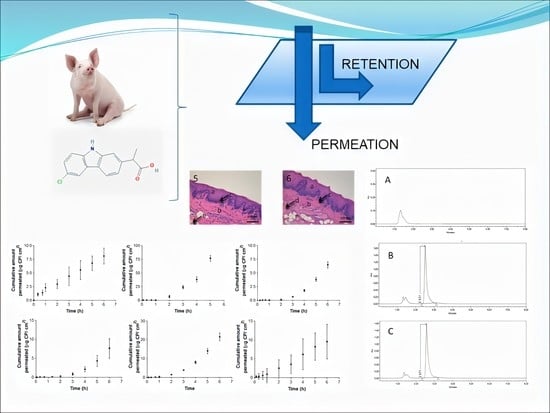
Carprofen Permeation Test through Porcine Ex Vivo Mucous Membranes and Ophthalmic Tissues for Tolerability Assessments: Validation and Histological Study

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
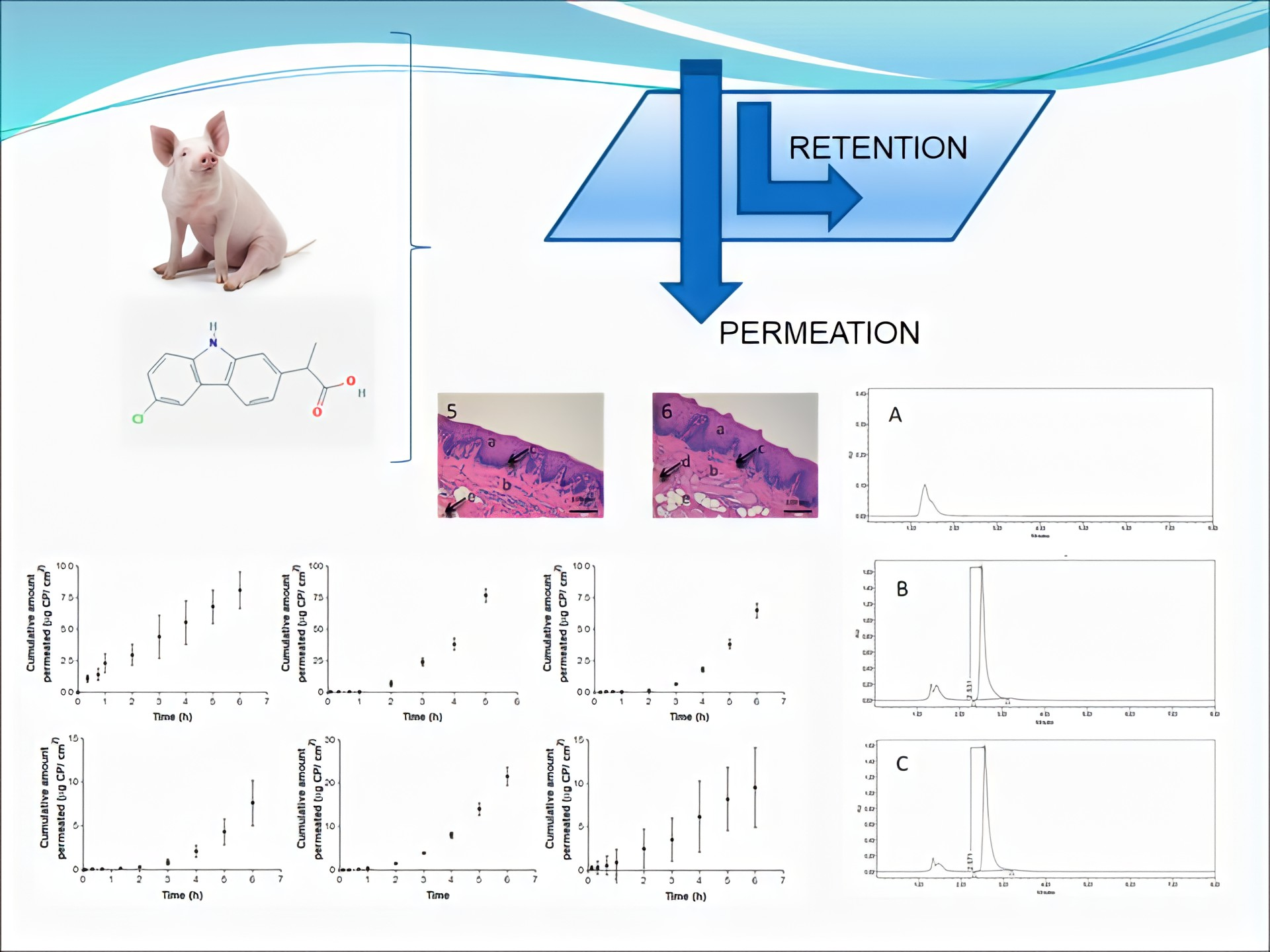
2.2. Biological Materials
2.3. Buffers and Solutions
2.4. Calibration Curve Standards (CCS), Quality Control Standards (QCS) and Fortified Samples (FS)
2.5. Carprofen Solubility
2.6. HPLC-UV
2.7. Analytical Method Validation
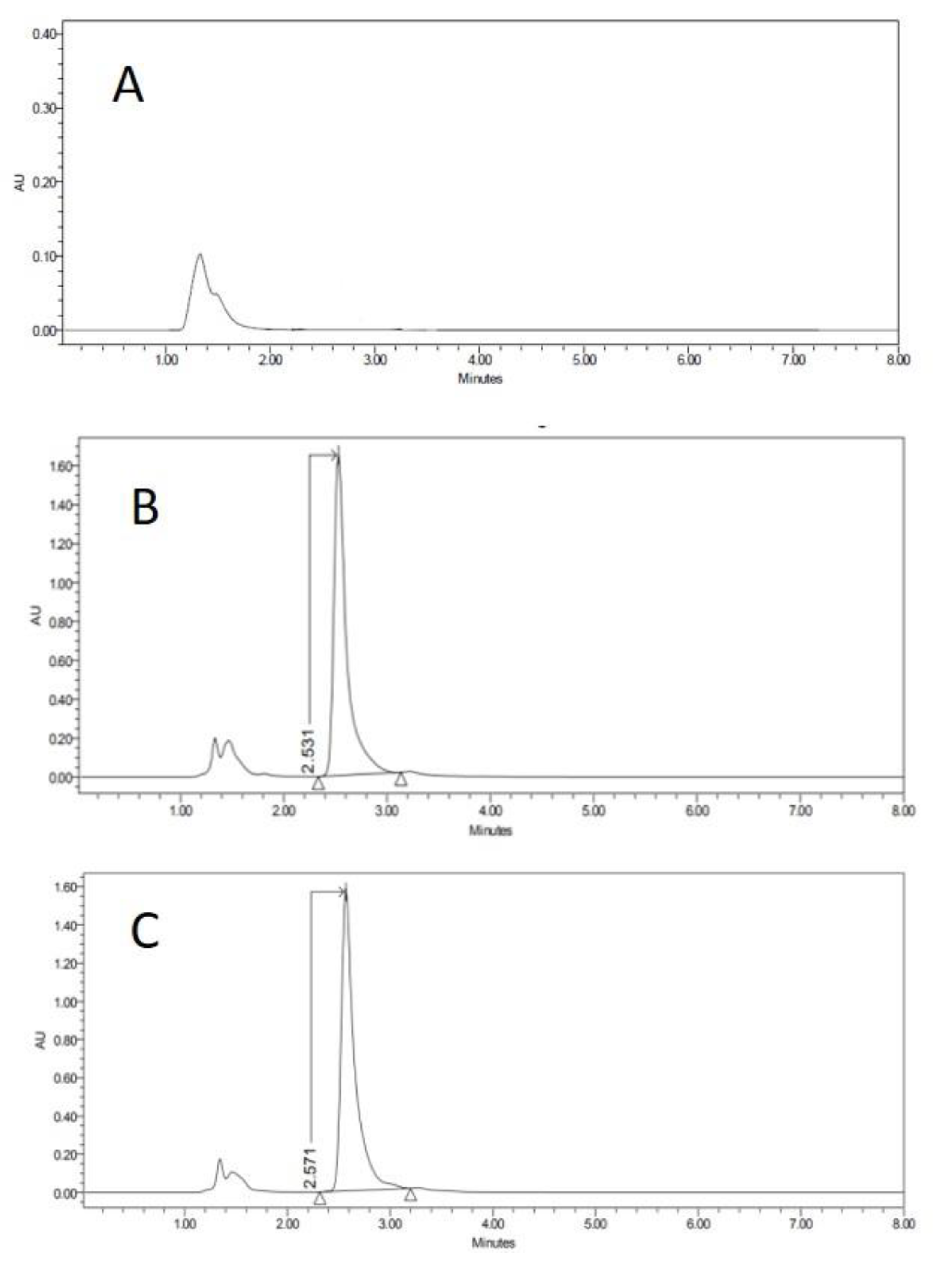
2.7.1. Specificity–Selectivity
2.7.2. Linearity and Range
2.7.3. Determination Limits
2.7.4. Accuracy and Precision
2.7.5. Stability of Standards
2.8. Applicability of the Method
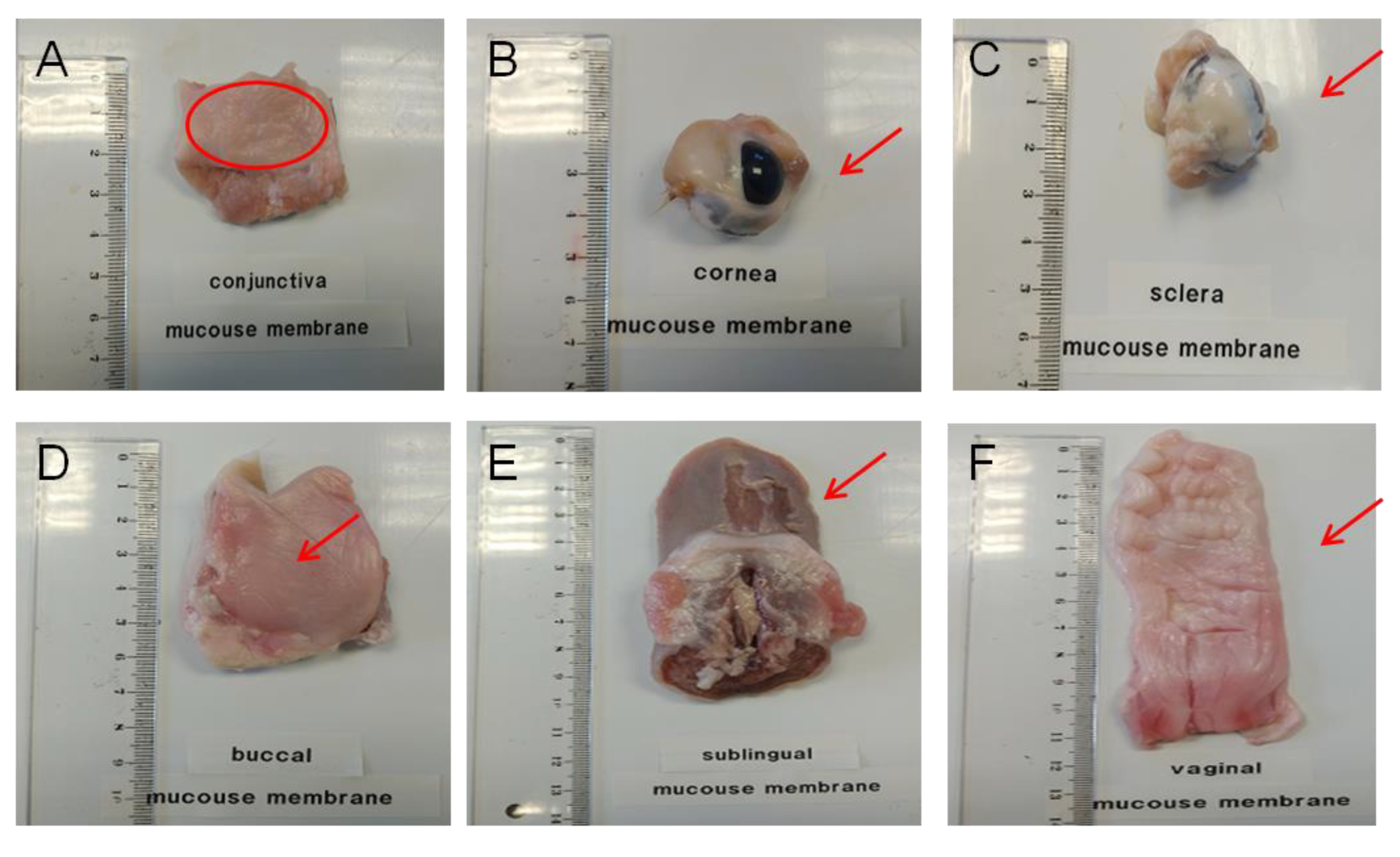
2.8.1. Permeation Test with Diffusion Cells
2.8.2. Recovery from Porcine Mucous Membranes or Ophthalmic Tissues
2.8.3. Drug Retention inside the Permeation Membrane
2.8.4. Transmembrane Flux under Sink Conditions
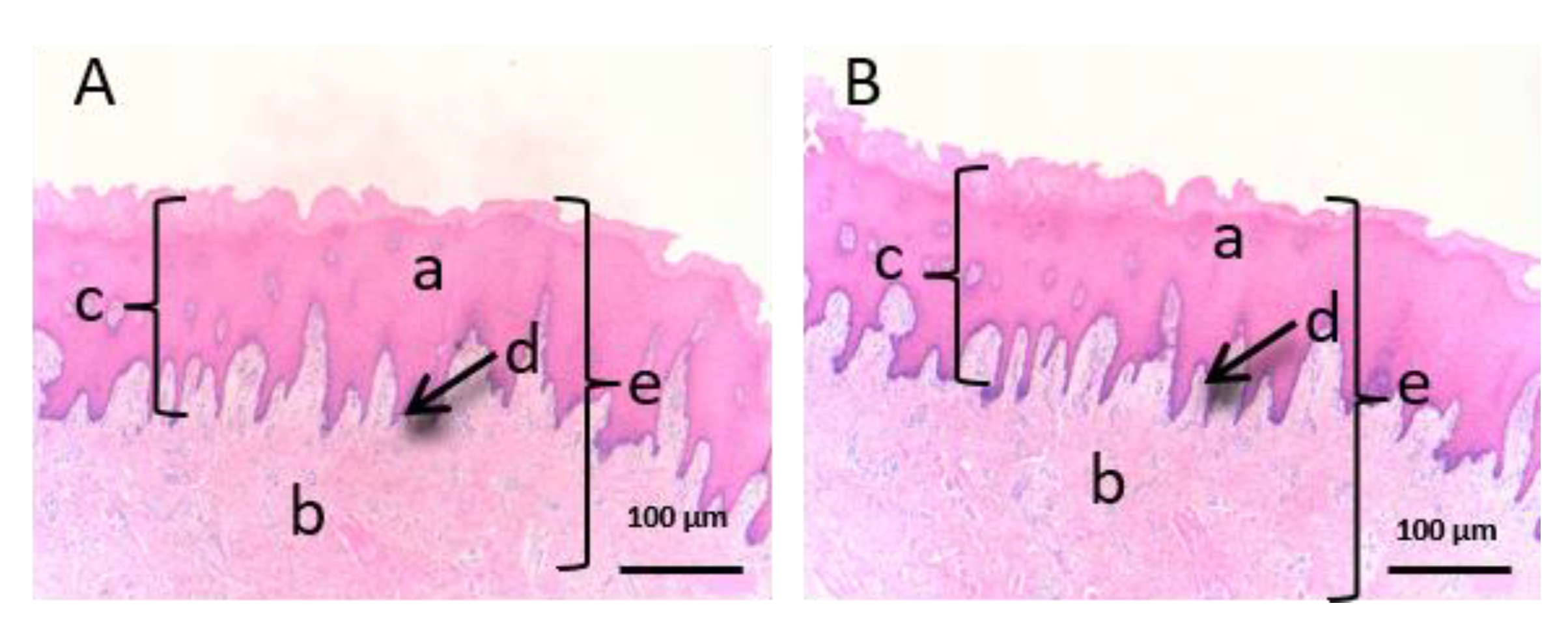
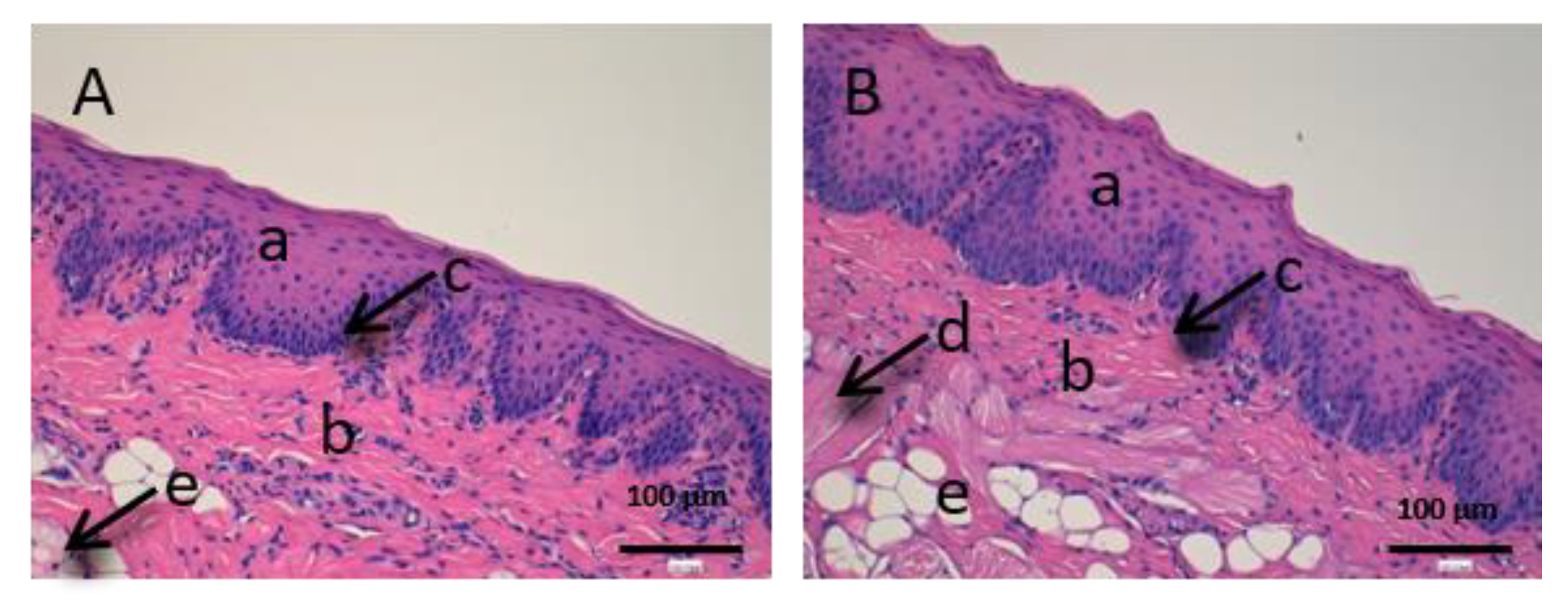
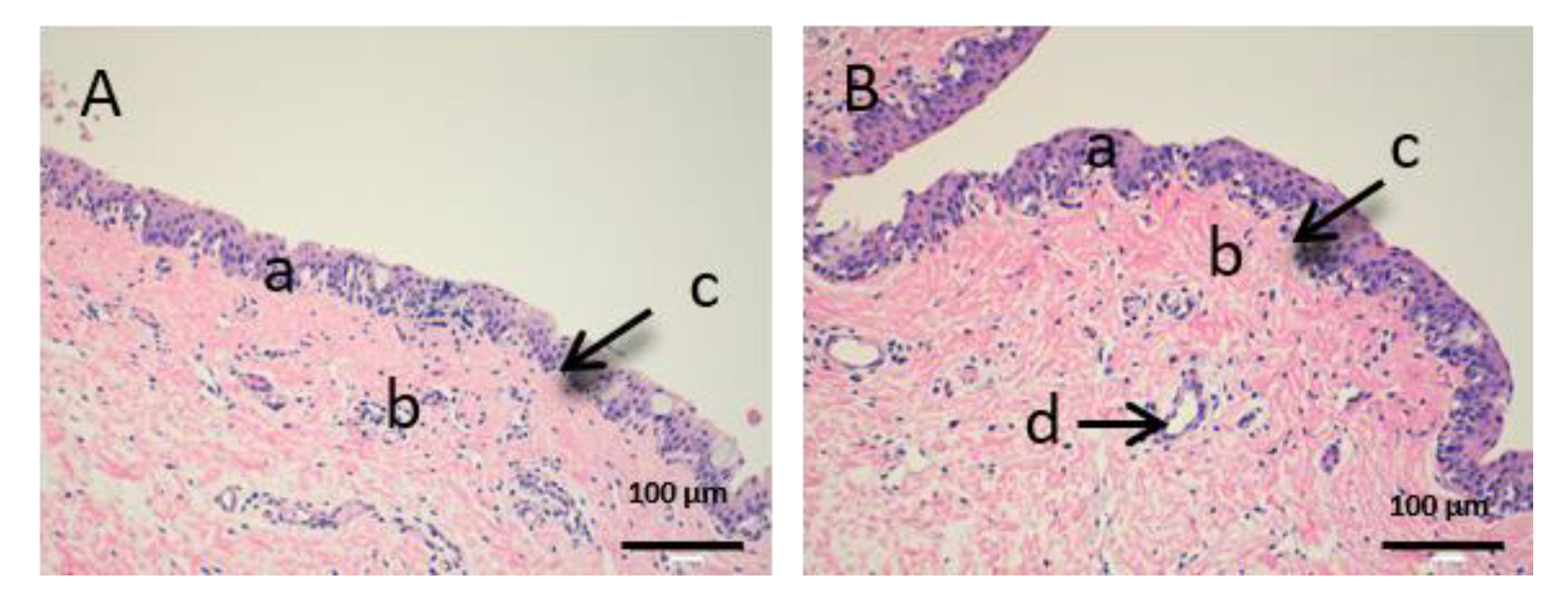
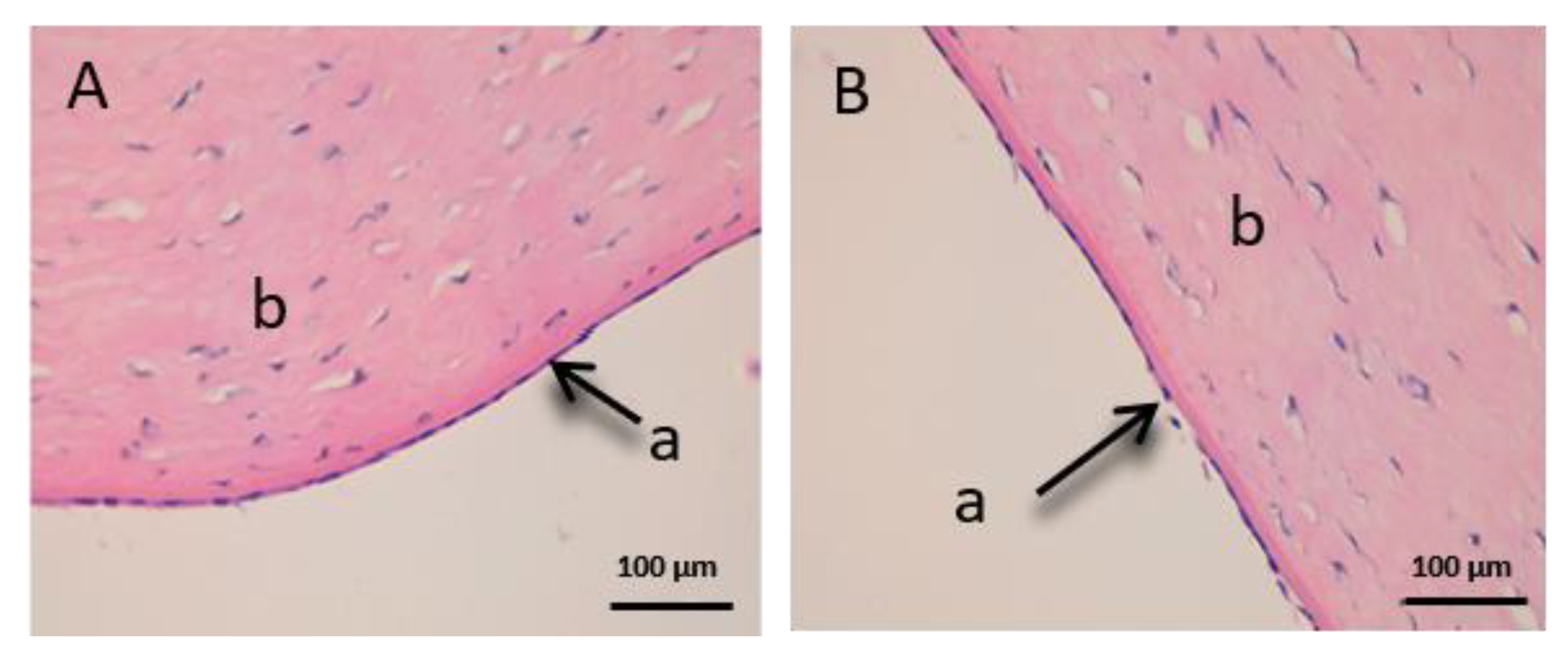
2.8.5. Histological Integrity of the Permeation Membranes
3. Results
3.1. Analytical Method Validation
3.2. Method Applicability
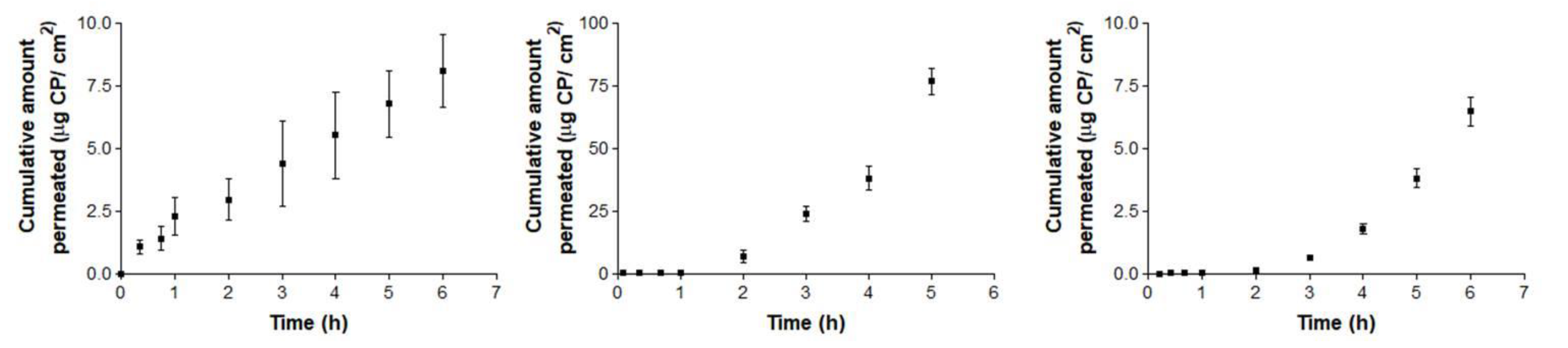
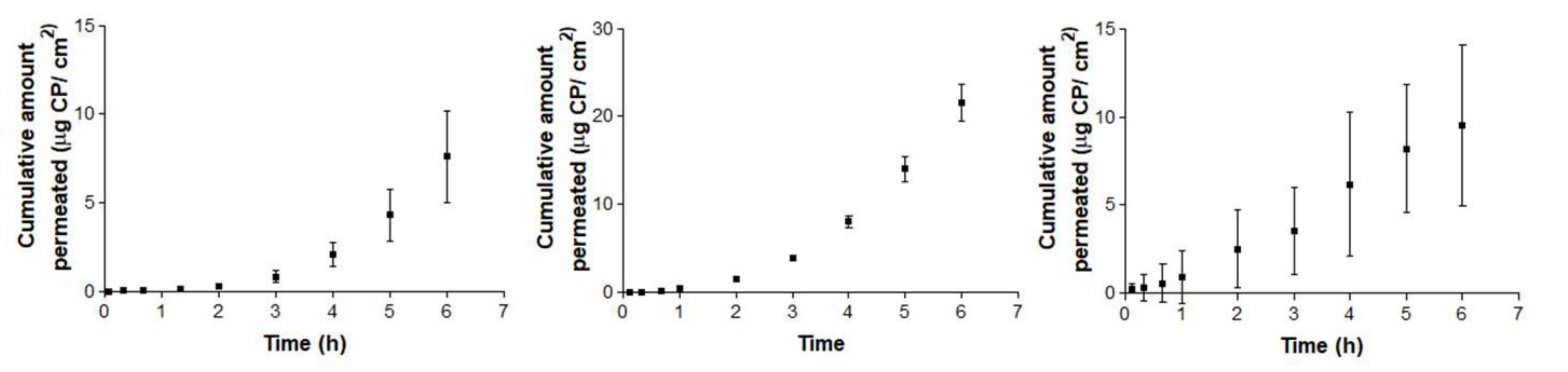
3.2.1. Permeation Experiment
3.2.2. Drug Recovery and Retention in Membranes
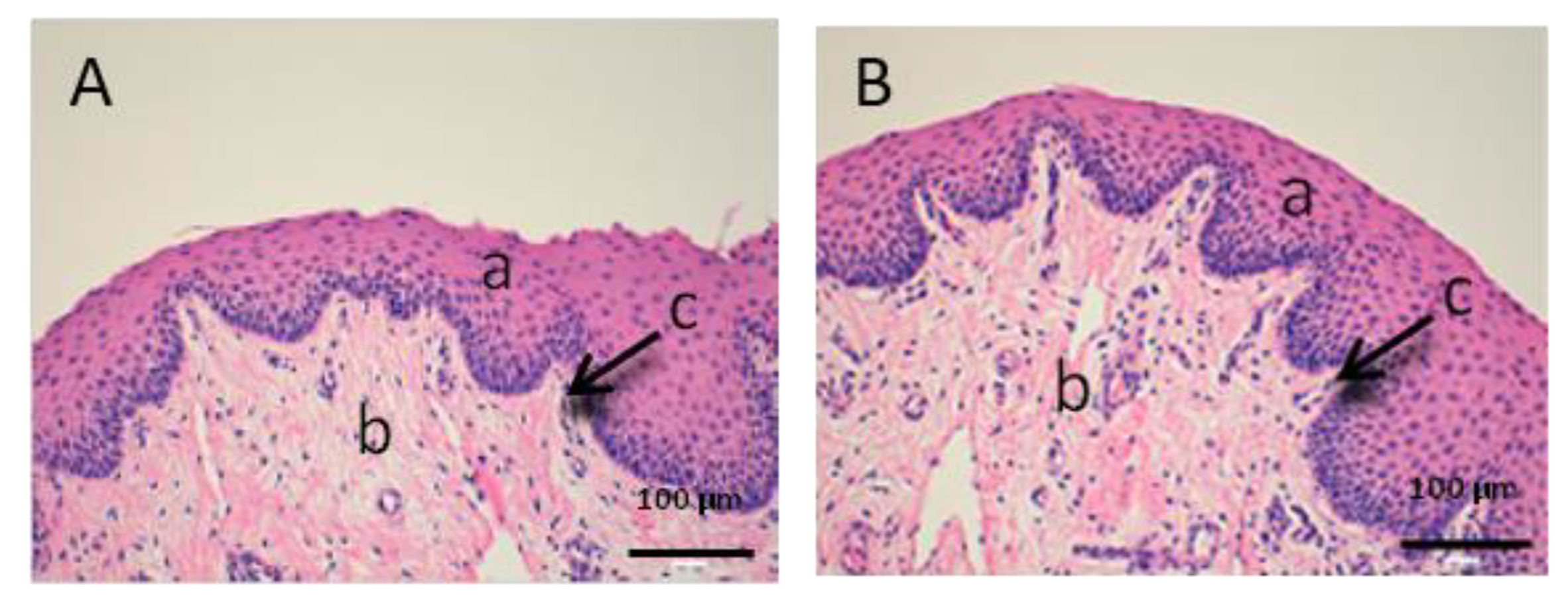
3.2.3. Histological Integrity of the Permeation Membranes
4. Discussion
4.1. Analytical Method Validation
4.2. Method Applicability
4.2.1. Permeation Experiments
4.2.2. Drug Recovery and Drug Retention in Membranes
4.2.3. Histological Integrity of the Permeation Membranes
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kujubu, D.A.; Fletcher, B.S.; Varnum, B.C.; Lim, R.W.; Herschman, H.R. TIS10, a phorbol ester tumor promoter inducible mRNA from Swiss 3T3 cells, encodes a novel prostaglandin synthase/cyclooxygenase homologue. J. Biol. Chem. 1991, 266, 12866–12872. [Google Scholar]
- Kerr, A.C.; Muller, F.; Ferguson, J.; Dawe, R.S. Occupational carprofen photoallergic contact dermatitis. Br. J. Dermatol. 2008, 159, 1303. [Google Scholar] [CrossRef] [PubMed]
- Sanderson, R.O.; Beata, C.; Flipo, R.M.; Genevois, J.P.; Macias, C.; Tacke, S.; Vezzoni, A.; Innes, J.F. Systematic review of the management of canine osteoarthritis. Vet. Rec. 2009, 164, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Vasseur, P.B.; Johnson, A.L.; Budsberg, S.C.; Lincoln, J.D.; Toombs, J.P.; Whitehair, J.G.; Lentz, E.L. Randomized, controlled trial of the efficacy of carprofen, a nonsteroidal anti-inflammatory drug, in the treatment of osteoarthritis in dogs. J. Am. Vet. Med. A 1995, 206, 807–811. [Google Scholar]
- Vangroenweghe, F.; Duchateau, L.; Boutet, P.; Lekeux, P.; Rainard, P.; Paape, M.J.; Burvenich, C. Effect of carprofen treatment following experimentally induced Escherichia coli mastitis in primiparous cows. J. Dairy Sci. 2005, 88, 2361–2376. [Google Scholar] [CrossRef]
- Bergmann, H.M.; Nolte, I.; Kramer, S. Comparison of analgesic effificacy of preoperative or postoperative carprofen with or without preincisional mepivacaine epidural anesthesia in canine pelvic or femoral fracture repair. Vet. Surg. 2007, 36, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Sidler, M.; Fouché, N.; Meth, I.; Von Hahn, F.; Von Rechenberg, B.; Kronen, P.W. Transcutaneous treatment with vetdrop sustains the adjacent cartilage in a microfracturing joint defect model in sheep. Open Orthop. J. 2013, 7, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Elitok, B.; Elitok, Ö.M. Clinical efficacy of carprofen as an adjunct to the antibacterial treatment of bovine respiratory disease. J. Vet. Pharmacol. Therap. 2004, 27, 317–320. [Google Scholar] [CrossRef]
- Lockwood, P.W.; Johnson, J.C.; Katz, T.L. Clinical efficacy of flunixin, carprofen and ketoprofen as adjuncts to the antibacterial treatment of bovine respiratory disease. Vet. Rec. 2003, 152, 392–394. [Google Scholar] [CrossRef]
- Armstrong, S.; Tricklebank, S.; Lake, A.; Frean, S.; Lees, P. Pharmacokinetics of carprofen enantiomers in equine plasma and synovial fluid—A comparison with ketoprofen. J. Vet. Pharmacol. Therap. 1999, 22, 196–201. [Google Scholar] [CrossRef]
- Lees, P.; Landoni, M.F.; Giraudel, J.; Toutain, P.L. Pharmacodynamics and pharmacokinetics of nonsteroidal anti-inflammatory drugs in species of veterinary interest. J. Vet. Pharmacol. Therap. 2004, 27, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Lascelles BD, X.; Cripps, P.J.; Jones, A.; Waterman-Pearson, A.E. Efficacy and kinetics of carprofen, administered preoperatively or postoperatively, for the prevention of pain in dogs undergoing ovariohysterectomy. Vet. Surg. 1998, 27, 568–582. [Google Scholar] [CrossRef] [PubMed]
- Grisneaux, E.; Pibarot, P.; Dupuis, J.; Biais, D. Comparison of ketoprofen and carprofen administered prior to orthopedic surgery for control of postoperative pain in dogs. J. Am. Vet. Med. Assoc. 1999, 215, 1105–1110. [Google Scholar] [PubMed]
- Slingsby, L.S.; Waterman-Pearson, A.E. Analgesic effects in dogs of carprofen and pethidine together compared with the effects of either drug alone. Vet. Rec. 2001, 148, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Slingsby, L.S.; Waterman-Pearson, A.E. Comparison between meloxicam and carprofen for postoperative analgesia after feline ovariohysterectomy. J. Small Anim. Pract. 2002, 43, 286–289. [Google Scholar] [CrossRef] [PubMed]
- McGeown, D.; Danbury, T.C.; Waterman-Pearson, A.E.; Kestin, S.C. Effect of carprofen on lameness in broiler chickens. Vet. Rec. 1999, 144, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Roughan, J.V.; Flecknell, P.A. Behaviour-based assessment of the duration of laparotomy-induced abdominal pain and the analgesic effects of carprofen and buprenorphine in rats. Behav. Pharmacol. 2004, 15, 461–472. [Google Scholar] [CrossRef]
- Hawkins, M.G.; Taylor, I.T.; Craigmill, A.L.; Tell, L.A. Enantioselective pharmacokinetics of racemic carprofen in New Zealand white rabbits, J. vet. Pharmacol. Therap. 2008, 31, 423–430. [Google Scholar]
- Simmons, D.L.; Regina, M.B.; Hla, T. Cyclooxygenase isozymes: The biology of prostaglandin synthesis and inhibition. Pharmacol. Rev. 2004, 56, 387–437. [Google Scholar] [CrossRef]
- MacPhail, C.M.; Lappin, M.R.; Meyer, D.J.; Smith, S.G.; Webster, C.R.; Armstrong, P.J. Hepatocellular Toxicosis Associated with Administration of Carprofen in 21 Dogs. J. Am. Vet. Med. Assoc. 1998, 212, 1895–1901. [Google Scholar]
- Chumbler, N.S.; Schildt, J.C.; Mawby, D.I.; Papich, M.G. Use of intravenous lipid therapy in a cat with carprofen overdose. Clin. Case Rep. 2020, 8, 653–657. [Google Scholar] [CrossRef] [PubMed]
- Trepanier, L.A. Idiosyncratic Drug Toxicity Affecting the Liver, Skin, and Bone Marrow in Dogs and Cats. Vet. Clin. Small Anim. 2013, 43, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Mealey, K.L.; Matthews, N.S.; Peck, K.E.; Burchfield, M.L.; Bennett, B.S.; Taylor, T.S. Pharmacokinetics of R(–) and S(+) carprofen after administration of racemic carprofen in donkeys and horses. Am. J. Vet. Res. 2004, 65, 1479–1482. [Google Scholar] [CrossRef] [PubMed]
- Becker, L.; Eberlein-König, B.; Przybilla, B. Phototoxicity of non-steroidal anti-inflammatory drugs: In vitro studies with visible light. Acta Derm. Venereol. 1996, 76, 337–340. [Google Scholar] [PubMed]
- Mcpherson, M.L.; Cimino, N.M. Topical NSAID formulations. Pain Med. 2013, 14, S35–S39. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Guideline on Bionalytical Method Validation-2011. Available online: http://www.ema.europa.eu/docs/enGB/documentlibrary/Scientificguideline/2011/08/WC500109686.pdf/ (accessed on 15 February 2020).
- Asociación Española de Farmacéuticos de la Indústria (AEFI). Validación de métodos analíticos- 2001 Version [homepage on the Internet]. Available online: https://www.aefi.org/venta-publicaciones/78-validacion-de-metodos-analiticos/ (accessed on 15 February 2020).
- Internatonal Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. Harmonised Guideline Bioanalytical Method Validation m10. Available online: https://www.ema.europa.eu/en/ich-m10-bioanalytical-method-validation/ (accessed on 15 February 2020).
- Scientific Working Group for Forensic Toxicology. Scientific Working Group for Forensic Toxicology (SWGTOX) Standard Practices for Method Validation in Forensic Toxicology. J. Anal. Toxicol. 2013, 37, 452–474. [Google Scholar] [CrossRef]
- Brugués, A.P.; Naveros, B.C.; Calpena Campmany, A.C.; Pastor, P.H.; Saladrigas, R.F.; Lizandra, C.R. Developing cutaneous applications of paromomycin entrapped in stimuli-sensitive block copolymer nanogel dispersions. Nanomedicine 2015, 10, 227–240. [Google Scholar] [CrossRef]
- Netzlaff, F.; Schaefer, U.F.; Lehr, C.M.; Meiers, P.; Stahl, J.; Kietzmann, M.; Niedorf, F. Comparison of bovine udder skin with human and porcine skin in percutaneous permeation experiments. Altern. Lab. Anim. 2006, 34, 499–513. [Google Scholar]
- Seto, J.E.; Polat, B.E.; Lopez RF, V.; Blankschtein, D.; Langer, R. Effects of ultrasound and sodium lauryl sulfate on the transdermal delivery of hydrophilic permeants: Comparative in vitro studies with full-thickness and split-thickness pig and human skin. J. Control. Release 2010, 145, 26–32. [Google Scholar] [CrossRef]
- Cañadas-Enrich, C.; Abrego, G.; Alvarado, H.L.; Calpena-Campmany, A.C.; Boix-Montañes, A. Pranoprofen quantification in ex vivo corneal and scleral permeation samples: Analytical validation. J. Pharmaceut. Biomed. Anal. 2018, 160, 109–118. [Google Scholar] [CrossRef]
- Sanz, R.; Clares, B.; Mallandrich, M.; Casals, I.; Bellido, D.; Calpena, A.C. Validation of doxepin quantitative determination methods for their application to in vitro, ex vivo and in vivo studies. Curr. Pharm. Anal. 2015, 11, 269–277. [Google Scholar] [CrossRef]
- OECD Guideline for the Testing of Chemicals, Skin Absorption: In Vitro Method-2018. Available online: https://ntp.niehs.nih.gov/iccvam/suppdocs/feddocs/oecd/oecdtg428-508.pdf/ (accessed on 15 February 2020).
- Gómez-Segura, L.; Parra, A.; Gimeno, A.; Calpena, A.C.; Gómez de Aranda, I.; Boix-Montañes, A. Ex Vivo Permeation of Carprofen Vehiculated by PLGA Nanoparticles through porcine Mucous Membranes and Ophthalmic Tissues. Nanomaterials 2020, 10, 355. [Google Scholar] [CrossRef] [PubMed]
- European Directorate for the Quality of Medicines & HealthCare: Recommendations on Dissolution Testing-2018 Version. Available online: https://www.edqm.eu/sites/default/files/institutional-brochure-edqm.pdf/ (accessed on 15 February 2020).
- Lindstrom, R.; Kim, T. Ocular permeation and inhibition of retinal inflammation: An examination of data and expert opinion on the clinical utility of nepafenac. Curr. Med. Res. Opin. 2006, 22, 397–404. [Google Scholar] [CrossRef]
- Gabani, B.B.; Kiran, V. Incurred sample reanalysis of cefuroxime in rabbit ocular tissues—A case study. Biomed. Chromatogr. 2020, 34, e4737. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.W.; Sanderson, S.; Feng, X.; Hubbard, W.C. Porcine Sclera: Thickness and surface area. Inv. Ophthalm. Vis. Sci. 2002, 43, 2529–2532. [Google Scholar]
- Menduni, F.; Davies, L.N.; Madrid-Costa, D.; Fratini, A.; Wolffsohn, J.S. Characterisation of the porcine eyeball as an in-vitro model for dry eye. Contact Lens Anterio. 2018, 41, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, I.; Martin, R.; Ussa, F.; Fernandez-Bueno, I. The parameters of the porcine eyeball. Graefe’s Arch. Exper. Ophthalm. 2011, 249, 475–482. [Google Scholar] [CrossRef]
- Ahmed, I.; Gokhale, R.; Shah, M.V.; Patton, T.F. Physicochemical determinants of drug diffusion across the conjunctiva, sclera and Cornea. J. Pharm. Sci. 1987, 76, 583–586. [Google Scholar] [CrossRef]
- Domínguez-Villegas, V.; Clares-Naveros, B.; García-López, M.L.; Calpena-Campmany, A.C.; Bustos-Zagal, P.; Garduño-Ramírez, M.L. Development and characterization of two nanostructured systems for topical application of flavanones isolated from Eysenhardtia platycarpa. Colloids Surf. B 2014, 116, 183–192. [Google Scholar] [CrossRef]
- Wu, A.B.; Chen, C.Y.; Chu, S.D.; Tsai, Y.C.; Chen, F.A. Stability-Indicating High-Performance Liquid Chromatographic Assay Method and Photostability of Carprofen. J. Chromatogr. Sci. 2001, 39, 7–11. [Google Scholar] [CrossRef]
- Parra, A.; Mallandrich, M.; Clares, B.; Egea, M.A.; Espina, M.; García, M.L.; Calpena, A.C. Design and elaboration of freeze-dried PLGA nanoparticles for the transcorneal permeation of carprofen: Ocular anti-inflammatory applications. Colloids Surf. B 2015, 136, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.K.W.; Xu, Y.; Xu, Y.; Worsley, A.; Wong, I.C.K. Oral transmucosal drug delivery for pediatric use. Adv. Drug Deliv. Rev. 2014, 73, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Bacha, W.J., Jr.; Bacha, L.M. Color Atlas of Veterinary Histology, 3rd ed.; Wiley & BlackWell: New York, NY, USA, 2012; pp. 102–149. [Google Scholar]
- Zimmerman, J.J.; Karriker, L.A.; Ramirez, A.; Schwartz, K.J.; Stevenson, G.W.; Zhang, J. Diseases of Swine, 11th ed.; Wiley & BlackWell: New York, NY, USA, 2019; pp. 292–392. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Carprofen | Linearity Test | |
| Range | p-Value | |
| 100–3.125 (µg/mL) | 0.404 | |
| 6.25–0.7813 (µg/mL) | 0.0783 | |
| Min., Medium and Max. Concentrations | Accuracy RE (%) | Precision RSD (%) |
| 100 (µg/mL) | 0.21 | 0.60 |
| 12.5 (µg/mL) | 0.96 | 1.77 |
| 0.7813 (µg/mL) | 0.87 | 1.95 |
| Mean | Desvest. | |
| Detection limit (µg/mL) | 0.17 | 0.13 |
| Quantification limit (µg/mL) | 0.51 | 0.40 |
| Carprofen | Conjunctiva (CJ) | Sclera (SC) | Cornea (CO) | p-Value |
|---|---|---|---|---|
| Js (µg/h) | 0.22 | 26.54 | 1.85 | SC vs. CO ** |
| (0.09–0.34) | (15.52–37.56) | (0.14–2.34) | SC vs. CJ *** | |
| Tl (h) | 0.91 | 1.57 | 3.29 | NS |
| (0.58–1.23) | (1.52–1.61) | (2.17–3.34) | ||
| Kp × 102 (cm·h) | 0.045 | 5.53 | 0.39 | SC vs. CO * |
| (0.019–0.071) | (3.23–7.82) | (0.03–0.49) | SC vs. CJ *** |
| Carprofen | Buccal (B) | Sublingual (SB) | Vagina (V) | p-Value |
|---|---|---|---|---|
| Js (µg/h) | 1.61 | 5.1 | 7.59 | NS |
| (0.46–2.77) | (2.38–6.76) | (1.68–13.51) | ||
| Tl (h) | 3.27 | 2.83 | 0.13 | B vs. V *** |
| (3.22–3.31) | (0.86–3.47) | (0.02–0.23) | SB vs. V * | |
| Kp × 102 (cm·h) | 0.085 | 1.0625 | 1.58 | NS |
| (0.024–0.45) | (0.5–1.14) | (0.35–2.81) |
| Membrane | Sample | Amount in Solution, before (µg) | Amount in Solution, after (µg) | Charge (µg) | Extracted Amount (µg) | Recovery (%) | RSD (%) |
|---|---|---|---|---|---|---|---|
| Conjunctiva | FSCN-1 | 91.67 | 0.79 | 90.88 | 16.14 | 17.8% | 15.93 |
| FSCN-2 | 91.67 | 0.73 | 90.94 | 12.88 | 14.2% | ||
| Sclera | FSSC-1 | 91.67 | 47.70 | 43.97 | 1.05 | 2.4% | 7.07 |
| FSSC-2 | 91.67 | 51.51 | 40.16 | 1.06 | 2.6% | ||
| Cornea | FSCR-1 | 91.67 | 51.51 | 40.16 | 1.22 | 3.0% | 14.17 |
| FSCR-2 | 91.67 | 49.13 | 42.54 | 1.58 | 3.7% | ||
| Buccal | FSBC-1 | 98.54 | 0.35 | 98.19 | 1.44 | 1.5% | 15.44 |
| FSBC-2 | 98.54 | 0.90 | 97.64 | 1.15 | 1.2% | ||
| Sublingual | FSSL-1 | 98.54 | 56.44 | 42.1 | 1.12 | 2.7% | 20.06 |
| FSSL-2 | 98.54 | 45.02 | 53.52 | 1.07 | 2.0% | ||
| Vaginal | FSVG-1 | 98.54 | 1.28 | 97.26 | 23.55 | 24.2% | 5.56 |
| FSVG-2 | 98.54 | 0.85 | 97.69 | 25.59 | 26.2% |
| Carprofen | Conjunctiva (CJ) | Cornea (CO) | Sclera (SC) | p-Value |
| Qr (µg/cm2/g) | 22.74 | 14.21 | 48.94 | SC vs. CO ** |
| (19.04–26.45) | (12.38–16.05) | (41.71–56.17) | ||
| Carprofen | Buccal (B) | Sublingual (SB) | Vagina (V) | p-Value |
| Qr (µg/cm2/g) | 10.41 | 18.58 | 26.3 | B vs. V ** |
| (9.22–11.6) | (18.25–18.91) | (26.01–26.59) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Segura, L.; Parra, A.; Calpena, A.C.; Gimeno, Á.; Boix-Montañes, A. Carprofen Permeation Test through Porcine Ex Vivo Mucous Membranes and Ophthalmic Tissues for Tolerability Assessments: Validation and Histological Study. Vet. Sci. 2020, 7, 152. https://doi.org/10.3390/vetsci7040152
Gómez-Segura L, Parra A, Calpena AC, Gimeno Á, Boix-Montañes A. Carprofen Permeation Test through Porcine Ex Vivo Mucous Membranes and Ophthalmic Tissues for Tolerability Assessments: Validation and Histological Study. Veterinary Sciences. 2020; 7(4):152. https://doi.org/10.3390/vetsci7040152
Chicago/Turabian StyleGómez-Segura, Lidia, Alexander Parra, Ana C. Calpena, Álvaro Gimeno, and Antonio Boix-Montañes. 2020. "Carprofen Permeation Test through Porcine Ex Vivo Mucous Membranes and Ophthalmic Tissues for Tolerability Assessments: Validation and Histological Study" Veterinary Sciences 7, no. 4: 152. https://doi.org/10.3390/vetsci7040152
APA StyleGómez-Segura, L., Parra, A., Calpena, A. C., Gimeno, Á., & Boix-Montañes, A. (2020). Carprofen Permeation Test through Porcine Ex Vivo Mucous Membranes and Ophthalmic Tissues for Tolerability Assessments: Validation and Histological Study. Veterinary Sciences, 7(4), 152. https://doi.org/10.3390/vetsci7040152