
Bilateral Sensorimotor Cortical Communication Modulated by Multiple Hand Training in Stroke Participants: A Single Training Session Pilot Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Design
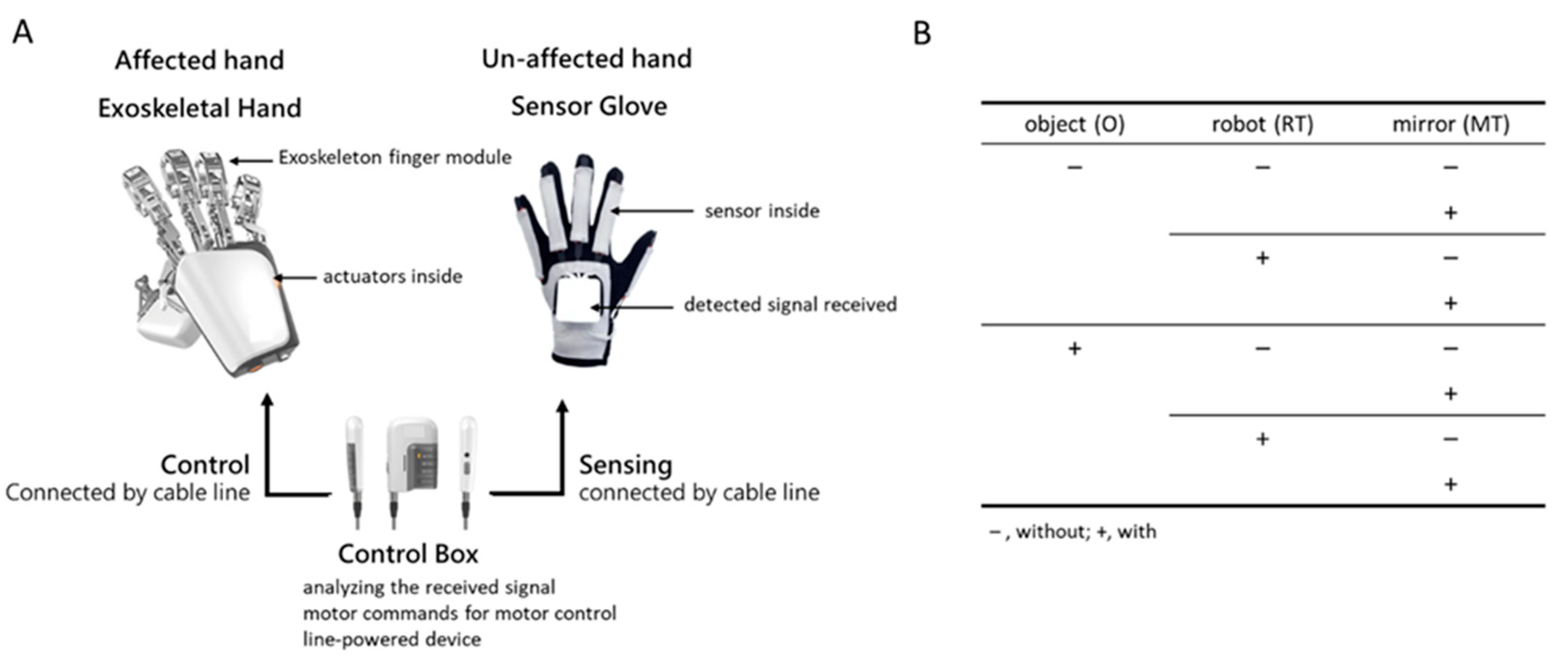
2.2. Exoskeleton Hand Device
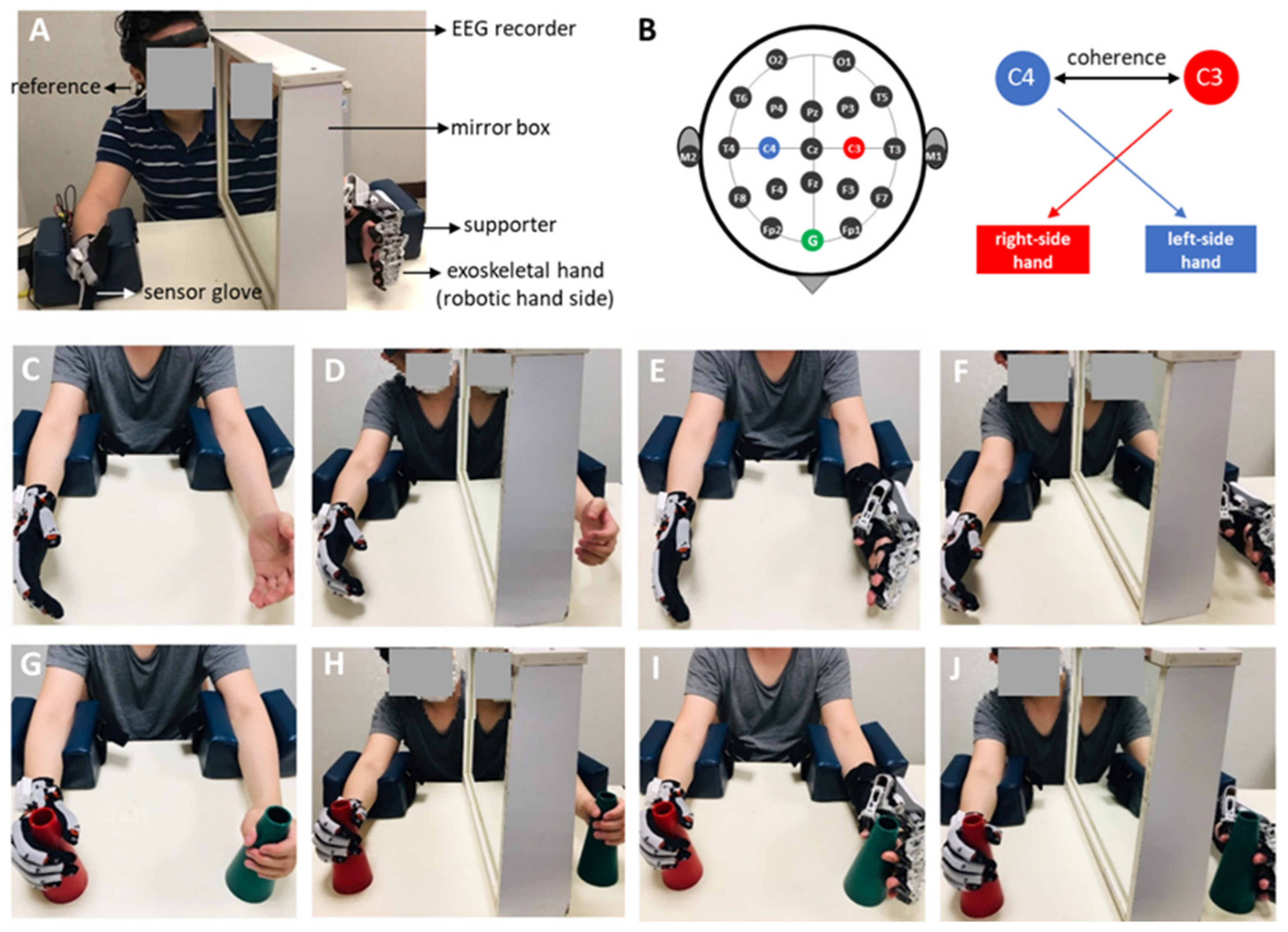
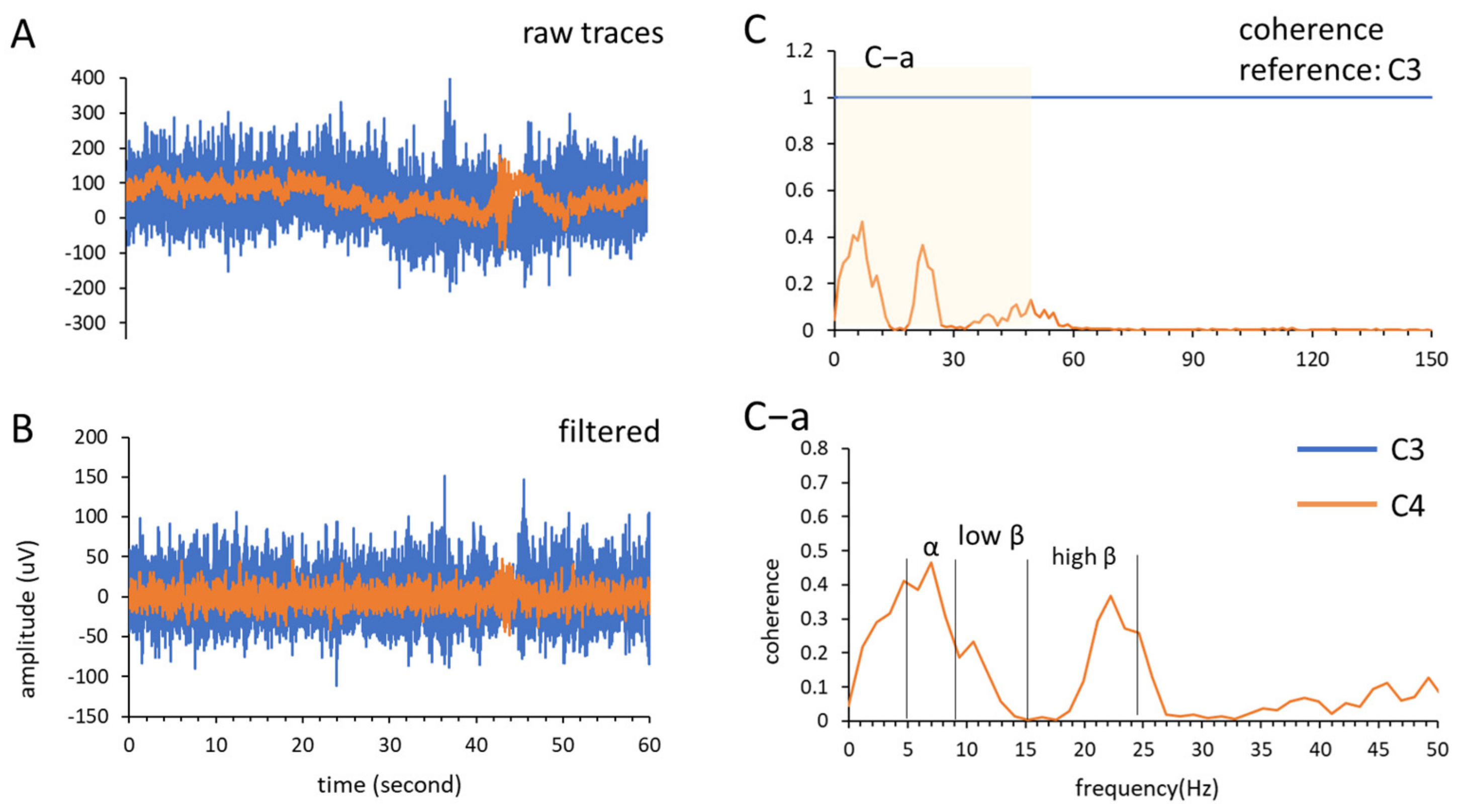
2.3. EEG Recording
2.4. Experimental Design and Procedure
2.4.1. Unilateral Free Hand Movement (Hand)
2.4.2. Mirror Therapy (MT)
2.4.3. Robot-Assisted Bimanual Therapy (RT)
2.4.4. Robotic Therapy with Mirror Therapy (RT × MT)
2.4.5. Object Manipulation (O)
2.5. Data Analysis
2.5.1. Coherence Sum
2.5.2. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feys, H.M.; De Weerdt, W.J.; Selz, B.E.; Cox Steck, G.A.; Spichiger, R.; Vereeck, L.E.; Putman, K.D.; Van Hoydonck, G.A. Effect of a therapeutic intervention for the hemiplegic upper limb in the acute phase after stroke: A single-blind, randomized, controlled multicenter trial. Stroke 1998, 29, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Goldstein, L.B.; Horner, R.D.; Landsman, P.B.; Samsa, G.P.; Matchar, D.B. Similar motor recovery of upper and lower extremities after stroke. Stroke 1994, 25, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Zhang, W.; Santello, M. Anticipatory planning and control of grasp positions and forces for dexterous two-digit manipulation. J. Neurosci. 2010, 30, 9117–9126. [Google Scholar] [CrossRef] [PubMed]
- Johnston, J.A.; Winges, S.A.; Santello, M. Neural control of hand muscles during prehension. Prog. Mot. Control 2009, 629, 577–596. [Google Scholar]
- Fischer, H.C.; Stubblefield, K.; Kline, T.; Luo, X.; Kenyon, R.V.; Kamper, D.G. Hand rehabilitation following stroke: A pilot study of assisted finger extension training in a virtual environment. Top. Stroke Rehabil. 2007, 14, 1–12. [Google Scholar] [CrossRef]
- Bayona, N.A.; Bitensky, J.; Salter, K.; Teasell, R. The role of task-specific training in rehabilitation therapies. Top. Stroke Rehabil. 2005, 12, 58–65. [Google Scholar] [CrossRef]
- Gordon, A.M.; Schneider, J.A.; Chinnan, A.; Charles, J.R. Efficacy of a hand–arm bimanual intensive therapy (HABIT) in children with hemiplegic cerebral palsy: A randomized control trial. Dev. Med. Child Neurol. 2007, 49, 830–838. [Google Scholar] [CrossRef]
- Yavuzer, G.; Selles, R.; Sezer, N.; Sütbeyaz, S.; Bussmann, J.B.; Köseoğlu, F.; Atay, M.B.; Stam, H.J. Mirror therapy improves hand function in subacute stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2008, 89, 393–398. [Google Scholar] [CrossRef]
- Kim, D.H.; Lee, K.-D.; Bulea, T.C.; Park, H.-S. Increasing motor cortex activation during grasping via novel robotic mirror hand therapy: A pilot fNIRS study. J. Neuroeng. Rehabil. 2022, 19, 8. [Google Scholar] [CrossRef]
- Chen, Y.-M.; Lai, S.-S.; Pei, Y.-C.; Hsieh, C.-J.; Chang, W.-H. Development of a Novel Task-oriented Rehabilitation Program using a Bimanual Exoskeleton Robotic Hand. JoVE J. Vis. Exp. 2020, 159, e61057. [Google Scholar] [CrossRef]
- Susanto, E.A.; Tong, R.K.; Ockenfeld, C.; Ho, N.S. Efficacy of robot-assisted fingers training in chronic stroke survivors: A pilot randomized-controlled trial. J. Neuroeng. Rehabil. 2015, 12, 42. [Google Scholar] [CrossRef]
- Cauraugh, J.H.; Summers, J.J. Neural plasticity and bilateral movements: A rehabilitation approach for chronic stroke. Prog. Neurobiol. 2005, 75, 309–320. [Google Scholar] [CrossRef]
- Zult, T.; Goodall, S.; Thomas, K.; Hortobágyi, T.; Howatson, G. Mirror illusion reduces motor cortical inhibition in the ipsilateral primary motor cortex during forceful unilateral muscle contractions. J. Neurophysiol. 2015, 113, 2262–2270. [Google Scholar] [CrossRef]
- Zult, T.; Howatson, G.; Goodall, S.; Thomas, K.; Solnik, S. Mirror training augments the cross-education of strength and affects inhibitory paths. Med. Sci. Sports Exerc. 2016, 48, 1001–1013. [Google Scholar] [CrossRef]
- Jasper, H.; Penfield, W. Electrocorticograms in man: Effect of voluntary movement upon the electrical activity of the precentral gyrus. Arch. Psychiatr. Nervenkrankh. 1949, 183, 163–174. [Google Scholar] [CrossRef]
- Rougeul, A.; Bouyer, J.; Dedet, L.; Debray, O. Fast somato-parietal rhythms during combined focal attention and immobility in baboon and squirrel monkey. Electroencephalogr. Clin. Neurophysiol. 1979, 46, 310–319. [Google Scholar] [CrossRef]
- Ray, A.M.; Figueiredo, T.D.; López-Larraz, E.; Birbaumer, N.; Ramos-Murguialday, A. Brain oscillatory activity as a biomarker of motor recovery in chronic stroke. Hum. Brain Mapp. 2020, 41, 1296–1308. [Google Scholar] [CrossRef]
- Platz, T.; Kim, I.; Pintschovius, H.; Winter, T.; Kieselbach, A.; Villringer, K.; Kurth, R.; Mauritz, K.-H. Multimodal EEG analysis in man suggests impairment-specific changes in movement-related electric brain activity after stroke. Brain 2000, 123, 2475–2490. [Google Scholar] [CrossRef]
- Grefkes, C.; Fink, G.R. Connectivity-based approaches in stroke and recovery of function. Lancet Neurol. 2014, 13, 206–216. [Google Scholar] [CrossRef]
- Irlbacher, K.; Brocke, J.; Mechow, J.; Brandt, S. Effects of GABAA and GABAB agonists on interhemispheric inhibition in man. Clin. Neurophysiol. 2007, 118, 308–316. [Google Scholar] [CrossRef]
- Pellegrino, G.; Tomasevic, L.; Tombini, M.; Assenza, G.; Bravi, M.; Sterzi, S.; Giacobbe, V.; Zollo, L.; Guglielmelli, E.; Cavallo, G. Inter-hemispheric coupling changes associate with motor improvements after robotic stroke rehabilitation. Restor. Neurol. Neurosci. 2012, 30, 497–510. [Google Scholar] [CrossRef] [PubMed]
- Naghdi, S.; Ansari, N.N.; Mansouri, K.; Hasson, S. A neurophysiological and clinical study of Brunnstrom recovery stages in the upper limb following stroke. Brain Inj. 2010, 24, 1372–1378. [Google Scholar] [CrossRef] [PubMed]
- Cordella, F.; Di Luzio, F.S.; Bravi, M.; Santacaterina, F.; Bressi, F.; Zollo, L. Hand motion analysis during robot-aided rehabilitation in chronic stroke. J. Biol. Regul. Homeost. Agents 2020, 34, 45–52. [Google Scholar] [PubMed]
- Takahashi, C.D.; Der-Yeghiaian, L.; Le, V.; Cramer, S.C. A robotic device for hand motor therapy after stroke. In Proceedings of the 9th International Conference on Rehabilitation Robotics (ICORR 2005), Chicago, IL, USA, 28 June–1 July 2005; pp. 17–20. [Google Scholar]
- Homan, R.W.; Herman, J.; Purdy, P. Cerebral location of international 10–20 system electrode placement. Electroencephalogr. Clin. Neurophysiol. 1987, 66, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Vecchio, F.; Lacidogna, G.; Miraglia, F.; Bramanti, P.; Ferreri, F.; Rossini, P.M. Prestimulus Interhemispheric Coupling of Brain Rhythms Predicts Cognitive–Motor Performance in Healthy Humans. J. Cogn. Neurosci. 2014, 26, 1883–1890. [Google Scholar] [CrossRef]
- Leiguarda, R.C.; Marsden, C.D. Limb apraxias: Higher-order disorders of sensorimotor integration. Brain 2000, 123, 860–879. [Google Scholar] [CrossRef]
- Rapcsak, S.Z.; Ochipa, C.; Anderson, K.C.; Poizner, H. Progressive ideomotor apraxia: Evidence for a selective impairment of the action production system. Brain Cogn. 1995, 27, 213–236. [Google Scholar] [CrossRef]
- Agnew, Z.K.; Wise, R.J.; Leech, R. Dissociating object directed and non-object directed action in the human mirror system; Implications for theories of motor simulation. PLoS ONE 2012, 7, e32517. [Google Scholar] [CrossRef]
- Pfurtscheller, G.; Pregenzer, M.; Neuper, C. Visualization of sensorimotor areas involved in preparation for hand movement based on classification of μ and central β rhythms in single EEG trials in man. Neurosci. Lett. 1994, 181, 43–46. [Google Scholar] [CrossRef]
- Schnitzler, A.; Gross, J.; Timmermann, L. Synchronised oscillations of the human sensorimotor cortex. Acta Neurobiol. Exp. 2000, 60, 271–288. [Google Scholar]
- Manganotti, P.; Gerloff, C.; Toro, C.; Katsuta, H.; Sadato, N.; Zhuang, P.; Leocani, L.; Hallett, M. Task-related coherence and task-related spectral power changes during sequential finger movements. Electroencephalogr. Clin. Neurophysiol. Electromyogr. Mot. Control 1998, 109, 50–62. [Google Scholar] [CrossRef]
- Gerloff, C.; Andres, F.G. Bimanual coordination and interhemispheric interaction. Acta Psychol. 2002, 110, 161–186. [Google Scholar] [CrossRef]
- Leocani, L.; Toro, C.; Manganotti, P.; Zhuang, P.; Hallett, M. Event-related coherence and event-related desynchronization/synchronization in the 10 Hz and 20 Hz EEG during self-paced movements. Electroencephalogr. Clin. Neurophysiol. Evoked Potentials Sect. 1997, 104, 199–206. [Google Scholar] [CrossRef]
- Gerloff, C.; Richard, J.; Hadley, J.; Schulman, A.E.; Honda, M.; Hallett, M. Functional coupling and regional activation of human cortical motor areas during simple, internally paced and externally paced finger movements. Brain A J. Neurol. 1998, 121, 1513–1531. [Google Scholar] [CrossRef]
- El Nahas, N.; Roushdy, T.M.; Shokri, H.M.; Moustafa, R.R.; Elsayed, A.M.; Amin, R.M.; Ashour, A.A.; Abd Eldayem, E.H.; Elhawary, G.A.; Elbokl, A.M. Lateralized readiness potentials can identify hemisphere of recovery in stroke patients. Restor. Neurol. Neurosci. 2022, 40, 63–71. [Google Scholar] [CrossRef]
- Philips, G.R.; Daly, J.J.; Príncipe, J.C. Topographical measures of functional connectivity as biomarkers for post-stroke motor recovery. J. Neuroeng. Rehabil. 2017, 14, 67. [Google Scholar] [CrossRef]
- Hao, Z.; Wang, D.; Zeng, Y.; Liu, M. Repetitive transcranial magnetic stimulation for improving function after stroke. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Vahdat, S.; Darainy, M.; Thiel, A.; Ostry, D.J. A single session of robot-controlled proprioceptive training modulates functional connectivity of sensory motor networks and improves reaching accuracy in chronic stroke. Neurorehabilit. Neural Repair 2019, 33, 70–81. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Stroke Patient (n = 40) |
|---|---|
| sex (n) | |
| Male/Female | 28/12 |
| age (y) | 53.28 ± 12.23 |
| affected hand side (n) | |
| Right-side/Left-side | 19/21 |
| affected brain area 1 (n) | |
| cortical/sub-cortical | 17/23 |
| time elapse after stroke (m) | 20.51 ± 23.41 |
| n = 20 | Alpha | Low Beta | High Beta | |||
|---|---|---|---|---|---|---|
| Effects | Mean | SEM | Mean | SEM | Mean | SEM |
| Hand | 0.77 | 0.10 | 0.49 | 0.05 | 0.49 | 0.10 |
| Mirror | 0.75 | 0.15 | 0.56 | 0.08 | 0.63 | 0.14 |
| Robot | 0.82 | 0.13 | 0.57 | 0.13 | 0.93 | 0.27 |
| Mirror × Robot | 0.62 | 0.07 | 0.50 | 0.05 | 0.63 | 0.13 |
| Object | 0.76 | 0.12 | 0.55 | 0.06 | 0.70 | 0.15 |
| Mirror × Object | 0.81 | 0.13 | 0.53 | 0.06 | 0.50 | 0.10 |
| Robot × Object | 0.76 | 0.11 | 0.43 | 0.06 | 0.51 | 0.11 |
| Mirror × Robot × Object | 0.66 | 0.07 | 0.43 | 0.06 | 0.45 | 0.08 |
| n = 20 | Alpha | Low Beta | High Beta | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Effects | F | p-Value | ⴄ2 | F | p-Value | ⴄ2 | F | p-Value | ⴄ2 |
| Object | 0.08 | 0.780 | 0.00 | 1.67 | 0.212 | 0.08 | 2.91 | 0.104 | 0.13 |
| Robot | 1.43 | 0.247 | 0.07 | 1.15 | 0.297 | 0.06 | 0.30 | 0.590 | 0.02 |
| Mirror | 2.99 | 0.100 | 0.14 | 0.03 | 0.874 | 0.00 | 1.17 | 0.293 | 0.06 |
| Robot × Object | 0.11 | 0.741 | 0.01 | 2.26 | 0.149 | 0.11 | 8.11 | 0.010 * | 0.30 |
| Mirror × Object | 0.92 | 0.350 | 0.05 | 0.03 | 0.868 | 0.00 | 0.20 | 0.661 | 0.01 |
| Robot × Mirror | 1.42 | 0.249 | 0.07 | 0.30 | 0.588 | 0.02 | 0.52 | 0.481 | 0.03 |
| Robot × Mirror × Object | 0.04 | 0.841 | 0.00 | 0.69 | 0.417 | 0.03 | 2.27 | 0.148 | 0.11 |
| n = 20 | Alpha | Low Beta | High Beta | |||
|---|---|---|---|---|---|---|
| Effects | Mean | SEM | Mean | SEM | Mean | SEM |
| Hand | 0.91 | 0.13 | 0.87 | 0.13 | 1.51 | 0.29 |
| Mirror | 0.74 | 0.13 | 0.55 | 0.10 | 0.93 | 0.28 |
| Robot | 0.82 | 0.12 | 0.59 | 0.09 | 0.99 | 0.25 |
| Mirror × Robot | 0.70 | 0.11 | 0.60 | 0.11 | 0.99 | 0.26 |
| Object | 0.83 | 0.12 | 0.75 | 0.14 | 1.39 | 0.33 |
| Mirror × Object | 0.67 | 0.14 | 0.74 | 0.10 | 1.23 | 0.28 |
| Robot × Object | 0.80 | 0.15 | 0.64 | 0.10 | 1.23 | 0.29 |
| Mirror × Robot × Object | 0.74 | 0.12 | 0.64 | 0.11 | 0.97 | 0.23 |
| n = 20 | Alpha | Low Beta | High Beta | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Effects | F | p-Value | ⴄ2 | F | p-Value | ⴄ2 | F | p-Value | ⴄ2 |
| Object | 0.36 | 0.553 | 0.02 | 1.33 | 0.26 | 0.07 | 2.18 | 0.156 | 0.10 |
| Robot | 0.21 | 0.654 | 0.01 | 2.86 | 0.11 | 0.13 | 4.88 | 0.040 * | 0.20 |
| Mirror | 7.61 | 0.012 * | 0.29 | 2.91 | 0.10 | 0.13 | 5.13 | 0.035 * | 0.21 |
| Robot × Object | 1.54 | 0.230 | 0.07 | 0.02 | 0.89 | 0.00 | 0.02 | 0.888 | 0.00 |
| Mirror × Object | 0.31 | 0.587 | 0.02 | 3.19 | 0.09 | 0.14 | 0.54 | 0.470 | 0.03 |
| Robot × Mirror | 0.95 | 0.341 | 0.05 | 3.02 | 0.10 | 0.14 | 1.06 | 0.317 | 0.05 |
| Robot × Mirror × Object | 0.11 | 0.746 | 0.01 | 3.86 | 0.06 | 0.17 | 4.48 | 0.048 * | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.-J.; Pei, Y.-C.; Chen, Y.-Y.; Tseng, S.-S.; Hung, J.-W. Bilateral Sensorimotor Cortical Communication Modulated by Multiple Hand Training in Stroke Participants: A Single Training Session Pilot Study. Bioengineering 2022, 9, 727. https://doi.org/10.3390/bioengineering9120727
Huang J-J, Pei Y-C, Chen Y-Y, Tseng S-S, Hung J-W. Bilateral Sensorimotor Cortical Communication Modulated by Multiple Hand Training in Stroke Participants: A Single Training Session Pilot Study. Bioengineering. 2022; 9(12):727. https://doi.org/10.3390/bioengineering9120727
Chicago/Turabian StyleHuang, Jian-Jia, Yu-Cheng Pei, Yi-Yu Chen, Shen-Shiou Tseng, and Jen-Wen Hung. 2022. "Bilateral Sensorimotor Cortical Communication Modulated by Multiple Hand Training in Stroke Participants: A Single Training Session Pilot Study" Bioengineering 9, no. 12: 727. https://doi.org/10.3390/bioengineering9120727
APA StyleHuang, J.-J., Pei, Y.-C., Chen, Y.-Y., Tseng, S.-S., & Hung, J.-W. (2022). Bilateral Sensorimotor Cortical Communication Modulated by Multiple Hand Training in Stroke Participants: A Single Training Session Pilot Study. Bioengineering, 9(12), 727. https://doi.org/10.3390/bioengineering9120727