
A Computationally Efficient Approach to Simulate Heart Rate Effects Using a Whole Human Heart Model

Abstract
1. Introduction
2. Methods
3. Results
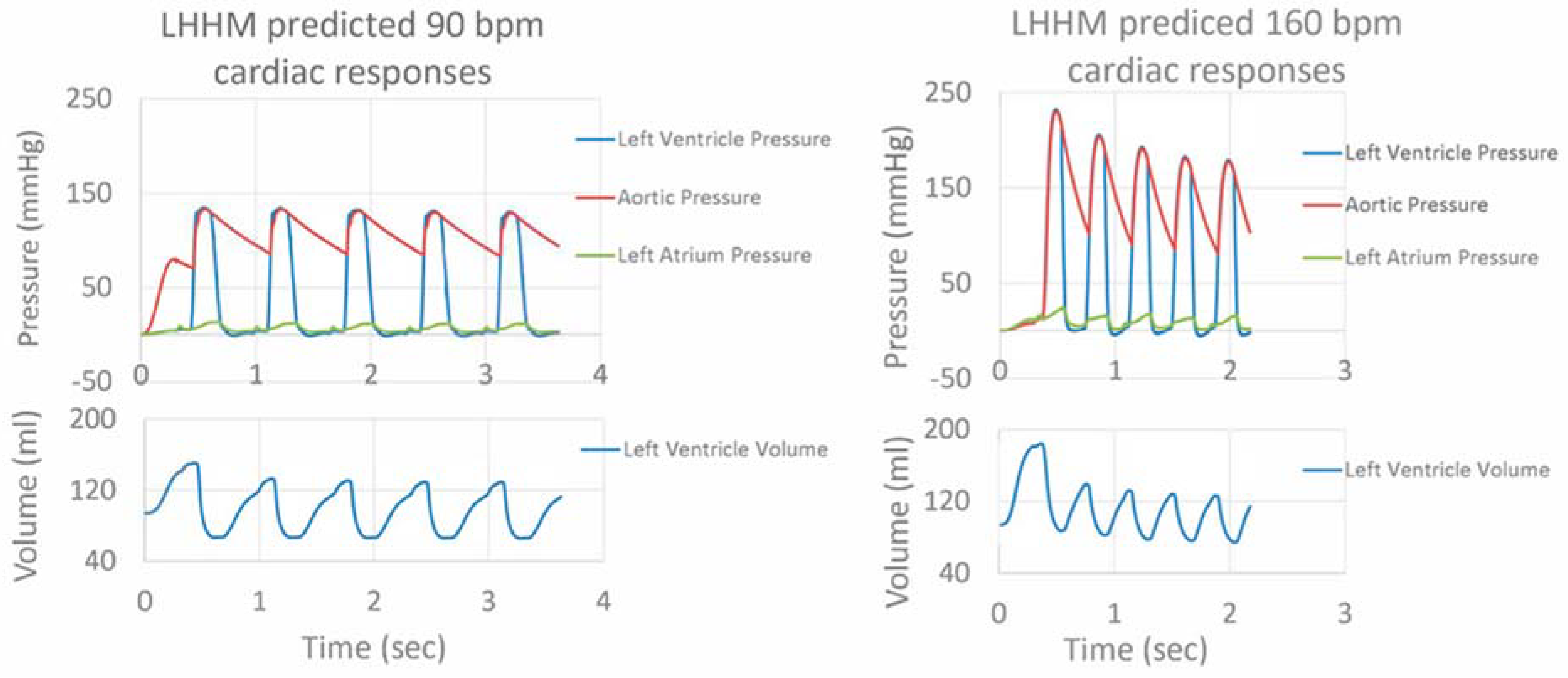
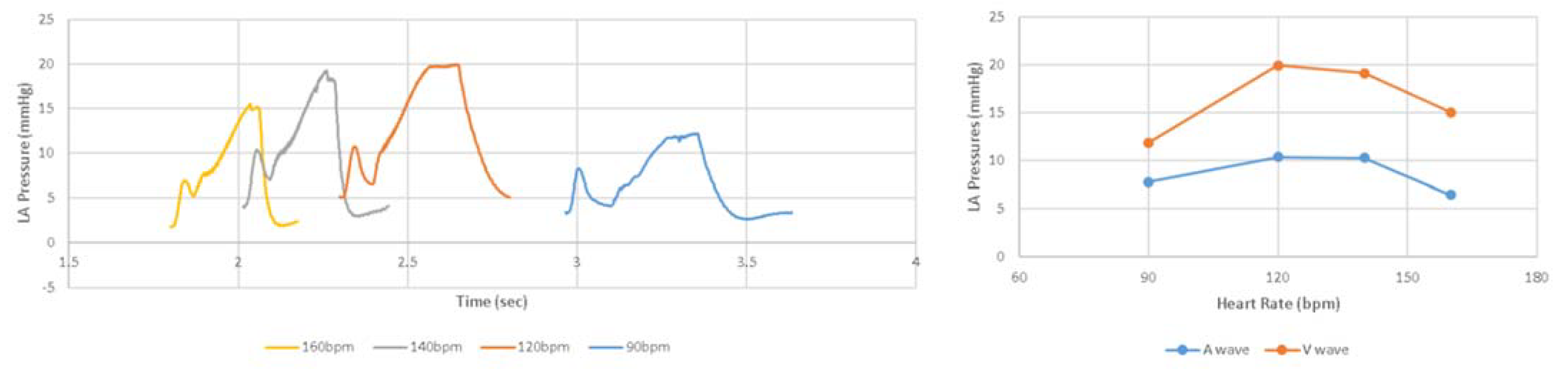
3.1. Results Related to Exercise-Induced Increased Heart Rate
3.2. Results Related to Pacing-Induced Increased Heart Rate
3.3. Results Related to Optimized AV Delay
4. Discussion
4.1. Comparison to Other Models for Simulating Heart Rate Effects
4.2. Parameter Estimation and Machine Learning
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baillargeon, B.; Rebelo, N.; Fox, D.D.; Taylor, R.L.; Kuhl, E. The living heart project: A robust and integrative simulator for human heart function. Eur. J. Mech.-A/Solids 2014, 48, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Sack, K.L.; Baillargeon, B.; Acevedo-Bolton, G.; Genet, M.; Rebelo, N.; Kuhl, E.; Klein, L.; Weiselthaler, G.M.; Burkhoff, D.; Franz, T.; et al. Partial LVAD restores ventricular outputs and normalizes LV but not RV stress distributions in the acutely failing heart in silico. Int. J. Artif. Organs 2016, 39, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Rausch, M.K.; Zöllner, A.M.; Genet, M.; Baillargeon, B.; Bothe, W.; Kuhl, E. A virtual sizing tool for mitral valve annuloplasty. Int. J. Numer. Methods Biomed. Eng. 2017, 33, e02788. [Google Scholar] [CrossRef]
- Peirlinck, M.; Costabal, F.S.; Yao, J.; Guccione, J.M.; Tripathy, S.; Wang, Y.; Ozturk, D.; Segars, P.; Morrison, T.M.; Levine, S.; et al. Precision medicine in human heart modeling. Biomech. Model. Mechanobiol. 2021, 20, 803–831. [Google Scholar] [CrossRef]
- Galili, L.; White Zeira, A.; Marom, G. Numerical biomechanics modelling of indirect mitral annuloplasty treatments for functional mitral regurgitation. R. Soc. Open Sci. 2022, 9, 211464. [Google Scholar] [CrossRef]
- Choi, B.R.; Salama, G. Optical mapping of atrioventricular node reveals a conduction barrier between atrial and nodal cells. Am. J. Physiol.-Heart Circ. Physiol. 1998, 274, H829–H845. [Google Scholar] [CrossRef]
- Antonini, L.; Auriti, A.; Pasceri, V.; Meo, A.; Pristipino, C.; Varveri, A.; Greco, S.; Santini, M. Optimization of the atrioventricular delay in sequential and biventricular pacing: Physiological bases, critical review, and new purposes. Europace 2012, 14, 929–938. [Google Scholar] [CrossRef]
- Kindermann, M.; ERÖHLIG, G.; Doerr, T.; Schieffer, H. Optimizing the AV delay in DDD pacemaker patients with high degree AV block: Mitral valve Doppler versus impedance cardiography. Pacing Clin. Electrophysiol. 1997, 20, 2453–2462. [Google Scholar] [CrossRef]
- Wish, M.; Fletcher, R.D.; Gottdiener, J.S.; Cohen, A.I. Importance of left atrial timing in the programming of dual-chamber pacemakers. Am. J. Cardiol. 1987, 60, 566–571. [Google Scholar] [CrossRef]
- Ausubel, K.; Furman, S. The pacemaker syndrome. Ann. Intern. Med. 1985, 103, 420–429. [Google Scholar] [CrossRef]
- Travill, C.M.; Sutton, R. Pacemaker syndrome: An iatrogenic condition. Br. Heart J. 1992, 68, 163. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.J.; Borlaug, B.A.; Kitzman, D.W.; McCulloch, A.D.; Blaxall, B.C.; Agarwal, R.; Chirinos, J.A.; Collins, S.; Deo, R.C.; Gladwin, M.T.; et al. Research Priorities for Heart Failure with Preserved Ejection Fraction: National Heart, Lung, and Blood Institute Working Group Summary. Circulation 2020, 141, 1001–1026. [Google Scholar] [CrossRef] [PubMed]
- Baillargeon, B.; Costa, I.; Leach, J.R.; Lee, L.C.; Genet, M.; Toutain, A.; Wenk, J.F.; Rausch, M.K.; Rebelo, N.; Acevedo-Bolton, G. Human cardiac function simulator for the optimal design of a novel annuloplasty ring with a subvalvular element for correction of ischemic mitral regurgitation. Cardiovasc. Eng. Technol. 2015, 6, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Saul, J.P.; Albrecht, P.; Hartley, L.H.; Lilly, L.S.; Cohen, R.J.; Colucci, W.S. Modulation of cardiac autonomic activity during and immediately after exercise. Am. J. Physiol.-Heart Circ. Physiol. 1989, 256, H132–H141. [Google Scholar]
- Klabunde, R. Cardiovascular Physiology Concepts; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2011. [Google Scholar]
- Naka, K.K.; Tweddel, A.C.; Parthimos, D.; Henderson, A.; Goodfellow, J.; Frenneaux, M.P. Arterial distensibility: Acute changes following dynamic exercise in normal subjects. Am. J. Physiol.-Heart Circ. Physiol. 2003, 284, H970–H978. [Google Scholar] [CrossRef]
- Hogan, T.S. Exercise-induced reduction in systemic vascular resistance: A covert killer and an unrecognised resuscitation challenge? Med. Hypotheses 2009, 73, 479–484. [Google Scholar] [CrossRef]
- Barbieri, D.; Percoco, G.F.; Toselli, T.; Guardigli, G.; Ansani, L.; Antonioli, G.E. AV delay and exercise stress tests: Behavior in normal subjects. Pacing Clin. Electrophysiol. 1990, 13, 1724–1727. [Google Scholar] [CrossRef]
- Gledhill, N.; Cox, D.; Jamnik, R. Endurance athletes’ stroke volume does not plateau: Major advantage is diastolic function. Med. Sci. Sports Exerc. 1994, 26, 1116–1121. [Google Scholar] [CrossRef]
- Anderson the Cardiovascular System and Exercise. 2017. Available online: https://www.jenreviews.com/cardiovascular-system-and-exercise (accessed on 21 July 2022).
- Morales, M.A.; Startari, U.; Panchetti, L.; Rossi, A.; Piacenti, M. Atrioventricular delay optimization by Doppler-derived left ventricular dP/dt improves 6-month outcome of resynchronized patients. Pacing Clin. Electrophysiol. 2006, 29, 564–568. [Google Scholar] [CrossRef]
- Wessale, J.L.; Voelz, M.B.; Geddes, L.A. Stroke volume and the three phase cardiac output rate relationship with ventricular pacing. Pacing Clin. Electrophysiol. 1990, 13, 673–680. [Google Scholar] [CrossRef]
- Kumada, M.; AZUMA, T.; MATSUDA, K. The cardiac output-heart rate relationship under different conditions. Jpn. J. Physiol. 1967, 17, 538–555. [Google Scholar] [CrossRef] [PubMed]
- Wessale, J.L.; Geddes, L.A.; Fearnot, N.E.; Janas, W.; ANN GROTE, L.E. Cardiac output versus pacing rate at rest and with exercise in dogs with AV block. Pacing Clin. Electrophysiol. 1988, 11, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Manisty, C.H.; Al-Hussaini, A.; Unsworth, B.; Baruah, R.; Pabari, P.A.; Mayet, J.; Hughes, A.D.; Whinnett, Z.I.; Francis, D.P. The acute effects of changes to AV delay on BP and stroke volume: Potential implications for design of pacemaker optimization protocols. Circ. Arrhythmia Electrophysiol. 2012, 5, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Strocchi, M.; Gsell, M.A.; Augustin, C.M.; Razeghi, O.; Roney, C.H.; Prassl, A.J.; Vigmond, E.J.; Behar, J.M.; Gould, J.S.; Rinaldi, C.A.; et al. Simulating ventricular systolic motion in a four-chamber heart model with spatially varying robin boundary conditions to model the effect of the pericardium. J. Biomech. 2020, 101, 109645. [Google Scholar] [CrossRef]
- Pfaller, M.R.; Cruz Varona, M.; Lang, J.; Bertoglio, C.; Wall, W.A. Using parametric model order reduction for inverse analysis of large nonlinear cardiac simulations. Int. J. Numer. Methods Biomed. Eng. 2020, 36, e3320. [Google Scholar] [CrossRef]
- Campos, J.O.; Sundnes, J.; Dos Santos, R.W.; Rocha, B.M. Uncertainty quantification and sensitivity analysis of left ventricular function during the full cardiac cycle. Philos. Trans. R. Soc. A 2020, 378, 20190381. [Google Scholar] [CrossRef]
- Krishnamurthy, A.; Gonzales, M.J.; Sturgeon, G.; Segars, W.P.; McCulloch, A.D. Biomechanics simulations using cubic Hermite meshes with extraordinary nodes for isogeometric cardiac modeling. Comput. Aided Geom. Des. 2016, 43, 27–38. [Google Scholar] [CrossRef]
- Sturla, F.; Vismara, R.; Jaworek, M.; Votta, E.; Romitelli, P.; Pappalardo, O.A.; Lucherini, F.; Antona, C.; Fiore, G.B.; Redaelli, A. In vitro and in silico approaches to quantify the effects of the Mitraclip system on mitral valve function. J. Biomech. 2017, 50, 83–92. [Google Scholar] [CrossRef]
- Jahandardoost, M.; Fradet, G.; Mohammadi, H. Effect of heart rate on the hemodynamics of bileaflet mechanical heart valves’ prostheses (St. Jude Medical) in the aortic position and in the opening phase: A computational study. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2016, 230, 175–190. [Google Scholar] [CrossRef]
- Dabiri, Y.; Van der Velden, A.; Sack, K.L.; Choy, J.S.; Kassab, G.S.; Guccione, J.M. Prediction of left ventricular mechanics using machine learning. Front. Phys. 2019, 7, 117. [Google Scholar] [CrossRef]
- Rice, J.J.; Wang, F.; Bers, D.M.; de Tombe, P.P. Approximate model of cooperative activation and crossbridge cycline in cardiac muscle using ordinary differential equations. Biophys. J. 2008, 95, 2368–2390. [Google Scholar] [CrossRef] [PubMed]
- Genet, M.; Lee, L.C.; Nguyen, R.; Haraldsson, H.; Acevedo-Bolton, G.; Zhang, Z.; Ge, L.; Ordovas, K.; Kozerke, S.; Guccione, J.M. Distribution of normal human left ventricular myofiber stress at end diastole and end systole: A target for in silico design of heart failure treatments. J. Appl. Physiol. 2014, 117, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Pezel, T.; Venkatesh, B.A.; De Vasconcellos, H.D.; Kato, Y.; Shabani, M.; Xie, E.; Heckbert, S.R.; Post, W.S.; Shea, S.J.; Allen, N.B.; et al. Left atrioventricular coupling index as a prognostic marker of cardiovascular events: The MESA study. Hypertension 2021, 78, 661–671. [Google Scholar] [CrossRef]
- Russo, C.; Jin, Z.; Takei, Y.; Hasegawa, T.; Koshaka, S.; Palmieri, V.; Elkind, M.S.; Homma, S.; Sacco, R.L.; Di Tullio, M.R. Arterial wave reflection and subclinical left ventricular systolic dysfunction. J. Hypertens. 2011, 29, 574. [Google Scholar] [CrossRef]
- Borlaug, B.A.; Paulus, W.J. Heart failure with preserved ejection fraction: Pathophysiology, diagnosis, and treatment. Eur. Heart J. 2011, 32, 670–679. [Google Scholar] [CrossRef]
- Gladden, J.D.; Linke, W.A.; Redfield, M.M. Heart failure with preserved ejection fraction. Pflügers Arch.-Eur. J. Physiol. 2014, 466, 1037–1053. [Google Scholar] [CrossRef] [PubMed]
- Dabiri, Y.; Sack, K.L.; Shaul, S.; Sengupta, P.P.; Guccione, J.M. Relationship of transmural variations in myofiber contractility to left ventricular ejection fraction: Implications for modeling heart failure phenotype with preserved ejection fraction. Front. Physiol. 2018, 9, 1003. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physiological Responses with Increased Heart Rate Due to Exercise | Implication for LHHM |
|---|---|
| Autonomic fibers increase SA firing rate | Reduce SA firing period |
| AV conduction accelerates | Reduce AV delay according to pre-ejection period on ECG |
| Myocardium contractility increases through the Bowditch effect | Reduce the “m” parameter that controls sarcomere relaxation duration |
| Heart blood volume increases as vascular system redistributes blood to tissues with greatest demand for oxygen | Increase preload to increase blood volume into heart |
| Systemic vascular resistance falls due to vasodilatation of blood vessels in active skeletal muscles | Reduce body resistance |
| Arterial distensibility decreases due to endothelial and neurohumoral influences in vasodilatation | Increase arterial stiffness |
| Heart rates (bpm) | 90 | 120 | 140 | 160 |
| SA firing period (second) | 0.67 | 0.50 | 0.43 | 0.38 |
| AV delay (second) | 0.122 | 0.087 | 0.068 | 0.057 |
| m (ms/mm) | 238 | 238 | 175 | 175 |
| Preload (×Baseline) | 1.0 | 2.0 | 3.0 | 3.0 |
| Body resistance (×Baseline) | 1.0 | 0.9 | 0.7 | 0.8 |
| Arterial stiffness (×Baseline) | 1.0 | 1.5 | 2.0 | 3.9 |
| Heart rates (bpm) | 90 | 120 | 140 | 160 |
| SA firing period (second) | 0.67 | 0.50 | 0.43 | 0.38 |
| AV delay (second) | 0.122 | 0.087 | 0.068 | 0.057 |
| m (ms/mm) | 238 | 238 | 175 | 175 |
| Preload (×Baseline) | 1.0 | 1.0 | 1.0 | 1.0 |
| Body resistance (×Baseline) | 1.0 | 1.0 | 1.0 | 1.0 |
| Arterial stiffness (×Baseline) | 1.0 | 1.0 | 1.0 | 1.0 |
| Measurement | Source | Heart Rate (bpm) | |||
|---|---|---|---|---|---|
| 90 | 120 | 140 | 160 | ||
| Cardiac Output (L min−1) | LHHM | 11.3 | 14.6 | 18.8 | 20.8 |
| Gledhill | 10.8 ± 0.4 | 15.1 ± 0.4 | 17.8 ± 0.6 | 20.2 ± 0.9 | |
| Cardiac Time Interval (ms) | |||||
| Left Ventricle Ejection Time | LHHM | 228 | 213 | 187 | 163 |
| Gledhill | 212 ± 11 | 208 ± 4 | 198 ± 2 | 175 ± 3 | |
| Diastolic Filling Time | LHHM | 317 | 200 | 174 | 155 |
| Gledhill | 342 ± 55 | 204 ± 9 | 185 ± 4 | 168 ± 4 | |
| Blood Pressure (mmHg) | |||||
| Diastolic | LHHM | 83 | 82 | 81 | 81 |
| Gledhill | 80 ± 2 | 79 ± 3 | 81 ± 2 | 82 ± 3 | |
| Systolic | LHHM | 129 | 141 | 159 | 178 |
| Gledhill | 135 ± 3 | 143±2 | 158 ± 4 | 172 ± 3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, J.; Chen, S.; Guccione, J.M. A Computationally Efficient Approach to Simulate Heart Rate Effects Using a Whole Human Heart Model. Bioengineering 2022, 9, 334. https://doi.org/10.3390/bioengineering9080334
Yao J, Chen S, Guccione JM. A Computationally Efficient Approach to Simulate Heart Rate Effects Using a Whole Human Heart Model. Bioengineering. 2022; 9(8):334. https://doi.org/10.3390/bioengineering9080334
Chicago/Turabian StyleYao, Jiang, Shawn Chen, and Julius M. Guccione. 2022. "A Computationally Efficient Approach to Simulate Heart Rate Effects Using a Whole Human Heart Model" Bioengineering 9, no. 8: 334. https://doi.org/10.3390/bioengineering9080334
APA StyleYao, J., Chen, S., & Guccione, J. M. (2022). A Computationally Efficient Approach to Simulate Heart Rate Effects Using a Whole Human Heart Model. Bioengineering, 9(8), 334. https://doi.org/10.3390/bioengineering9080334