
Primary Evaluation of Three-Dimensional Printing-Guided Endodontics in the Dog Maxillary

 , ,
, ,  ,
, 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
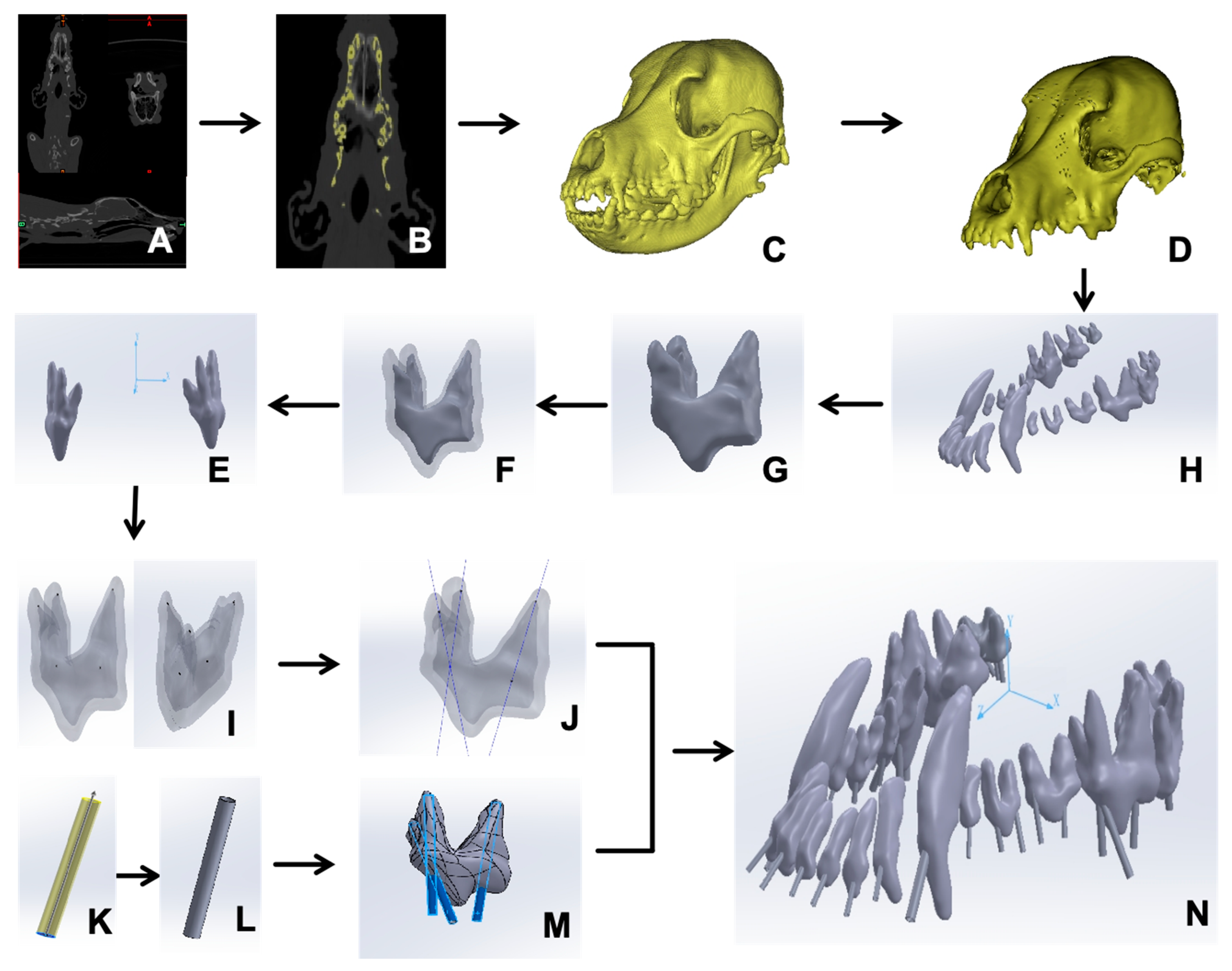
2.1. Creation of a 3D Model of the Beagle Maxillary
2.2. Extraction of Maxillary Teeth
2.3. Formulation of Root Canal Pathways and Guiding Templates
2.4. Root Canal Experiment in Vitro
2.5. Statistical Analysis
3. Results
3.1. Computer-Aided Design of the Root Canal Guided Lines
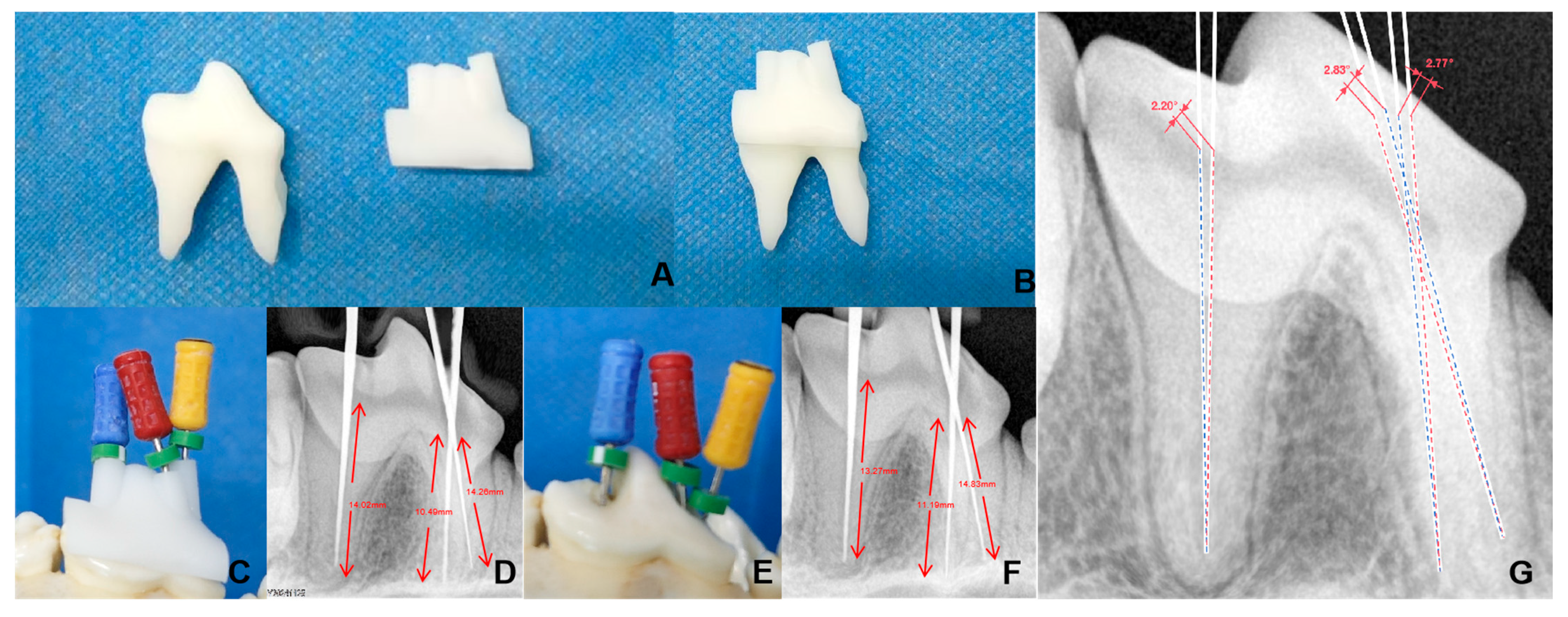
3.2. Three-Dimensional-Printed Maxillary and Guided Endodontic Templates
3.3. Comparison of 3D Printing-Guided Endodontics and Conventional Root Canal Methods
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peng, J.; Yang, J.; Liu, R.; Liu, H.; Zhong, Z.; Peng, G.; Zhang, K.; Zheng, C.; Zhang, M.; Zhou, Z. Evaluating the concept of three-dimensional printing guided endodontics in the dog. Front. Vet. Sci. 2024, 11, 1481612. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, B.; Fang, B.; Gong, H.; Han, Y.; Pei, S.; Zhang, S.; Song, G. Finite element analysis of a three-dimensional cervical spine model with muscles based on CT scan data. Comput. Methods Biomech. Biomed. Eng. 2024, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Yang, J.; Zhu, Y.; Zhou, X.; Zhou, Q.; Liang, T.; Wang, H.; Luo, Y.; Xie, Y.; Liu, H.; et al. A forecasting model for suitable dental implantation in canine mandibular premolar region based on finite element analysis. BMC Vet. Res. 2024, 20, 353. [Google Scholar] [CrossRef]
- Rodillo, M.; Cunha, R.S.; Bauer, P.A.; Travan, S.; Cavalcanti, B.; McDonald, N. Incidence of missed canals during endodontic treatment of maxillary first and second molars. Gen. Dent. 2024, 72, 10–14. [Google Scholar] [PubMed]
- Prabhuji, V.; Archana, S.; Srirekha, A.; Pai, V.; Champa, C.; Shetty, A. Comparative evaluation of efficacy of guided endodontic technique with and without sleeve for access cavity preparation: An In Vitro study. J. Oral Biol. Craniofacial Res. 2024, 14, 825–829. [Google Scholar] [CrossRef]
- Banka, A.; Patri, G.; Pradhan, P.K.; Lath, H. Comparative evaluation between guided endodontics and conventional techniques for calcific metamorphosis—A systematic review and meta-analysis. J. Conserv. Dent. Endod. 2024, 27, 891–896. [Google Scholar] [CrossRef]
- AlTamimi, E.A.; Agwan, M.A.S.; Ahmad, M.Z. Endodontic Management of Failed Root Canal Treatment in Teeth with Previously Missed Canals: A Report of Two Cases with Rare Root Canal Morphology. Cureus 2024, 16, e73466. [Google Scholar] [CrossRef]
- Hernández, S.Z.; Negro, V.B.; Maresca, B.M. Morphologic Features of the Root Canal System of the Maxillary Fourth Premolar and the Mandibular First Molar in Dogs. J. Vet. Dent. 2001, 18, 9–13. [Google Scholar] [CrossRef]
- Jinesh, A.; Nair, S.J.; Gupta, S.; Chansoria, H.; Rawat, G.; Jinesh, A., Jr.; Chansoria, H.; Rawat, G. Unusual Canal Morphology in Mandibular Premolars with Two Distal and One Mesial Canal: A Case Series. Cureus 2024, 16, e73832. [Google Scholar]
- Maravić, T.; Vasiljević, D.; Kantardžić, I.; Lainović, T.; Lužanin, O.; Blažić, L. Influence of restorative procedures on endodontically treated premolars: Finite element analysis of a CT-scan based three-dimensional model. Dent. Mater. J. 2018, 37, 493–500. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Chong, B.; McCabe, P.; Shah, P.; Priya, E.; Jayaraman, J.; Pulikkotil, S.; Dummer, P. PRICE 2020 guidelines for reporting case reports in Endodontics: Explanation and elaboration. Int. Endod. J. 2020, 53, 922–947. [Google Scholar] [CrossRef] [PubMed]
- ISO 3630-1:2008; Dentistry—Root-Canal Instruments—Part 1: General Requirements and Test Methods. International Organization for Standardization (ISO): Geneva, Switzerland, 2008.
- Armenta, H.B.; Mireles, A.G.R.; Martinez, J.S.; Alvarez, J.P.; Herrera, Y.R.; Maldonado, O.T.; Ojeda, O.A.; Pacheco, J.S.; Sarabia, G.O.; Juarez, F.X.C.; et al. Prevalence and Classification of C-Shaped Canal and Radix in Mandibular Molars Using Cone-Beam Computed Tomography on Mexican Population. Dent. J. 2024, 12, 212. [Google Scholar] [CrossRef]
- Prasad, P.; Galani, M.; Nawal, R.R.; Talwar, S.; Kumar, G. Three-dimensional Assessment of Two-rooted Maxillary Central Incisor with Labiogingival Groove: Endodontic and Periodontal Surgical Management. Int. J. Clin. Pediatr. Dent. 2023, 16, 528–533. [Google Scholar] [PubMed]
- Lee, D.B.; Arzi, B.; Kass, P.H.; Verstraete, F.J. Radiographic outcome of root canal treatment in dogs: 281 teeth in 204 dogs (2001–2018). J. Am. Vet. Med. Assoc. 2022, 260, 535–542. [Google Scholar] [CrossRef]
- Dan, Z.; Weige, X.; Tianguo, L.; Anqi, W.; Li, W.; Wen, K.; Lu, W.; Shiliang, G.; Xuna, T.; Sijing, X. New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: A study of 14 upper anterior teeth. Sci. Rep. 2023, 13, 15512. [Google Scholar]
- Ahn, S.-Y.; Kim, N.-H.; Kim, S.; Karabucak, B.; Kim, E. Computer-aided Design/Computer-aided Manufacturing–guided Endodontic Surgery: Guided Osteotomy and Apex Localization in a Mandibular Molar with a Thick Buccal Bone Plate. J. Endod. 2018, 44, 665–670. [Google Scholar] [CrossRef]
- Torres, A.; Dierickx, M.; Lerut, K.; Bleyen, S.; Shaheen, E.; Coucke, W.; Pedano, M.S.; Lambrechts, P.; Jacobs, R. Clinical outcome of guided endodontics versus freehand drilling: A controlled clinical trial, single arm with external control group. Int. Endod. J. 2024, 58, 209–224. [Google Scholar] [CrossRef]
- Buchgreitz, J.; Buchgreitz, M.; Bjørndal, L. Guided Endodontics Modified for Treating Molars by Using an Intracoronal Guide Technique. J. Endod. 2019, 45, 818–823. [Google Scholar] [CrossRef]
- Tandir, F.; Avdić, R.; Dučić, N.; Džanković, A.; Tandir, R.; Šaljić, E.; Vejzović, A.; Hadžiomerović, N. Position and frequency of lateral canals in carnassial teeth of dogs. Res. Vet. Sci. 2024, 179, 105384. [Google Scholar] [CrossRef]
- Fossati, C. Retreatment of a mandibular second premolar with two canals in two roots. G. Ital. Endod. 2018, 32, 31–35. [Google Scholar] [CrossRef]
- SunMi, K.; Eunsuk, A. Tooth Survival Following Non-Surgical Root Canal Treatment in South Korean Adult Population: A 11-Year Follow-Up Study of a Historical Cohort. Eur. Endod. J. 2022, 7, 20–26. [Google Scholar]
- Fernandes, G.W.; Roberti, G.L.d.F.; Peressoni, V.D.; Antunes, B.E.; Lima, D.L.C.d.; Silveira, T.C.d. Guided Endodontics in Root Canals with Complex Access: Two Case Reports. Braz. Dent. J. 2021, 32, 115–123. [Google Scholar]
- Wei, X.; Du, Y.; Zhou, X.; Yue, L.; Yu, Q.; Hou, B.; Chen, Z.; Liang, J.; Chen, W.; Qiu, L.; et al. Expert consensus on digital guided therapy for endodontic diseases. Int. J. Oral Sci. 2023, 15, 540–551. [Google Scholar] [CrossRef]
- Abdelhafeez, M.M. Applications of Finite Element Analysis in Endodontics: A Systematic Review and Meta-Analysis. J. Pharm. Bioallied Sci. 2024, 16, S1977–S1980. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Tooth Number | Root Position | Apex Point (x1, y1, z1) | Central Point of the Dental Root Canal Orifice (x2, y2, z2) | Tooth Number | Root Position | Apex Point (x1, y1, z1) | Central Point of the Dental Root Canal Orifice (x2, y2, z2) |
|---|---|---|---|---|---|---|---|
| 101 | / | (−1.84, 5.78, 51.91) | (−0.88, 1.03, 60.62) | 201 | / | (3.19, 5.84, 51.10) | (4.01, 1.42, 59.73) |
| 102 | / | (−4.55, 6.43, 49.65) | (−5.85, 1.17, 59.41) | 202 | / | (5.74, 7.03, 48.82) | (8.81, 1.21, 58.28) |
| 103 | / | (−6.89, 7.03, 46.31) | (−10.34, 0.93, 55.93) | 203 | / | (6.85, 7.40, 43.00) | (11.84, 2.32, 54.22) |
| 104 | / | (−12.30, 13.23, 23.33) | (−13.64, −0.42, 44.52) | 204 | / | (9.42, 14.41, 25.21) | (13.98, 1.30, 42.73) |
| 105 | / | (−13.72, 3.27, 29.12) | (−14.22, −2.82, 33.54) | 205 | / | (11.87, 3.96, 27.36) | (14.44, −1.42, 31.66) |
| 106 | mesial | (−14.52, 1.48, 24.99) | (−14.58, −5.28, 26.86) | 206 | mesial | (12.36, 3.40, 23.84) | (14.84, −2.93, 25.23) |
| distal | (−14.47, 0.42, 19.42) | (−16.16, −5.03, 21.69) | distal | (12.97, 0.95, 18.55) | (15.86, −3.76, 20.54) | ||
| 107 | mesial | (−15.72, 0.36, 13.91) | (−17.09, −6.14, 14.57) | 207 | mesial | (13.50, 1.32, 13.13) | (16.15, −3.96, 15.00) |
| distal | (−18.44, −0.84, 8.17) | (−20.25, −7.27, 9.93) | distal | (16.62, 0.40, 6.68) | (19.04, −5.43, 9.79) | ||
| 108 | mesiobuccal | (−17.27, −0.41, 3.09) | (−22.41, −10.18, 3.83) | 208 | mesiobuccal | (15.53, 0.21, 1.64) | (21.37, −8.46, 2.57) |
| mesiopalatal | (−23.07, 3.62, 3.06) | (−22.41, −10.18, 3.83) | mesiopalatal | (19.84, 5.76, 1.27) | (22.58, −17.97, 2.63) | ||
| distal | (−26.45, 1.46, −6.39) | (−25.10, −10.69, −3.45) | distal | (23.00, 3.75, −9.03) | (24.10, −9.05, −5.70) | ||
| 109 | mesiobuccal | (−27.84, −3.89, 10.04) | (−25.47, −13.04, −11.20) | 209 | mesiobuccal | (16.34, 0.19, −15.28) | (17.62, −8.05, −14.04) |
| mesiopalatal | (−20.62, 2.96, −14.25) | (−19.85, −9.75, −12.74) | mesiopalatal | (24.37, −0.17, −18.00) | (22.86, −8.32, −16.81) | ||
| distobuccal | (−28.12, −3.51, −16.38) | (−25.14, −12.14, −14.89) | distobuccal | (24.83, −1.94, −12.00) | (24.54, −9.57, −13.16) | ||
| 110 | mesiobuccal | (−24.82, 5.03, −19.16) | (−22.23, −8.93, −20.12) | 210 | mesiobuccal | (16.49, −1.93, −24.18) | (16.80, −6.21, −24.17) |
| mesiopalatal | (−18.22, −2.86, 19.99) | (−17.48, −7.54, −20.01) | mesiopalatal | (13.21, −1.88, −21.51) | (13.84, −6.00, −21.97) | ||
| distobuccal | (−21.29, 4.10, −22.51) | (−19.96, −8.32, −21.95) | distobuccal | (20.78, −2.00, −20.96) | (18.96, −7.39, −21.85) |
| Tooth Number | Root Position | Guided Endodontics/mm | Classic Method/mm | Deviation Rate | Angular Deviation | Tooth Number | Root Position | Guided Endodontics/mm | Classic Method/mm | Deviation Rate | Angular Deviation |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 101 | / | 9.97 | 9.87 | 1.00% | 2.38° | 201 | / | 9.73 | 9.5 | 2.36% | 1.17° |
| 102 | / | 11.16 | 11.34 | 1.61% | 1.65° | 202 | / | 11.52 | 11.75 | 2.00% | 2.03° |
| 103 | / | 11.9 | 11.98 | 0.67% | 2.08° | 203 | / | 13.29 | 13.42 | 0.98% | 1.41° |
| 104 | / | 24.01 | 24.46 | 1.87% | 1.28° | 204 | / | 23.92 | 23.82 | 0.42% | 1.34° |
| 105 | / | 7.55 | 7.47 | 1.06% | 1.81° | 205 | / | 7.36 | 7.19 | 2.31% | 2.24° |
| 106 | mesial | 7.12 | 7.41 | 4.07% | 2.17° | 206 | mesial | 6.93 | 6.85 | 1.15% | 1.31° |
| distal | 6.14 | 6.13 | 0.16% | 1.45° | distal | 5.88 | 6.13 | 4.25% | 1.64° | ||
| 107 | mesial | 6.67 | 6.54 | 1.95% | 2.41° | 207 | mesial | 6.20 | 6.56 | 5.81% | 2.4° |
| distal | 6.90 | 6.84 | 0.87% | 1.77° | distal | 7.04 | 6.79 | 3.55% | 1.68° | ||
| 108 | mesiobuccal | 11.06 | 11.67 | 5.52% | 2.21° | 208 | mesiobuccal | 10.49 | 11.19 | 6.67% | 1.83° |
| mesiopalatal | 13.63 | 14.31 | 4.99% | 2.27° | mesiopalatal | 14.26 | 14.83 | 4.00% | 1.77° | ||
| distal | 12.54 | 11.91 | 5.02% | 1.72° | distal | 14.02 | 13.27 | 5.35% | 2.2° | ||
| 109 | mesiobuccal | 9.53 | 9.17 | 3.78% | 1.61° | 209 | mesiobuccal | 7.73 | 7.61 | 1.55% | 1.41° |
| palatal | 6.99 | 7.29 | 4.29% | 2.25° | palatal | 8.65 | 8.43 | 2.54% | 1.98° | ||
| distobuccal | 9.24 | 9.57 | 3.57% | 2.07° | distobuccal | 8.38 | 8.75 | 4.42% | 1.36° | ||
| 110 | mesiobuccal | 4.77 | 4.97 | 4.19% | 1.75° | 210 | mesiobuccal | 5.55 | 5.39 | 2.88% | 2.17° |
| palatal | 4.94 | 5.11 | 3.44% | 2.18° | palatal | 4.29 | 4.41 | 2.80% | 1.87° | ||
| distobuccal | 5.73 | 5.47 | 4.54% | 1.94° | distobuccal | 4.40 | 4.63 | 5.23% | 2.28° |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, C.; Pan, X.; Peng, J.; Zhou, X.; Shi, X.; Yang, L.; Luo, Y.; Liu, H.; Zhong, Z.; Peng, G.; et al. Primary Evaluation of Three-Dimensional Printing-Guided Endodontics in the Dog Maxillary. Vet. Sci. 2025, 12, 665. https://doi.org/10.3390/vetsci12070665
Zheng C, Pan X, Peng J, Zhou X, Shi X, Yang L, Luo Y, Liu H, Zhong Z, Peng G, et al. Primary Evaluation of Three-Dimensional Printing-Guided Endodontics in the Dog Maxillary. Veterinary Sciences. 2025; 12(7):665. https://doi.org/10.3390/vetsci12070665
Chicago/Turabian StyleZheng, Chengli, Xiaoxuan Pan, Jiahui Peng, Xiaoxiao Zhou, Xin Shi, Liuqing Yang, Yan Luo, Haifeng Liu, Zhijun Zhong, Guangneng Peng, and et al. 2025. "Primary Evaluation of Three-Dimensional Printing-Guided Endodontics in the Dog Maxillary" Veterinary Sciences 12, no. 7: 665. https://doi.org/10.3390/vetsci12070665
APA StyleZheng, C., Pan, X., Peng, J., Zhou, X., Shi, X., Yang, L., Luo, Y., Liu, H., Zhong, Z., Peng, G., Yang, M., Zhang, M., & Zhou, Z. (2025). Primary Evaluation of Three-Dimensional Printing-Guided Endodontics in the Dog Maxillary. Veterinary Sciences, 12(7), 665. https://doi.org/10.3390/vetsci12070665