy cats. J. Feline Med. Surg. 2019, 21, 788–792. [Google Scholar] [CrossRef]
- Moore, C.P. Disease and surgery of the lacrimal secretory system. In Veterinary Ophthalmology; Gelatt, K.N., Ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1999; pp. 583–607. [Google Scholar]
- Meng, I.D.; Barton, S.T.; Mecum, N.E.; Kurose, M. Corneal Sensitivity Following Lacrimal Gland Excision in the Rat. Investig. Opthalmol. Vis. Sci. 2015, 56, 3347. [Google Scholar] [CrossRef]
- Peche, N.; Köstlin, R.; Reese, S.; Pieper, K. Postanaesthetic tear production and ocular irritation in cats. Tierarztl Prax. Ausg. K Kleintiere Heimtiere 2015, 43, 75–82. [Google Scholar]
- Dodam, J.R.; Branson, K.R.; Martin, D.D. Effects of intramuscular sedative and opioid combinations on tear production in dogs. Vet. Ophthalmol. 1998, 1, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, F.; Costa, G.L.; Stagnoli, A.; Zubin, E.; Boschi, P.; Sabbioni, A.; Simonazzi, B. The effect of intramuscular dexmedetomidine-butorphanol combination on tear production in dogs. Can. Vet. J. 2019, 60, 55–59. [Google Scholar] [PubMed]
- Virtanen, R. Pharmacological profiles of medetomidine and its antagonist, atipamezole. Acta Vet. Scand. Suppl. 1989, 85, 29–37. [Google Scholar] [PubMed]
- Nakamura, S.; Kimura, Y.; Mori, D.; Imada, T.; Izuta, Y.; Shibuya, M.; Sakaguchi, H.; Oonishi, E.; Okada, N.; Matsumoto, K.; et al. Restoration of Tear Secretion in a Murine Dry Eye Model by Oral Administration of Palmitoleic Acid. Nutrients 2017, 9, 364. [Google Scholar] [CrossRef]
- Hegarty, D.M.; David, L.L.; Aicher, S.A. Lacrimal Gland Denervation Alters Tear Protein Composition and Impairs Ipsilateral Eye Closures and Corneal Nociception. Investig. Opthalmol. Vis. Sci. 2018, 59, 5217–5224. [Google Scholar] [CrossRef]
- Vähä-Vahe, A.T. The clinical effectiveness of atipamezole as a medetomidine antagonist in the dog. J. Vet. Pharmacol. Ther. 1990, 13, 198–205. [Google Scholar] [CrossRef]
- Vainio, O.; Vähä-Vahe, T. Reversal of medetomidine sedation by atipamezole in dogs. J. Vet. Pharmacol. Ther. 1990, 13, 15–22. [Google Scholar] [CrossRef]
- Hu, C.; Flecknell, P.A.; Liles, J.H. Fentanyl and medetomidine anaesthesia in the rat and its reversal using atipamazole and either nalbuphine or butorphanol. Lab. Anim. 1992, 26, 15–22. [Google Scholar] [CrossRef]
- Jang, H.S.; Choi, H.S.; Lee, S.H.; Jang, K.H.; Lee, M.-G. Evaluation of the anaesthetic effects of medetomidine and ketamine in rats and their reversal with atipamezole. Vet. Anaesth. Analg. 2009, 36, 319–327. [Google Scholar] [CrossRef]
- Hedenqvist, P.; Roughan, J.V.; Flecknell, P.A. Sufentanil and medetomidine anaesthesia in the rat and its reversal with atipamezole and butorphanol. Lab. Anim. 2000, 34, 244–251. [Google Scholar] [CrossRef]
- Nishimura, R.; Kim, H.; Matsunaga, S.; Hayashi, K.; Sakai, N.; Tamura, H.; Takeuchi, A. Antagonistic Effects of Atipamezole and Flumazenil on Medetomidine-Midazolam Induced Sedation in Laboratory Pigs. J. Vet. Med. Sci. 1993, 55, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Yonezawa, K.; Izumisawa, Y.; Kotani, T. Antagonistic Effects of Atipamezole on Medetomidine-Induced Sedation in Horses. J. Vet. Med. Sci. 1996, 58, 1049–1052. [Google Scholar] [CrossRef] [PubMed]
- Pertovaara, A.; Kauppila, T.; Tukeva, T. The effect of medetomidine, an alpha 2-adrenoceptor agonist, in various pain tests. Eur. J. Pharmacol. 1990, 179, 323–328. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanda, T.; Gotoh, M.; Makino, A.; Furumoto, K.; Shimizu, Y.; Itoi, T.; Maeta, N.; Furukawa, T. Effect of Different Doses of Atipamezole on Reversal of Medetomidine-Induced Tear-Flow Decrease in Rats. Vet. Sci. 2020, 7, 197. https://doi.org/10.3390/vetsci7040197
Kanda T, Gotoh M, Makino A, Furumoto K, Shimizu Y, Itoi T, Maeta N, Furukawa T. Effect of Different Doses of Atipamezole on Reversal of Medetomidine-Induced Tear-Flow Decrease in Rats. Veterinary Sciences. 2020; 7(4):197. https://doi.org/10.3390/vetsci7040197
Chicago/Turabian StyleKanda, Teppei, Manami Gotoh, Ayumi Makino, Kayo Furumoto, Yuki Shimizu, Takamasa Itoi, Noritaka Maeta, and Toshinori Furukawa. 2020. "Effect of Different Doses of Atipamezole on Reversal of Medetomidine-Induced Tear-Flow Decrease in Rats" Veterinary Sciences 7, no. 4: 197. https://doi.org/10.3390/vetsci7040197
APA StyleKanda, T., Gotoh, M., Makino, A., Furumoto, K., Shimizu, Y., Itoi, T., Maeta, N., & Furukawa, T. (2020). Effect of Different Doses of Atipamezole on Reversal of Medetomidine-Induced Tear-Flow Decrease in Rats. Veterinary Sciences, 7(4), 197. https://doi.org/10.3390/vetsci7040197