

The Role of Cyanoacrylate after Mandibular Third Molar Surgery: A Single Center Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
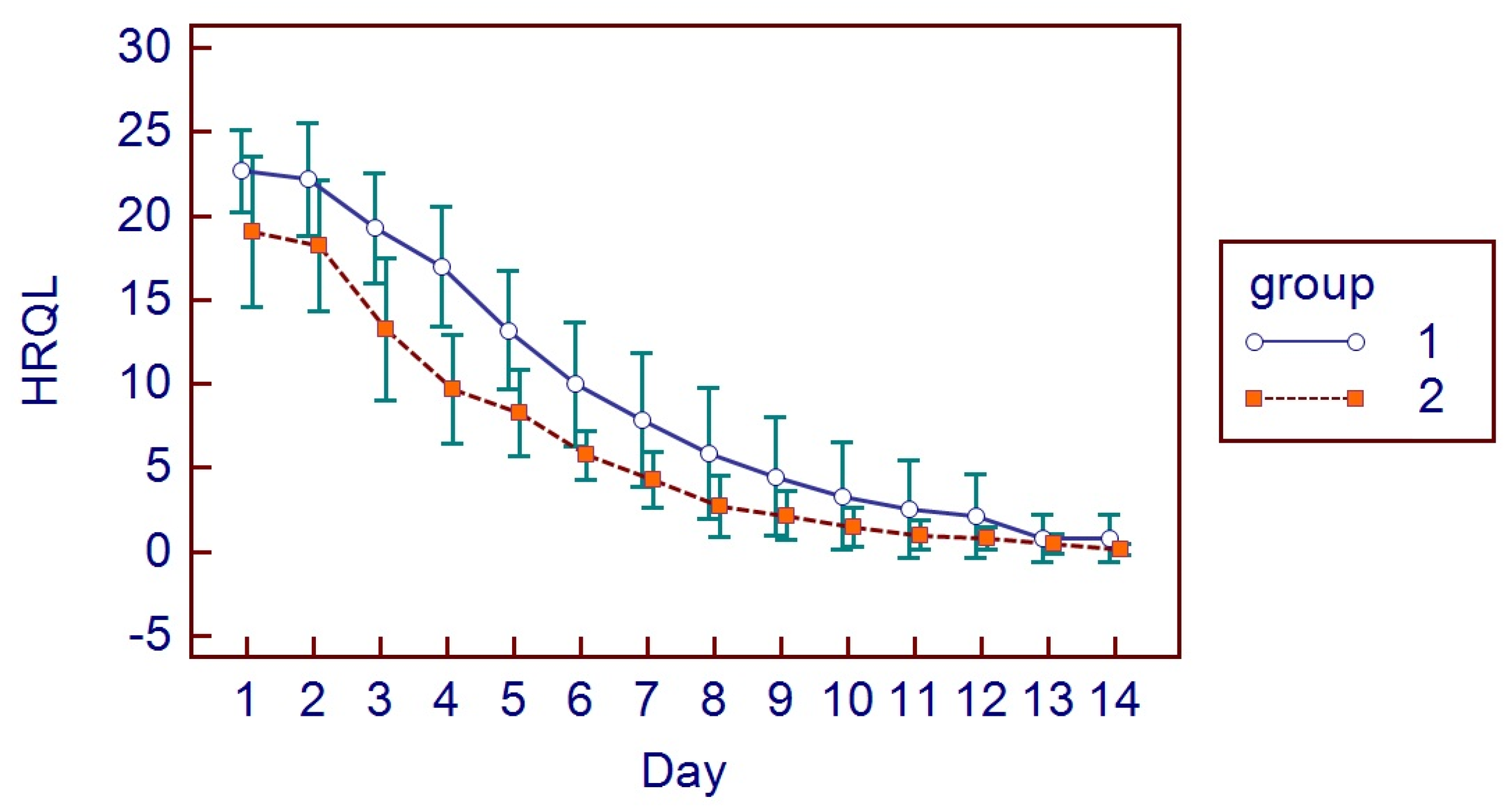
2.3. Health-Related Quality of Life
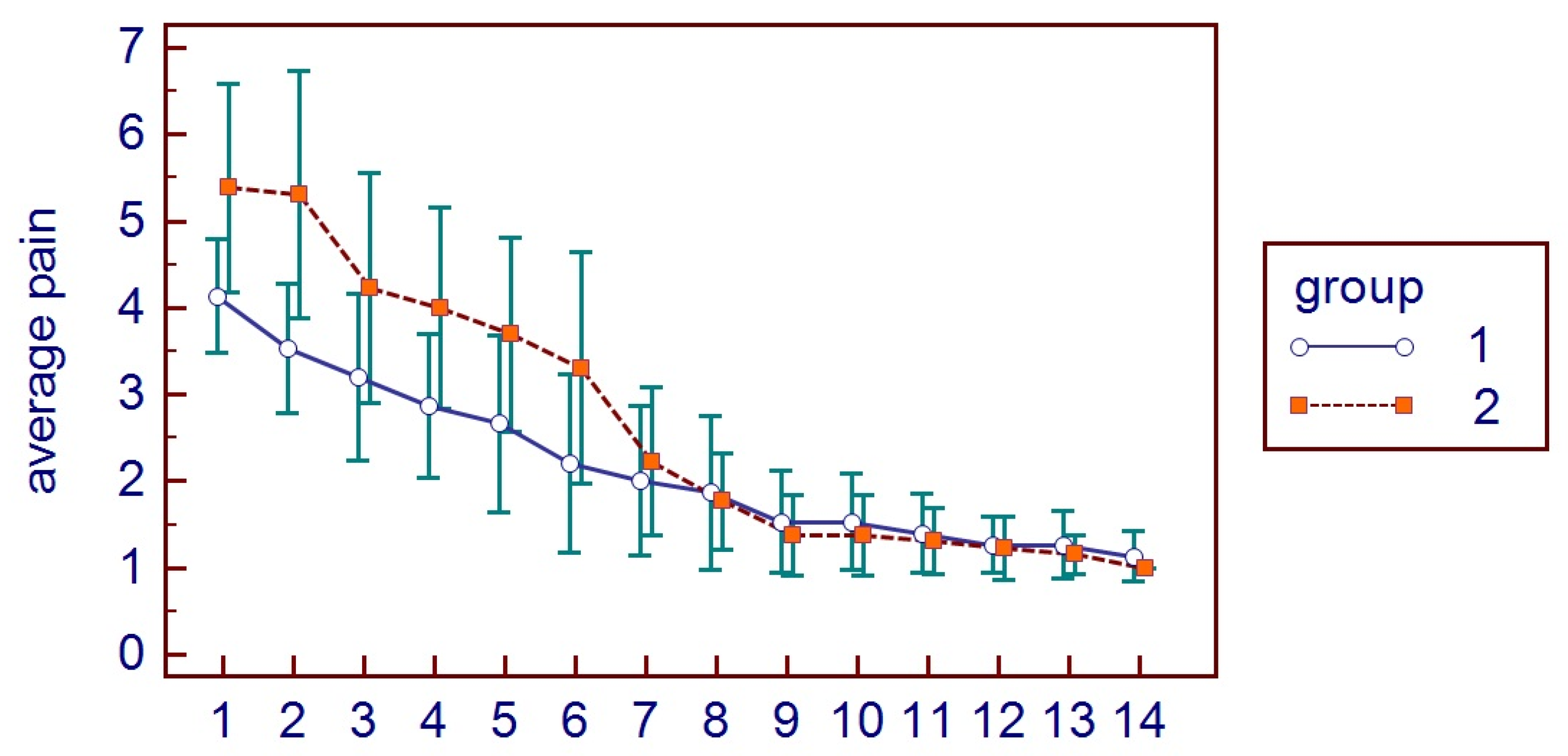
2.4. Pain
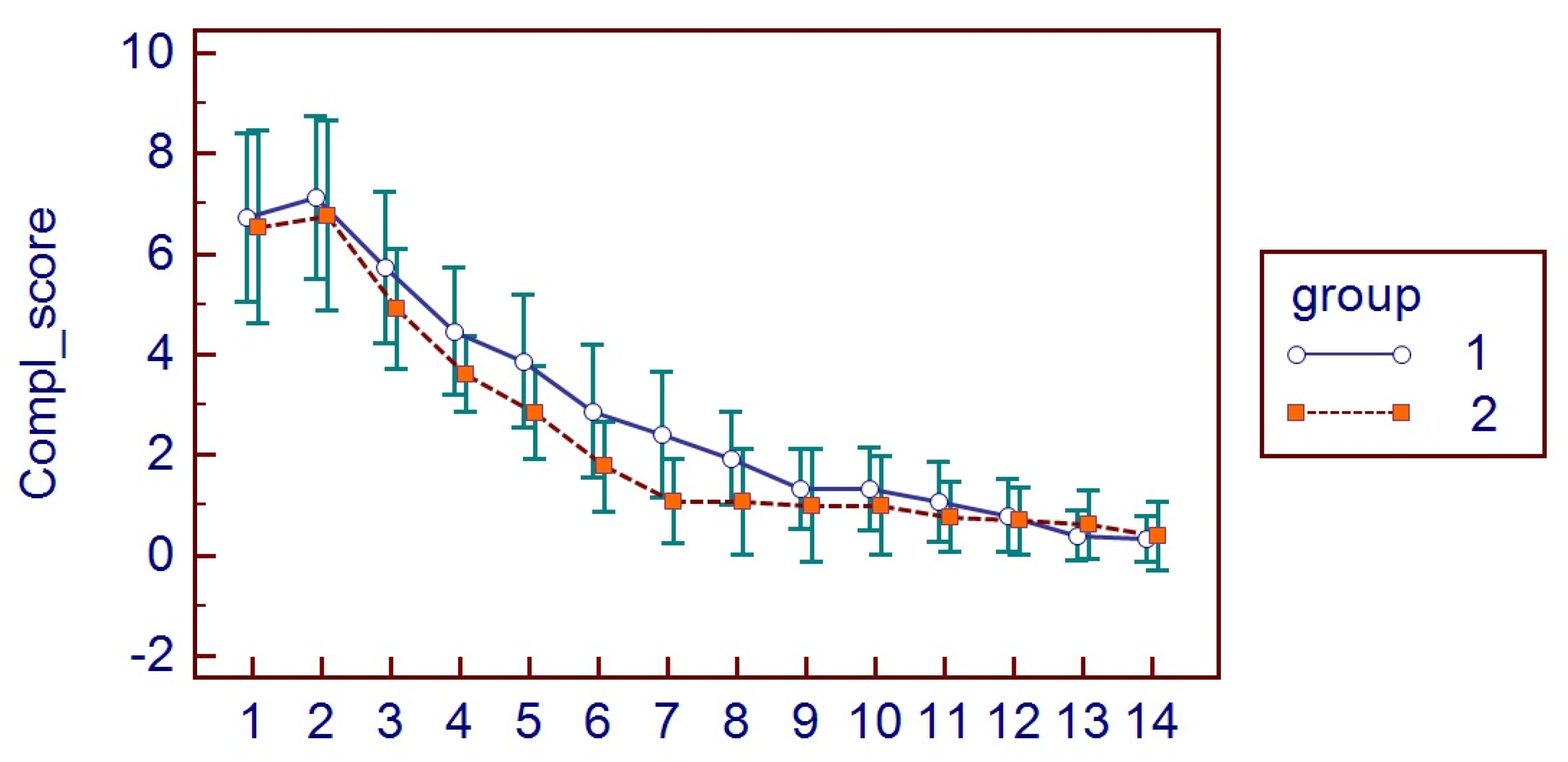
2.5. Complications Score
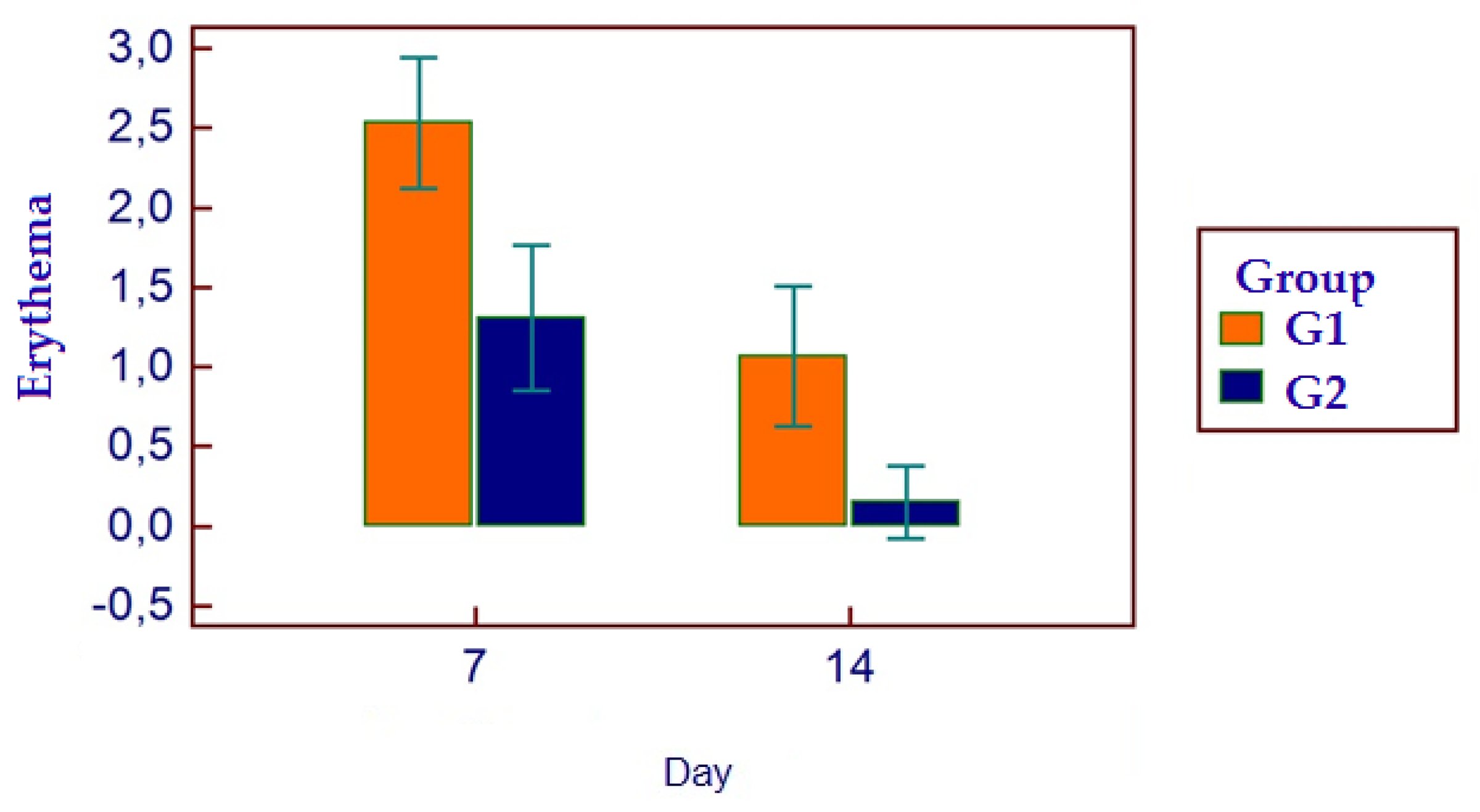
2.6. Facial Swelling and Erythema
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chisci, D.; Parrini, S.; Baldini, N.; Chisci, G. Patterns of Third-Molar-Pericoronitis-Related Pain: A Morphometrical Observational Retrospective Study. Healthcare 2023, 11, 1890. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Omran, A.; Hutchison, I.; Ridout, F.; Bose, A.; Maroni, R.; Dhanda, J.; Hammond, D.; Moynihan, C.; Ciniglio, A.; Chiu, G. Current perspectives on the surgical management of mandibular third molars in the United Kingdom: The need for further research. Br. J. Oral. Maxillofac. Surg. 2020, 58, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Labra, A.; Brignardello-Petersen, R.; Yanine, N.; Araya, I.; Guyatt, G. Secondary versus primary closure techniques for the prevention of postoperative complications following removal of impacted mandibular third molars: A systematic review and meta-analysis of randomized controlled trials. J. Oral. Maxillofac. Surg. 2012, 70, e441–e457. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Li, X.; Zhang, A.; Liu, S.; Zhao, H.; Zhao, H. Efficacy of secondary closure technique after extraction of third molars: A meta-analysis. Br. J. Oral. Maxillofac. Surg. 2019, 57, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Azab, M.; Ibrahim, S.; Li, A.; Khosravirad, A.; Carrasco-Labra, A.; Zeng, L.; Brignardello-Petersen, R. Efficacy of secondary vs primary closure techniques for the prevention of postoperative complications after impacted mandibular third molar extractions: A systematic review update and meta-analysis. J. Am. Dent. Assoc. 2022, 153, 943–956.e48. [Google Scholar] [CrossRef] [PubMed]
- Chisci, G.; De Felice, C.; Parrini, S.; Signorini, C.; Leoncini, S.; Ciccoli, L.; Volpi, N.; Capuano, A. The role of preoperative oxidative stress and mandibular third molar postoperative outcome. Int. J. Oral. Maxillofac. Surg. 2013, 42, 1499–1500. [Google Scholar] [CrossRef] [PubMed]
- Parrini, S.; Chisci, G.; Leoncini, S.; Signorini, C.; Volpi, N.; Capuano, A.; Ciccoli, L.; De Felice, C. F2-Isoprostanes in soft oral tissues and degree of oral disability after mandibular third molar surgery. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2012, 114, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Candotto, V.; Oberti, L.; Gabrione, F.; Scarano, A.; Rossi, D.; Romano, M. Complication in third molar extractions. J. Biol. Regul. Homeost. Agents. 2019, 33 (Suppl. S1), 169–172. [Google Scholar] [PubMed]
- Pogrel, M.A. What is the effect of timing of removal on the incidence and severity of complications? J. Oral. Maxillofac. Surg. 2012, 70 (Suppl. S1), S37–S40. [Google Scholar] [CrossRef] [PubMed]
- Waite, P.D.; Cherala, S. Surgical outcomes for suture-less surgery in 366 impacted third molar patients. J. Oral. Maxillofac. Surg. 2006, 64, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Sharma, P.; Chhabra, S.; Bali, R. Comparative Evaluation of Suture Versus Sutureless Surgery in Mandibular Third Molar Impactions. J. Maxillofac. Oral. Surg. 2022, 21, 620–626. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alkadi, S.; Stassen, L. Effect of One-Suture and Sutureless Techniques on Postoperative Healing After Third Molar Surgery. J. Oral. Maxillofac. Surg. 2019, 77, e1–e703. [Google Scholar] [CrossRef] [PubMed]
- Athavale, A.; Thao, M.; Sassaki, V.S.; Lewis, M.; Chandra, V.; Fukaya, E. Cyanoacrylate glue reactions: A systematic review, cases, and proposed mechanisms. J. Vasc. Surg. Venous Lymphat. Disord. 2023, 11, 876–888.e1. [Google Scholar] [CrossRef] [PubMed]
- Haghpanah, S.; Vafafar, A.; Golzadeh, M.H.; Ardeshiri, R.; Karimi, M. Use of Glubran 2 and Glubran tissue skin adhesive in patients with hereditary bleeding disorders undergoing circumcision and dental extraction. Ann. Hematol. 2011, 90, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Idle, M.R.; Monaghan, A.M.; Lamin, S.M.; Grant, S.W. N-butyl-2-cyanoacrylate (NBCA) tissue adhesive as a haemostatic agent in a venous malformation of the mandible. Br. J. Oral. Maxillofac. Surg. 2013, 51, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Pell, G.; Gregory, B. Impacted mandibular third molars: Classification and modified techniques for removal. Dent. Dig. 1933, 39, 330–338. [Google Scholar]
- Duarte-Rodrigues, L.; Miranda, E.F.P.; Souza, T.O.; de Paiva, H.N.; Falci, S.G.M.; Galvão, E.L. Third molar removal and its impact on quality of life: Systematic review and meta-analysis. Qual. Life Res. 2018, 27, 2477–2489. [Google Scholar] [CrossRef] [PubMed]
- Ibikunle, A.A.; Adeyemo, W.L. Oral Health-Related Quality of Life Following Third Molar Surgery in an African Population. Contemp. Clin. Dent. 2017, 8, 545–551. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shugars, D.A.; Gentile, M.A.; Ahmad, N.; Stavropoulos, M.F.; Slade, G.D.; Phillips, C.; Conrad, S.M.; Fleuchaus, P.T.; White, R.P., Jr. Assessment of oral health-related quality of life before and after third molar surgery. J. Oral. Maxillofac. Surg. 2006, 64, 1721–1730. [Google Scholar] [CrossRef] [PubMed]
- White, R.P., Jr.; Shugars, D.A.; Shafer, D.M.; Laskin, D.M.; Buckley, M.J.; Phillips, C. Recovery after third molar surgery: Clinical and health-related quality of life outcomes. J. Oral. Maxillofac. Surg. 2003, 61, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Mahat, A.K.; Yadav, R.; Yadav, A.K.; Acharya, P.; Dongol, A.; Sagtani, A.; Jaisani, M.R. A Comparative Study of the Effect of Sutureless Versus Multiple Sutures Technique on Complications following Third Molar Surgery in Nepalese Subpopulation. Int. J. Dent. 2020, 2020, 9314762. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Møller, J.F.; Petersen, J.K. Efficacy of a fibrin sealant on healing of extraction wounds. Int. J. Oral. Maxillofac. Surg. 1988, 17, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Marco de Lucas, E.; Gutiérrez, A.; González Mandly, A.; García-Pire, F.; Marco de Lucas, M.T.; Parra, J.A.; Sáiz-Bustillo, R. Life-threatening pseudoaneurysm of the facial artery after dental extraction: Successful treatment with emergent endovascular embolization. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2008, 106, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Ghoreishian, M.; Gheisari, R.; Fayazi, M. Tissue adhesive and suturing for closure of the surgical wound after removal of impacted mandibular third molars: A comparative study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2009, 108, e14–e16. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.D.; Saluja, H.; Mahindra, U.; Halli, R. A comparative study: Efficacy of tissue glue and sutures after impacted mandibular third molar removal. J. Maxillofac. Oral. Surg. 2011, 10, 310–315. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wasson, M.; Ghodke, B.; Dillon, J.K. Exsanguinating hemorrhage following third molar extraction: Report of a case and discussion of materials and methods in selective embolization. J. Oral. Maxillofac. Surg. 2012, 70, 2271–2275. [Google Scholar] [CrossRef] [PubMed]
- Sagara, Y.; Kiyosue, H.; Tanoue, S.; Shimada, R.; Hongo, N.; Kohno, T.; Kawano, K.; Mori, H. Selective transarterial embolization with n-butyl-2-cyanoacrylate for the treatment of arterial hemorrhage after third molar extraction. Neuroradiology 2013, 55, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Chisci, G.; Chisci, D.; Chisci, E.; Chisci, V.; Stumpo, M.; Chisci, E. The Management of a Geriatric Patient Using Dabigatran Therapy on Dentigerous Cyst with Oral Bleeding. J. Clin. Med. 2024, 13, 1499. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tokuyama, K.; Kiyosue, H.; Shimada, R.; Miyamoto, S.; Abe, A.; Kawano, K.; Asayama, Y. Selective transarterial embolization for arterial hemorrhage after upper third molar extraction: Illustrative cases. J. Neurosurg. Case Lessons 2023, 6, CASE23118. [Google Scholar] [CrossRef] [PubMed]
- Gogulanathan, M.; Elavenil, P.; Gnanam, A.; Raja, V.B. Evaluation of fibrin sealant as a wound closure agent in mandibular third molar surgery--a prospective, randomized controlled clinical trial. Int. J. Oral. Maxillofac. Surg. 2015, 44, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Oladega, A.A.; James, O.; Adeyemo, W.L. Cyanoacrylate tissue adhesive or silk suture for closure of surgical wound following removal of an impacted mandibular third molar: A randomized controlled study. J. Craniomaxillofac Surg. 2019, 47, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Chisci, G.; Capuano, A.; Parrini, S. Alveolar Osteitis and Third Molar Pathologies. J. Oral. Maxillofac. Surg. 2018, 76, 235–236. [Google Scholar] [CrossRef] [PubMed]
- Parrini, S.; Bovicelli, A.; Chisci, G. Microbiological Retention on PTFE versus Silk Suture: A Quantitative Pilot Study in Third Molar Surgery. Antibiotics 2023, 12, 562. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stran-Lo Giudice, A.F.; Ortiz, A.M.; Sánchez-Labrador, L.; Cortés-Bretón Brinkmann, J.; Cobo-Vázquez, C.M.; Meniz-García, C. Current status of split-mouth controlled clinical trials comparing cyanoacrylate vs. conventional suture after lower third molar surgeries: A systematic literature review. Acta Odontol. Scand. 2023, 81, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.J.F.; Monteiro, J.L.G.C.; Moraes, S.L.D.; Vasconcelos, B.C.E.; Pellizzer, E.P. Clinical comparison of conventional suture and tissue adhesive in third molar surgeries: A systematic review. Gen. Dent. 2023, 71, 25–29. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographic Data | Group1 | Group2 | SMD (Standardized Mean Difference) |
|---|---|---|---|
| Age (mean (SD)) | 30.53 (±9.77) | 31.85 (±10.51) | 1.32 |
| Sex (Female/Male) | 22/18 | 17/20 | 5/2 |
| Surgical site (Right/Left) | 19/22 | 21/16 | 2/6 |
| G1 Mean ± (SD) | G2 Mean ± (SD) | |
|---|---|---|
| HRQL | 9.43 ± (9.49) | 6.23 ± (7.42) |
| CS | 2.88 ± (3) | 2.36 ± (2.77) |
| MP | 2.75 ± (1.86) | 3.5 ± (2.57) |
| AP | 2.19 ± (1.57) | 2.67 ± (2.11) |
| erythema | 1.70 ± (1.08) | 0.73 ± (0.82) |
| FS | 2 ± (1.08) | 0.69 ± (0.78) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrini, S.; Arzente, G.; Bartali, E.; Chisci, G. The Role of Cyanoacrylate after Mandibular Third Molar Surgery: A Single Center Study. Bioengineering 2024, 11, 569. https://doi.org/10.3390/bioengineering11060569
Parrini S, Arzente G, Bartali E, Chisci G. The Role of Cyanoacrylate after Mandibular Third Molar Surgery: A Single Center Study. Bioengineering. 2024; 11(6):569. https://doi.org/10.3390/bioengineering11060569
Chicago/Turabian StyleParrini, Stefano, Giulia Arzente, Elena Bartali, and Glauco Chisci. 2024. "The Role of Cyanoacrylate after Mandibular Third Molar Surgery: A Single Center Study" Bioengineering 11, no. 6: 569. https://doi.org/10.3390/bioengineering11060569
APA StyleParrini, S., Arzente, G., Bartali, E., & Chisci, G. (2024). The Role of Cyanoacrylate after Mandibular Third Molar Surgery: A Single Center Study. Bioengineering, 11(6), 569. https://doi.org/10.3390/bioengineering11060569