
Regulation of Inflammatory Responses by Pulsed Electromagnetic Fields


Abstract
1. Introduction
2. Effects of PEMF on Inflammation
3. Effects of PEMF on Inflammation in Soft Tissue Wound Healing
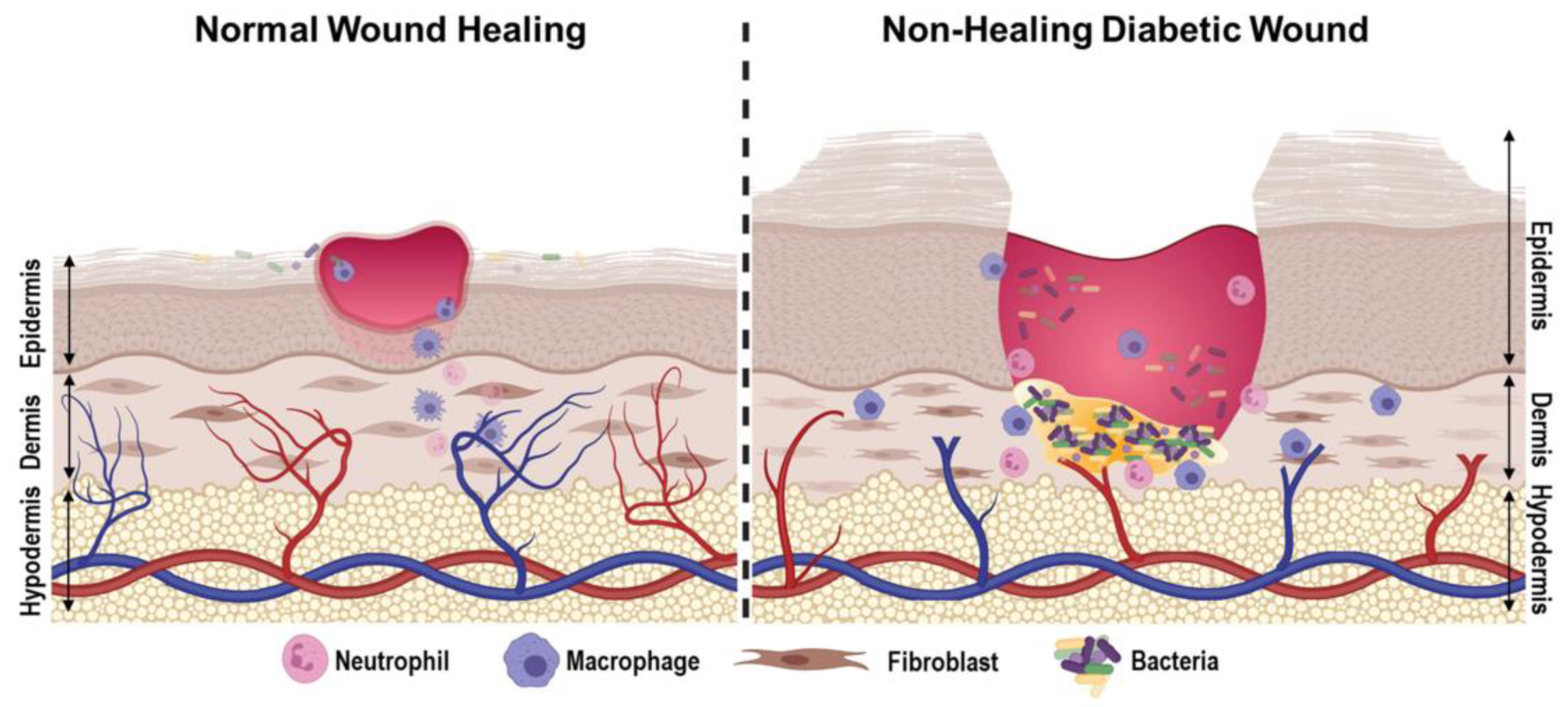
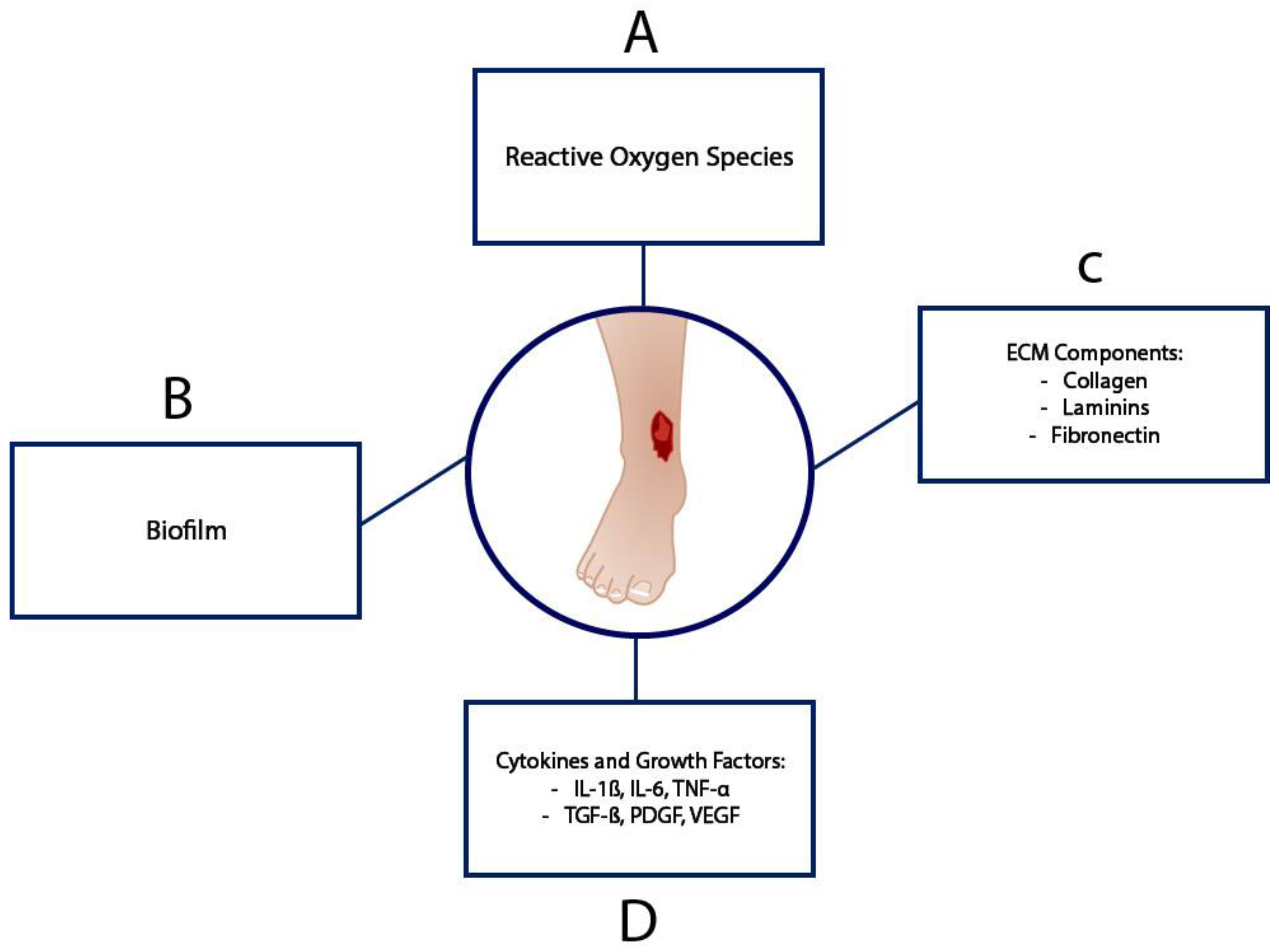
3.1. Diabetic Wound Healing
3.2. Venous Ulcer Healing
3.3. Hypoxic and Vascular Damage
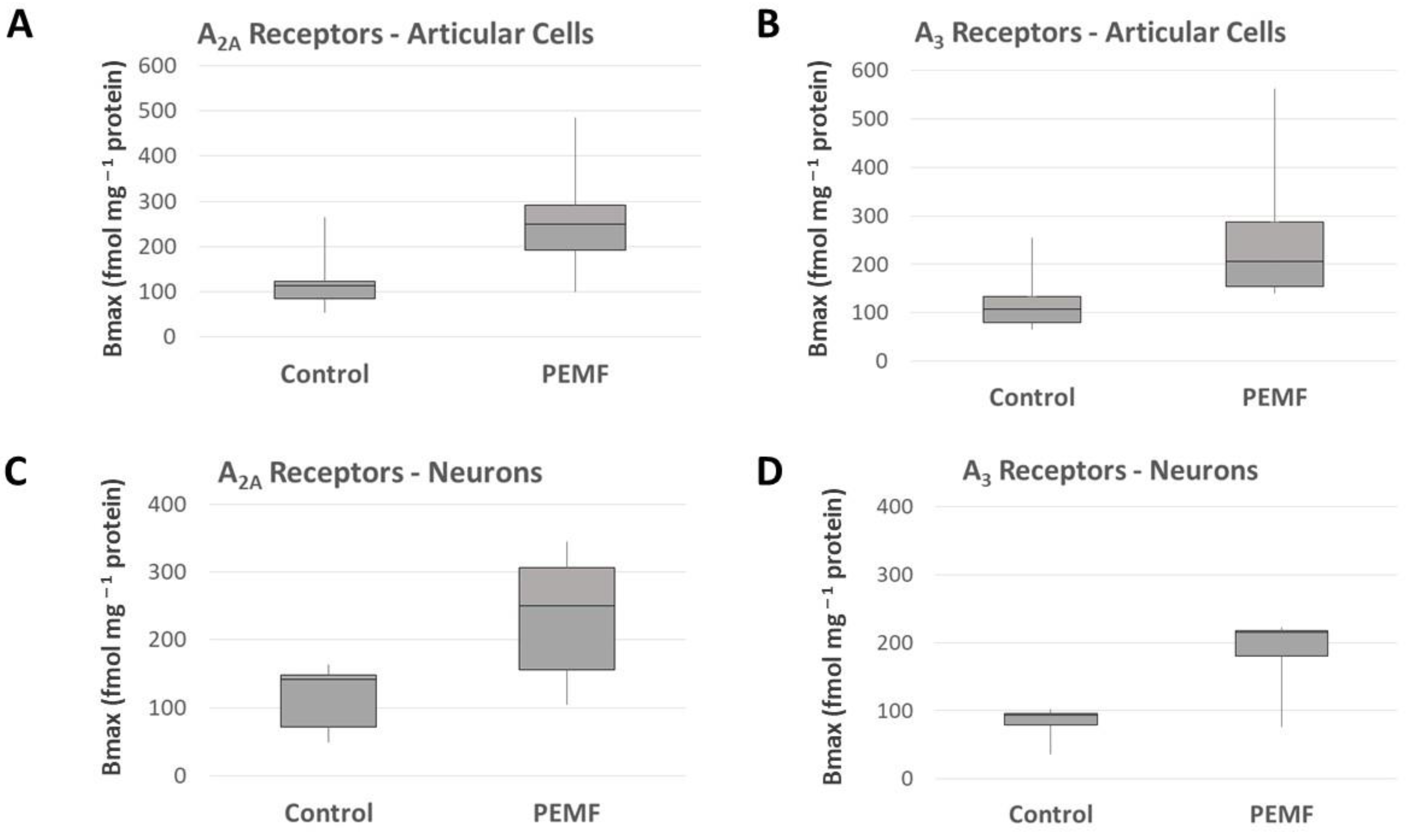
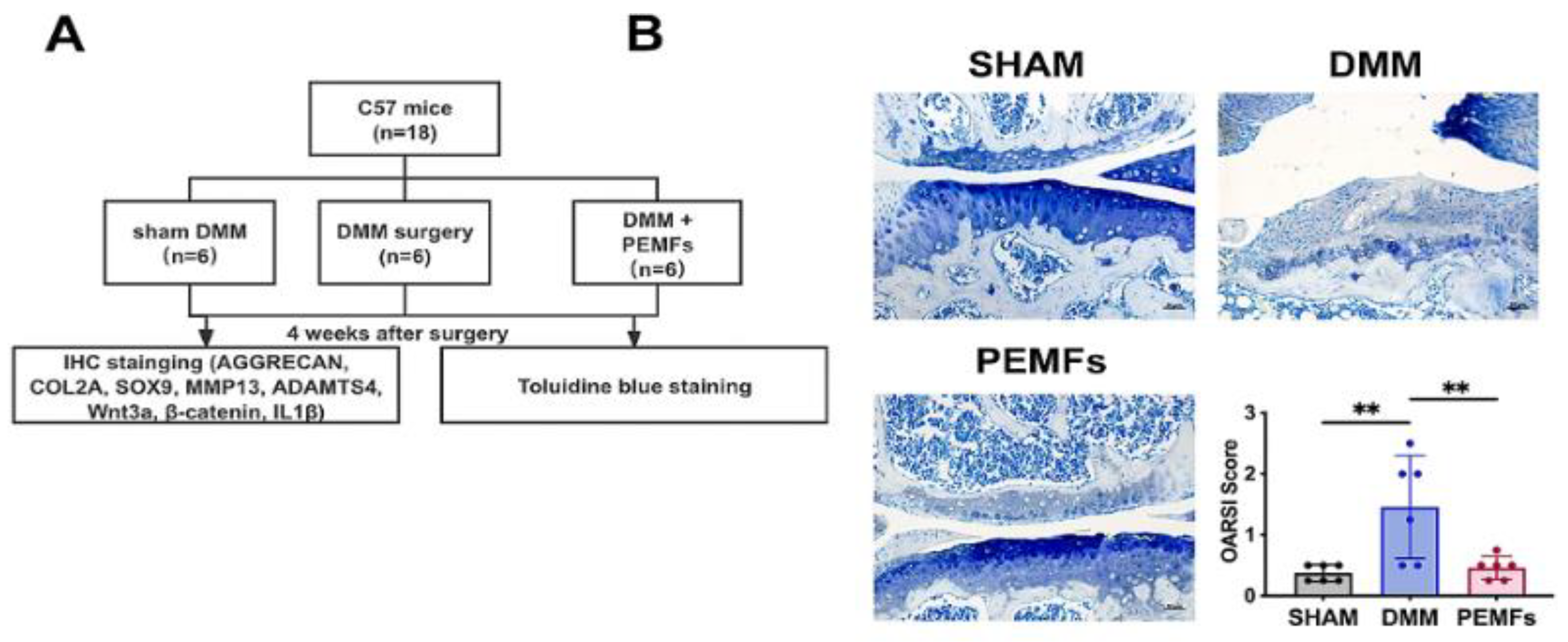
4. Effects of PEMF on Inflammation in Cartilage and Joints
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Varani, K.; Gessi, S.; Merighi, S.; Iannotta, V.; Cattabriga, E.; Spisani, S.; Cadossi, R.; Borea, P.A. Effect of low frequency electromagnetic fields on A2A adenosine receptors in human neutrophils. Br. J. Pharmacol. 2002, 136, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Borea, P.A.; Gessi, S.; Merighi, S.; Varani, K. Adenosine as a Multi-Signalling Guardian Angel in Human Diseases: When, Where and How Does it Exert its Protective Effects? Trends Pharmacol. Sci. 2016, 37, 419–434. [Google Scholar] [CrossRef] [PubMed]
- Borea, P.A.; Gessi, S.; Merighi, S.; Vincenzi, F.; Varani, K. Pathological overproduction: The bad side of adenosine: Bad sides of adenosine. Br. J. Pharmacol. 2017, 174, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Borea, P.A.; Gessi, S.; Merighi, S.; Vincenzi, F.; Varani, K. Pharmacology of Adenosine Receptors: The State of the Art. Physiol. Rev. 2018, 98, 1591–1625. [Google Scholar] [CrossRef]
- Varani, K.; De Mattei, M.; Vincenzi, F.; Gessi, S.; Merighi, S.; Pellati, A.; Ongaro, A.; Caruso, A.; Cadossi, R.; Borea, P. Characterization of adenosine receptors in bovine chondrocytes and fibroblast-like synoviocytes exposed to low frequency low energy pulsed electromagnetic fields. Osteoarthr. Cartil. 2008, 16, 292–304. [Google Scholar] [CrossRef]
- Varani, K.; Vincenzi, F.; Ravani, A.; Pasquini, S.; Merighi, S.; Gessi, S.; Setti, S.; Cadossi, M.; Borea, P.A.; Cadossi, R. Adenosine Receptors as a Biological Pathway for the Anti-Inflammatory and Beneficial Effects of Low Frequency Low Energy Pulsed Electromagnetic Fields. Mediat. Inflamm. 2017, 2017, 2740963. [Google Scholar] [CrossRef]
- Ongaro, A.; Varani, K.; Masieri, F.; Pellati, A.; Massari, L.; Cadossi, R.; Vincenzi, F.; Borea, P.; Fini, M.; Caruso, A.; et al. Electromagnetic fields (EMFs) and adenosine receptors modulate prostaglandin E2 and cytokine release in human osteoarthritic synovial fibroblasts. J. Cell. Physiol. 2012, 227, 2461–2469. [Google Scholar] [CrossRef]
- De Mattei, M.; Varani, K.; Masieri, F.; Pellati, A.; Ongaro, A.; Fini, M.; Cadossi, R.; Vincenzi, F.; Borea, P.; Caruso, A. Adenosine analogs and electromagnetic fields inhibit prostaglandin E2 release in bovine synovial fibroblasts. Osteoarthr. Cartil. 2009, 17, 252–262. [Google Scholar] [CrossRef]
- Vincenzi, F.; Targa, M.; Corciulo, C.; Gessi, S.; Merighi, S.; Setti, S.; Cadossi, R.; Goldring, M.B.; Borea, P.A.; Varani, K. Pulsed electromagnetic fields increased the anti-inflammatory effect of A2A and A3 adenosine receptors in human T/C-28a2 chondrocytes and hFOB 1.19 osteoblasts. PLoS ONE 2013, 8, e65561. [Google Scholar] [CrossRef]
- Franceschi, C.; Bonafe, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging: An Evolutionary Perspective on Immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Ross, C.L.; Zhou, Y.; McCall, C.E.; Soker, S.; Criswell, T.L. The Use of Pulsed Electromagnetic Field to Modulate Inflammation and Improve Tissue Regeneration: A Review. Bioelectricity 2019, 1, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Velnar, T.; Gradisnik, L. Tissue Augmentation in Wound Healing: The Role of Endothelial and Epithelial Cells. Med. Arch. 2018, 72, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Childs, D.R.; Murthy, A.S. Overview of Wound Healing and Management. Surg. Clin. N. Am. 2017, 97, 189–207. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.L.; Wyant, W.A.; Abdo Abujamra, B.; Kirsner, R.S.; Jozic, I. Diabetic Wound-Healing Science. Medicina 2021, 57, 1072. [Google Scholar] [CrossRef]
- Kwan, R.L.-C.; Lu, S.; Choi, H.M.-C.; Kloth, L.C.; Cheing, G.L.-Y. Efficacy of Biophysical Energies on Healing of Diabetic Skin Wounds in Cell Studies and Animal Experimental Models: A Systematic Review. Int. J. Mol. Sci. 2019, 20, 368. [Google Scholar] [CrossRef]
- Choi, H.M.; Cheing, A.K.; Ng, G.Y.; Cheing, G.L. Effects of pulsed electromagnetic field (PEMF) on the tensile biomechanical properties of diabetic wounds at different phases of healing. PLoS ONE 2018, 13, e0191074. [Google Scholar] [CrossRef]
- Goudarzi, I.; Hajizadeh, S.; Salmani, M.E.; Abrari, K. Pulsed electromagnetic fields accelerate wound healing in the skin of diabetic rats. Bioelectromagnetics 2010, 31, 318–323. [Google Scholar] [CrossRef]
- Bonkemeyer Millan, S.; Gan, R.; Townsend, P.E. Venous Ulcers: Diagnosis and Treatment. Am. Fam. Physician 2019, 100, 298–305. [Google Scholar]
- Coelho, G.A.; Secretan, P.H.; Tortolano, L.; Charvet, L.; Yagoubi, N. Evolution of the Chronic Venous Leg Ulcer Microenvironment and Its Impact on Medical Devices and Wound Care Therapies. J. Clin. Med. 2023, 12, 5605. [Google Scholar] [CrossRef]
- Mohamady, H.; Taha, M.; Aneis, Y.; Aldhahi, M.; Attalla, A. Effect of Combined Electromagnetic Field and Plantar Flexion Resistance Exercise on Wound Healing in Patients with Venous Leg Ulcers: A Randomized Controlled Trial. Medicina 2023, 59, 1157. [Google Scholar] [CrossRef]
- Ieran, M.; Zaffuto, S.; Bagnacani, M.; Annovi, M.; Moratti, A.; Cadossi, R. Effect of low frequency pulsing electromagnetic fields on skin ulcers of venous origin in humans: A double-blind study. J. Orthop. Res. 1990, 8, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Stiller, M.; Pak, G.H.; Shupack, J.; Thaler, S.; Kenny, C.; Jondreau, L. A portable pulsed electromagnetic field (PEMF) device to enhance healing of recalcitrant venous ulcers: A double-blind, placebo-controlled clinical trial. Br. J. Dermatol. 1992, 127, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Varani, K.; Vincenzi, F.; Targa, M.; Corciulo, C.; Fini, M.; Setti, S.; Cadossi, R.; Borea, P.A. Effect of pulsed electromagnetic field exposure on adenosine receptors in rat brain. Bioelectromagnetics 2012, 33, 279–287. [Google Scholar] [CrossRef]
- Vincenzi, F.; Targa, M.; Corciulo, C.; Gessi, S.; Merighi, S.; Setti, S.; Cadossi, R.; Borea, P.A.; Varani, K. The Anti-Tumor Effect of A3 Adenosine Receptors Is Potentiated by Pulsed Electromagnetic Fields in Cultured Neural Cancer Cells. PLoS ONE 2012, 7, e39317. [Google Scholar] [CrossRef] [PubMed]
- Vincenzi, F.; Ravani, A.; Pasquini, S.; Merighi, S.; Gessi, S.; Setti, S.; Cadossi, R.; Borea, P.A.; Varani, K. Pulsed Electromagnetic Field Exposure Reduces Hypoxia and Inflammation Damage in Neuron-Like and Microglial Cells: Pemfs reduce hypoxia and inflammation damage. J. Cell. Physiol. 2017, 232, 1200–1208. [Google Scholar] [CrossRef]
- Merighi, S.; Gessi, S.; Bencivenni, S.; Battistello, E.; Vincenzi, F.; Setti, S.; Cadossi, M.; Borea, P.A.; Cadossi, R.; Varani, K. Signaling pathways involved in anti-inflammatory effects of Pulsed Electromagnetic Field in microglial cells. Cytokine 2020, 125, 154777. [Google Scholar] [CrossRef]
- Stone, T.W. Purines and Neuroprotection. In Molecular and Cellular Biology of Neuroprotection in the CNS; Alzheimer, C., Ed.; Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2002; Volume 513, pp. 249–280. [Google Scholar] [CrossRef]
- Osera, C.; Amadio, M.; Falone, S.; Fassina, L.; Magenes, G.; Amicarelli, F.; Ricevuti, G.; Govoni, S.; Pascale, A. Pre-exposure of neuroblastoma cell line to pulsed electromagnetic field prevents H2O2-induced ROS production by increasing MnSOD activity: PEMF Pre-Treatment Increases MnSOD Activity. Bioelectromagnetics 2015, 36, 219–232. [Google Scholar] [CrossRef]
- Gessi, S.; Merighi, S.; Bencivenni, S.; Battistello, E.; Vincenzi, F.; Setti, S.; Cadossi, M.; Borea, P.A.; Cadossi, R.; Varani, K. Pulsed electromagnetic field and relief of hypoxia-induced neuronal cell death: The signaling pathway. J. Cell. Physiol. 2019, 234, 15089–15097. [Google Scholar] [CrossRef]
- Vincenzi, F.; Pasquini, S.; Setti, S.; Salati, S.; Cadossi, R.; Borea, P.A.; Varani, K. Pulsed Electromagnetic Fields Stimulate HIF-1α-Independent VEGF Release in 1321N1 Human Astrocytes Protecting Neuron-like SH-SY5Y Cells from Oxygen-Glucose Deprivation. Int. J. Mol. Sci. 2020, 21, 8053. [Google Scholar] [CrossRef]
- Zhang, Y.; Ding, J.; Duan, W.; Fan, W. Influence of pulsed electromagnetic field with different pulse duty cycles on neurite outgrowth in PC12 rat pheochromocytoma cells. Bioelectromagnetics 2005, 26, 406–411. [Google Scholar] [CrossRef]
- Kudo, T.-A.; Kanetaka, H.; Shimizu, Y.; Abe, T.; Mori, H.; Mori, K.; Suzuki, E.; Takagi, T.; Izumi, S.-I. Induction of Neuritogenesis in PC12 Cells by a Pulsed Electromagnetic Field via MEK-ERK1/2 Signaling. Cell Struct. Funct. 2013, 38, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Fontana, F.; Cafarelli, A.; Iacoponi, F.; Gasparini, S.; Pratellesi, T.; Koppes, A.N.; Ricotti, L. Pulsed electromagnetic field stimulation enhances neurite outgrowth in neural cells and modulates inflammation in macrophages. Eng. Regen. 2024, 5, 80–91. [Google Scholar] [CrossRef]
- Lekhraj, R.; Cynamon, D.E.; DeLuca, S.E.; Taub, E.S.; Pilla, A.A.; Casper, D. Pulsed electromagnetic fields potentiate neurite outgrowth in the dopaminergic MN9D cell line: PEMF Signals Enhance Neuronal Differentiation. J. Neurosci. Res. 2014, 92, 761–771. [Google Scholar] [CrossRef]
- Grant, G.; Cadossi, R.; Steinberg, G. Protection against focal cerebral ischemia following exposure to a pulsed electromagnetic field. Bioelectromagnetics 1994, 15, 205–216. [Google Scholar] [CrossRef]
- Albertini, A.; Zucchini, P.; Noera, G.; Cadossi, R.; Napoleone, C.P.; Pierangeli, A. Protective effect of low frequency low energy pulsing electromagnetic fields on acute experimental myocardial infarcts in rats. Bioelectromagnetics 1999, 20, 372–377. [Google Scholar] [CrossRef]
- Peng, L.; Fu, C.; Liang, Z.; Zhang, Q.; Xiong, F.; Chen, L.; He, C.; Wei, Q. Pulsed Electromagnetic Fields Increase Angiogenesis and Improve Cardiac Function After Myocardial Ischemia in Mice. Circ. J. 2020, 84, 186–193. [Google Scholar] [CrossRef]
- Weber, R.V.; Navarro, A.; Wu, J.K.; Yu, H.-L.; Strauch, B. Pulsed Magnetic Fields Applied to a Transferred Arterial Loop Support the Rat Groin Composite FlapPlast. Reconstr. Surg. 2004, 114, 1185–1189. [Google Scholar] [CrossRef]
- Pena-Philippides, J.C.; Yang, Y.; Bragina, O.; Hagberg, S.; Nemoto, E.; Roitbak, T. Effect of Pulsed Electromagnetic Field (PEMF) on Infarct Size and Inflammation After Cerebral Ischemia in Mice. Transl. Stroke Res. 2014, 5, 491–500. [Google Scholar] [CrossRef]
- Urnukhsaikhan, E.; Mishig-Ochir, T.; Kim, S.-C.; Park, J.-K.; Seo, Y.-K. Neuroprotective Effect of Low Frequency-Pulsed Electromagnetic Fields in Ischemic Stroke. Appl. Biochem. Biotechnol. 2017, 181, 1360–1371. [Google Scholar] [CrossRef]
- Cichoń, N.; Czarny, P.; Bijak, M.; Miller, E.; Śliwiński, T.; Szemraj, J.; Saluk-Bijak, J. Benign Effect of Extremely Low-Frequency Electromagnetic Field on Brain Plasticity Assessed by Nitric Oxide Metabolism during Poststroke Rehabilitation. Oxid. Med. Cell. Longev. 2017, 2017, 2181942. [Google Scholar] [CrossRef]
- Cichoń, N.; Bijak, M.; Miller, E.; Saluk, J. Extremely low frequency electromagnetic field (ELF-EMF) reduces oxidative stress and improves functional and psychological status in ischemic stroke patients: Antioxidative Effect of ELF-EMF. Bioelectromagnetics 2017, 38, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Cichoń, N.; Bijak, M.; Czarny, P.; Miller, E.; Synowiec, E.; Sliwinski, T.; Saluk-Bijak, J. Increase in Blood Levels of Growth Factors Involved in the Neuroplasticity Process by Using an Extremely Low Frequency Electromagnetic Field in Post-stroke Patients. Front. Aging Neurosci. 2018, 10, 294. [Google Scholar] [CrossRef] [PubMed]
- Cichon, N.; Saluk-Bijak, J.; Miller, E.; Sliwinski, T.; Synowiec, E.; Wigner, P.; Bijak, M. Evaluation of the effects of extremely low frequency electromagnetic field on the levels of some inflammatory cytokines in post-stroke patients. J. Rehabilitation Med. 2019, 51, 854–860. [Google Scholar] [CrossRef]
- Cichon, N.; Synowiec, E.; Miller, E.; Sliwinski, T.; Ceremuga, M.; Saluk-Bijak, J.; Bijak, M. Effect of Rehabilitation with Extremely Low Frequency Electromagnetic Field on Molecular Mechanism of Apoptosis in Post-Stroke Patients. Brain Sci. 2020, 10, 266. [Google Scholar] [CrossRef]
- Capone, F.; Liberti, M.; Apollonio, F.; Camera, F.; Setti, S.; Cadossi, R.; Quattrocchi, C.C.; Di Lazzaro, V. An open-label, one-arm, dose-escalation study to evaluate safety and tolerability of extremely low frequency magnetic fields in acute ischemic stroke. Sci. Rep. 2017, 7, 12145. [Google Scholar] [CrossRef]
- Colella, M.; Camera, F.; Capone, F.; Setti, S.; Cadossi, R.; Di Lazzaro, V.; Apollonio, F.; Liberti, M. Patient Semi-specific Computational Modeling of Electromagnetic Stimulation Applied to Neuroprotective Treatments in Acute Ischemic Stroke. Sci. Rep. 2020, 10, 2945. [Google Scholar] [CrossRef]
- Capone, F.; Zini, A.; Valzania, F.; Diomedi, M.; Tugnoli, V.; Leocani, L.; Comi, G.; Anzalone, N.; Contardi, S.; Colella, M.; et al. Neuroprotective Effects of Pulsed Electromagnetic Fields in Acute Stroke. J. Stroke 2024, 26, 458–462. [Google Scholar] [CrossRef]
- Knights, A.J.; Redding, S.J.; Maerz, T. Inflammation in osteoarthritis: The latest progress and ongoing challenges. Curr. Opin. Rheumatol. 2023, 35, 128–134. [Google Scholar] [CrossRef]
- Maldonado, M.; Nam, J. The Role of Changes in Extracellular Matrix of Cartilage in the Presence of Inflammation on the Pathology of Osteoarthritis. BioMed Res. Int. 2013, 2013, 284873. [Google Scholar] [CrossRef]
- Reboul, P.; Pelletier, J.P.; Tardif, G.; Cloutier, J.M.; Martel-Pelletier, J. The new collagenase, collagenase-3, is expressed and synthesized by human chondrocytes but not by synoviocytes. A role in osteoarthritis. J. Clin. Investig. 1996, 97, 2011–2019. [Google Scholar] [CrossRef]
- Kobayashi, M.; Squires, G.R.; Mousa, A.; Tanzer, M.; Zukor, D.J.; Antoniou, J.; Feige, U.; Poole, A.R. Role of interleukin-1 and tumor necrosis factor α in matrix degradation of human osteoarthritic cartilage. Arthritis Rheum. 2005, 52, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Goldring, M.B.; Otero, M. Inflammation in osteoarthritis. Curr. Opin. Rheumatol. 2011, 23, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Saklatvala, J. Inflammatory signaling in cartilage: MAPK and NF-kappaB pathways in chondrocytes and the use of inhibitors for research into pathogenesis and therapy of osteoarthritis. Curr. Drug Targets 2007, 8, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Pérez-García, S.; Carrión, M.; Gutiérrez-Cañas, I.; Villanueva-Romero, R.; Castro, D.; Martínez, C.; González-Álvaro, I.; Blanco, F.J.; Juarranz, Y.; Gomariz, R.P. Profile of Matrix-Remodeling Proteinases in Osteoarthritis: Impact of Fibronectin. Cells 2019, 9, 40. [Google Scholar] [CrossRef]
- Klatt, A.R.; Paul-Klausch, B.; Klinger, G.; Kühn, G.; Renno, J.H.; Banerjee, M.; Malchau, G.; Wielckens, K. A critical role for collagen II in cartilage matrix degradation: Collagen II induces pro-inflammatory cytokines and MMPs in primary human chondrocytes. J. Orthop. Res. 2009, 27, 65–70. [Google Scholar] [CrossRef]
- Benazzo, F.; Cadossi, M.; Cavani, F.; Fini, M.; Giavaresi, G.; Setti, S.; Cadossi, R.; Giardino, R. Cartilage repair with osteochondral autografts in sheep: Effect of biophysical stimulation with pulsed electromagnetic fields. J. Orthop. Res. 2008, 26, 631–642. [Google Scholar] [CrossRef]
- De Mattei, M.; Pasello, M.; Pellati, A.; Stabellini, G.; Massari, L.; Gemmati, D.; Caruso, A. Effects of electromagnetic fields on proteoglycan metabolism of bovine articular cartilage explants. Connect. Tissue Res. 2003, 44, 154–159. [Google Scholar] [CrossRef]
- Ongaro, A.; Pellati, A.; Masieri, F.F.; Caruso, A.; Setti, S.; Cadossi, R.; Biscione, R.; Massari, L.; Fini, M.; De Mattei, M. Chondroprotective effects of pulsed electromagnetic fields on human cartilage explants. Bioelectromagnetics 2011, 32, 543–551. [Google Scholar] [CrossRef]
- Ongaro, A.; Pellati, A.; Setti, S.; Masieri, F.F.; Aquila, G.; Fini, M.; Caruso, A.; De Mattei, M. Electromagnetic fields counteract IL-1β activity during chondrogenesis of bovine mesenchymal stem cells. J. Tissue Eng. Regen. Med. 2015, 9, E229–E238. [Google Scholar] [CrossRef]
- Song, K.; Hu, J.; Yang, M.; Xia, Y.; He, C.; Yang, Y.; Zhu, S. Pulsed electromagnetic fields potentiate bone marrow mesenchymal stem cell chondrogenesis by regulating the Wnt/β-catenin signaling pathway. J. Transl. Med. 2024, 22, 741. [Google Scholar] [CrossRef]
- Xu, Y.; Wang, Q.; Wang, X.-X.; Xiang, X.-N.; Peng, J.-L.; He, C.-Q.; He, H.-C. The Effect of Different Frequencies of Pulsed Electromagnetic Fields on Cartilage Repair of Adipose Mesenchymal Stem Cell–Derived Exosomes in Osteoarthritis. Cartilage 2022, 13, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Pegtel, D.M.; Gould, S.J. Exosomes. Annu. Rev. Biochem. 2019, 88, 487–514. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, L.; Li, Y.; Feng, L.; Wang, B.; Wang, M.; Wang, H.; Zhu, M.; Yang, Y.; Waldorff, E.I.; et al. Enhancing cartilage repair with optimized supramolecular hydrogel-based scaffold and pulsed electromagnetic field. Bioact. Mater. 2022, 22, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, F.; Torricelli, P.; Giavaresi, G.; Sartori, M.; Cavani, F.; Setti, S.; Cadossi, M.; Ongaro, A.; Fini, M. In Vivo effect of two different pulsed electromagnetic field frequencies on osteoarthritis. J. Orthop. Res. 2014, 32, 677–685. [Google Scholar] [CrossRef]
- Yang, X.; He, H.; Zhou, Y.; Zhou, Y.; Gao, Q.; Wang, P.; He, C. Pulsed electromagnetic field at different stages of knee osteoarthritis in rats induced by low-dose monosodium iodoacetate: Effect on subchondral trabecular bone microarchitecture and cartilage degradation: Effect of PEMF on Osteoarthritis. Bioelectromagnetics 2017, 38, 227–238. [Google Scholar] [CrossRef]
- Massari, L.; Benazzo, F.; Falez, F.; Perugia, D.; Pietrogrande, L.; Setti, S.; Osti, R.; Vaienti, E.; Ruosi, C.; Cadossi, R. Biophysical stimulation of bone and cartilage: State of the art and future perspectives. Int. Orthop. 2019, 43, 539–551. [Google Scholar] [CrossRef]
- Gobbi, A.; Lad, D.; Petrera, M.; Karnatzikos, G. Symptomatic Early Osteoarthritis of the Knee Treated With Pulsed Electromagnetic Fields. Cartilage 2014, 5, 78–85. [Google Scholar] [CrossRef]
- Benazzo, F.; Zanon, G.; Pederzini, L.; Modonesi, F.; Cardile, C.; Falez, F.; Ciolli, L.; La Cava, F.; Giannini, S.; Buda, R.; et al. Effects of biophysical stimulation in patients undergoing arthroscopic reconstruction of anterior cruciate ligament: Prospective, randomized and double blind study. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 595–601. [Google Scholar] [CrossRef]
- Zorzi, C.; Dall’Oca, C.; Cadossi, R.; Setti, S. Effects of pulsed electromagnetic fields on patients’ recovery after arthroscopic surgery: Prospective, randomized and double-blind study. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 830–834. [Google Scholar] [CrossRef]
- Cadossi, R.; Massari, L.; Racine-Avila, J.; Aaron, R.K. Pulsed Electromagnetic Field Stimulation of Bone Healing and Joint Preservation: Cellular Mechanisms of Skeletal Response. JAAOS Glob. Res. Rev. 2020, 4, e19.00155. [Google Scholar] [CrossRef]
- Hung, C.T.; Racine-Avila, J.; Pellicore, M.J.; Aaron, R. Biophysical Modulation of Mesenchymal Stem Cell Differentiation in the Context of Skeletal Repair. Int. J. Mol. Sci. 2022, 23, 3919. [Google Scholar] [CrossRef] [PubMed]
- Littman, J.; Aaron, R.K. Stimulation of Chondrogenesis in a Developmental Model of Endochondral Bone Formation by Pulsed Electromagnetic Fields. Int. J. Mol. Sci. 2023, 24, 3275. [Google Scholar] [CrossRef] [PubMed]
- Kaadan, A.; Salati, S.; Setti, S.; Aaron, R. Augmentation of Deficient Bone Healing by Pulsed Electromagnetic Fields—From Mechanisms to Clinical Outcomes. Bioengineering 2024, 11, 1223. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Treatment | Wound Healing Time (Days) | Scar Tensile Strength (N/mm2) |
|---|---|---|---|
| Diabetic Rats (n = 14) | PEMF (n = 7) | 15 * | 0.5 ** |
| Sham (n = 7) | 19 | 0.2 | |
| Non-Diabetic Rats (n = 14) | PEMF (n = 7) | 13–14 + | 0.4 ++ |
| Sham (n = 7) | 16–17 | 0.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaadan, A.; Salati, S.; Cadossi, R.; Aaron, R. Regulation of Inflammatory Responses by Pulsed Electromagnetic Fields. Bioengineering 2025, 12, 474. https://doi.org/10.3390/bioengineering12050474
Kaadan A, Salati S, Cadossi R, Aaron R. Regulation of Inflammatory Responses by Pulsed Electromagnetic Fields. Bioengineering. 2025; 12(5):474. https://doi.org/10.3390/bioengineering12050474
Chicago/Turabian StyleKaadan, Amr, Simona Salati, Ruggero Cadossi, and Roy Aaron. 2025. "Regulation of Inflammatory Responses by Pulsed Electromagnetic Fields" Bioengineering 12, no. 5: 474. https://doi.org/10.3390/bioengineering12050474
APA StyleKaadan, A., Salati, S., Cadossi, R., & Aaron, R. (2025). Regulation of Inflammatory Responses by Pulsed Electromagnetic Fields. Bioengineering, 12(5), 474. https://doi.org/10.3390/bioengineering12050474