Impact of Coping Veneering Techniques on the Survival of Implant-Supported Zirconia-Based-Crowns Cemented to Hybrid-Abutments: An-In-Vitro Study


Abstract
1. Introduction
2. Materials and Methods
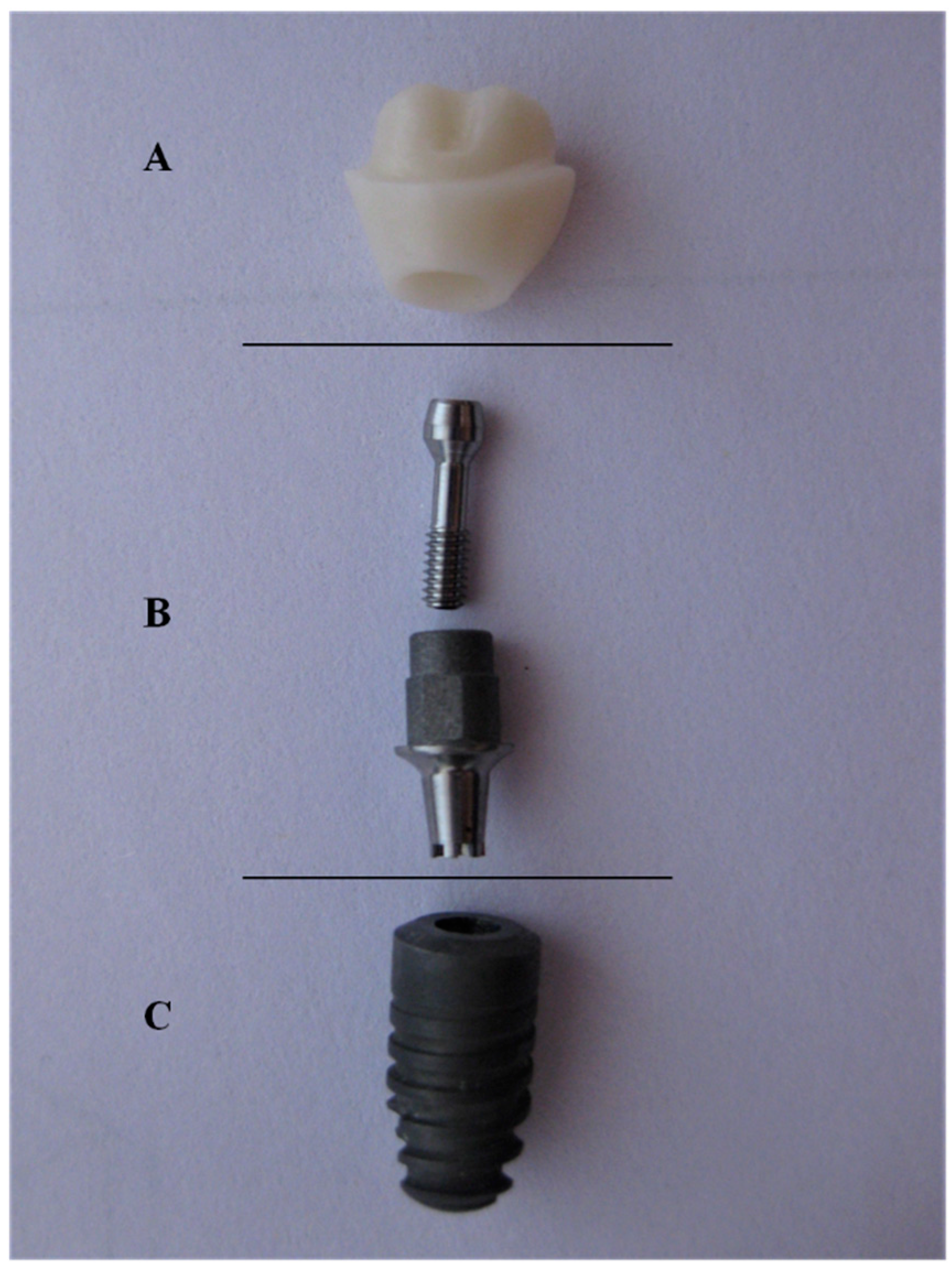
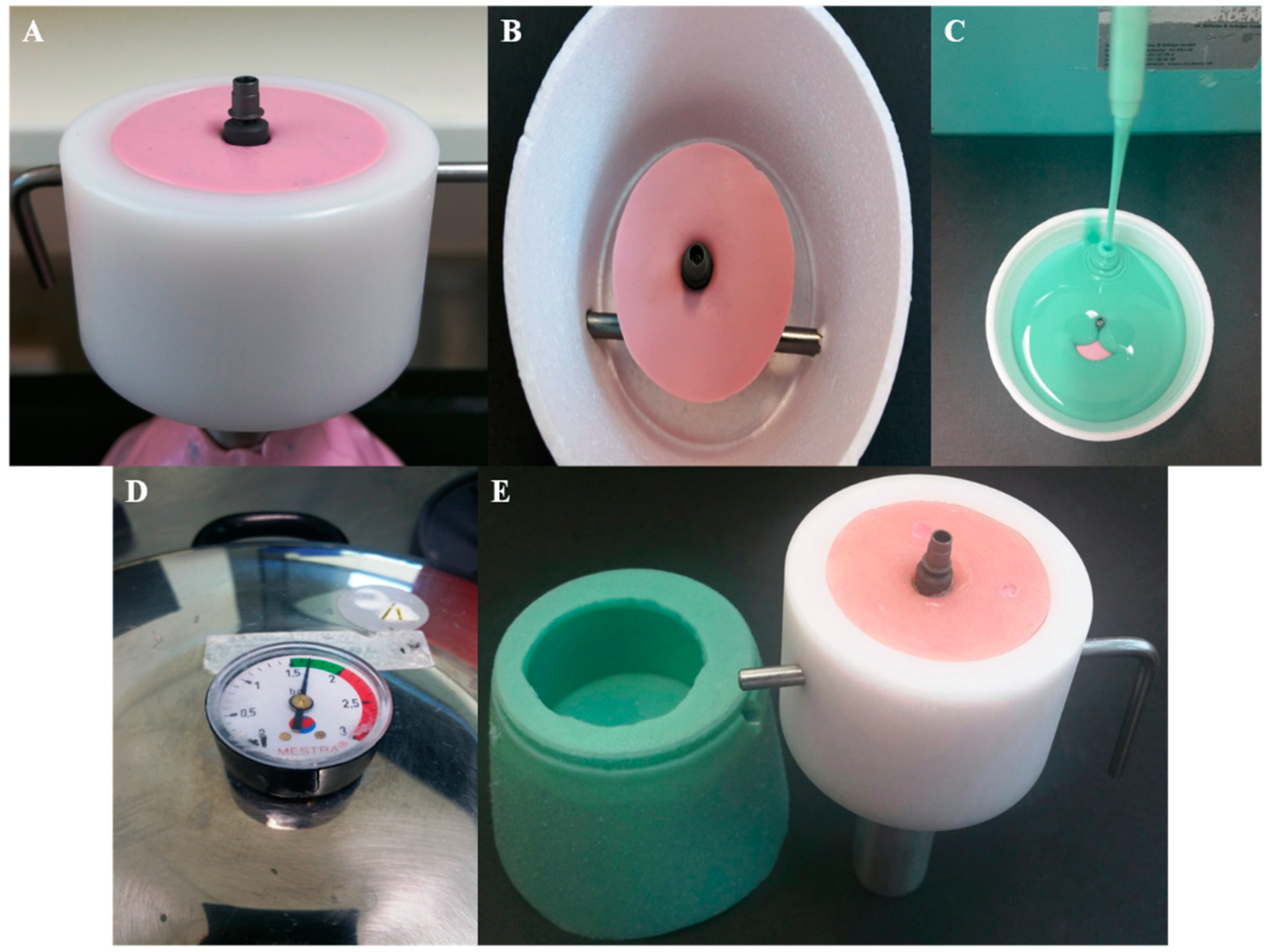
2.1. Sample Preparation
2.1.1. Manufacturing Process for CAD-On Crowns (LD)
2.1.2. Manufacturing Process for Hand-Layered Crowns (HL)
2.2. In-Vitro Testing
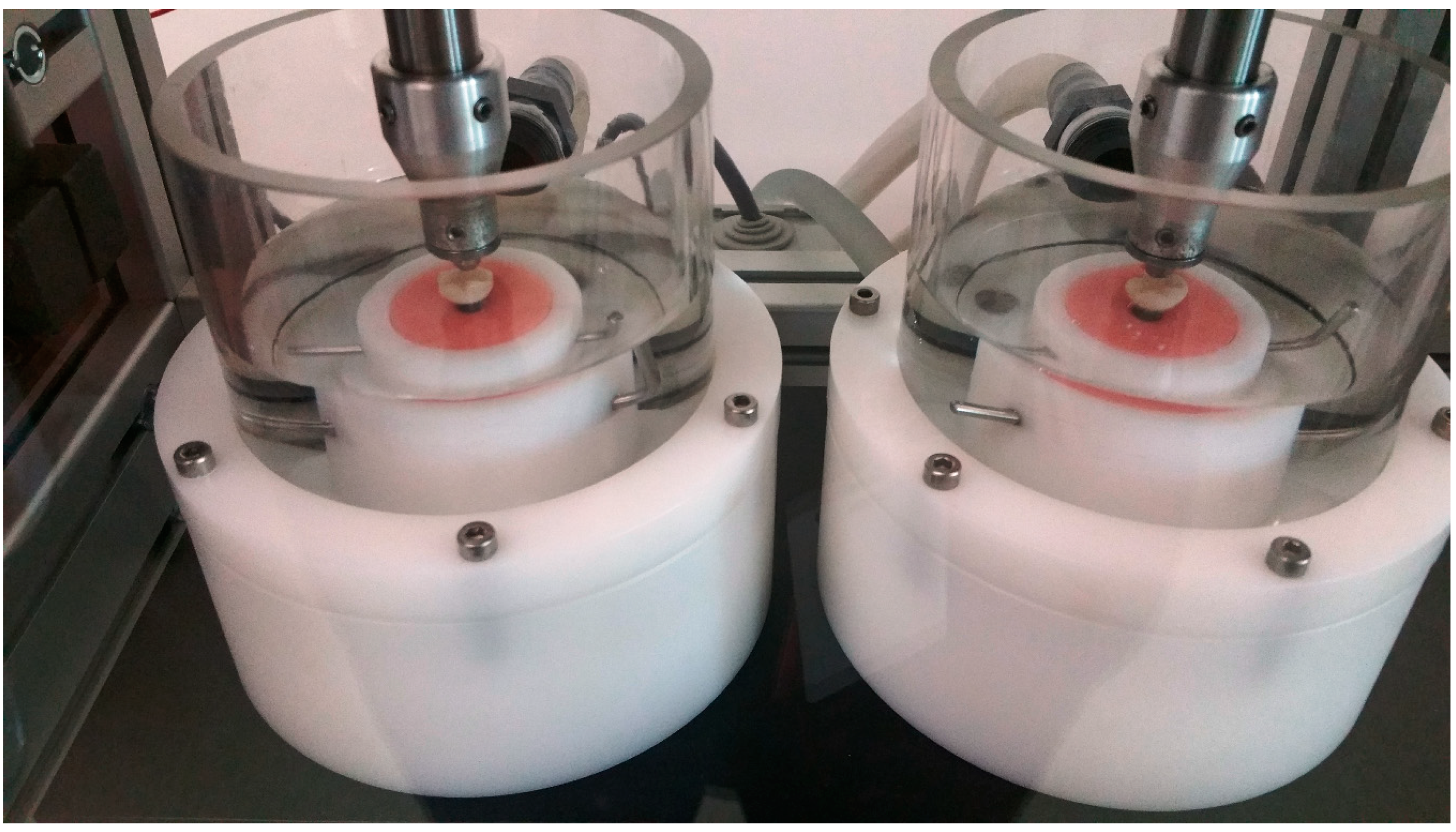
2.2.1. Thermal Cycling Mechanical Loading (Fatigue)
2.2.2. Compressive Static Load to Fracture Testing (SLF)
2.3. Scanning Electron Microscopy (SEM)
2.4. Statistical Analysis
3. Results
3.1. Thermal Cycling Mechanical Loading (Fatigue)
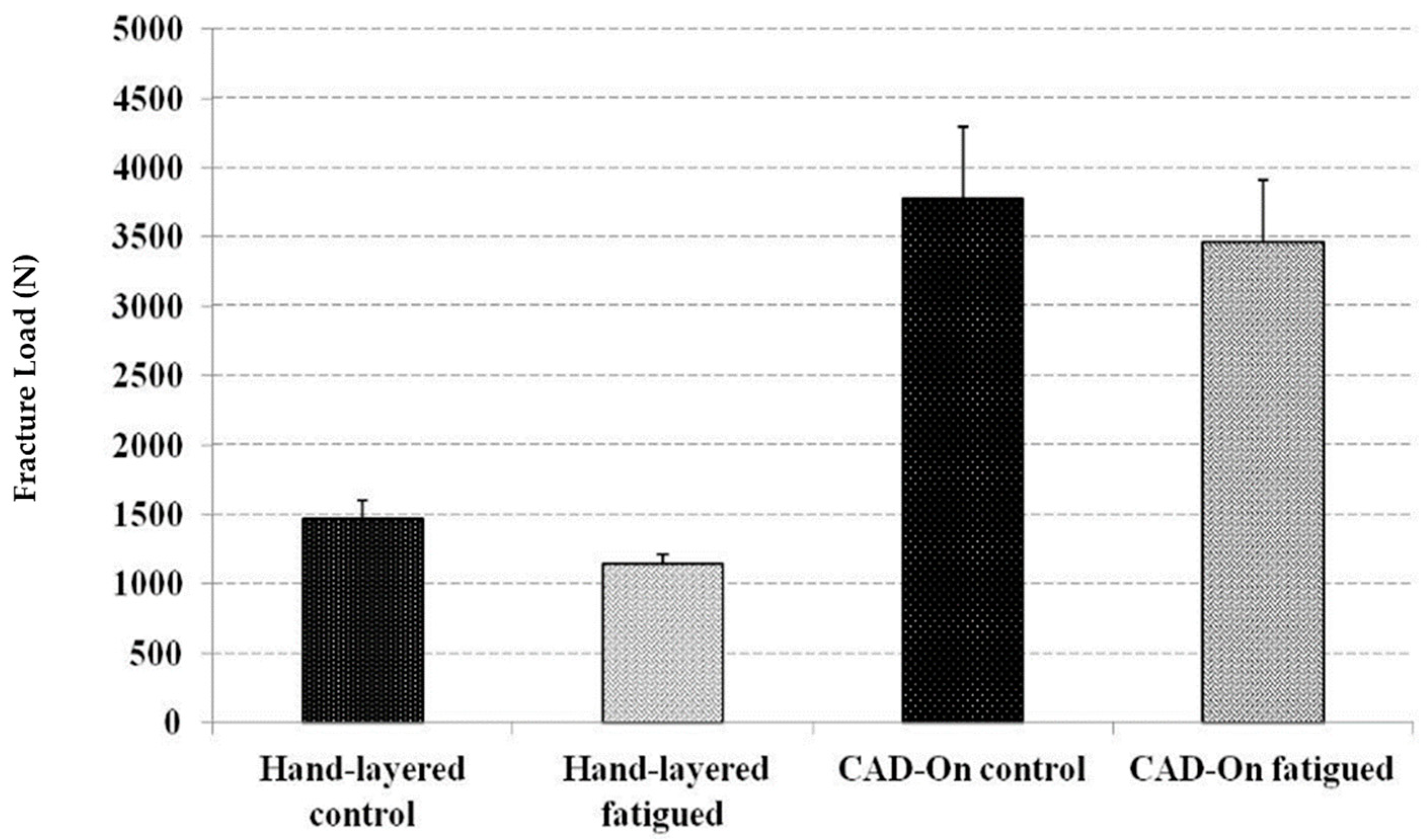
3.2. Static Load to Fracture (SLF)
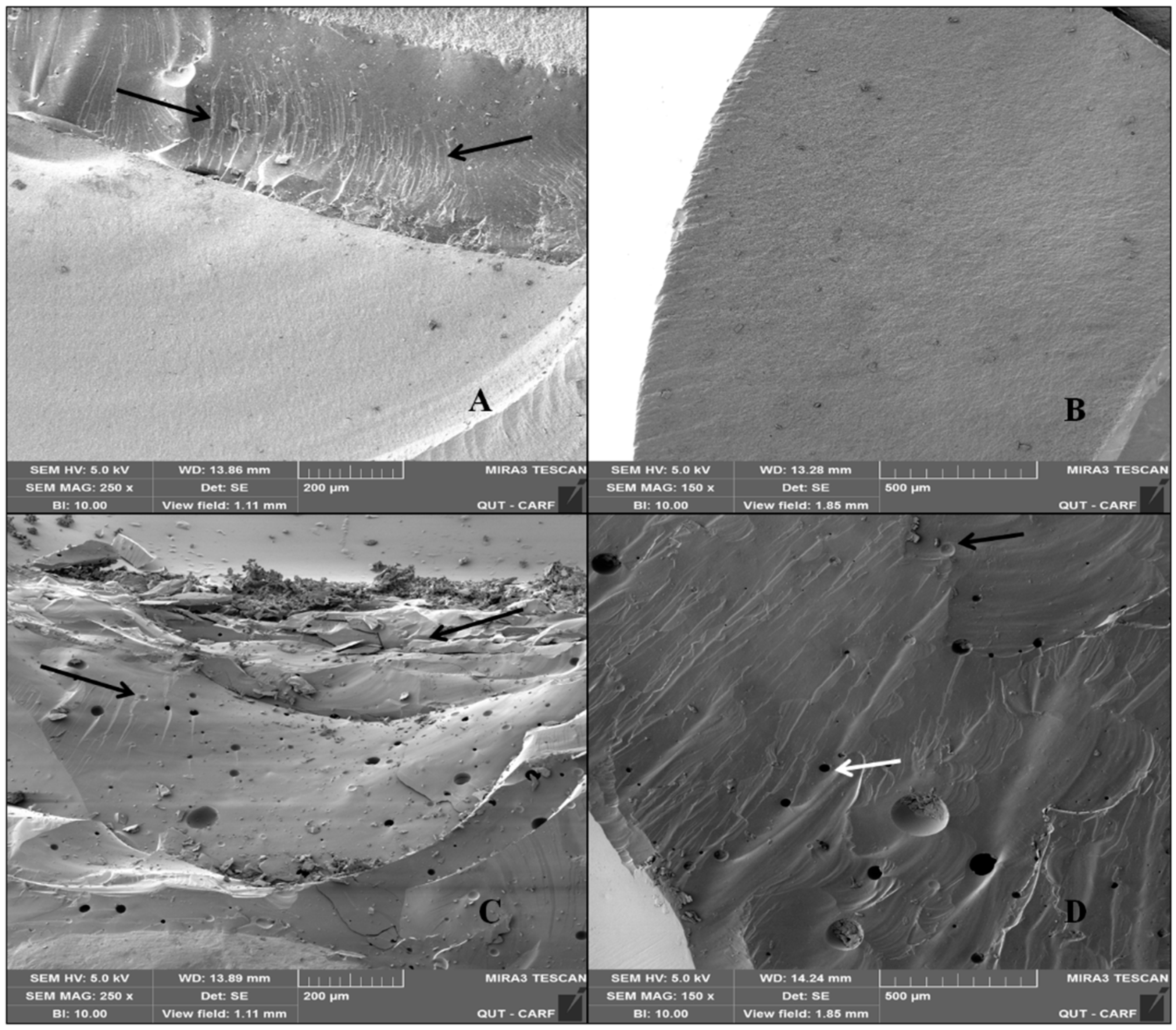
3.3. Scanning Electron Microscopy (SEM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Christel, P.; Meunier, A.; Heller, M.; Torre, J.P.; Peille, C.N. Mechanical properties and short-term in-vivo evaluation of yttrium-oxide-partially-stabilized zirconia. J. Biomed. Mater. Res. 1989, 23, 45–61. [Google Scholar] [CrossRef]
- Larsson, C.; Wennerberg, A. The clinical success of zirconia-based crowns: A systematic review. Int. J. Prosthodont. 2014, 27, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Zhang, Y.; Pines, M.; Thompson, V.P. Fracture of porcelain-veneered structures in fatigue. J. Dent. Res. 2007, 86, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Philipp, A.; Zembic, A.; Pjetursson, B.E.; Hammerle, C.H.; Zwahlen, M. A systematic review of the performance of ceramic and metal implant abutments supporting fixed implant reconstructions. Clin. Oral Implants Res. 2009, 20, 4–31. [Google Scholar] [PubMed]
- Nothdurft, F.P.; Pospiech, P.R. Zirconium dioxide implant abutments for posterior single-tooth replacement: First results. J. Periodontol. 2009, 80, 2065–2072. [Google Scholar] [CrossRef]
- Larsson, C.; von Steyern, P.V.; Sunzel, B.; Nilner, K. All-ceramic two- to five-unit implant-supported reconstructions. A randomized, prospective clinical trial. Swed. Dent. J. 2006, 30, 45–53. [Google Scholar]
- Al-Amleh, B.; Lyons, K.; Swain, M. Clinical trials in zirconia: A systematic review. J. Oral Rehabil. 2010, 37, 641–652. [Google Scholar] [PubMed]
- Raigrodski, A.J.; Chiche, G.J.; Potiket, N.; Hochstedler, J.L.; Mohamed, S.E.; Billiot, S.; Mercante, D.E. The efficacy of posterior three-unit zirconium-oxide-based ceramic fixed partial dental prostheses: A prospective clinical pilot study. J. Prosthet. Dent. 2006, 96, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Raigrodski, A.J.; Hillstead, M.B.; Meng, G.K.; Chung, K.H. Survival and complications of zirconia-based fixed dental prostheses: A systematic review. J. Prosthet. Dent. 2012, 107, 170–177. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Sailer, I.; Zwahlen, M.; Hammerle, C.H. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin. Oral Implants Res. 2007, 18, 73–85. [Google Scholar] [PubMed]
- Von Steyern, P.V.; Carlson, P.; Nilner, K. All-ceramic fixed partial dentures designed according to the DC-Zirkon technique. A 2-year clinical study. J. Oral Rehabil. 2005, 32, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Feher, A.; Filser, F.; Gauckler, L.J.; Luthy, H.; Hammerle, C.H. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 383–388. [Google Scholar] [PubMed]
- Edelhoff, D.; Florian, B.; Florian, W.; Johnen, C. HIP zirconia fixed partial dentures—Clinical results after 3 years of clinical service. Quintessence Int. 2008, 39, 459–471. [Google Scholar]
- Schmitt, J.; Holst, S.; Wichmann, M.; Reich, S.; Gollner, M.; Hamel, J. Zirconia posterior fixed partial dentures: A prospective clinical 3-year follow-up. Int. J. Prosthodont. 2009, 22, 597–603. [Google Scholar]
- Fischer, J.; Stawarczyk, B.; Sailer, I.; Hammerle, C.H. Shear bond strength between veneering ceramics and ceria-stabilized zirconia/alumina. J. Prosthet. Dent. 2010, 103, 267–274. [Google Scholar] [CrossRef][Green Version]
- Guess, P.C.; Kulis, A.; Witkowski, S.; Wolkewitz, M.; Zhang, Y.; Strub, J.R. Shear bond strengths between different zirconia cores and veneering ceramics and their susceptibility to thermocycling. Dent. Mater. 2008, 24, 1556–1567. [Google Scholar] [CrossRef] [PubMed]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Microtensile bond strength of different components of core veneered all-ceramic restorations. Part II: Zirconia veneering ceramics. Dent. Mater. 2006, 22, 857–863. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Microtensile bond strength of different components of core veneered all-ceramic restorations. Part 3: Double veneer technique. J. Prosthodont. 2008, 17, 9–13. [Google Scholar] [CrossRef]
- Kim, M.J.; Kim, Y.K.; Kim, K.H.; Kwon, T.Y. Shear bond strengths of various luting cements to zirconia ceramic: Surface chemical aspects. J. Dent. 2011, 39, 795–803. [Google Scholar] [CrossRef]
- Schmitter, M.; Mueller, D.; Rues, S. In vitro chipping behaviour of all-ceramic crowns with a zirconia framework and feldspathic veneering: Comparison of CAD/CAM-produced veneer with manually layered veneer. J. Oral Rehabil. 2013, 40, 519–525. [Google Scholar] [CrossRef]
- Saito, A.; Komine, F.; Blatz, M.B.; Matsumura, H. A comparison of bond strength of layered veneering porcelains to zirconia and metal. J. Prosthet. Dent. 2010, 104, 247–257. [Google Scholar] [CrossRef]
- De Jager, N.; Pallav, P.; Feilzer, A.J. The influence of design parameters on the FEA-determined stress distribution in CAD-CAM produced all-ceramic dental crowns. Dent. Mater. 2005, 21, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Manicone, P.F.; Iommetti, P.R.; Raffaelli, L. An overview of zirconia ceramics: Basic properties and clinical applications. J. Dent. 2007, 35, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Prestipino, V.; Ingber, A. Esthetic high-strength implant abutments. Part I. J. Esthet. Dent. 1993, 5, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Prestipino, V.; Ingber, A. Esthetic high-strength implant abutments. Part II. J. Esthet. Dent. 1993, 5, 63–68. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: An in vivo human study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef]
- Rimondini, L.; Cerroni, L.; Carrassi, A.; Torricelli, P. Bacterial colonization of zirconia ceramic surfaces: An in vitro and in vivo study. Int. J. Oral Maxillofac. Implants 2002, 17, 793–798. [Google Scholar]
- Degidi, M.; Artese, L.; Scarano, A.; Perrotti, V.; Gehrke, P.; Piattelli, A. Inflammatory infiltrate, microvessel density, nitric oxide synthase expression, vascular endothelial growth factor expression, and proliferative activity in peri-implant soft tissues around titanium and zirconium oxide healing caps. J. Periodontol. 2006, 77, 73–80. [Google Scholar] [CrossRef]
- Lin, W.S.; Harris, B.T.; Zandinejad, A.; Martin, W.C.; Morton, D. Use of prefabricated titanium abutments and customized anatomic lithium disilicate structures for cement-retained implant restorations in the esthetic zone. J. Prosthet. Dent. 2014, 111, 181–185. [Google Scholar] [CrossRef]
- Hornbrook, D. Case report using the “H” abutment: Achieving esthetics, strength, and predictability for the anterior implant. Compend. Contin. Educ. Dent. 2015, 36, 192, 194–198, 200–201. [Google Scholar]
- Silva, N.R.; Teixeira, H.S.; Silveira, L.M.; Bonfante, E.A.; Coelho, P.G.; Thompson, V.P. Reliability and Failure Modes of a Hybrid Ceramic Abutment Prototype. J. Prosthodont. 2018, 27, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Honda, J.; Komine, F.; Kamio, S.; Taguchi, K.; Blatz, M.B.; Matsumura, H. Fracture resistance of implant-supported screw-retained zirconia-based molar restorations. Clin. Oral Implants Res. 2017, 28, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.R.; Rungruanganunt, P. Fatigue Behavior of Computer-Aided Design/Computer-Assisted Manufacture Ceramic Abutments as a Function of Design and Ceramics Processing. Int. J. Oral Maxillofac. Implants 2016, 31, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Elshiyab, S.H.; Nawafleh, N.; Öchsner, A.; George, R. Fracture resistance of implant-supported monolithic crowns cemented to zirconia hybrid-abutments: Zirconia-based crowns vs. lithium disilicate crowns. J. Adv. Prosthodont. 2018, 10, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Elshiyab, S.H.; Nawafleh, N.; Walsh, L.; George, R. Fracture resistance and survival of implant-supported, zirconia-based hybrid-abutment crowns: Influence of aging and crown structure. J. Investig. Clin. Dent. 2018, 9, e12355. [Google Scholar] [CrossRef]
- Selz, C.F.; Vuck, A.; Guess, P.C. Full-mouth rehabilitation with monolithic CAD/CAM-fabricated hybrid and all-ceramic materials: A case report and 3-year follow up. Quintessence Int. 2016, 47, 115–121. [Google Scholar]
- Edelhoff, D.; Schweiger, J.; Prandtner, O.; Stimmelmayr, M.; Güth, J.-F. Metal-free implant-supported single-tooth restorations. Part II: Hybrid abutment crowns and material selection. Quintessence Int. 2019, 50, 260–269. [Google Scholar]
- Rabel, K.; Spies, B.C.; Pieralli, S.; Vach, K.; Kohal, R.J. The clinical performance of all-ceramic implant-supported single crowns: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 29, 196–223. [Google Scholar] [CrossRef]
- Coelho, P.G.; Silva, N.R.; Bonfante, E.A.; Guess, P.C.; Rekow, E.D.; Thompson, V.P. Fatigue testing of two porcelain-zirconia all-ceramic crown systems. Dent. Mater. 2009, 25, 1122–1127. [Google Scholar] [CrossRef]
- Att, W.; Kurun, S.; Gerds, T.; Strub, J.R. Fracture resistance of single-tooth implant-supported all-ceramic restorations: An in vitro study. J. Prosthet. Dent. 2006, 95, 111–116. [Google Scholar] [CrossRef]
- Rosentritt, M.; Behr, M.; van der Zel, J.M.; Feilzer, A.J. Approach for valuating the influence of laboratory simulation. Dent. Mater. 2009, 25, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Rosentritt, M.; Siavikis, G.; Behr, M.; Kolbeck, C.; Handel, G. Approach for valuating the significance of laboratory simulation. J. Dent. 2008, 36, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- DeLong, R.; Douglas, W.H. Development of an artificial oral environment for the testing of dental restoratives: Bi-axial force and movement control. J. Dent. Res. 1983, 62, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, C.H.; Lundeen, H.C.; Mahan, P.E.; Fujimoto, J. Chewing movements in relation to border movements at the first molar. J. Prosthet. Dent. 1981, 46, 308–322. [Google Scholar] [CrossRef]
- Strub, J.R.; Gerds, T. Fracture strength and failure mode of five different single-tooth implant-abutment combinations. Int. J. Prosthodont. 2003, 16, 167–171. [Google Scholar]
- Beuer, F.; Schweiger, J.; Eichberger, M.; Kappert, H.F.; Gernet, W.; Edelhoff, D. High-strength CAD/CAM-fabricated veneering material sintered to zirconia copings—A new fabrication mode for all-ceramic restorations. Dent. Mater. 2009, 25, 121–128. [Google Scholar] [CrossRef]
- Schmitter, M.; Mueller, D.; Rues, S. Chipping behaviour of all-ceramic crowns with zirconia framework and CAD/CAM manufactured veneer. J. Dent. 2012, 40, 154–162. [Google Scholar] [CrossRef]
- Kanat, B.; Comlekoglu, E.M.; Dundar-Comlekoglu, M.; Sen, B.H.; Ozcan, M.; Gungor, M.A. Effect of various veneering techniques on mechanical strength of computer-controlled zirconia framework designs. J. Prosthodont. 2014, 23, 445–455. [Google Scholar] [CrossRef]
- Bindl, A.; Luthy, H.; Mormann, W.H. Thin-wall ceramic CAD/CAM crown copings: Strength and fracture pattern. J. Oral Rehabil. 2006, 33, 520–528. [Google Scholar] [CrossRef]
- Von Steyern, P.V.; Ebbesson, S.; Holmgren, J.; Haag, P.; Nilner, K. Fracture strength of two oxide ceramic crown systems after cyclic pre-loading and thermocycling. J. Oral Rehabil. 2006, 33, 682–689. [Google Scholar] [CrossRef]
- Tsalouchou, E.; Cattell, M.J.; Knowles, J.C.; Pittayachawan, P.; McDonald, A. Fatigue and fracture properties of yttria partially stabilized zirconia crown systems. Dent. Mater. 2008, 24, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Kassem, A.S.; Atta, O.; El-Mowafy, O. Fatigue resistance and microleakage of CAD/CAM ceramic and composite molar crowns. J. Prosthodont. 2012, 21, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Ivoclarvivadent.com. Available online: http://www.pda-lab.com/documents/IPS-emax-cad-on-ivoclar-4-pgs.pdf (accessed on 13 May 2017).
- Vlaar, S.T.; van der Zel, J.M. Accuracy of dental digitizers. Int. Dent. J. 2006, 56, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Aboushelib, M.N.; de Kler, M.; van der Zel, J.M.; Feilzer, A.J. Microtensile bond strength and impact energy of fracture of CAD-veneered zirconia restorations. J. Prosthodont 2009, 18, 211–216. [Google Scholar] [CrossRef]
- Sato, T.; Tsuji, K.; Kawashima, N.; Sato, H.; Nakamura, Y. Effect of defect size on fracture strength of dental low fusion porcelain. Colloids Surf. B Biointerfaces 2004, 38, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Rekow, D.; Thompson, V.P. Engineering long term clinical success of advanced ceramic prostheses. J. Mater. Sci. Mater. Med. 2007, 18, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Bonfante, E.A.; Silva, N.R.; Rekow, E.D.; Thompson, V.P. Laboratory simulation of Y-TZP all-ceramic crown clinical failures. J. Dent. Res. 2009, 88, 382–386. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Description | Manufacturer |
|---|---|---|
| Forty implants | 5.5 mm diameter Ankylos® C/X titanium implants | DENTSPLY–Friadent GmbH, Mannheim, Germany |
| Forty Hybrid-Abutments | ||
| 1. Titanium base (Ti-Base) 2. Zirconia abutments | 1. Internal Ankylos® compatible Ti-Base; 1.00 mm hex screw, 4 mm height and 0° angulations 2. Zirconia abutments with 1.0 mm depth shoulder | 1. Dess, Dental Smart Solutions, Montcada, Spain 2. Zenostar, Ivoclar Vivadent, Lichtenstein, Germany |
| Forty copings | Anatomically designed as per manufacturer recommendations (0.5 mm circular and 0.7 occlusal) and milled from pre-sintered zirconia discs | Zenostar, Ivoclar Vivadent, Lichtenstein, Germany |
| Veneering material | 1. Hand-layered nano-fluorapatite ceramic. IPS e.max Ceram (0.7 mm circular and 0.7 occlusal) 2. Milled lithium disilicate blocks, IPS e.max CAD (0.7 mm circular and 0.7 occlusal) | Ivoclar Vivadent, Lichtenstein, Germany |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elshiyab, S.H.; Nawafleh, N.; Khan, U.; Öchsner, A.; George, R. Impact of Coping Veneering Techniques on the Survival of Implant-Supported Zirconia-Based-Crowns Cemented to Hybrid-Abutments: An-In-Vitro Study. Bioengineering 2020, 7, 117. https://doi.org/10.3390/bioengineering7040117
Elshiyab SH, Nawafleh N, Khan U, Öchsner A, George R. Impact of Coping Veneering Techniques on the Survival of Implant-Supported Zirconia-Based-Crowns Cemented to Hybrid-Abutments: An-In-Vitro Study. Bioengineering. 2020; 7(4):117. https://doi.org/10.3390/bioengineering7040117
Chicago/Turabian StyleElshiyab, Shareen Hayel, Noor Nawafleh, Usman Khan, Andreas Öchsner, and Roy George. 2020. "Impact of Coping Veneering Techniques on the Survival of Implant-Supported Zirconia-Based-Crowns Cemented to Hybrid-Abutments: An-In-Vitro Study" Bioengineering 7, no. 4: 117. https://doi.org/10.3390/bioengineering7040117
APA StyleElshiyab, S. H., Nawafleh, N., Khan, U., Öchsner, A., & George, R. (2020). Impact of Coping Veneering Techniques on the Survival of Implant-Supported Zirconia-Based-Crowns Cemented to Hybrid-Abutments: An-In-Vitro Study. Bioengineering, 7(4), 117. https://doi.org/10.3390/bioengineering7040117