The dog had initially been treated by the referring veterinarian with short courses of amoxicillin-clavulanic acid (Synulox; Zoetis, Rome, Italy) 25 mg/kg orally twice daily combined with prednisone (Deltacortene; Bruno Farmaceutici, Rome, Italy) 0.5 mg/kg orally once daily, leading to a temporary improvement, followed by progressive worsening of the condition.
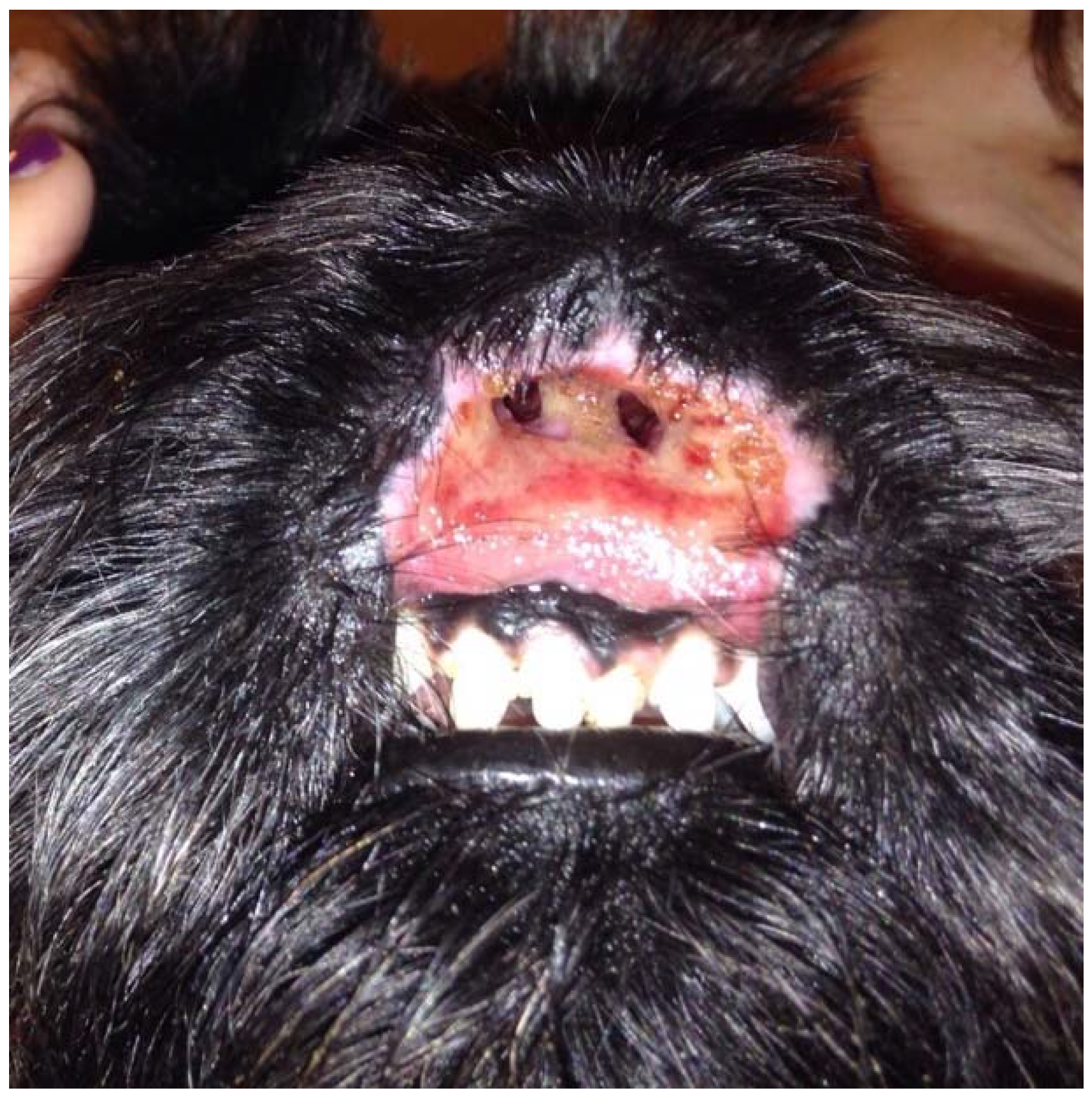
Pseudomonas aeruginosa, which was sensitive to gentamycin and quinolones, was isolated from the nasal tissues by a bacterial culture performed by the referring veterinarian when the dog was nine months old. Marbofloxacin (Aristos; ATI, Ozzano nell’Emilia, Italy) 2 mg/kg orally once daily was administered for one month without improvement. The referring veterinarian then administered methylprednisolone acetate (DepoMedrol Vet; Zoetis, Rome, Italy) 1 mg/kg intramuscularly, leading to clinical improvement of the lesions and abnormal scarring and stenosis of the nostrils. Three weeks later, erosions and ulcerations were progressively worsening, and the dog was referred for dermatological consultation. The dog was regularly vaccinated, dewormed, on heartworm prevention, and fed a commercial dry food. A fipronil-S-methoprene spot-on product (Frontline Combo; Merial, Milano, Italy) was applied monthly for flea and tick prevention. The patient had no history of previous diseases. On general examination, the dog appeared to be in good health. The rectal temperature was normal and respiratory and heart rates were within normal limits. Lymph nodes were normal in size. On dermatological examination, wide and deep ulcers were apparent, with complete destruction of the nasal planum, philtrum, and nostrils as well as the central part of the upper lips. The ulcerative process also affected the gum, in correspondence with the upper central incisors. These lesions were neither painful nor pruritic, and the dog could eat normally (
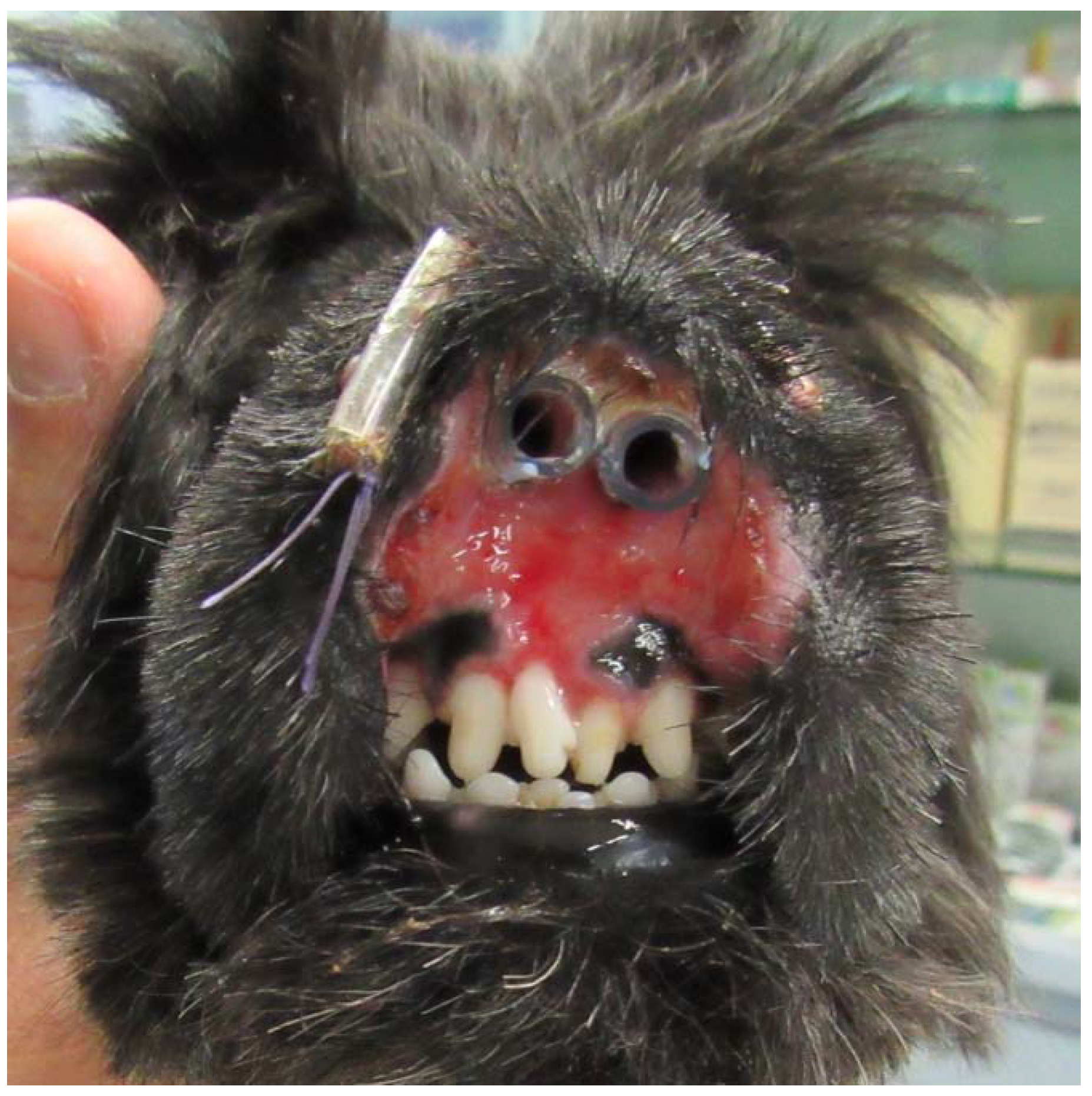
Figure 1). Differential diagnoses considered for this presentation included nasal planum vasculopathy of the Scottish Terrier dog, dermal arteritis of the nasal philtrum, discoid lupus erythematosus, pemphigus complex, squamous cell carcinoma, and leishmaniosis. The latter was unlikely because the dog lived in a nonendemic area in Northern Italy and Immunofluorescence Antibody Test titer was negative. Cytological examination of cutaneous lesions revealed sparse cocci, rare neutrophils, and many erythrocytes and was therefore considered inconclusive. Biopsy specimens were collected by the referring veterinarian under general anesthesia with a 5 mm biopsy punch from erosions and ulcers. Histological examination of haematoxylin and eosin-stained sections revealed an irregularly hyperplastic epidermis, erosions, ulcerations, and granulation tissue, and it was not diagnostic. Even if the primary pathognomonic lesions were not observed, the clinical presentation and response to therapy were consistent with the diagnosis of a dermatosis previously described as vasculopathy of the nasal planum of the Scottish Terrier dog. The dog was treated with oral prednisolone, 1 mg/kg once daily (Vetsolone; Bayer, Milano, Italy) and oral ciclosporin, 5 mg/kg once daily (Atoplus; Elanco, Sesto Fiorentino, Italy) for three weeks. Prednisolone was slowly tapered and discontinued after 20 weeks of therapy, while ciclosporin was continued at the same dosage. Two stents were placed in the nostrils in order to prevent abnormal scarring and subsequent stenosis (
Figure 2). Stents consisted of two sections of silicone drainage tubes measuring 1.5 cm in length and 0.4 cm diameter. These were inserted in the nares rostrally and fixed to the dorsolateral walls of the nasal cavities with a monofilament EP 3.5 suture material composed of polyglycolide-poly (e-caprolactone) copolymer (Monofil; Assut Europe, Rome, Italy) under general anesthesia. Stents were well tolerated by the dog and were removed and replaced twice, every two months, due to dissolution of the suture material. Stents were definitely removed after six months from the first application.
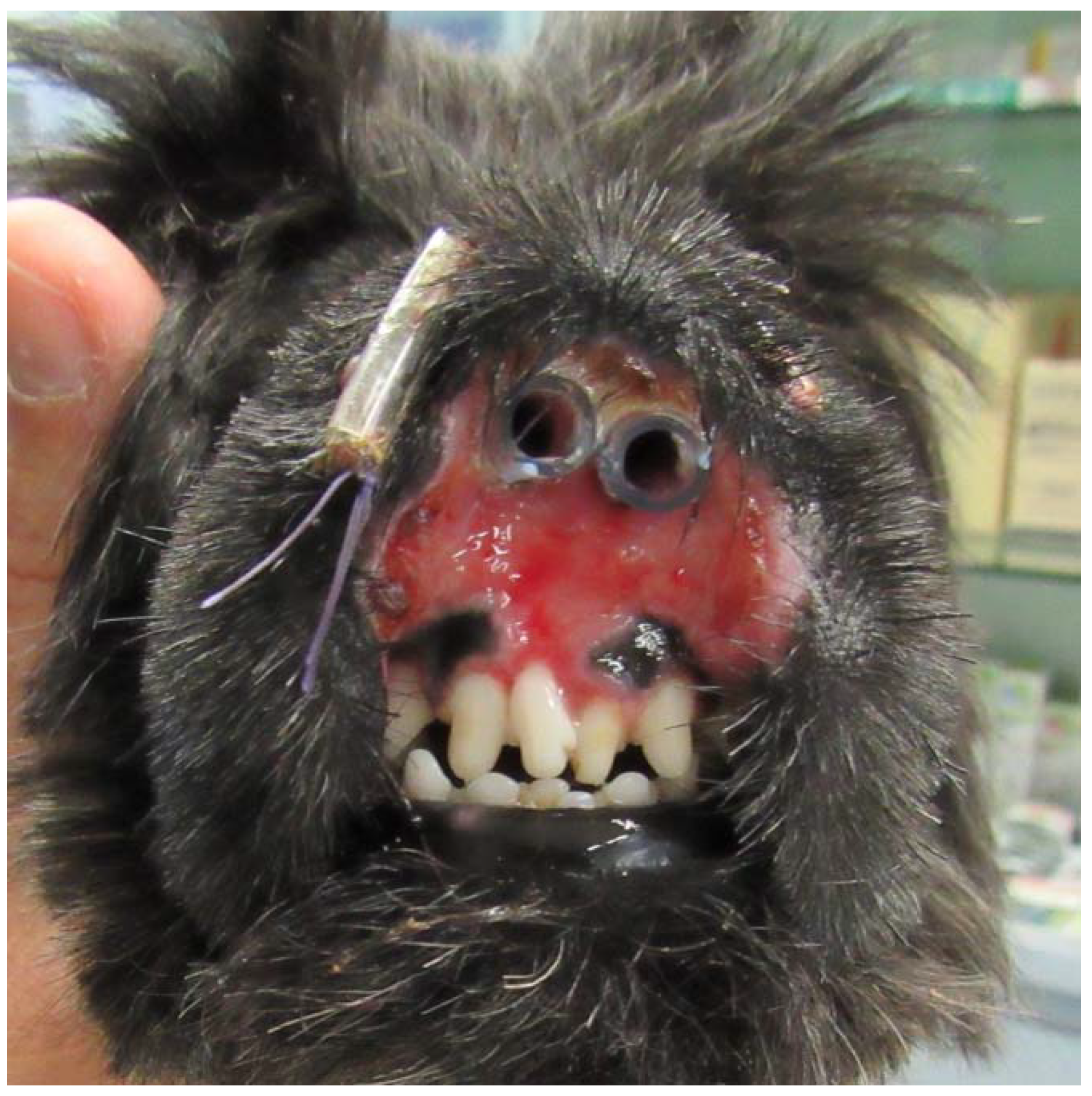
During the treatment, no adverse effects were observed except for polyuria and mild polydipsia. Haematological and biochemical profiles were performed once monthly. No relevant haematologic abnormalities were recorded. Biochemistry panel showed moderate elevation of alkaline phosphatase (ALP) consistent with glucocorticoid administration. All these abnormalities resolved when prednisolone was discontinued. During the first month of therapy, the dog’s condition showed improvement at the weekly rechecks. Ulcers, although still present, markedly decreased in size and depth. Erosive and ulcerative lesions completely regressed within five months after stents removal (
Figure 3). There was complete re-epithelialization of the muzzle, although with severe scarring, and regrowth of hair at the periphery of the affected area. The nasal planum and the central part of the upper lip were absent, and two remnants of the nares were present; however, the dog could breathe and eat normally. More than one and a half years after the start of the medications, the dog is still on treatment with 5 mg/kg ciclosporin orally once daily, breathes and eats normally, and the quality of life is excellent.


{kind=link}
{kind=link}
{kind=link}