


Gait Initiation Impairment in Patients with Parkinson’s Disease and Freezing of Gait


Abstract

1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Protocol
2.3. Biomechanical Measurements
2.3.1. Anthropometric Measurements and Base of Support
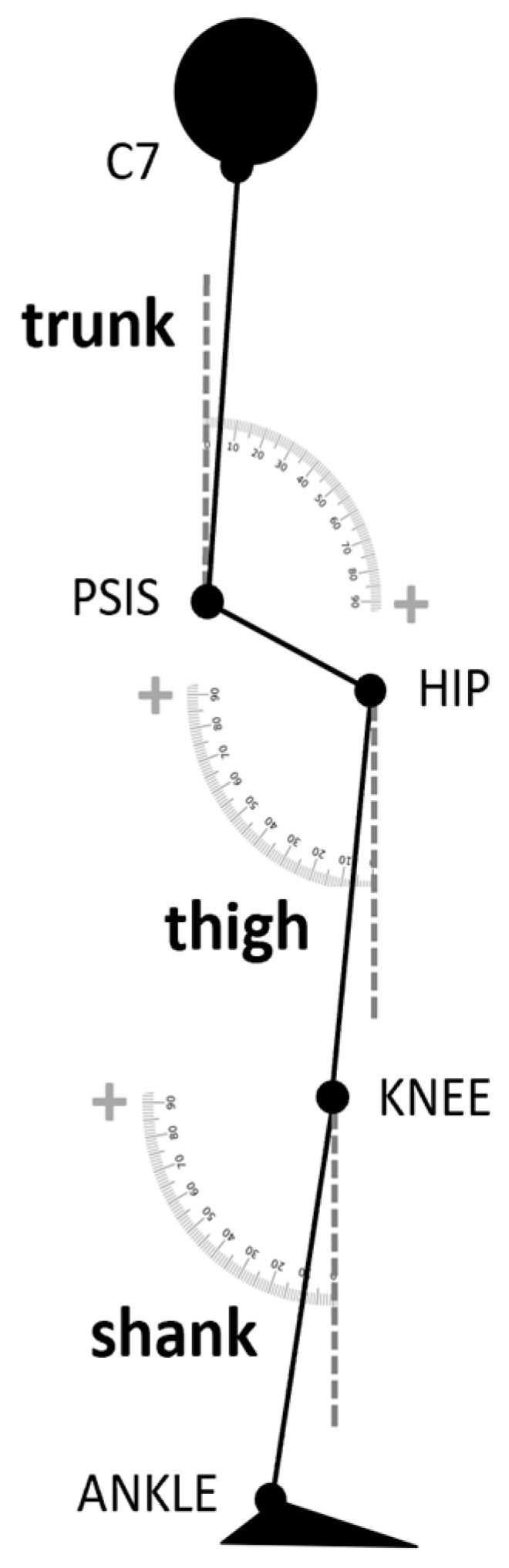
2.3.2. Postural Profile
2.3.3. Anticipatory Postural Adjustments and Gait Initiation
2.3.4. Segmental Centers of Mass
2.4. Statistical Analysis
3. Results
3.1. Selection of GI Variables

{kind=link}
{kind=link}
{kind=link}
| HC | PDNF | ||
|---|---|---|---|
| IMB duration (s) | 0.39 (0.08) | 0.38 (0.08) | 0.33 (0.09) |
| IMB displacement (mm) | 61.23 + (20.32) | 35.54 (19.71) | 23.67 + (9.94) |
| IMB displacement ML (mm) | 42.07 #,+ (13.04) | 24.04 # (13.61) | 17.76 + (8.59) |
| IMB displacement AP (mm) | 36.53 + (16.17) | 18.79 (14.75) | 9.16 + (5.93) |
| IMB average velocity (mm/s) | 163.40 #,+ (62.29) | 90.79 # (47.29) | 84.03 + (46.81) |
| IMB average velocity ML (mm/s) | 110.94 # (34.90) | 62.14 # (34.80) | 67.53 (41.47) |
| IMB average velocity AP (mm/s) | 103.36 #,+ (53.78) | 47.74 # (34.39) | 40.19 + (30.45) |
| IMB maximal velocity (mm/s) | 344.22 #,+ (149.41) | 189.88 # (113.54) | 150.41 + (64.26) |
| IMB maximal velocity ML (mm/s) | 238.29 #,+ (77.82) | 137.25 # (72.76) | 124.97 + (56.96) |
| IMB maximal velocity AP (mm/s) | 225.81 + (110.67) | 124.78 (65.52) | 101.41 + (55.74) |
| IMB end CoM velocity (m/s) | 0.09 + (0.03) | 0.06 (0.03) | 0.04 + (0.02) |
| IMB end CoP–CoM distance (m) | 0.07 + (0.02) | 0.04 (0.02) | 0.03 + (0.01) |
| UNL duration (s) | 0.36 (0.08) | 0.40 (0.08) | 0.45 (0.19) |
| UNL displacement AP (mm) | −9.67 + (15.30) | −6.25 * (18.22) | 14.69 +,* (14.70) |
| UNL average velocity (mm/s) | 465.61 (162.21) | 323.94 (131.02) | 320.34 (150.20) |
| UNL average velocity ML (mm/s) | 422.79 (148.96) | 289.26 (121.24) | 290.67 (140.81) |
| UNL average velocity AP (mm/s) | 53.11 (20.97) | 37.29 (17.16) | 46.04 (34.21) |
| UNL maximal velocity AP (mm/s) | 344.48 (154.35) | 388.76 (169.88) | 359.19 (178.76) |
| UNL end CoM velocity (m/s) | 0.21 + (0.06) | 0.16 (0.07) | 0.11 + (0.04) |
| UNL end CoM acceleration (m/s2) | 1.29 (0.33) | 1.08 (0.41) | 1.12 (0.25) |
| UNL end CoP–CoM distance (m) | 0.08 (0.03) | 0.07 (0.03) | 0.07 (0.02) |
| ST toe-off CoM velocity (m/s) | 0.86 #,+ (0.13) | 0.63 # (0.24) | 0.53 + (0.18) |
| ST toe-off CoM acceleration (m/s2) | 1.73 + (0.38) | 1.28 (0.42) | 1.08 + (0.33) |
| ST toe CoP–CoM distance (m) | 0.48 (0.32) | 0.51 (0.29) | 0.34 (0.28) |
| First step length (m) | 0.56 + (0.07) | 0.43 (0.14) | 0.33 + (0.13) |
3.2. Postural Features
3.3. Effect of PD and History of FOG on GI

3.4. Relationship between the Standing Postural Profile and the GI
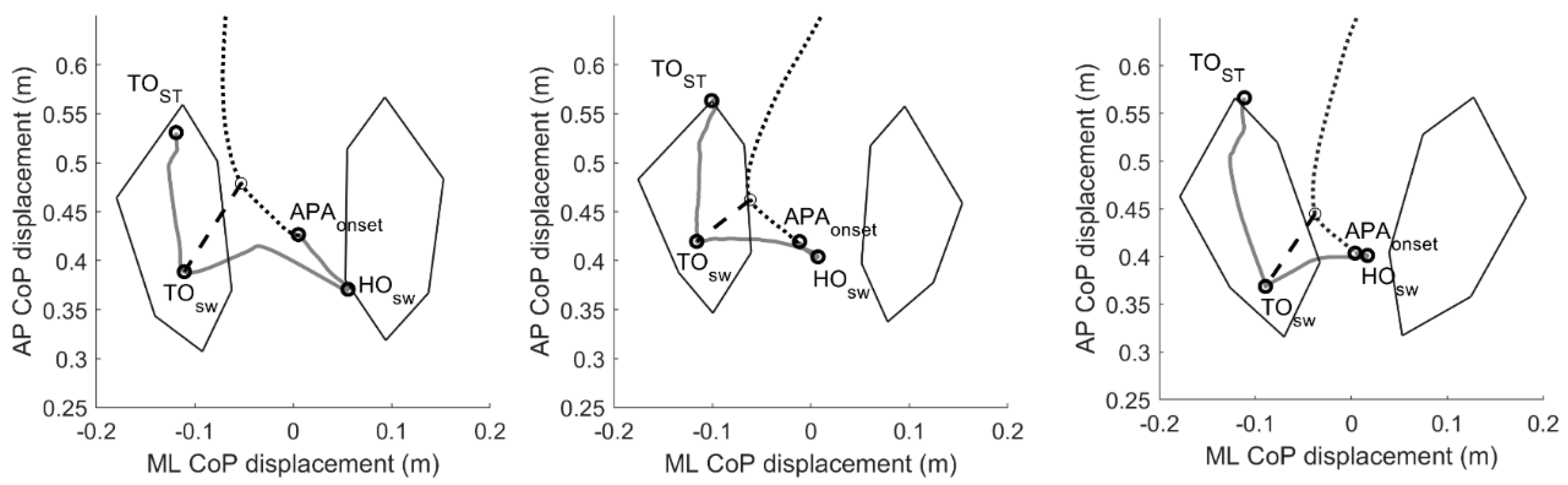
3.5. Pattern of Movements during GI
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perez-Lloret, S.; Negre-Pages, L.; Damier, P.; Delval, A.; Derkinderen, P.; Destée, A.; Meissner, W.G.; Schelosky, L.; Tison, F.; Rascol, O. Prevalence, Determinants, and Effect on Quality of Life of Freezing of Gait in Parkinson Disease. JAMA Neurol. 2014, 71, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Kerr, G.K.; Worringham, C.J.; Cole, M.H.; Lacherez, P.F.; Wood, J.M.; Silburn, P.A. Predictors of Future Falls in Parkinson Disease. Neurology 2010, 75, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Fukumoto, T.; Takatori, K.; Nagino, K.; Hiraoka, K. Abnormalities of the First Three Steps of Gait Initiation in Patients with Parkinson’s Disease with Freezing of Gait. Parkinsons. Dis. 2011, 2011, 202937. [Google Scholar] [CrossRef] [PubMed]
- Pelykh, O.; Klein, A.-M.; Bötzel, K.; Kosutzka, Z.; Ilmberger, J. Dynamics of Postural Control in Parkinson Patients with and without Symptoms of Freezing of Gait. Gait Posture 2015, 42, 246–250. [Google Scholar] [CrossRef]
- Nutt, J.G.; Bloem, B.R.; Giladi, N.; Hallett, M.; Horak, F.B.; Nieuwboer, A. Freezing of Gait: Moving Forward on a Mysterious Clinical Phenomenon. Lancet Neurol. 2011, 10, 734–744. [Google Scholar] [CrossRef]
- Yiou, E.; Caderby, T.; Delafontaine, A.; Fourcade, P.; Honeine, J.-L.L. Balance Control during Gait Initiation: State-of-the-Art and Research Perspectives. World J. Orthop. 2017, 8, 815–828. [Google Scholar] [CrossRef]
- Crenna, P.; Frigo, C. A Motor Programme for the Initiation of Foroward-Oriented Movements in Humans. J. Physiol. 1991, 437, 635–653. [Google Scholar] [CrossRef]
- Petersen, N.T.; Butler, J.E.; Marchand-Pauvert, V.; Fisher, R.; Ledebt, A.; Pyndt, H.S.; Hansen, N.L.; Nielsen, J.B. Suppression of EMG Activity by Transcranial Magnetic Stimulation in Human Subjects during Walking. J. Physiol. 2001, 537, 651–656. [Google Scholar] [CrossRef]
- Hiraoka, K.; Matuo, Y.; Iwata, A.; Onishi, T.; Abe, K. The Effects of External Cues on Ankle Control during Gait Initiation in Parkinson’s Disease. Park. Relat. Disord. 2006, 12, 97–102. [Google Scholar] [CrossRef]
- Jacobs, J.V.; Nutt, J.G.; Carlson-Kuhta, P.; Stephens, M.; Horak, F.B. Knee Trembling during Freezing of Gait Represents Multiple Anticipatory Postural Adjustments. Exp. Neurol. 2009, 215, 334–341. [Google Scholar] [CrossRef]
- Palmisano, C.; Todisco, M.; Marotta, G.; Volkmann, J.; Pacchetti, C.; Frigo, C.A.; Pezzoli, G.; Isaias, I.U. Gait Initiation in Progressive Supranuclear Palsy: Brain Metabolic Correlates. NeuroImage Clin. 2020, 28, 102408. [Google Scholar] [CrossRef]
- Palmisano, C.; Brandt, G.; Vissani, M.; Pozzi, N.G.; Canessa, A.; Brumberg, J.; Marotta, G.; Volkmann, J.; Mazzoni, A.; Pezzoli, G.; et al. Gait Initiation in Parkinson’s Disease: Impact of Dopamine Depletion and Initial Stance Condition. Front. Bioeng. Biotechnol. 2020, 8, 137. [Google Scholar] [CrossRef]
- Inglis, J.T.; Horak, F.B.; Shupert, C.L.; Jones-Rycewicz, C. The Importance of Somatosensory Information in Triggering and Scaling Automatic Postural Responses in Humans. Exp. Brain Res. 1994, 101, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Mouchnino, L.; Fontan, A.; Tandonnet, C.; Perrier, J.; Saradjian, A.; Blouin, J.; Simoneau, M. Facilitation of Cutaneous Inputs during the Planning Phase of Gait Initiation. J. Neurophysiol. 2015, 114, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Brenière, Y.; Cuong Do, M.; Bouisset, S. Are Dynamic Phenomena Prior to Stepping Essential to Walking? J. Mot. Behav. 1987, 19, 62–76. [Google Scholar] [CrossRef] [PubMed]
- Lepers, R.; Brenière, Y. The Role of Anticipatory Postural Adjustments and Gravity in Gait Initiation. Exp. Brain Res. 1995, 107, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Caderby, T.; Yiou, E.; Peyrot, N.; Begon, M.; Dalleau, G. Influence of Gait Speed on the Control of Mediolateral Dynamic Stability during Gait Initiation. J. Biomech. 2014, 47, 417–423. [Google Scholar] [CrossRef]
- Burleigh-Jacobs, A.; Horak, F.B.; Nutt, J.G.; Obeso, J.A. Step Initiation in Parkinson’s Disease: Influence of Levodopa and External Sensory Triggers. Mov. Disord. 1997, 12, 206–215. [Google Scholar] [CrossRef]
- Frank, J.S.; Horak, F.B.; Nutt, J. Centrally Initiated Postural Adjustments in Parkinsonian Patients on and off Levodopa. J. Neurophysiol. 2000, 84, 2440–2448. [Google Scholar] [CrossRef]
- Crenna, P.; Carpinella, I.; Rabuffetti, M.; Rizzone, M.; Lopiano, L.; Lanotte, M.; Ferrarin, M. Impact of Subthalamic Nucleus Stimulation on the Initiation of Gait in Parkinson’s Disease. Exp. Brain Res. 2006, 172, 519–532. [Google Scholar] [CrossRef]
- Liu, W.; McIntire, K.; Kim, S.H.; Zhang, J.; Dascalos, S.; Lyons, K.E.; Pahwa, R. Bilateral Subthalamic Stimulation Improves Gait Initiation in Patients with Parkinson’s Disease. Gait Posture 2006, 23, 492–498. [Google Scholar] [CrossRef]
- Rocchi, L.; Chiari, L.; Mancini, M.; Carlson-Kuhta, P.; Gross, A.; Horak, F.B. Step Initiation in Parkinson’s Disease: Influence of Initial Stance Conditions. Neurosci. Lett. 2006, 406, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Chastan, N.; Do, M.C.; Bonneville, F.; Torny, F.; Bloch, F.; Westby, G.W.M.; Dormont, D.; Agid, Y.; Welter, M.L. Gait and Balance Disorders in Parkinson’s Disease: Impaired Active Braking of the Fall of Centre of Gravity. Mov. Disord. 2009, 24, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Pötter-Nerger, M.; Volkmann, J. Deep Brain Stimulation for Gait and Postural Symptoms in Parkinson’s Disease. Mov. Disord. 2013, 28, 1609–1615. [Google Scholar] [CrossRef]
- Mazzone, P.; Paoloni, M.; Mangone, M.; Santilli, V.; Insola, A.; Fini, M.; Scarnati, E. Unilateral Deep Brain Stimulation of the Pedunculopontine Tegmental Nucleus in Idiopathic Parkinson’s Disease: Effects on Gait Initiation and Performance. Gait Posture 2014, 40, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa Is a Double-Edged Sword for Balance and Gait in People With Parkinson’s Disease. Mov. Disord. 2015, 30, 1361–1370. [Google Scholar] [CrossRef]
- Nonnekes, J.; Geurts, A.C.H.; Nijhuis, L.B.O.; van Geel, K.; Snijders, A.H.; Bloem, B.R.; Weerdesteyn, V. Reduced StartReact Effect and Freezing of Gait in Parkinson’s Disease: Two of a Kind? J. Neurol. 2014, 261, 943–950. [Google Scholar] [CrossRef]
- de Souza Fortaleza, A.C.; Mancini, M.; Carlson-Kuhta, P.; King, L.A.; Nutt, J.G.; Chagas, E.F.; Freitas, I.F.; Horak, F.B. Dual Task Interference on Postural Sway, Postural Transitions and Gait in People with Parkinson’s Disease and Freezing of Gait. Gait Posture 2017, 56, 76–81. [Google Scholar] [CrossRef]
- Schlenstedt, C.; Mancini, M.; Nutt, J.; Hiller, A.P.; Maetzler, W.; Deuschl, G.; Horak, F. Are Hypometric Anticipatory Postural Adjustments Contributing to Freezing of Gait in Parkinson’s Disease? Front. Aging Neurosci. 2018, 10, 36. [Google Scholar] [CrossRef]
- Cohen, R.G.; Nutt, J.G.; Horak, F.B. Recovery from Multiple APAs Delays Gait Initiation in Parkinson’s Disease. Front. Hum. Neurosci. 2017, 11, 60. [Google Scholar] [CrossRef]
- Bayot, M.; Delval, A.; Moreau, C.; Defebvre, L.; Hansen, C.; Maetzler, W.; Schlenstedt, C. Initial Center of Pressure Position Prior to Anticipatory Postural Adjustments during Gait Initiation in People with Parkinson’s Disease with Freezing of Gait. Park. Relat. Disord. 2021, 84, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Dalton, E.; Bishop, M.; Tillman, M.D.; Hass, C.J. Simple Change in Initial Standing Position Enhances the Initiation of Gait. Med. Sci. Sports Exerc. 2011, 43, 2352–2358. [Google Scholar] [CrossRef] [PubMed]
- Leteneur, S.; Simoneau, E.; Gillet, C.; Dessery, Y.; Barbier, F. Trunk’s Natural Inclination Influences Stance Limb Kinetics, but Not Body Kinematics, during Gait Initiation in Able Men. PLoS ONE 2013, 8, e55256. [Google Scholar] [CrossRef]
- Fortin, A.P.; Dessery, Y.; Leteneur, S.; Barbier, F.; Corbeil, P. Effect of Natural Trunk Inclination on Variability in Soleus Inhibition and Tibialis Anterior Activation during Gait Initiation in Young Adults. Gait Posture 2015, 41, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Fawver, B.; Roper, J.A.; Sarmento, C.; Hass, C.J. Forward Leaning Alters Gait Initiation Only at Extreme Anterior Postural Positions. Hum. Mov. Sci. 2018, 59, 1–11. [Google Scholar] [CrossRef]
- Yoshii, F.; Moriya, Y.; Ohnuki, T.; Ryo, M.; Takahashi, W. Postural Deformities in Parkinson’s Disease–Mutual Relationships among Neck Flexion, Fore-Bent, Knee-Bent and Lateral-Bent Angles and Correlations with Clinical Predictors. J. Clin. Mov. Disord. 2016, 3, 1. [Google Scholar] [CrossRef]
- Delafontaine, A.; Gagey, O.; Colnaghi, S.; Do, M.C.; Honeine, J.L. Rigid Ankle Foot Orthosis Deteriorates Mediolateral Balance Control and Vertical Braking during Gait Initiation. Front. Hum. Neurosci. 2017, 11, 214. [Google Scholar] [CrossRef]
- Stansfield, B.; Hawkins, K.; Adams, S.; Church, D. Spatiotemporal and Kinematic Characteristics of Gait Initiation across a Wide Speed Range. Gait Posture 2018, 61, 331–338. [Google Scholar] [CrossRef]
- Ferrari, A.; Benedetti, M.G.; Pavan, E.; Frigo, C.; Bettinelli, D.; Rabuffetti, M.; Crenna, P.; Leardini, A. Quantitative Comparison of Five Current Protocols in Gait Analysis. Gait Posture 2008, 28, 207–216. [Google Scholar] [CrossRef]
- Isaias, I.U.; Dipaola, M.; Michi, M.; Marzegan, A.; Volkmann, J.; Roidi, M.L.R.; Frigo, C.A.; Cavallari, P. Gait Initiation in Children with Rett Syndrome. PLoS ONE 2014, 9, e92736. [Google Scholar] [CrossRef]
- Palmisano, C.; Brandt, G.; Pozzi, N.G.; Alice, L.; Maltese, V.; Andrea, C.; Jens, V.; Pezzoli, G.; Frigo, C.A.; Isaias, I.U. Sit-to-Walk Performance in Parkinson’s Disease: A Comparison between Faller and Non-Faller Patients. Clin. Biomech. 2019, 63, 140–146. [Google Scholar] [CrossRef]
- Muniz, A.M.S.; Nadal, J.; Lyons, K.E.; Pahwa, R.; Liu, W. Long-Term Evaluation of Gait Initiation in Six Parkinson’s Disease Patients with Bilateral Subthalamic Stimulation. Gait Posture 2012, 35, 452–457. [Google Scholar] [CrossRef]
- Zatsiorsky, V.M. Kinematics of Human Motion; Human Kinetics: Champaign, IL, USA, 1998. [Google Scholar]
- Dipaola, M.; Pavan, E.E.; Cattaneo, A.; Frazzitta, G.; Pezzoli, G.; Cavallari, P.; Frigo, C.A.; Isaias, I.U. Mechanical Energy Recovery during Walking in Patients with Parkinson Disease. PLoS ONE 2016, 11, e0156420. [Google Scholar] [CrossRef]
- Martin, M.; Shinberg, M.; Kuchibhatla, M.; Ray, L.; Carollo, J.J.; Schenkman, M.L. Gait Initiation in Community-Dwelling Adults with Parkinson Disease: Comparison with Older and Younger Adults without the Disease. Phys. Ther. 2002, 82, 566–577. [Google Scholar] [CrossRef]
- Rosin, R.; Topka, H.; Dichgans, J. Gait Initiation in Parkinson’s Disease. Mov. Disord. 1997, 12, 682–690. [Google Scholar] [CrossRef]
- Mahalanobis, P.C. On the Generalized Distance in Statistics. Proc. Natl. Inst. Sci. India 1936, 2, 49–55. [Google Scholar]
- Farinelli, V.; Hosseinzadeh, L.; Palmisano, C.; Frigo, C. An Easily Applicable Method to Analyse the Ankle-Foot Power Absorption and Production during Walking. Gait Posture 2019, 71, 56–61. [Google Scholar] [CrossRef]
- O’Malley, M.J. Normalization of Temporal-Distance Parameters in Pediatric Gait. J. Biomech. 1996, 29, 619–625. [Google Scholar] [CrossRef]
- Crenna, P.; Carpinella, I.; Rabuffetti, M.; Calabrese, E.; Mazzoleni, P.; Nemni, R.; Ferrarin, M. The Association between Impaired Turning and Normal Straight Walking in Parkinson’s Disease. Gait Posture 2007, 26, 172–178. [Google Scholar] [CrossRef]
- Halliday, S.E.; Winter, D.A.; Frank, J.S.; Patla, A.E.; Prince, F. The Initiation of Gait in Young, Elderly, and Parkinson’s Disease Subjects. Gait Posture 1998, 8, 8–14. [Google Scholar] [CrossRef]
- Dibble, L.E.; Nicholson, D.E.; Shultz, B.; MacWilliams, B.A.; Marcus, R.L.; Moncur, C. Sensory Cueing Effects on Maximal Speed Gait Initiation in Persons with Parkinson’s Disease and Healthy Elders. Gait Posture 2004, 19, 215–225. [Google Scholar] [CrossRef]
- Plate, A.; Klein, K.; Pelykh, O.; Singh, A.; Bötzel, K. Anticipatory Postural Adjustments Are Unaffected by Age and Are Not Absent in Patients with the Freezing of Gait Phenomenon. Exp. Brain Res. 2016, 234, 2609–2618. [Google Scholar] [CrossRef]
- Schlenstedt, C.; Mancini, M.; Horak, F.; Peterson, D. Anticipatory Postural Adjustment During Self-Initiated, Cued, and Compensatory Stepping in Healthy Older Adults and Patients With Parkinson Disease. Arch. Phys. Med. Rehabil. 2017, 98, 1316–1324.e1. [Google Scholar] [CrossRef]
- Heilbron, M.; Scholten, M.; Schlenstedt, C.; Mancini, M.; Schöllmann, A.; Cebi, I.; Pötter-Nerger, M.; Gharabaghi, A.; Weiss, D. Anticipatory Postural Adjustmens Are Modulated by Substantia Nigra Stimulation in People with Parkinson’s Disease and Freezing of Gait. Park. Relat. Disord. 2019, 66, 34–39. [Google Scholar] [CrossRef]
- Lee, K.M.; Chang, K.H.; Roh, J.K. Subregions within the Supplementary Motor Area Activated at Different Stages of Movement Preparation and Execution. Neuroimage 1999, 9, 117–123. [Google Scholar] [CrossRef]
- Jacobs, J.V.; Lou, J.S.; Kraakevik, J.A.; Horak, F.B. The Supplementary Motor Area Contributes to the Timing of the Anticipatory Postural Adjustment during Step Initiation in Participants with and without Parkinson’s Disease. Neuroscience 2009, 164, 877–885. [Google Scholar] [CrossRef]
- Bolzoni, F.; Bruttini, C.; Esposti, R.; Castellani, C.; Cavallari, P. Transcranial Direct Current Stimulation of SMA Modulates Anticipatory Postural Adjustments without Affecting the Primary Movement. Behav. Brain Res. 2015, 291, 407–413. [Google Scholar] [CrossRef]
- Varghese, J.P.; Merino, D.M.; Beyer, K.B.; McIlroy, W.E. Cortical Control of Anticipatory Postural Adjustments Prior to Stepping. Neuroscience 2016, 313, 99–109. [Google Scholar] [CrossRef]
- Richard, A.; Van Hamme, A.; Drevelle, X.; Golmard, J.L.; Meunier, S.; Welter, M.L. Contribution of the Supplementary Motor Area and the Cerebellum to the Anticipatory Postural Adjustments and Execution Phases of Human Gait Initiation. Neuroscience 2017, 358, 181–189. [Google Scholar] [CrossRef]
- Morris, G.; Nevet, A.; Arkadir, D.; Vaadia, E.; Bergman, H. Midbrain Dopamine Neurons Encode Decisions for Future Action. Nat. Neurosci. 2006, 9, 1057–1063. [Google Scholar] [CrossRef]
- Mazzoni, P.; Hristova, A.; Krakauer, J.W. Why Don’t We Move Faster? Parkinson’s Disease, Movement Vigor, and Implicit Motivation. J. Neurosci. 2007, 27, 7105–7116. [Google Scholar] [CrossRef]
- Gepshtein, S.; Li, X.; Snider, J.; Plank, M.; Lee, D.; Poizner, H. Dopamine Function and the Efficiency of Human Movement. J. Cogn. Neurosci. 2014, 26, 645–657. [Google Scholar] [CrossRef]
- Schultz, W. Multiple Dopamine Functions at Different Time Courses. Annu. Rev. Neurosci. 2007, 30, 259–288. [Google Scholar] [CrossRef]
- Ruget, H.; Blouin, J.; Teasdale, N.; Mouchnino, L. Can Prepared Anticipatory Postural Adjustments Be Updated by Proprioception? Neuroscience 2008, 155, 640–648. [Google Scholar] [CrossRef]
- Lhomond, O.; Teasdale, N.; Simoneau, M.; Mouchnino, L. Supplementary Motor Area and Superior Parietal Lobule Restore Sensory Facilitation Prior to Stepping When a Decrease of Afferent Inputs Occurs. Front. Neurol. 2018, 9, 1132. [Google Scholar] [CrossRef]
- Picard, N.; Strick, P.L. Imaging the Premotor Areas. Curr. Opin. Neurobiol. 2001, 11, 663–672. [Google Scholar] [CrossRef]
- Tard, C.; Delval, A.; Devos, D.; Lopes, R.; Lenfant, P.; Dujardin, K.; Hossein-Foucher, C.; Semah, F.; Duhamel, A.; Defebvre, L.; et al. Brain Metabolic Abnormalities during Gait with Freezing in Parkinson’s Disease. Neuroscience 2015, 307, 281–301. [Google Scholar] [CrossRef]
- Wolbers, T.; Hegarty, M.; Büchel, C.; Loomis, J.M. Spatial Updating: How the Brain Keeps Track of Changing Object Locations during Observer Motion. Nat. Neurosci. 2008, 11, 1223–1230. [Google Scholar] [CrossRef]
- Hanakawa, T.; Fukuyama, H.; Katsumi, Y.; Honda, M.; Shibasaki, H. Enhanced Lateral Premotor Activity during Paradoxical Gait in Parkinson’s Disease. Ann. Neurol. 1999, 45, 329–336. [Google Scholar] [CrossRef]
- Voss, M.; Ingram, J.N.; Haggard, P.; Wolpert, D.M. Sensorimotor Attenuation by Central Motor Command Signals in the Absence of Movement. Nat. Neurosci. 2006, 9, 26–27. [Google Scholar] [CrossRef]
- Jacobs, J.V.; Horak, F.B. External Postural Perturbations Induce Multiple Anticipatory Postural Adjustments When Subjects Cannot Pre-Select Their Stepping Foot. Exp. brain Res. 2007, 179, 29–42. [Google Scholar] [CrossRef]
- Amboni, M.; Cozzolino, A.; Longo, K.; Picillo, M.; Barone, P. Freezing of Gait and Executive Functions in Patients with Parkinson’s Disease. Mov. Disord. 2008, 23, 395–400. [Google Scholar] [CrossRef]
- Naismith, S.L.; Shine, J.M.; Lewis, S.J.G. The Specific Contributions of Set-Shifting to Freezing of Gait in Parkinson’s Disease. Mov. Disord. 2010, 25, 1000–1004. [Google Scholar] [CrossRef]
- Heremans, E.; Nieuwboer, A.; Vercruysse, S. Freezing of Gait in Parkinson’s Disease: Where Are We Now? Topical Collection on Movement Disorders. Curr. Neurol. Neurosci. Rep. 2013, 13, 350. [Google Scholar] [CrossRef]
- Cohen, R.G.; Klein, K.A.; Nomura, M.; Fleming, M.; Mancini, M.; Giladi, N.; Nutt, J.G.; Horak, F.B. Inhibition, Executive Function, and Freezing of Gait. J. Parkinsons. Dis. 2014, 4, 111–122. [Google Scholar] [CrossRef]
- Lira, J.L.O.; Ugrinowitsch, C.; Coelho, D.B.; Teixeira, L.A.; de Lima-Pardini, A.C.; Magalhães, F.H.; Barbosa, E.R.; Horak, F.B.; Silva-Batista, C. Loss of Presynaptic Inhibition for Step Initiation in Parkinsonian Individuals with Freezing of Gait. J. Physiol. 2020, 598, 1611–1624. [Google Scholar] [CrossRef]
- Drucker, J.H.; Sathian, K.; Crosson, B.; Krishnamurthy, V.; McGregor, K.M.; Bozzorg, A.; Gopinath, K.; Krishnamurthy, L.C.; Wolf, S.L.; Hart, A.R.; et al. Internally Guided Lower Limb Movement Recruits Compensatory Cerebellar Activity in People with Parkinson’s Disease. Front. Neurol. 2019, 10, 573. [Google Scholar] [CrossRef]
- Avanzino, L.; Pelosin, E.; Vicario, C.M.; Lagravinese, G.; Abbruzzese, G.; Martino, D. Time Processing and Motor Control in Movement Disorders. Front. Hum. Neurosci. 2016, 10, 631. [Google Scholar] [CrossRef]
- Isaias, I.U.; Brumberg, J.; Pozzi, N.G.; Palmisano, C.; Canessa, A.; Marotta, G.; Volkmann, J.; Pezzoli, G. Brain Metabolic Alterations Herald Falls in Patients with Parkinson’s Disease. Ann. Clin. Transl. Neurol. 2020, 7, 579–583. [Google Scholar] [CrossRef]
- Lipski, W.J.; Wozny, T.A.; Alhourani, A.; Kondylis, E.D.; Turner, R.S.; Crammond, D.J.; Richardson, R.M. Dynamics of Human Subthalamic Neuron Phase-Locking to Motor and Sensory Cortical Oscillations during Movement. J. Neurophysiol. 2017, 118, 1472–1487. [Google Scholar] [CrossRef]
- Arnulfo, G.; Pozzi, N.G.; Palmisano, C.; Leporini, A.; Canessa, A.; Brumberg, J.; Pezzoli, G.; Matthies, C.; Volkmann, J.; Isaias, I.U. Phase Matters: A Role for the Subthalamic Network during Gait. PLoS ONE 2018, 13, e0198691. [Google Scholar] [CrossRef]
- Georgiades, M.J.; Shine, J.M.; Gilat, M.; McMaster, J.; Owler, B.; Mahant, N.; Lewis, S.J.G. Hitting the Brakes: Pathological Subthalamic Nucleus Activity in Parkinson’s Disease Gait Freezing. Brain 2019, 142, 3906–3916. [Google Scholar] [CrossRef]
- Pozzi, N.G.; Canessa, A.; Palmisano, C.; Brumberg, J.; Steigerwald, F.; Reich, M.M.; Minafra, B.; Pacchetti, C.; Pezzoli, G.; Volkmann, J.; et al. Freezing of Gait in Parkinson’s Disease Reflects a Sudden Derangement of Locomotor Network Dynamics. Brain 2019, 142, 2037–2050. [Google Scholar] [CrossRef]

| Description | Decomposition |
|---|---|
| Anthropometric measurements (AMs) | |
| Body Height [BH] (cm) | |
| Inter Anterior Superior Iliac Spine Distance [IAD] (cm) | |
| Limb Length [LL] (cm) | |
| Foot Length [FL] (cm) | |
| Body Mass [BM] (kg) | |
| Body Mass Index [BMI] (kg/cm2) | |
| Base of support (BoS) | |
| BoS Area (cm2): area of the polygon described by the markers placed on the heels, the lateral malleoli, the fifth metatarsal bones, and the hallux | |
| BoS Width (cm): distance between the ankle joint centers, estimated as the mid points between the lateral and medial malleoli | |
| Foot Alignment (cm): AP distance between the two markers placed on the heels | |
| βΔ: Difference between the left (βL) and right (βR) feet extra-rotation angles (angles between the axis passing through the lateral and medial malleoli and the horizontal axis of the reference system of the laboratory) (°) | |
| β: BoS opening angle, sum of βL and βR (°) | |
| Postural angles | |
| Angle between the line connecting the markers on the middle point between the PSIS and the C7 and the laboratory vertical axis (°) | |
| Angle between the line connecting the knee and hip centers of rotation and the laboratory vertical axis (°) | |
| Angle between the line connecting the knee and ankle centers of rotation and the laboratory vertical axis (°) | |
| GI measurements—Imbalance (IMB) | |
| IMB duration (s) | |
| IMB CoP displacement (mm) | AP, ML |
| IMB CoP average velocity (mm/s) | AP, ML |
| IMB CoP maximal velocity (mm/s) | AP, ML |
| CoM velocity at IMB end (m/s) | |
| CoM acceleration at IMB end (m/s2) | |
| CoP–CoM distance at IMB end (m) | |
| Orientation of CoP–CoM vector with respect to the progression line at IMB end (°) | |
| GI measurements—Unloading (UNL) | |
| CoP distance from the line passing through the markers on the heels at swing heel off (mm) | AP |
| UNL duration (s) | |
| UNL CoP displacement (mm) | AP, ML |
| UNL CoP average velocity (mm/s) | AP, ML |
| UNL CoP maximal velocity (mm/s) | AP, ML |
| CoM velocity at UNL end (m/s) | |
| CoM acceleration at UNL end (m/s2) | |
| CoP–CoM distance at UNL end (m) | |
| Slope of CoP–CoM vector at UNL end (°) | |
| GI measurements—Stepping phase | |
| CoP distance from the line passing through the markers on the heels at the swing foot toe-off (mm) | AP |
| CoM velocity at stance foot toe-off (m/s) | |
| CoM acceleration at stance foot toe-off (m/s2) | |
| CoP–CoM distance at stance toe-off (m) | |
| First step length (m) | |
| First step average velocity (m/s) | |
| First step maximal velocity (m/s) | |
| HC | PDNF | |||
|---|---|---|---|---|
| Demographic features | Gender (males/total) | 14/23 (~61%) | 10/20 (50%) | 14/23 (~61%) |
| Age (years) | 61.17 (4.93) | 63.32 (10.76) | 63.83 (8.34) | |
| Clinical data | Disease duration (years) | (-) | 9.26 (3.89) | 11.14 (3.47) |
| Hoen and Yahr (I–V stage) | (-) | 2.24 (0.42) | 2.39 (0.50) | |
| UPDRS-III (0–108 score) | (-) | 24.81 (9.43) | 28.05 (9.96) | |
| LEDD (mg) | (-) | 741.18 (221.26) | 803.70 (358.33) | |
| Anthropometric Measurements | BH (cm) | 169.94 (10.53) | 167.79 (11.05) | 168.09 (11.44) |
| LL (cm) | 88.81 (5.37) | 88.23 (7.81) | 87.21 (5.84) | |
| FL (cm) | 24.93 (1.66) | 25.17 (1.58) | 24.59 (1.65) | |
| BM (kg) | 72.28 (11.11) | 66.36 (13.01) | 72.02 (14.83) | |
| BMI (kg/cm2) | 24.59 (3.02) | 23.00 (3.99) | 24.89 (5.18) | |
| IAD (cm) | 27.76 (2.35) | 27.89 (2.53) | 27.42 (3.40) | |
| Base of Support | BoS area (cm2) | 685.24 (91.56) | 668.18 (75.19) | 651.85 (114.90) |
| BoS width (cm) | 17.64 (4.10) | 16.26 (2.78) | 15.67 (2.59) | |
| Foot alignment (cm) | 6.57 (3.36) | 8.37 (4.54) | 6.92 (3.76) | |
| Angle difference βΔ (°) | 6.66 (3.29) | 4.67 (2.58) | 7.75 (4.98) | |
| BoS opening angle β (°) | 40.67 (15.76) | 37.25 (14.05) | 43.56 (13.92) | |
| HC | PDNF | ||
|---|---|---|---|
| Trunk (°) | 4.08 #,+ (2.43) | 9.06 # (4.37) | 12.58 + (5.65) |
| Thigh (°) | 6.31 #,+ (2.69) | 0.54 # (3.70) | −0.48 + (4.00) |
| Shank (°) | 9.22 (2.93) | 10.67 (2.77) | 10.95 (2.47) |
| Spearman’s ρ | p-Value | ||
|---|---|---|---|
| Shank (°) | IMB average velocity (mm/s) | 0.32 | 0.014 |
| IMB average velocity AP (mm/s) | 0.31 | 0.016 | |
| IMB maximal velocity AP (mm/s) | 0.38 | 0.003 | |
| Segmental Center of Mass | HC | PDNF | |
|---|---|---|---|
| Pelvis (%) | 60.62 (9.27) | 62.47 (13.74) | 62.66 (21.69) |
| Thigh ST (%) | 65.76 (10.75) | 71.72 (20.13) | 63.39 (19.97) |
| Shank ST (%) | 71.17 (14.36) | 68.57 (19.98) | 65.73 (21.95) |
| Foot ST (%) | 68.37 (10.46) | 77.24 (22.53) | 65.02 (22.87) |
| Thigh SW (%) | 62.67 (9.23) | 64.75 (15.47) | 55.85 (18.80) |
| Shank SW (%) | 74.21 (13.85) | 75.35 (24.26) | 67.26 (19.36) |
| Foot SW (%) | 69.15 (15.41) | 64.63 (16.55) | 59.20 (19.86) |
| Chest (%) | 73.48 (14.29) | 74.47 (26.12) | 69.22 (19.85) |
| Abdomen (%) | 79.50 (13.87) | 81.57 (25.30) | 57.88 (20.58) |
| Arm ST (%) | 55.49 (18.27) | 65.80 (26.63) | 54.17 (19.98) |
| Arm SW (%) | 62.71 (9.34) | 65.08 (13.49) | 56.57 (17.72) |
| Forearm ST (%) | 38.98 (12.65) | 53.73 (24.00) | 39.40 (12.69) |
| Forearm SW (%) | 51.34 (11.80) | 62.57 (13.59) | 47.26 (13.34) |
| Hand ST (%) | 44.37 (19.82) | 49.64 (21.32) | 41.99 (30.95) |
| Hand SW (%) | 34.36 (13.06) | 46.93 (19.96) | 47.71 (16.69) |
| Head (%) | 54.33 (11.81) | 58.15 (14.06) | 60.06 (18.41) |
| Rank-Ordered Segmental Center of Mass | HC | PDNF | |
|---|---|---|---|
| 1st segment (%) | 27.88 (10.66) | 35.42 (13.61) | 26.51 (11.98) |
| 2nd segment (%) | 36.33 (10.40) | 45.51 (15.10) | 34.90 (13.48) |
| 3rd segment (%) | 42.62 (9.68) | 50.70 (14.76) | 41.43 (12.61) |
| 4th segment (%) | 46.70 (8.60) | 54.47 (14.37) | 44.29 (13.88) |
| 5th segment (%) | 50.58 (8.32) | 57.41 (12.53) | 46.68 (14.44) |
| 6th segment (%) | 54.40 (6.50) | 59.49 (13.25) | 49.54 (15.11) |
| 7th segment (%) | 57.49 (6.79) | 61.70 (14.11) | 51.87 (14.85) |
| 8th segment (%) | 59.71 (7.51) | 64.81 (15.85) | 54.13 (15.05) |
| 9th segment (%) | 61.31 (8.04) | 66.18 (16.05) | 55.93 (15.08) |
| 10th segment (%) | 62.94 (7.84) | 67.59 (16.18) | 58.10 (14.84) |
| 11th segment (%) | 65.75 (9.10) | 68.86 (16.49) | 60.79 (14.94) |
| 12th segment (%) | 67.89 (9.02) | 70.65 (17.45) | 62.66 (15.16) |
| 13th segment (%) | 70.64 (10.11) | 72.32 (18.32) | 65.83 (14.82) |
| 14th segment (%) | 73.91 (10.70) | 74.85 (19.26) | 68.93 (16.35) |
| 15th segment (%) | 78.42 (11.79) | 78.81 (21.00) | 74.20 (15.35) |
| 16th segment (%) | 84.95 (11.99) | 83.19 (23.21) | 82.42 (18.88) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmisano, C.; Beccaria, L.; Haufe, S.; Volkmann, J.; Pezzoli, G.; Isaias, I.U. Gait Initiation Impairment in Patients with Parkinson’s Disease and Freezing of Gait. Bioengineering 2022, 9, 639. https://doi.org/10.3390/bioengineering9110639
Palmisano C, Beccaria L, Haufe S, Volkmann J, Pezzoli G, Isaias IU. Gait Initiation Impairment in Patients with Parkinson’s Disease and Freezing of Gait. Bioengineering. 2022; 9(11):639. https://doi.org/10.3390/bioengineering9110639
Chicago/Turabian StylePalmisano, Chiara, Laura Beccaria, Stefan Haufe, Jens Volkmann, Gianni Pezzoli, and Ioannis U. Isaias. 2022. "Gait Initiation Impairment in Patients with Parkinson’s Disease and Freezing of Gait" Bioengineering 9, no. 11: 639. https://doi.org/10.3390/bioengineering9110639
APA StylePalmisano, C., Beccaria, L., Haufe, S., Volkmann, J., Pezzoli, G., & Isaias, I. U. (2022). Gait Initiation Impairment in Patients with Parkinson’s Disease and Freezing of Gait. Bioengineering, 9(11), 639. https://doi.org/10.3390/bioengineering9110639