
Exploring Pain Reduction through Physical Activity: A Case Study of Seven Fibromyalgia Patients

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Sample
2.2. Data Collection
2.2.1. Physical Activity Data
- Five participants used the Fitbit Charge 4: This model provides advanced health metrics, including heart rate monitoring, step counting, and sleep tracking. It also features GPS tracking for precise measurement of outdoor activities.
- One participant used the Fitbit Charge 3: Similar to the Charge 4 but lacks the built-in GPS feature.
- One participant used the Fitbit Versa 3: This model offers functionalities similar to the Charge 4 but includes additional features such as voice control and the ability to store and play music directly from the watch.
- Heart Rate: Continuous monitoring throughout the day and calculating the resting heart rate.
- Steps Counted: Total number of steps taken each day.
- Activity Levels: Categorized as sedentary, lightly active, moderately active, and very active.
2.2.2. Pain Data
2.2.3. Data Handling
2.3. Statistical Analysis
2.3.1. Correlation
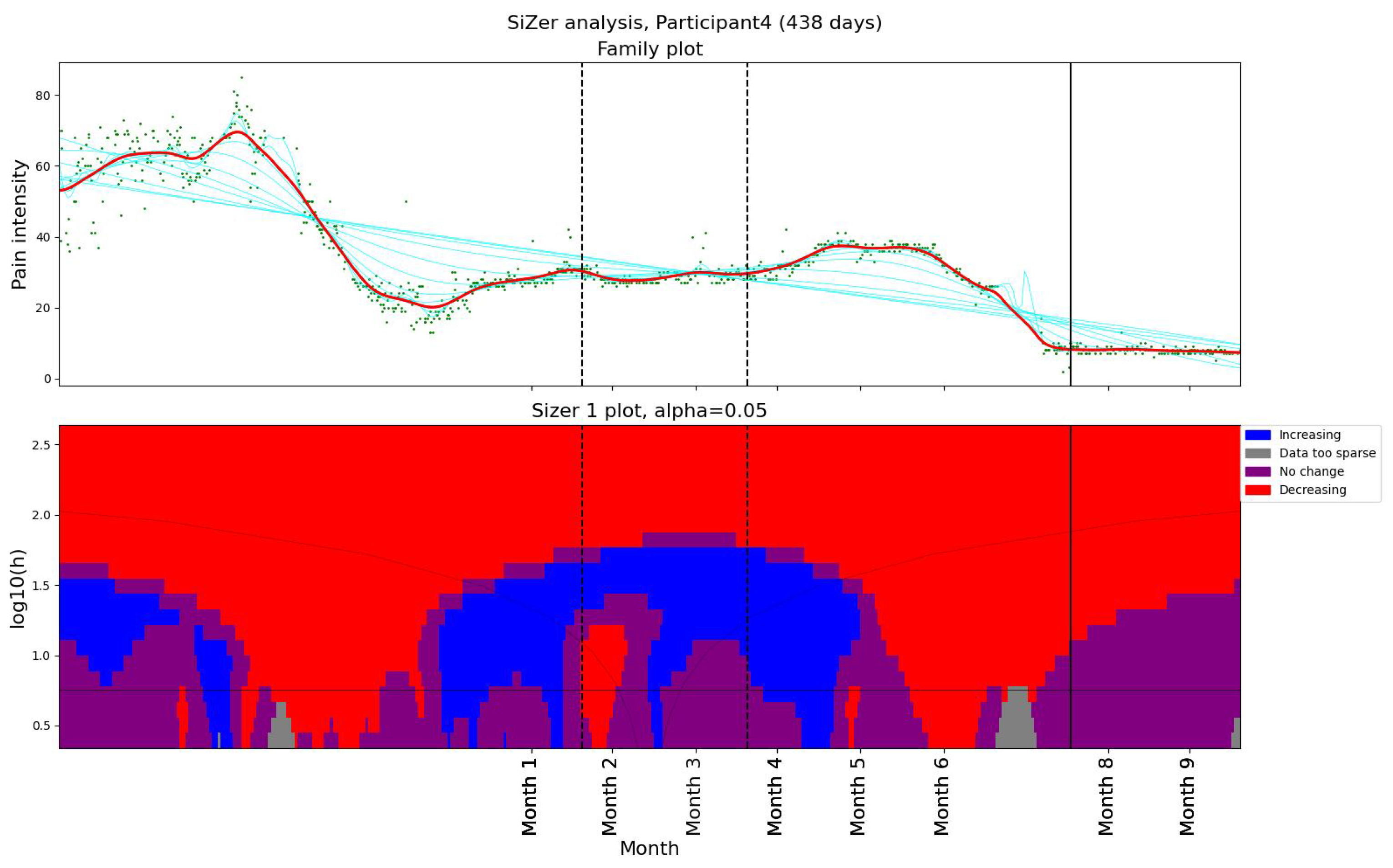
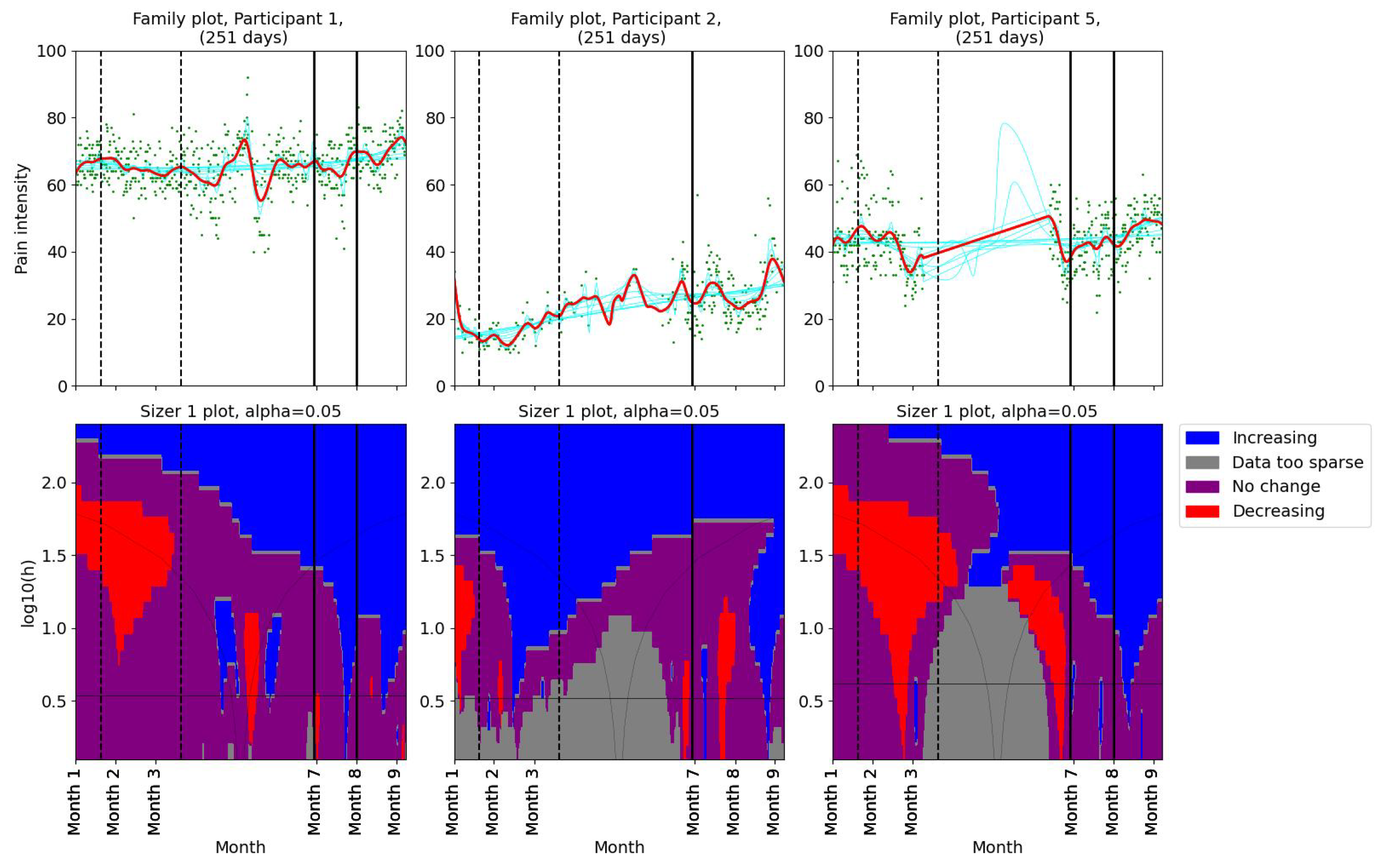
2.3.2. SiZer
2.4. Intervention
- Does spontaneous physical activity affect the pain pattern in our research participants?
- Can the results of one patient’s successful pain reduction intervention be replicated for other FM patients?
- Baseline period: the 20th of month 1–20th of month 3.
- Intervention period: the date of the first meeting with the physiotherapist—month 9.
- Background: The participants were invited to share their everyday life experiences and challenges related to chronic pain.
- Data review: Using graphs visualizing activity and pain, the physiotherapist helped the participant understand the relationship between activity and pain.
- Hypothesis formulation: The participant was encouraged to articulate her hypotheses for why activity might have an impact on chronic pain.
- Activity evaluation: The physiotherapist evaluated the activities that the participants were already doing spontaneously and challenged them to consider how to improve (e.g., increase/decrease the intensity, increase/decrease the frequency).
- Patience and care: The physiotherapist emphasized the importance of starting carefully and being patient, as changes take time.
- Goal setting: The participant and physiotherapist agreed on trying to make a change before the follow-up meeting.
- Participant 1 agreed to try increasing their activity level, dancing, and using stairs.
- Participant 2 liked walking in the woods. The plan was to increase activity level, but starting slowly.
- Participant 4 was already active and used to the activity. The plan was to continue her current activities.
- Participant 5 planned to resume walking, making sure to increase heart rate.
- Participant 6 was already used to being very active with various exercise equipment.
- Participant 9 was active with hiking and swimming. The plan was to continue her current activities.
- Participant 12 had a morning stretch routine and hiked regularly. The plan was to increase hiking speed to increase heart rate.
2.5. Questionnaire
- How did you feel about wearing a Fitbit and registering pain intensity 3 times per day for the duration of this project?
- How would you rate your level of satisfaction with the Fitbit tracker?
- How would you rate your level of satisfaction with the pain registration app?
- How did you feel about the fact that the meeting with the physiotherapist was digital, instead of in person?
- How did you feel about the physical activity plan that you have created with the physiotherapist?
- Was it useful to discuss the graphs that were provided during the meeting?
- Do you agree with this affirmation: “I think that the personalized activity plan that I followed has helped me improve my pain management”?
- If you do not agree with the affirmation above: What do you think are the reasons the personalized activity plan did not work for you?
- If offered, would you like to continue with the “assisted” personalized activity intervention?
- We are considering keeping the app up and running for 6 extra months. It would be possible to register pain 3 times a day and collect Fitbit data. However, consultations with the physiotherapist would not be available. Would you be willing to collect data for us?
- Help us improve the project. Do you have any input to share with us?
3. Results
3.1. Observed Relationships
3.2. Pain and Activity Patterns
3.2.1. Changes in Pain Levels
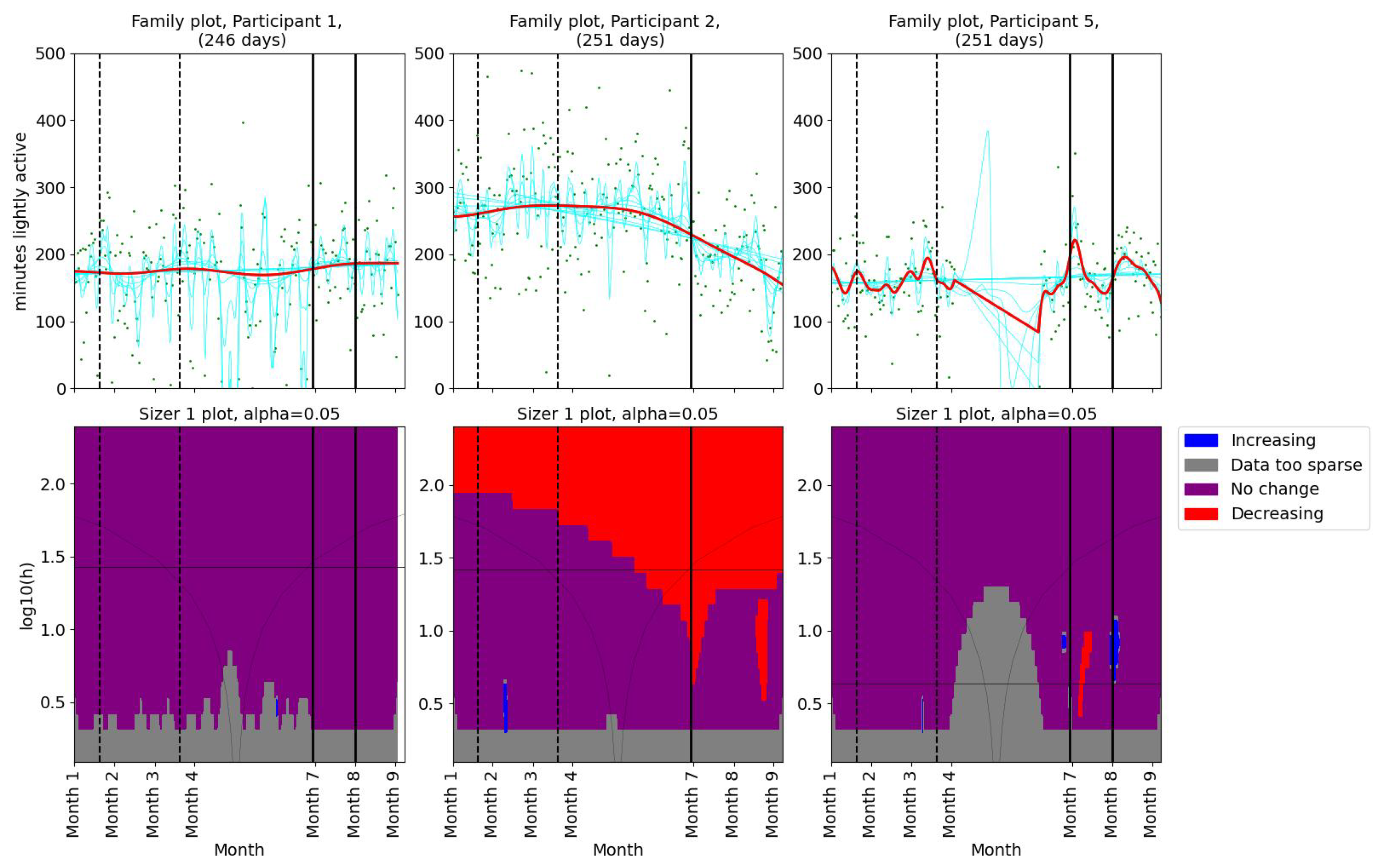
3.2.2. Changes in Activity Patterns
3.2.3. Results From the Follow-Up Meeting
- Participant 1 reported feeling unwell and bad sleep quality.
- Participant 5 reported that she had difficulties in her private life and did not prioritize physical activity.
- Participant 9 reported that she was not comfortable with walking faster. She agreed to continue being physically active and swimming.
- Participant 12 reported decreased headaches, decreased pain, and feeling better with more physical activity.
3.3. Answers From Questionnaire
4. Discussion
5. Limitations
6. Conclusions
- Does spontaneous physical activity affect the pain pattern in our research participants?
- For four participants, we detected a significant positive correlation between pain and resting heart rate. This might indicate that their physical condition affects their pain levels.
- One of the patients in this study started regular activity spontaneously, resulting in a significant improvement in pain management.
- Can the results of one patient’s successful pain reduction intervention be replicated for other FM patients?
- Three participants showed a reduction in pain while they increased their time spent lightly active per day. This suggests that personalized activity recommendations can be helpful for FM patients.
- Three participants did not experience a reduction in pain during the intervention. However, for personal reasons, they were not able to follow the recommendations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| FM | fibromyalgia |
| VAS | visual analog scale |
| SiZer | significant zero crossings of derivatives |
Appendix A
Questionnaire
- How did you feel about wearing a Fitbit and registering pain intensity 3 times a day for the duration of this project?
- 1
- It felt very uncomfortable, and I stopped doing it during the project.
- 2
- It felt uncomfortable, but I managed to do it for the duration of the project.
- 3
- Neutral.
- 4
- I was comfortable doing it for the duration of the project, but I do not feel like continuing to register/collect data for a longer time (1 participant).
- 5
- I felt comfortable doing it for the duration of the project, and I would not mind continuing to collect data. (6 participants)I do not want to answer.
- How would you rate your level of satisfaction with the Fitbit tracker?
- 1
- Very dissatisfied.
- 2
- Dissatisfied
- 3
- Neutral: neither satisfied nor dissatisfied
- 4
- Satisfied (5 participants)
- 5
- Very satisfied (2 participants)I do not want to answer.
- How would you rate your level of satisfaction with the pain registration app?
- 1
- Very dissatisfied.
- 2
- Dissatisfied
- 3
- Neutral: neither satisfied nor dissatisfied
- 4
- Satisfied (6 participants)
- 5
- Very satisfied (1 participant)I do not want to answer.
- How did you feel about the fact that the meeting with the physiotherapist was digital, instead of in person?
- 1
- It felt uncomfortable and I would not do it again.
- 2
- It felt uncomfortable, but I would do it again if it was the only option.
- 3
- Neutral: no preferences when it comes to digital VS in-person; I am comfortable with both (2 participants).
- 4
- I was comfortable with the digital meeting, but I still prefer in-person meetings (4 participants).
- 5
- I felt very comfortable with it being digital: I prefer digital meetings over in-person meetings (1 participant).I do not want to answer.
- How did you feel about the physical activity plan that you have created with the physiotherapist?
- 1
- It felt very uncomfortable and I stopped following the activity plan before the end of the project.
- 2
- It felt uncomfortable, but I managed to follow the activity plan, just to complete the project.
- 3
- Neutral (2 participants).
- 4
- I felt comfortable following my activity plan for the duration of the intervention, but I do not feel like continuing.
- 5
- I felt comfortable following my activity plan for the duration of the intervention, and I would not mind continuing (5 participants).I do not want to answer.
- Was it useful to discuss the graphs that were provided during the meeting?
- 1
- Totally useless.
- 2
- Useless.
- 3
- Neutral (4 participants).
- 4
- Useful.
- 5
- Very useful (2 participants).Did not receive graphs due to lack of Fitbit data (1 participant).
- Do you agree with this affirmation: “I think that the personalized activity plan that I followed has helped me improve my pain management”?
- 1
- Strongly disagree (2 participants).
- 2
- Disagree (2 participants).
- 3
- Neutral (2 participants).
- 4
- Agree (1 participant).
- 5
- Strongly agree.I do not want to answer.
[If the answer to question 4 is 1 or 2] - What do you think are the reasons the personalized activity plan did not work for you? You can select several answers
- I was not able to follow it due to reasons that are not related to pain or FM (e.g., I did not have time for it, I was sick) (2 participants).
- I was not able to follow it due to reasons related to pain or FM.
- The duration was too short: I think it may work if I continue following it (1 participant).
- I was not satisfied with my personalized activity plan, but I think that a different activity plan could work
- I do not think that exercising regularly can help with pain management (1 participant).
- Other (free text)
- –
- I had a good plan in place already.
Would you like to elaborate on your answer? (Free text)- I do not think that physical activity can help with pain management. But if my general health can be improved by other methods, physical activity might contribute to maintaining my health.
- Light physical activity has been helpful for my pain management.
- I have several strategies for pain management; physical activity, stress reduction, good sleep quality, and the right diet.
- If offered, would you like to continue with the “assisted” personalized activity intervention?
- Yes (6 participants).
- No (1 participant).
Would you like to elaborate on your answer? (Free text)- I found it valuable to contribute to better health and quality of life for future chronic pain patients.
- I think this is an interesting project. More research on chronic pain is needed.
- I think it is important to contribute to research on chronic pain.
- We are considering keeping the app up and running for 6 extra months. It would be possible to register pain 3 times a day and collect Fitbit data. However, consultations with the physiotherapist would not be available. Would you be willing to collect data for us?
- Yes (5 participants).
- No (2 participants).
- Help us improve the project! Do you have any input to share with us?
References
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, ITC33–ITC48. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.G.; Bennett, R.M. Pharmacological therapies in fibromyalgia. Best Pract. Res. Clin. Rheumatol. 2003, 17, 611–627. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Fitzcharles, M.A. Facts and myths pertaining to fibromyalgia. Dialogues Clin. Neurosci. 2022, 20, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Borchers, A.T.; Gershwin, M.E. Fibromyalgia: A critical and comprehensive review. Clin. Rev. Allergy Immunol. 2015, 49, 100–151. [Google Scholar] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.T.; Atzeni, F.; Beasley, M.; Flüß, E.; Sarzi-Puttini, P.; Macfarlane, G.J. The prevalence of fibromyalgia in the general population: A comparison of the American College of Rheumatology 1990, 2010, and modified 2010 classification criteria. Arthritis Rheumatol. 2015, 67, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Heidari, F.; Afshari, M.; Moosazadeh, M. Prevalence of fibromyalgia in general population and patients, a systematic review and meta-analysis. Rheumatol. Int. 2017, 37, 1527–1539. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, L.P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 1–6. [Google Scholar] [CrossRef]
- Yunus, M.B. The role of gender in fibromyalgia syndrome. Curr. Rheumatol. Rep. 2001, 3, 128–134. [Google Scholar] [CrossRef]
- Branco, J.C.; Bannwarth, B.; Failde, I.; Carbonell, J.A.; Blotman, F.; Spaeth, M.; Saraiva, F.; Nacci, F.; Thomas, E.; Caubère, J.P.; et al. Prevalence of fibromyalgia: A survey in five European countries. Semin. Arthritis Rheum. 2010, 39, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Crofford, L.J.; Mease, P.J.; Burgess, S.M.; Palmer, S.C.; Abetz, L.; Martin, S.A. Patient perspectives on the impact of fibromyalgia. Patient Educ. Couns. 2008, 73, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Sempere-Rubio, N.; Aguilar-Rodríguez, M.; Inglés, M.; Izquierdo-Alventosa, R.; Serra-Añó, P. Physical condition factors that predict a better quality of life in women with fibromyalgia. Int. J. Environ. Res. Public Health 2019, 16, 3173. [Google Scholar] [CrossRef] [PubMed]
- Annemans, L.; Le Lay, K.; Taïeb, C. Societal and patient burden of fibromyalgia syndrome. Pharmacoeconomics 2009, 27, 547–559. [Google Scholar] [CrossRef] [PubMed]
- D’Onghia, M.; Ciaffi, J.; Ruscitti, P.; Cipriani, P.; Giacomelli, R.; Ablin, J.N.; Ursini, F. The economic burden of fibromyalgia: A systematic literature review. Semin. Arthritis Rheum. 2022, 56, 152060. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, M. Epidemiology, costs, and the economic burden of fibromyalgia. Arthritis Res. Ther. 2009, 11, 117. [Google Scholar] [CrossRef] [PubMed]
- White, L.A.; Birnbaum, H.G.; Kaltenboeck, A.; Tang, J.; Mallett, D.; Robinson, R.L. Employees with fibromyalgia: Medical comorbidity, healthcare costs, and work loss. J. Occup. Environ. Med. 2008, 50, 13–24. [Google Scholar] [CrossRef]
- Chinn, S.; Caldwell, W.; Gritsenko, K. Fibromyalgia pathogenesis and treatment options update. Curr. Pain Headache Rep. 2016, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lowry, E.; Marley, J.; McVeigh, J.G.; McSorley, E.; Allsopp, P.; Kerr, D. Dietary interventions in the management of fibromyalgia: A systematic review and best-evidence synthesis. Nutrients 2020, 12, 2664. [Google Scholar] [CrossRef] [PubMed]
- Field, R.; Pourkazemi, F.; Turton, J.; Rooney, K. Dietary interventions are beneficial for patients with chronic pain: A systematic review with meta-analysis. Pain Med. 2021, 22, 694–714. [Google Scholar] [CrossRef]
- Field, R.; Pourkazemi, F.; Rooney, K. Effects of a Low-Carbohydrate Ketogenic Diet on Reported Pain, Blood Biomarkers and Quality of Life in Patients with Chronic Pain: A Pilot Randomized Clinical Trial. Pain Med. 2022, 23, 326–338. [Google Scholar] [CrossRef] [PubMed]
- Hernando-Garijo, I.; Jimenez-Del-Barrio, S.; Mingo-Gomez, T.; Medrano-de-la Fuente, R.; Ceballos-Laita, L. Effectiveness of non-pharmacological conservative therapies in adults with fibromyalgia: A systematic review of high-quality clinical trials. J. Back Musculoskelet. Rehabil. 2022, 35, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Couto, N.; Monteiro, D.; Cid, L.; Bento, T. Effect of different types of exercise in adult subjects with fibromyalgia: A systematic review and meta-analysis of randomised clinical trials. Sci. Rep. 2022, 12, 10391. [Google Scholar] [CrossRef] [PubMed]
- Mannerkorpi, K.; Henriksson, C. Non-pharmacological treatment of chronic widespread musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2007, 21, 513–534. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Ram, P.R.; Jeyaraman, M.; Jeyaraman, N.; Nallakumarasamy, A.; Khanna, M.; Gupta, A.; Yadav, S.; Ram, R. Beyond the Pain: A Systematic Narrative Review of the Latest Advancements in Fibromyalgia Treatment. Cureus 2023, 15, e48032. [Google Scholar] [CrossRef]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Overend, T.J.; Kim, S.Y.; Góes, S.M.; Boden, C.; Foulds, H.J.; Group, C.M. Aerobic exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 1996, 2017, CD012700. [Google Scholar] [CrossRef]
- Chen, J.; Han, B.; Wu, C. On the superiority of a combination of aerobic and resistance exercise for fibromyalgia syndrome: A network meta-analysis. Front. Psychol. 2022, 13, 949256. [Google Scholar] [CrossRef]
- Häuser, W.; Klose, P.; Langhorst, J.; Moradi, B.; Steinbach, M.; Schiltenwolf, M.; Busch, A. Efficacy of different types of aerobic exercise in fibromyalgia syndrome: A systematic review and meta-analysis of randomised controlled trials. Arthritis Res. Ther. 2010, 12, 1–14. [Google Scholar] [CrossRef]
- Schachter, C.L.; Busch, A.J.; Peloso, P.M.; Sheppard, M.S. Effects of short versus long bouts of aerobic exercise in sedentary women with fibromyalgia: A randomized controlled trial. Phys. Ther. 2003, 83, 340–358. [Google Scholar] [CrossRef]
- Albuquerque, M.L.L.; Monteiro, D.; Alvarez, M.C.; Vilarino, G.T.; Andrade, A.; Neiva, H.P. Effects of strength training in fibromyalgia on balance, neuromuscular performance, and symptomatic analysis: A 12-week study protocol. Front. Neurol. 2023, 14, 1149268. [Google Scholar] [CrossRef]
- Vancampfort, D.; Van Damme, T.; Albanio Machado, V.; McGrath, R.L.; Stubbs, B.; Schuch, F.B. Levels of sedentary behaviour in people with fibromyalgia: A systematic review and meta-analysis. Disabil. Rehabil. 2024, 46, 1921–1927. [Google Scholar] [CrossRef]
- Ocagli, H.; Agarinis, R.; Azzolina, D.; Zabotti, A.; Treppo, E.; Francavilla, A.; Bartolotta, P.; Todino, F.; Binutti, M.; Gregori, D.; et al. Physical activity assessment with wearable devices in rheumatic diseases: A systematic review and meta-analysis. Rheumatology 2023, 62, 1031–1046. [Google Scholar] [CrossRef]
- Nijs, J.; Roussel, N.; Van Oosterwijck, J.; De Kooning, M.; Ickmans, K.; Struyf, F.; Meeus, M.; Lundberg, M. Fear of movement and avoidance behaviour toward physical activity in chronic-fatigue syndrome and fibromyalgia: State of the art and implications for clinical practice. Clin. Rheumatol. 2013, 32, 1121–1129. [Google Scholar] [CrossRef]
- Leon-Llamas, J.L.; Murillo-Garcia, A.; Villafaina, S.; Domínguez-Muñoz, F.J.; Morenas, J.; Gusi, N. Relationship between kinesiophobia and mobility, impact of the disease, and fear of falling in women with and without fibromyalgia: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 8257. [Google Scholar] [CrossRef]
- Vader, K.; Doulas, T.; Patel, R.; Miller, J. Experiences, barriers, and facilitators to participating in physical activity and exercise in adults living with chronic pain: A qualitative study. Disabil. Rehabil. 2021, 43, 1829–1837. [Google Scholar] [CrossRef]
- Fitbit Official Site. Available online: https://www.fitbit.com (accessed on 16 May 2024).
- Ringeval, M.; Wagner, G.; Denford, J.; Paré, G.; Kitsiou, S. Fitbit-based interventions for healthy lifestyle outcomes: Systematic review and meta-analysis. J. Med. Internet Res. 2020, 22, e23954. [Google Scholar] [CrossRef]
- Lazaridou, A.; Paschali, M.; Schreiber, K.; Galenkamp, L.; Berry, M.; Paschalis, T.; Napadow, V.; Edwards, R.R. The association between daily physical exercise and pain among women with fibromyalgia: The moderating role of pain catastrophizing. Pain Rep. 2020, 5, e832. [Google Scholar] [CrossRef]
- Izquierdo-Alventosa, R.; Inglés, M.; Cortés-Amador, S.; Gimeno-Mallench, L.; Chirivella-Garrido, J.; Kropotov, J.; Serra-Añó, P. Low-intensity physical exercise improves pain catastrophizing and other psychological and physical aspects in women with fibromyalgia: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 3634. [Google Scholar] [CrossRef]
- Ambrose, K.R.; Golightly, Y.M. Physical exercise as non-pharmacological treatment of chronic pain: Why and when. Best Pract. Res. Clin. Rheumatol. 2015, 29, 120–130. [Google Scholar] [CrossRef]
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise therapy for fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef]
- Borisovskaya, A.; Chmelik, E.; Karnik, A. Exercise and chronic pain. In Physical Exercise for Human Health; Springer: Singapore, 2020; pp. 233–253. [Google Scholar]
- Masquelier, E.; D’haeyere, J. Physical activity in the treatment of fibromyalgia. Jt. Bone Spine 2021, 88, 105202. [Google Scholar] [CrossRef]
- Lucini, D.; Giovanelli, L.; Bazzichi, L.; Bernardelli, G.; Pellegrino, G.; Filippou, G.; Sarzi-Puttini, P. Tailored exercise programmes for fibromyalgia: A clinical practice guide. Clin. Exp. Rheumatol. 2024, 42, 1262–1271. [Google Scholar] [CrossRef]
- Norges Fibromyalgiforbund. Available online: https://fibromyalgi.no/ (accessed on 14 May 2024).
- Karni, L.; Dalal, K.; Memedi, M.; Kalra, D.; Klein, G.O. Information and communications technology–based interventions targeting patient empowerment: Framework development. J. Med. Internet Res. 2020, 22, e17459. [Google Scholar] [CrossRef]
- Reips, U.D.; Funke, F. Interval-level measurement with visual analogue scales in Internet-based research: VAS Generator. Behav. Res. Methods 2008, 40, 699–704. [Google Scholar] [CrossRef]
- Crichton, N. Visual analogue scale (VAS). J. Clin. Nurs. 2001, 10, 697–706. [Google Scholar]
- Walpole, R.; Myers, R.; Myers, S.; Ye, K. Probability and Statistics for Engineers and Scientists; Pearson: London, UK, 2016. [Google Scholar]
- Chaudhuri, P.; Marron, J.S. SiZer for exploration of structures in curves. J. Am. Stat. Assoc. 1999, 94, 807–823. [Google Scholar] [CrossRef]
- Rondonotti, V.; Marron, J.; Park, C. SiZer for time series: A new approach to the analysis of trends. Electron. J. Stat. 2007, 1, 268–289. [Google Scholar] [CrossRef]
- Jones, M.C.; Marron, J.S.; Sheather, S.J. A brief survey of bandwidth selection for density estimation. J. Am. Stat. Assoc. 1996, 91, 401–407. [Google Scholar] [CrossRef]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert scale: Explored and explained. Br. J. Appl. Sci. Technol. 2015, 7, 396. [Google Scholar] [CrossRef]
- Juhlin, S.; Bergenheim, A.; Gjertsson, I.; Larsson, A.; Mannerkorpi, K. Physical activity with person-centred guidance supported by a digital platform for persons with chronic widespread pain: A randomized controlled trial. J. Rehabil. Med. 2021, 53, 2756. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Noma, H.; Caldwell, D.M.; Honyashiki, M.; Shinohara, K.; Imai, H.; Chen, P.; Hunot, V.; Churchill, R. Waiting list may be a nocebo condition in psychotherapy trials: A contribution from network meta-analysis. Acta Psychiatr. Scand. 2014, 130, 181–192. [Google Scholar] [CrossRef]
- Sælensminde, K.; Line, T.M. Samfunnskostnader ved Sykdom og Ulykker 2015; Report; Norwegian Directory of Health: Oslo, Norway, 2015; Available online: https://www.helsedirektoratet.no/rapporter/samfunnskostnader-ved-sykdom-og-ulykker/Samfunnskostnader%20ved%20sykdom%20og%20ulykker%202015.pdf/_/attachment/inline/761dd2be-6458-4baf-99c9-34d58a621aad:e3291994cf460a6d1c5174eab5f27b4165208afe/Samfunnskostnader%20ved%20sykdom%20og%20ulykker%202015.pdf (accessed on 8 February 2023).
- PraksisNett. Available online: https://www.uib.no/praksisnett (accessed on 16 May 2024).
- Kaleycheva, N.; Cullen, A.E.; Evans, R.; Harris, T.; Nicholson, T.; Chalder, T. The role of lifetime stressors in adult fibromyalgia: Systematic review and meta-analysis of case-control studies. Psychol. Med. 2021, 51, 177–193. [Google Scholar] [CrossRef]
- Vancampfort, D.; Van Damme, T.; Brunner, E.; McGrath, R.L.; Hemmings, L.; Guimaraes, M.E.; Schuch, F. Dropout from exercise interventions in adults with fibromyalgia: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2023, 105, 571–579. [Google Scholar] [CrossRef]
- Feehan, L.M.; Geldman, J.; Sayre, E.C.; Park, C.; Ezzat, A.M.; Yoo, J.Y.; Hamilton, C.B.; Li, L.C. Accuracy of Fitbit devices: Systematic review and narrative syntheses of quantitative data. JMIR MHealth UHealth 2018, 6, e10527. [Google Scholar] [CrossRef]
- Germini, F.; Noronha, N.; Borg Debono, V.; Abraham Philip, B.; Pete, D.; Navarro, T.; Keepanasseril, A.; Parpia, S.; de Wit, K.; Iorio, A. Accuracy and acceptability of wrist-wearable activity-tracking devices: Systematic review of the literature. J. Med. Internet Res. 2022, 24, e30791. [Google Scholar] [CrossRef]
- Balbim, G.M.; Marques, I.G.; Marquez, D.X.; Patel, D.; Sharp, L.K.; Kitsiou, S.; Nyenhuis, S.M. Using Fitbit as an mHealth intervention tool to promote physical activity: Potential challenges and solutions. JMIR MHealth UHealth 2021, 9, e25289. [Google Scholar] [CrossRef]
- Hackshaw, K.V.; Plans-Pujolras, M.; Rodriguez-Saona, L.E.; Moore, M.A.; Jackson, E.K.; Sforzo, G.A.; Buffington, C.T. A pilot study of health and wellness coaching for fibromyalgia. BMC Musculoskelet. Disord. 2016, 17, 457. [Google Scholar] [CrossRef]
- Andersson, U.M.; Åberg, A.C.; von Koch, L.; Palstam, A. Women with fibromyalgia prefer resistance exercise with heavy loads—A randomized crossover pilot study. Int. J. Environ. Res. Public Health 2021, 18, 6276. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Variable | Test Statistic | p-Value | # Values |
|---|---|---|---|---|
| Participant 1 | Resting heart rate | 0.256 | <0.001 | 333 |
| Participant 2 | Minutes lightly active | −0.265 | <0.001 | 254 |
| Participant 2 | Steps | −0.247 | <0.001 | 254 |
| Participant 2 | Resting heart rate | 0.334 | <0.001 | 254 |
| Participant 9 | Minutes spent sedentary | 0.234 | <0.001 | 246 |
| Participant 9 | Resting heart rate | 0.167 | 0.005 | 238 |
| Participant 12 | Minutes spent very active | −0.120 | 0.036 | 224 |
| Participant 12 | Resting heart rate | 0.419 | <0.001 | 223 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jenssen, M.D.K.; Salvi, E.; Fors, E.A.; Nilsen, O.A.; Ngo, P.D.; Tejedor, M.; Bellika, J.G.; Godtliebsen, F. Exploring Pain Reduction through Physical Activity: A Case Study of Seven Fibromyalgia Patients. Bioengineering 2024, 11, 765. https://doi.org/10.3390/bioengineering11080765
Jenssen MDK, Salvi E, Fors EA, Nilsen OA, Ngo PD, Tejedor M, Bellika JG, Godtliebsen F. Exploring Pain Reduction through Physical Activity: A Case Study of Seven Fibromyalgia Patients. Bioengineering. 2024; 11(8):765. https://doi.org/10.3390/bioengineering11080765
Chicago/Turabian StyleJenssen, Marit Dagny Kristine, Elisa Salvi, Egil Andreas Fors, Ole Andreas Nilsen, Phuong Dinh Ngo, Miguel Tejedor, Johan Gustav Bellika, and Fred Godtliebsen. 2024. "Exploring Pain Reduction through Physical Activity: A Case Study of Seven Fibromyalgia Patients" Bioengineering 11, no. 8: 765. https://doi.org/10.3390/bioengineering11080765
APA StyleJenssen, M. D. K., Salvi, E., Fors, E. A., Nilsen, O. A., Ngo, P. D., Tejedor, M., Bellika, J. G., & Godtliebsen, F. (2024). Exploring Pain Reduction through Physical Activity: A Case Study of Seven Fibromyalgia Patients. Bioengineering, 11(8), 765. https://doi.org/10.3390/bioengineering11080765