1. Introduction
The skin serves vital functions, including protection against pathogens, regulation of body temperature, and prevention of fluid loss. Severe skin injuries, such as acute or chronic wounds, can significantly impair these essential roles, leading to increased risks of infection, osteomyelitis, dehydration, and metabolic complications [
1]. Although autologous skin grafts and flap reconstruction are regarded as the standard treatments for severe skin injuries, their use is often restricted due to the availability of donor sites and the associated morbidity. These limitations underscore the urgent need for alternative wound management strategies. Therefore, interest in skin substitutes has grown and may offer promising solutions for the effective coverage of large wounds [
2].
Recent advancements in wound healing technology have resulted in the creation of various artificial dermal substitutes [
3,
4]. However, these substitutes often lead to noticeable and undesirable scarring [
5,
6]. A primary challenge is wound contraction, which plays a crucial role in minimizing scar formation following complete healing. Although artificial dermis can be utilized for wound coverage, the lack of cellular components typically results in delayed healing and abnormal scar formation, including scar contractures. Recent developments in wound healing technologies have enabled the implementation of cell-based therapies and tissue-engineered artificial skin as an alternative to traditional treatments and a way to overcome the limitations associated with artificial dermis [
7].
Tissue-engineered artificial skin has the capability to improve wound healing while minimizing the need for extensive surgical interventions and reducing the risk of donor site complications. This innovative approach is applicable to both acute and chronic wounds and represents a promising strategy for improving tissue regeneration [
8]. Cryopreserved human fibroblast-derived dermal substitutes, such as Dermagraft (Shire Regenerative Medicine) [
9] and Apligraf (Organogenesis) [
10], are allogeneic skin replacements that have been shown to be effective for wound healing. Additionally, non-cryopreserved fresh human fibroblast allografts have demonstrated safety and effectiveness as treatment options for these ulcers. A bioengineered dermal substitute known as Hyalograft 3D, which consists of cultured autologous fibroblasts seeded on a hyaluronic acid scaffold, has also been developed.
The current artificial skin substitutes and tissue engineering strategies encounter several challenges that limit their clinical effectiveness. Traditional methods typically utilize multi-layered structures to replicate the architecture of natural skin, which necessitates complex fabrication processes and the careful management of individual dermal and epidermal components [
11]. Although recent advancements in three-dimensional (3D) bioprinting have shown promise in developing sophisticated skin constructs with precise cell placement and biomaterial distribution [
12], these techniques often require considerable technical expertise, specialized equipment, and significant financial investment [
13].
Cell scaffolds feature precisely controlled density variations within a unified structure, enabling the spatial organization of keratinocytes and stromal vascular fraction (SVF) cells. This study utilized 3D printing to fabricate a basement membrane to mimic the natural papillary epidermal–dermal skin junction. This structure was strategically placed between the epidermal and dermal layers to maintain cellular separation and prevent unintended mixing.
The purpose of this in vitro study was to investigate the feasibility of developing tri-layered tissue-engineered full-thickness artificial skin, incorporating a basement membrane for clinical applications aimed at accelerating wound healing. Our objectives included establishing a rapid fabrication protocol that maintains cell functionality, achieving a structural organization that closely resembles native skin architecture, and assessing mechanical stability and biocompatibility. This innovative approach may represent a significant advancement over existing substitutes by integrating the regenerative potential of SVF cells with the epidermal function of keratinocytes within a biomimetic structure designed for the wound healing of full-thickness skin and soft tissue defects.
2. Materials and Methods
This study protocol was approved by the Institutional Review Board and written informed consent was obtained from the patient prior to surgery. This study was conducted in full accordance with the principles of the Declaration of Helsinki.
2.1. Preparation of Stromal Vascular Fraction Cells for the Dermal Layer
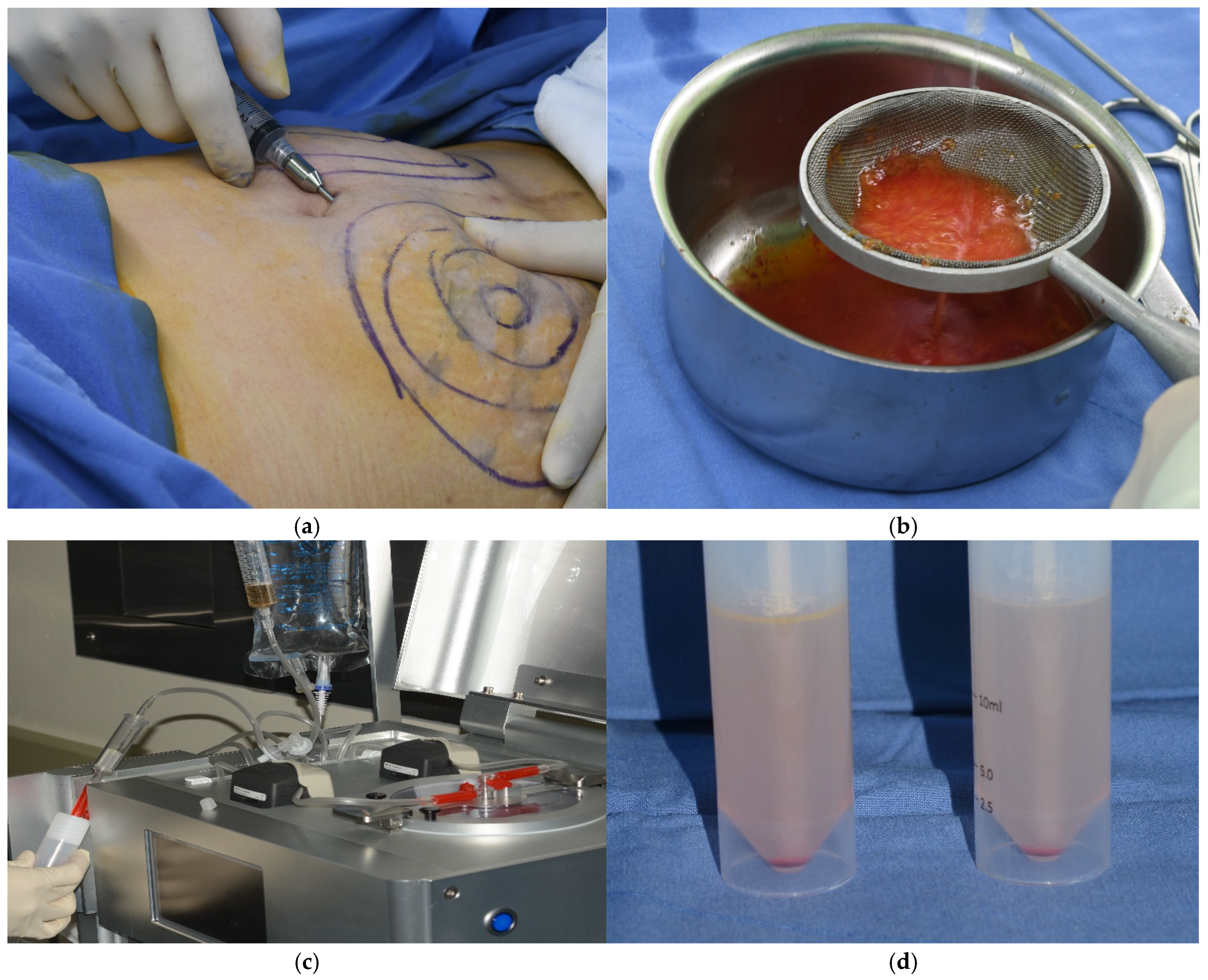
Abdominal adipose tissue was obtained from a patient by liposuction. A small incision was made in the umbilical area, and a local anesthetic solution was administered using a blunt Lamis infiltration cannula. The adipose tissue was aspirated using a 50 mL syringe connected to a cannula with a 3 mm inner diameter designed to maintain the integrity of the adipose tissue. The plunger of the syringe was retracted gently during the aspiration process to avoid creating excessive negative pressure that could lead to tissue rupture. The collected adipose tissue was then processed to isolate autologous SVF cells utilizing an automated cell isolation system (Cellunit; CGBio Inc., Seoul, Republic of Korea). This apparatus features a device along with sterile, disposable cartridges tailored for the processes of tissue digestion, washing, and waste management. In brief, the harvested samples underwent enzymatic digestion with 0.1% collagenase (SERVA Electrophoresis GmbH, Heidelberg, Germany) inside a processing chamber. The digested tissue was subsequently washed with saline to eliminate any leftover collagenase before centrifugation to separate the SVF cells, which were harvested within 50 min (
Figure 1).
2.2. Preparation of Keratinocytes for the Epidermal Layer
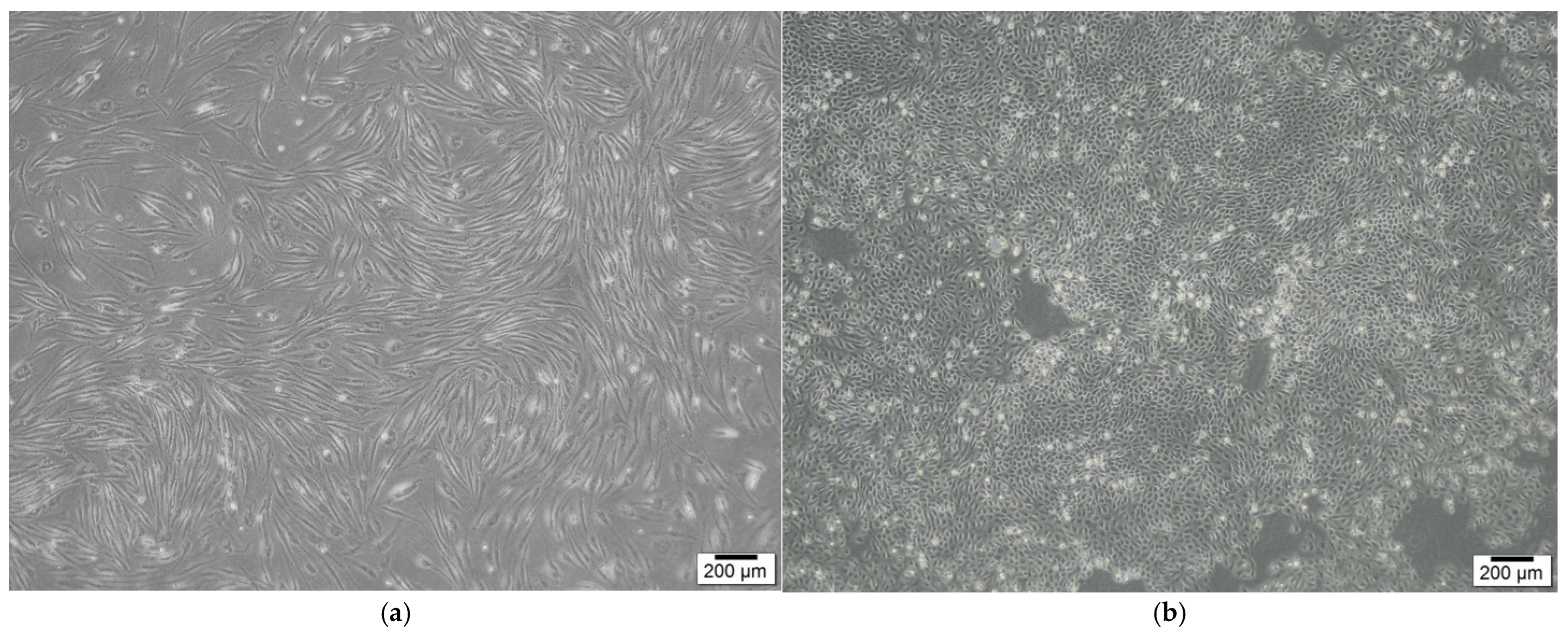
Keratinocytes were sourced from a skin biopsy and cultured in Dulbecco’s Modified Eagle Medium (DMEM; Gibco), enriched with 10% fetal bovine serum (FBS; Gibco) and 1% penicillin-streptomycin (Gibco). The cultures were kept at 37 °C in a humidified environment with 5% CO
2. Once the adherent monolayer achieved 70–80% confluence, the cells were detached using TrypLE Express (Gibco), which contains 0.25% trypsin. After detachment, the cells were washed, re-suspended in DMEM supplemented with 10% FBS, and sub-cultured. The cells were then incubated for 24 h (
Figure 2).
2.3. Cell Layer Scaffolds
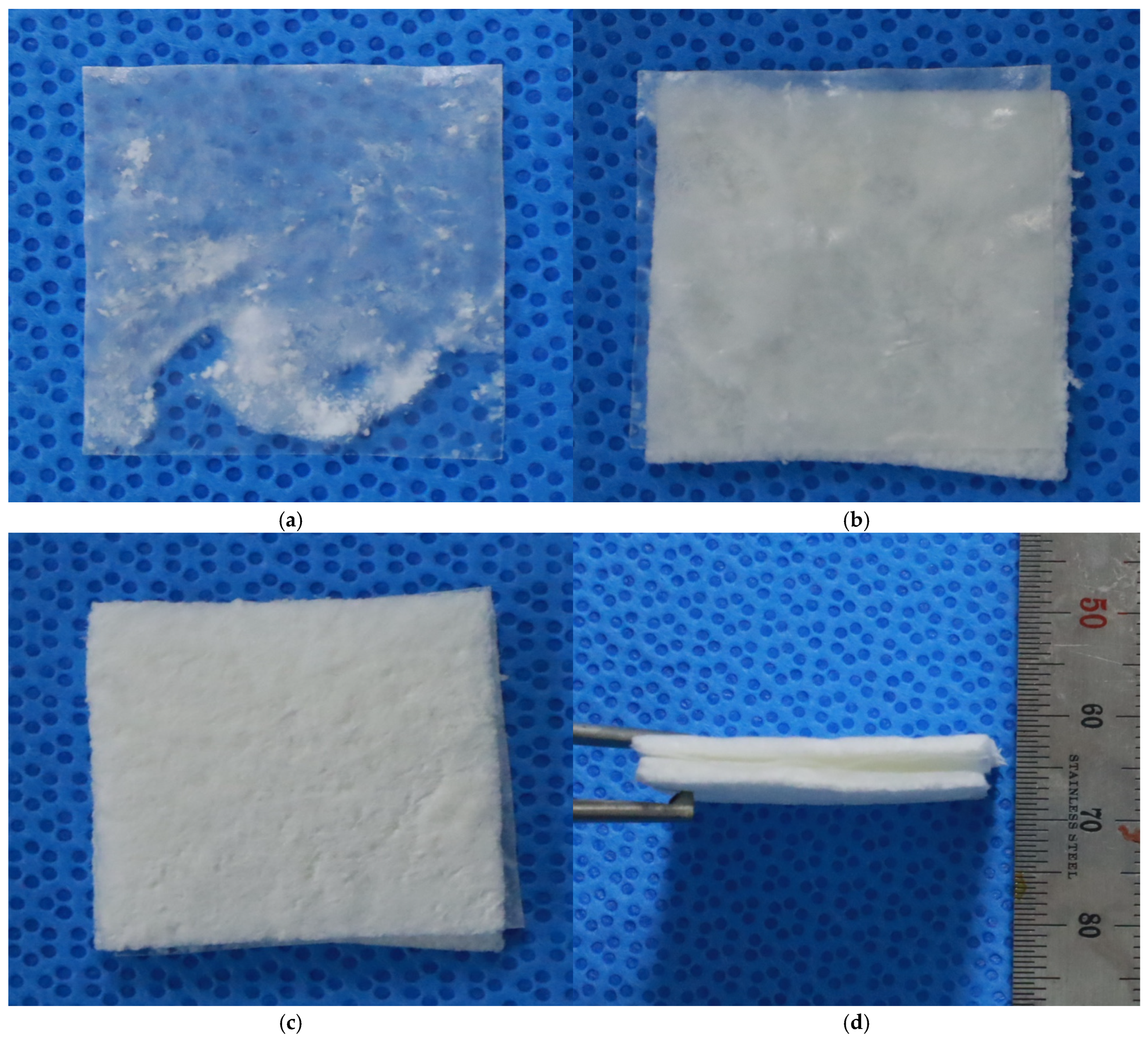
Cell scaffolds were fabricated using 100% bovine collagen in a low-temperature 3D printer. Three-dimensional printing created a single-layered structure, which was chemically crosslinked for mechanical stability and freeze-dried to develop a multiporous architecture for cell fixation. This design streamlines the manufacturing process and clinical application by minimizing handling challenges and enhancing the scaffold’s adaptability to various wound environments.
2.4. Basement Membrane Between the Cell Layer Scaffolds
A basement membrane for use between the scaffolds in the full-thickness artificial skin was fabricated using 100% bovine collagen and elastin in a low-temperature 3D printer. Scaffolds with collagen-to-elastin ratios of 100:4 were printed. Three-dimensional printing created a dense thin film structure, which was chemically cross-linked for mechanical stability and freeze-dried to develop a stable architecture for cell–cell interaction without mixing the two cell layers.
2.5. Analysis of the Basement Membrane and Tri-Layered Full-Thickness Artificial Skin
Degradation and tensile strength tests were performed to analyze the basement membrane composed of collagen and elastin. Biocompatibility was also assessed by seeding SVF cells and keratinocytes onto the basement membrane and evaluating cell viability and cytotoxicity over a 7-day period. Keratinocytes and SVF cells were seeded onto a UV-sterilized 1 × 1 cm collagen-elastin based basement membrane and cultured under standard conditions (37 °C, 5% CO2) to assess the biocompatibility of the fabricated full-thickness artificial skin constructs. Cytotoxicity and cell viability were evaluated using the Cell Counting Kit-8 (CCK-8; Sigma-Aldrich, St. Louis, MO, USA) assay, and absorbance was measured at 450 nm. The CCK-8 assay was conducted at 1, 3, 5, and 7 days of culture to assess cell viability and cytotoxic effects. A commercial acellular artificial dermis made entirely of collagen sourced from porcine skin (Insuregraf, Atozbio, Seoul, Republic of Korea) was employed as the control.
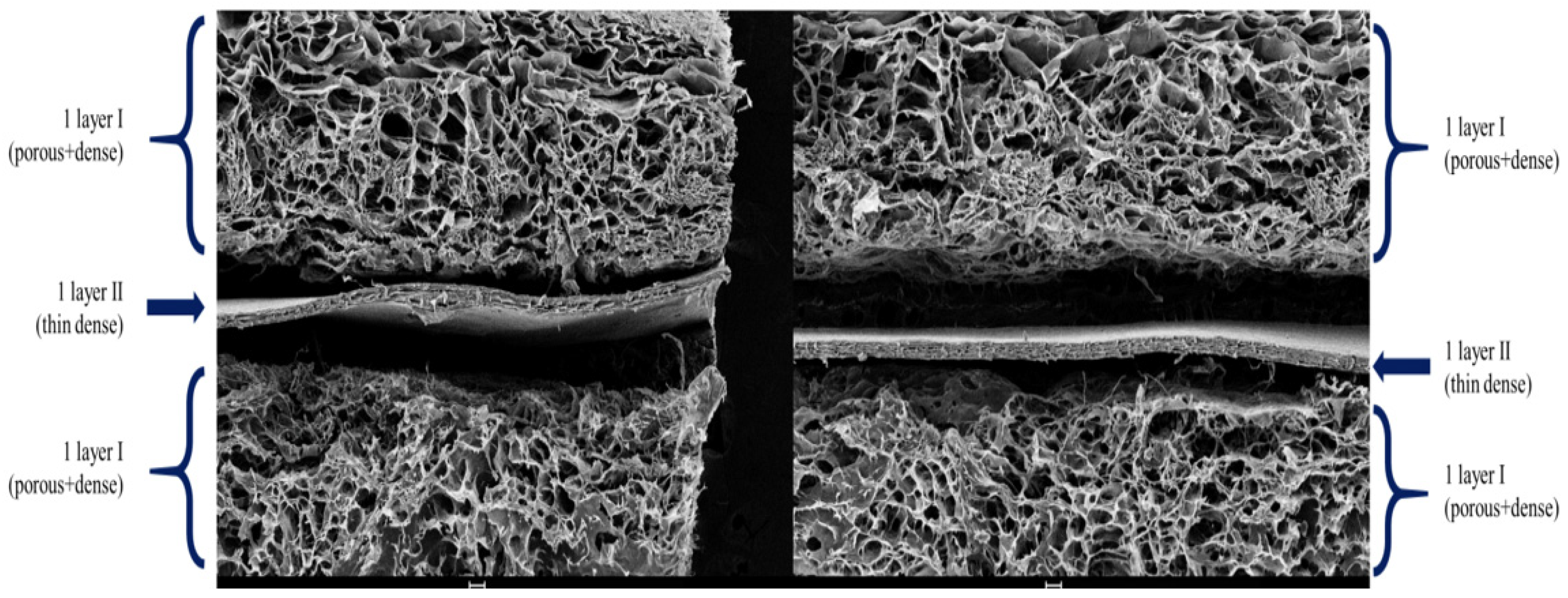
The final tri-layered full-thickness artificial skin included two cell scaffolds with a basement membrane between them (
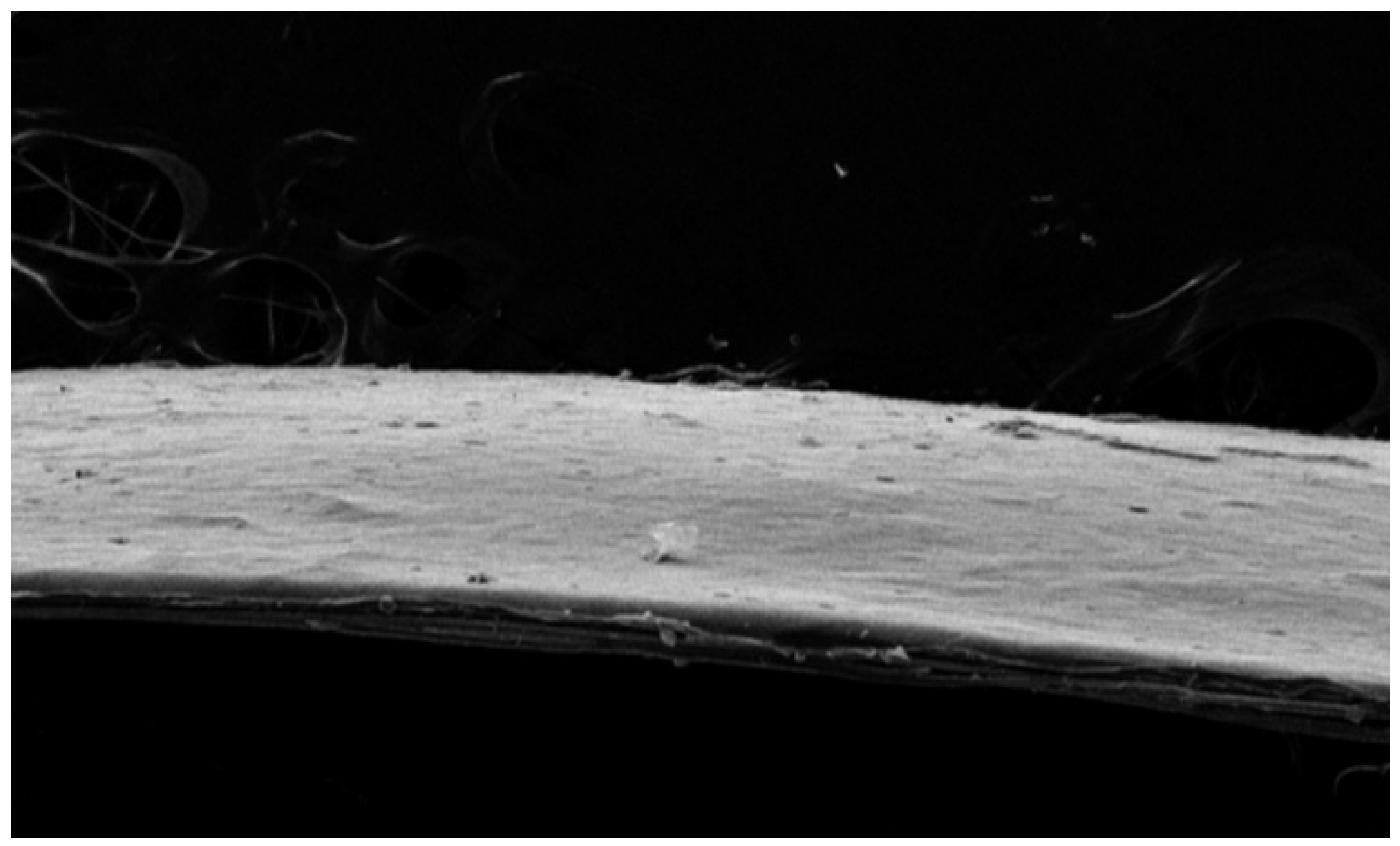
Figure 3). Scanning electron microscopy (SEM) was utilized to examine the structural characteristics of the basement membrane and the final structural features of the tri-layered full-thickness artificial skin.
2.6. Cell Imaging of the Tri-Layered Full-Thickness Artificial Skin
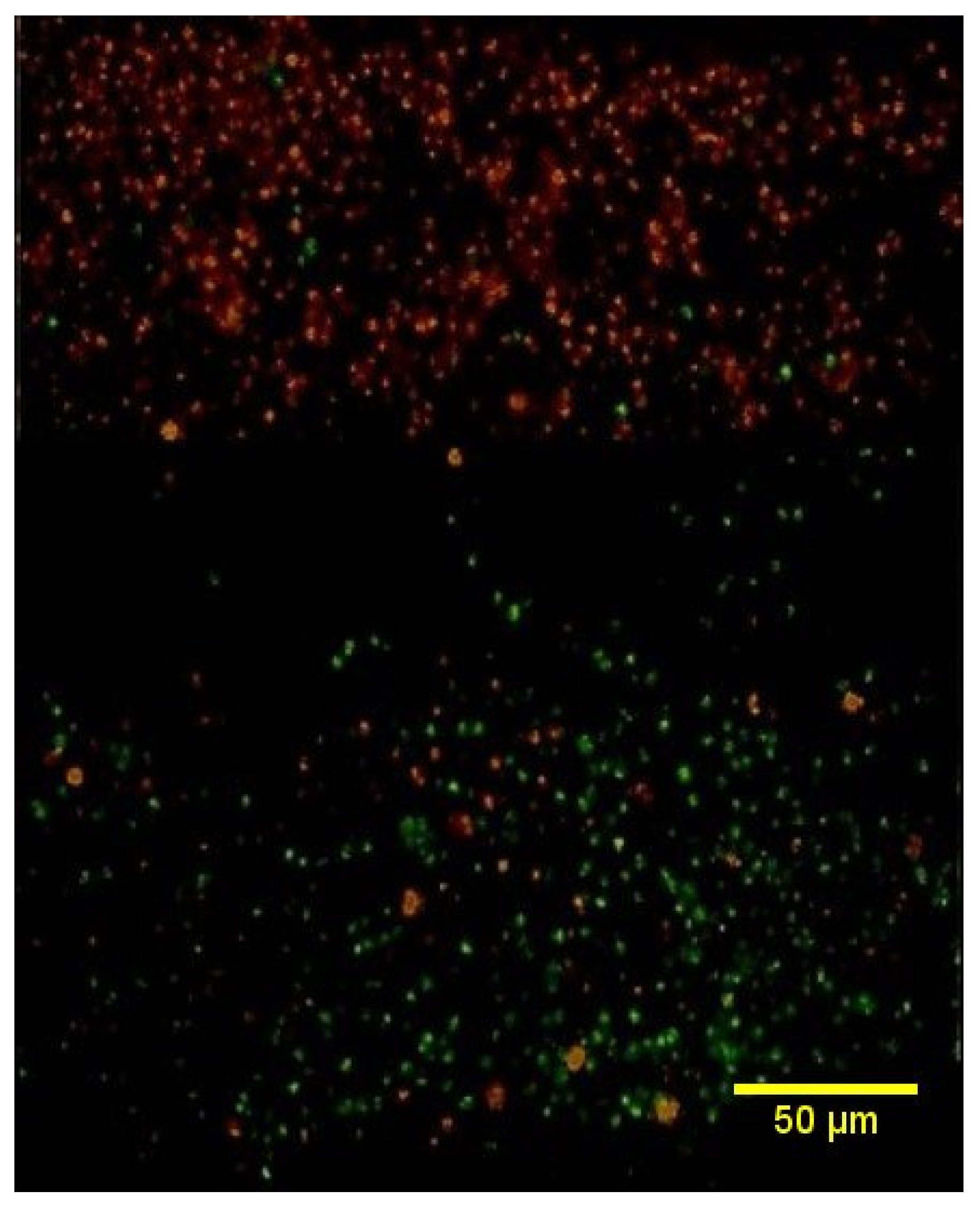
The cell membranes of keratinocytes and SVF cells were labeled by 2μM PKH26 red fluorescent dye and green fluorescent dye (Sigma-Aldrich), respectively. Subsequently, cells were cultured on collagen scaffolds to create the full-thickness artificial skin. Keratinocytes were applied to the epidermal layer, while SVF cells were applied to the dermal layer, with a basement membrane laminated between each layer to fabricate the complete construct. The fabricated full-thickness artificial skin was placed on a cell culture insert (Millicell, Millipore, Burlington, MO, USA) and cultured for 5 days under standard conditions (37 °C, 5% CO2). For imaging purposes, the cultured artificial skin was washed three times with phosphate-buffered saline (PBS) and fixed in 4% paraformaldehyde for 12 h. After fixation, the samples were rinsed three times with PBS, agarose-embedded, and sectioned to a thickness of 30 μm using a vibratome (Leica VT1000S). The sectioned samples were mounted on slides, and fluorescence expression was captured using an EVOS FL2 fluorescence microscope (Thermo Fisher Scientific, Waltham, MO, USA).
4. Discussion
Full-thickness skin and soft tissue defects, including acute and chronic wounds, represent a significant global healthcare burden, with extensive full-thickness injuries often exceeding the natural healing capacity. While autologous skin grafting and flap reconstruction remain the gold standard, their application is limited by donor site availability and associated morbidity [
14]. Recent advances in tissue engineering have led to various artificial skin substitutes, from collagen scaffolds to bioprinted constructs, typically involving biomaterial scaffolds seeded with cultured autologous keratinocytes or fibroblasts [
15,
16].
However, keratinocytes are epithelializing cells in superficial wounds and fibroblasts are involved in granulation tissue growth in deep and chronic wounds. Because each cell has a different effect on wound healing, the wounds to which each can be applied are limited. These approaches also face significant limitations, including extended fabrication times due to cell expansion requirements and challenges in achieving adequate host tissue integration. Furthermore, the existing substitutes often fail to fully replicate the complex structural and functional characteristics of native skin tissue [
17]. Therefore, full-thickness artificial skin, composed of epidermal and dermal layers, is necessary for better wound healing in full-thickness skin and soft tissue defects.
SVF cells can be obtained in one hour and present a promising alternative, offering rapid extraction and a heterogeneous population of regenerative cells, including fibroblasts, stromal cells, endothelial progenitors, and immune cells [
18]. This diverse cellular composition potentially facilitates better tissue integration and vascularization compared to purified cell populations. When combined with autologous keratinocytes, which can be efficiently isolated and expanded from small skin biopsies [
19], this approach enables the construction of immunologically compatible skin substitutes. Despite these advantages, there remains a significant gap in developing clinically viable full-thickness artificial skin models that effectively mimic native tissue architecture while maintaining practical feasibility [
20].
This study successfully developed a biomimetic full-thickness artificial skin construct by integrating SVF and autologous keratinocytes onto a tri-layered collagen-elastin scaffold. The incorporation of elastin enhanced mechanical properties, nearly doubling the tensile strength and improving resistance to enzymatic degradation compared to collagen-only scaffolds and acellular artificial dermis. Importantly, the construct retained substantial mechanical integrity (3.9 N) after gamma sterilization, indicating its robustness for clinical applications.
The tri-layered architecture, characterized by SEM analysis, effectively replicates the natural dermal-epidermal interface. Uniform pore distribution (100–300 μm) in the porous layers facilitates nutrient diffusion and cellular infiltration, while the dense barrier basement membrane provides structural separation and mechanical support. This hierarchical design addresses a key limitation of the existing full-thickness artificial skin substitutes, which often fail to mimic the complexity of native skin tissue [
17].
The excellent biocompatibility observed in keratinocytes and SVF cells over 7 days demonstrated the suitability of the basement membrane as a septum to which both cells can adhere. The rapid isolation of SVF cells and diverse cellular composition, including endothelial progenitors, offers significant advantages over traditional fibroblast-based methods, potentially enhancing vascularization and integration [
18]. These attributes address critical challenges in tissue engineering, particularly the need for rapid fabrication and effective host-tissue integration. Long-term culture observations further validated the biocompatibility of the constructs. Both keratinocytes and SVF cells showed consistent growth trends, with no signs of cytotoxicity or abnormal cellular morphology throughout the 7-day culture period. The CCK-8 assay results aligned with the microscopic findings, indicating that the fabricated constructs provide a favorable microenvironment for cellular growth and function.
The present study had some limitations. First, due to the lack of direct comparative data between SVF cells and fibroblasts, the extent to which SVF cells contribute to granulation tissue formation relative to fibroblasts remains unclear. Second, additional biomaterials, such as fibrin glue, capable of handling tri-layered full-thickness artificial skin without significant cell loss are needed. The CCK-8 assay alone may not provide a comprehensive evaluation of cytotoxicity and cell proliferation. Incorporating additional methods, such as immunostaining and flow cytometry to assess cell apoptosis, would strengthen claims of biocompatibility. Additionally, variability in SVF composition between donors could impact reproducibility and standardization in clinical applications. Addressing these limitations through in vivo studies and optimized SVF isolation protocols will be essential for future translation. Therefore, further in vivo studies should be conducted to assess the histological and functional roles of the full-thickness artificial skin developed in this study, focusing on its efficacy in wound closure, vascularization, host integration, potential immunogenicity issues related to bovine collagen, and associated immune responses.
Despite these limitations, the tri-layered full-thickness artificial skin with a basement membrane for wound healing developed in this study offers unique advancements in mechanical stability, structural biomimicry, and biocompatibility for developing full-thickness artificial skin for wound healing. The scaffold’s ability to maintain mechanical properties post-sterilization and its resistance to enzymatic degradation particularly highlight its clinical viability. Future research should focus on validating these constructs in vivo, exploring their vascularization potential, and establishing standardized preparation protocols to facilitate clinical adoption.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}