Author Contributions
Conceptualization, L.R. and A.S.; methodology, L.R., P.W., S.A.P. and G.F.; software, G.F. and S.A.P.; formal analysis, S.A.P. and G.F.; investigation, A.-G.S. and L.R..; resources, M.C.; data curation, A.-G.S., L.R. and G.F.; writing—original draft preparation, M.S.; writing—review and editing, L.R., A.S., M.C., P.W. and G.F.; visualization, S.A.P. and G.F.; supervision, L.R., S.A.P. and P.W.; project administration, A.-G.S. and L.R. All authors have read and agreed to the published version of the manuscript.
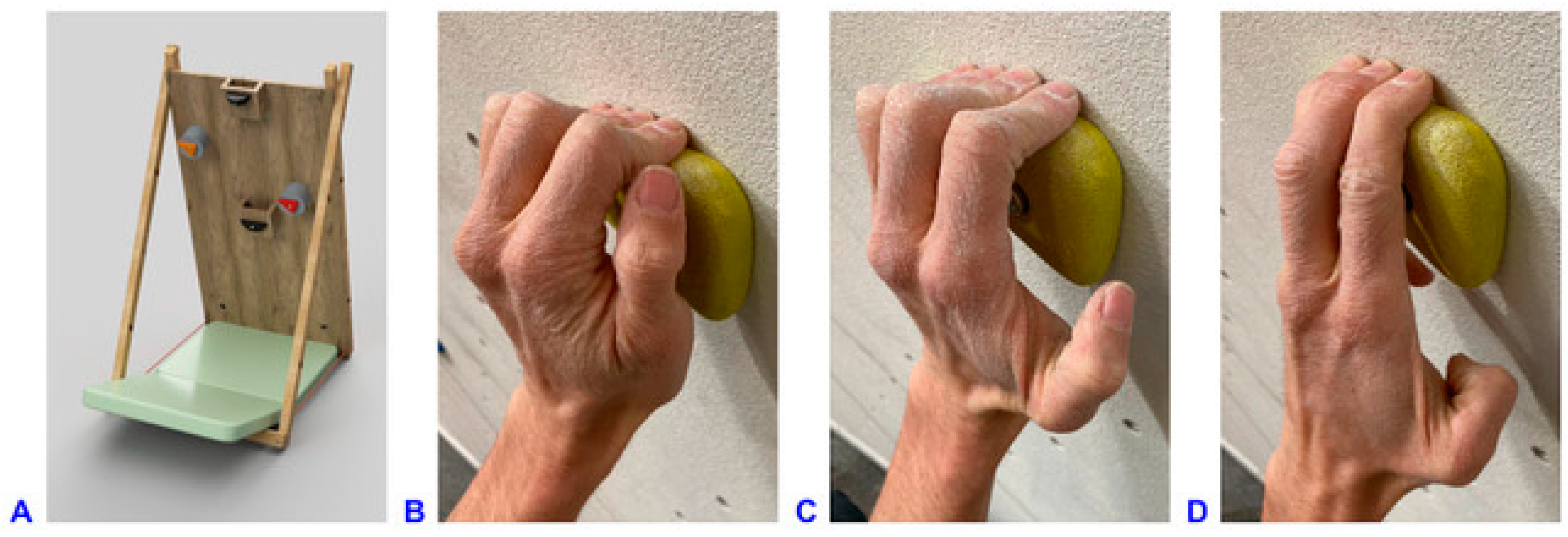
Figure 1.
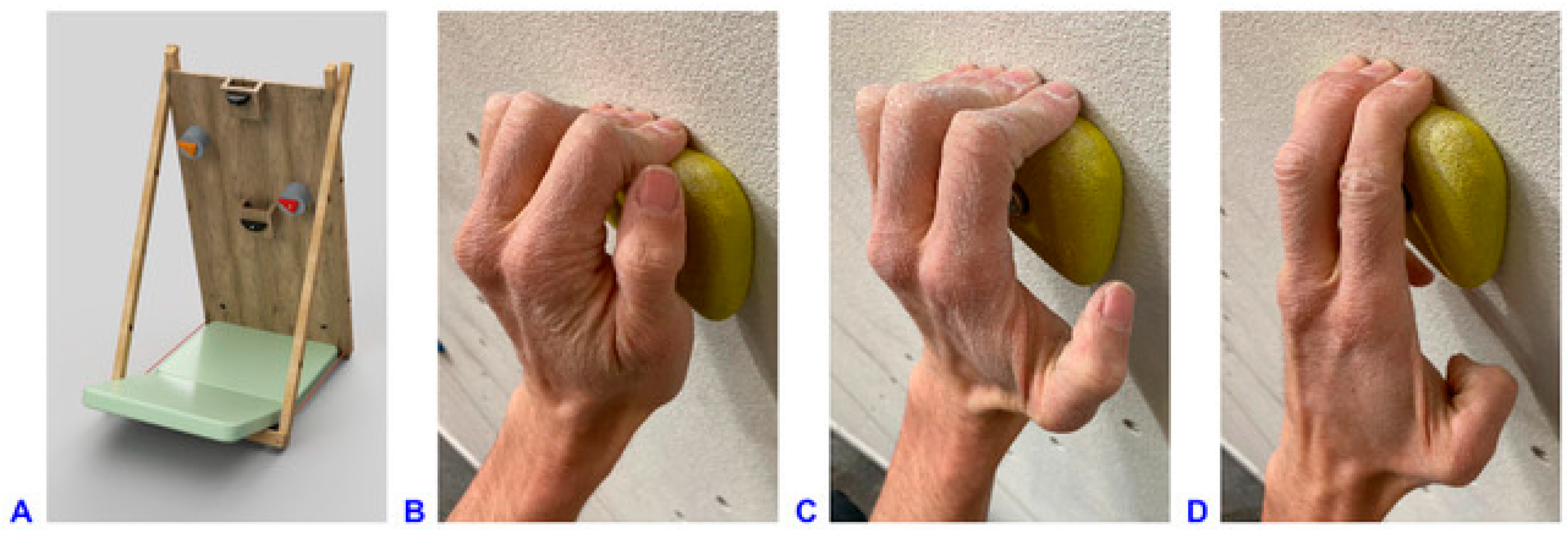
(A) 3D representation of the climbing wall used in the experiment. Climbing wall dimensions: 100 cm × 200 cm, −20° inclination angle, removable square board of 86 cm × 74 cm at the central bottom of the wall. Dimensions and position coordinates of the holds (@ refers to position of the holds with respect to the coordinate system origin at the lower left corner of the climbing wall): left foothold: 20 mm deep @15 cm/25 cm; right foothold: 20 mm deep @85 cm/25 cm; starting hold: 180 mm wide, 36 mm deep @50 cm/110 cm, placed on wooden box 105 mm deep; right instrumented hold (red): 110 mm wide, 23 mm deep, 25° incut angle, @75 cm/130 cm, placed on load cell unit 105 mm deep; left instrumented hold (orange): 110 mm wide, 23 mm deep, 25° incut angle, 15/160 cm, placed on load cell unit 105 mm deep; top hold: 140 mm wide, 75 mm deep @50 cm/198 cm. (B) Crimp grip with flexed PIP (approximately 90°) and hyperextended DIP joints, without using the thumb. (C) Half-crimp grip with only slightly flexed or even straight little finger, leading to less PIP joint flexion and not fully hyperextended DIP joints. (D) Open-hand grip with straight index finger, with (four-finger open-hand) or without (three-finger drag, shown in picture) little finger on the hold.
Figure 1.
(A) 3D representation of the climbing wall used in the experiment. Climbing wall dimensions: 100 cm × 200 cm, −20° inclination angle, removable square board of 86 cm × 74 cm at the central bottom of the wall. Dimensions and position coordinates of the holds (@ refers to position of the holds with respect to the coordinate system origin at the lower left corner of the climbing wall): left foothold: 20 mm deep @15 cm/25 cm; right foothold: 20 mm deep @85 cm/25 cm; starting hold: 180 mm wide, 36 mm deep @50 cm/110 cm, placed on wooden box 105 mm deep; right instrumented hold (red): 110 mm wide, 23 mm deep, 25° incut angle, @75 cm/130 cm, placed on load cell unit 105 mm deep; left instrumented hold (orange): 110 mm wide, 23 mm deep, 25° incut angle, 15/160 cm, placed on load cell unit 105 mm deep; top hold: 140 mm wide, 75 mm deep @50 cm/198 cm. (B) Crimp grip with flexed PIP (approximately 90°) and hyperextended DIP joints, without using the thumb. (C) Half-crimp grip with only slightly flexed or even straight little finger, leading to less PIP joint flexion and not fully hyperextended DIP joints. (D) Open-hand grip with straight index finger, with (four-finger open-hand) or without (three-finger drag, shown in picture) little finger on the hold.
![Bioengineering 11 00370 g001]()
Figure 2.
Applied marker set with 23 hemispherical 3 mm markers on the hand and 4 spherical 5 mm-markers on the forearm of each hand. The kinematic evaluation was based on 8 segments per hand defined by the marker clusters on the forearm, palm, and the proximal, intermediate and distal phalanges of the fingers. The flexion axis of the joints was determined by a functional approach.
Figure 2.
Applied marker set with 23 hemispherical 3 mm markers on the hand and 4 spherical 5 mm-markers on the forearm of each hand. The kinematic evaluation was based on 8 segments per hand defined by the marker clusters on the forearm, palm, and the proximal, intermediate and distal phalanges of the fingers. The flexion axis of the joints was determined by a functional approach.
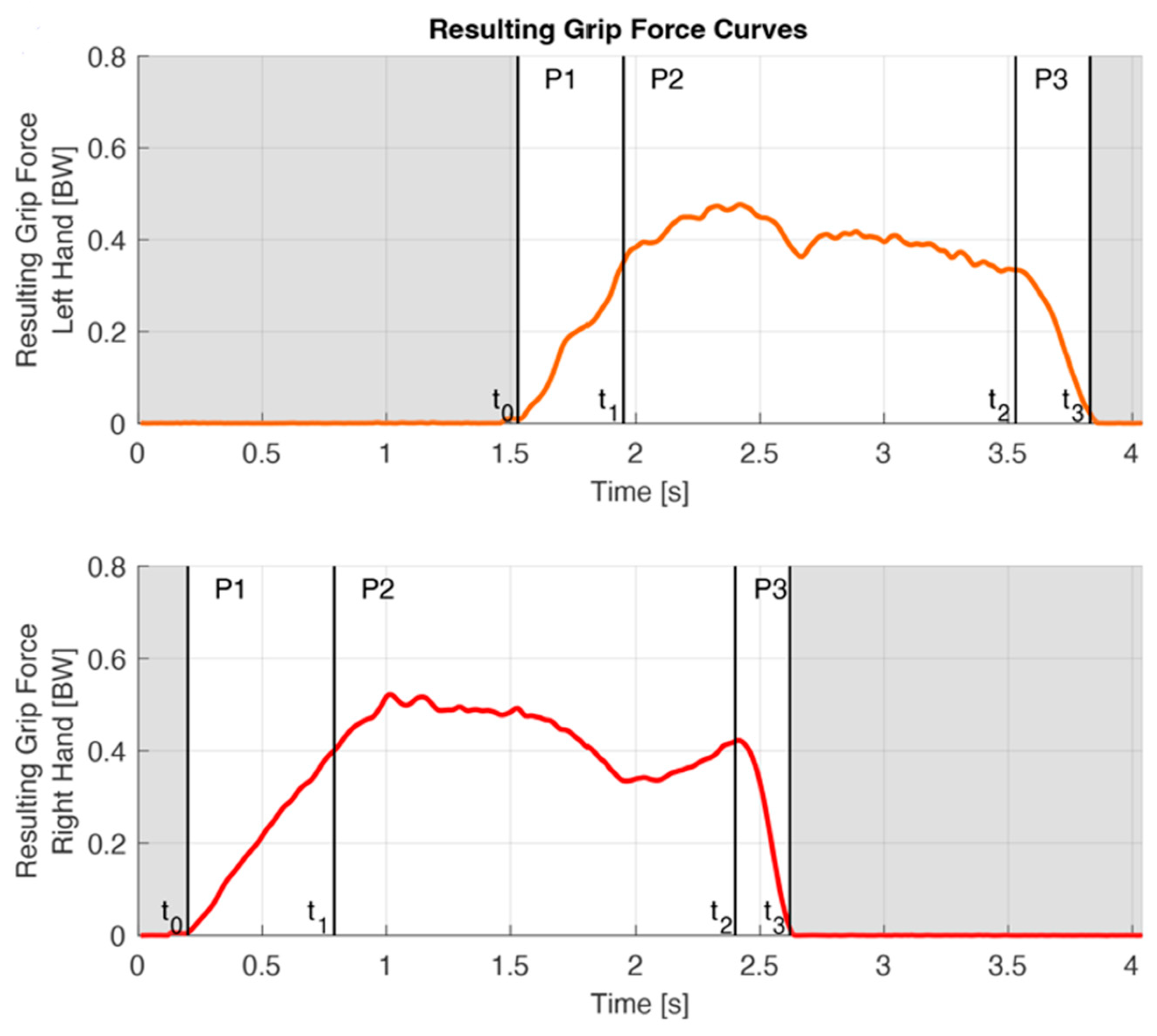
Figure 3.
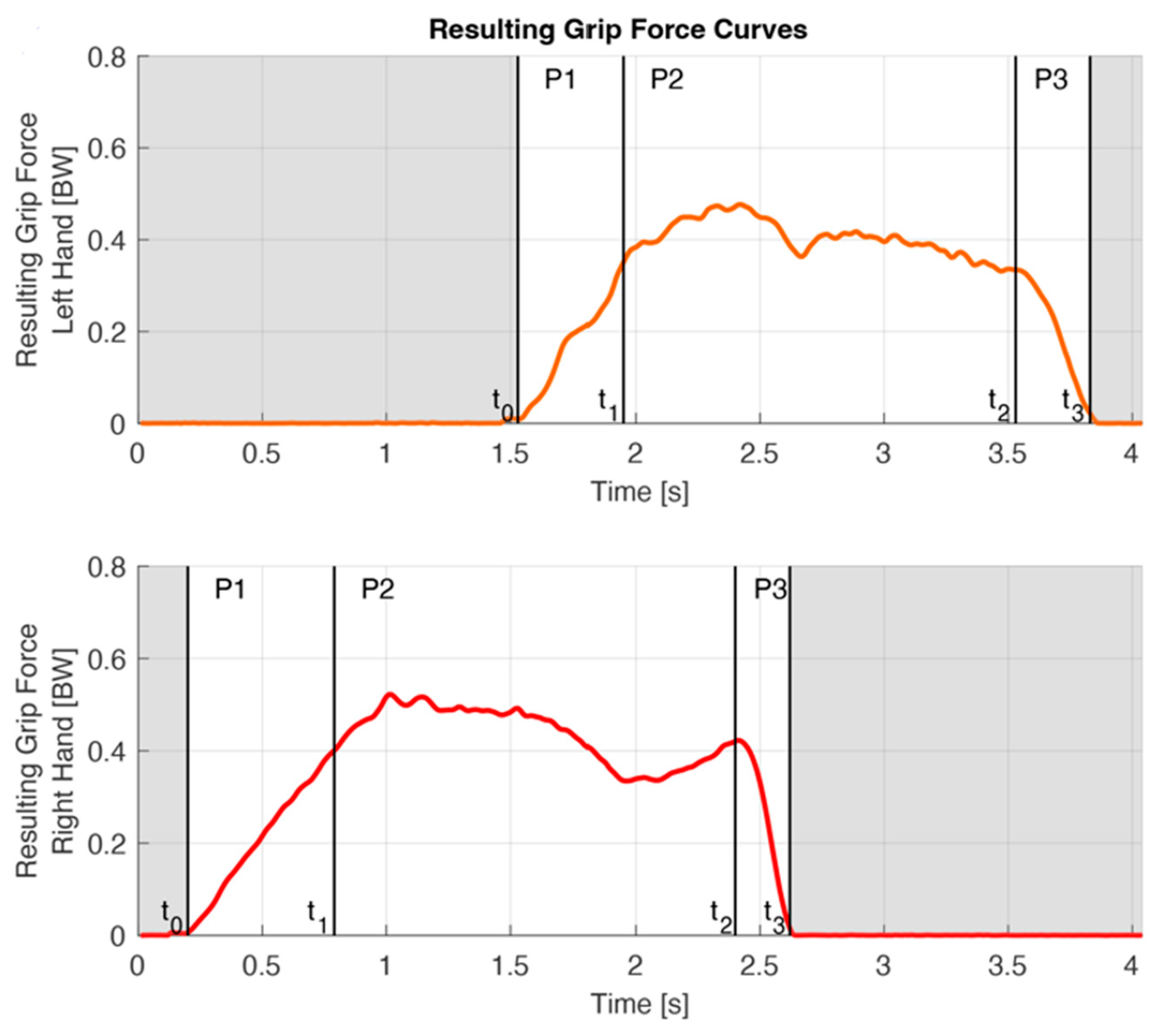
On the basis of the force curves, the handhold contact period was divided into three phases: the grabbing, holding and releasing phase (P1–P3) bordered by four phase transitions (t0–t3), here shown for a crimp grip trial. The red line refers to the resulting grip force of the right hand, the orange line to that of the right hand. Initial contact t0 was defined as the penultimate frame before 15N was exceeded for the first time during a trial or, in the case of a regrip, as the point of time of the local minimum of the force curve. Left t1 was determined by the moment of the local load minimum on the right hand between left t0 and right t2. Right t1 was assumed based on the average duration of P1 of the left hand, as the starting hold was not instrumented. (Note that right and left P1 durations are different in a single trial, as the right P1 duration was assumed based on the mean P1 duration of all trials of the left.) t2 was defined as the last moment before the slope of the kinetic curve drops below −1.5 N per frame (0.01 s). t3 was defined as the data point two frames after the interaction force fell below 15 N for the last time during a trial.
Figure 3.
On the basis of the force curves, the handhold contact period was divided into three phases: the grabbing, holding and releasing phase (P1–P3) bordered by four phase transitions (t0–t3), here shown for a crimp grip trial. The red line refers to the resulting grip force of the right hand, the orange line to that of the right hand. Initial contact t0 was defined as the penultimate frame before 15N was exceeded for the first time during a trial or, in the case of a regrip, as the point of time of the local minimum of the force curve. Left t1 was determined by the moment of the local load minimum on the right hand between left t0 and right t2. Right t1 was assumed based on the average duration of P1 of the left hand, as the starting hold was not instrumented. (Note that right and left P1 durations are different in a single trial, as the right P1 duration was assumed based on the mean P1 duration of all trials of the left.) t2 was defined as the last moment before the slope of the kinetic curve drops below −1.5 N per frame (0.01 s). t3 was defined as the data point two frames after the interaction force fell below 15 N for the last time during a trial.
![Bioengineering 11 00370 g003]()
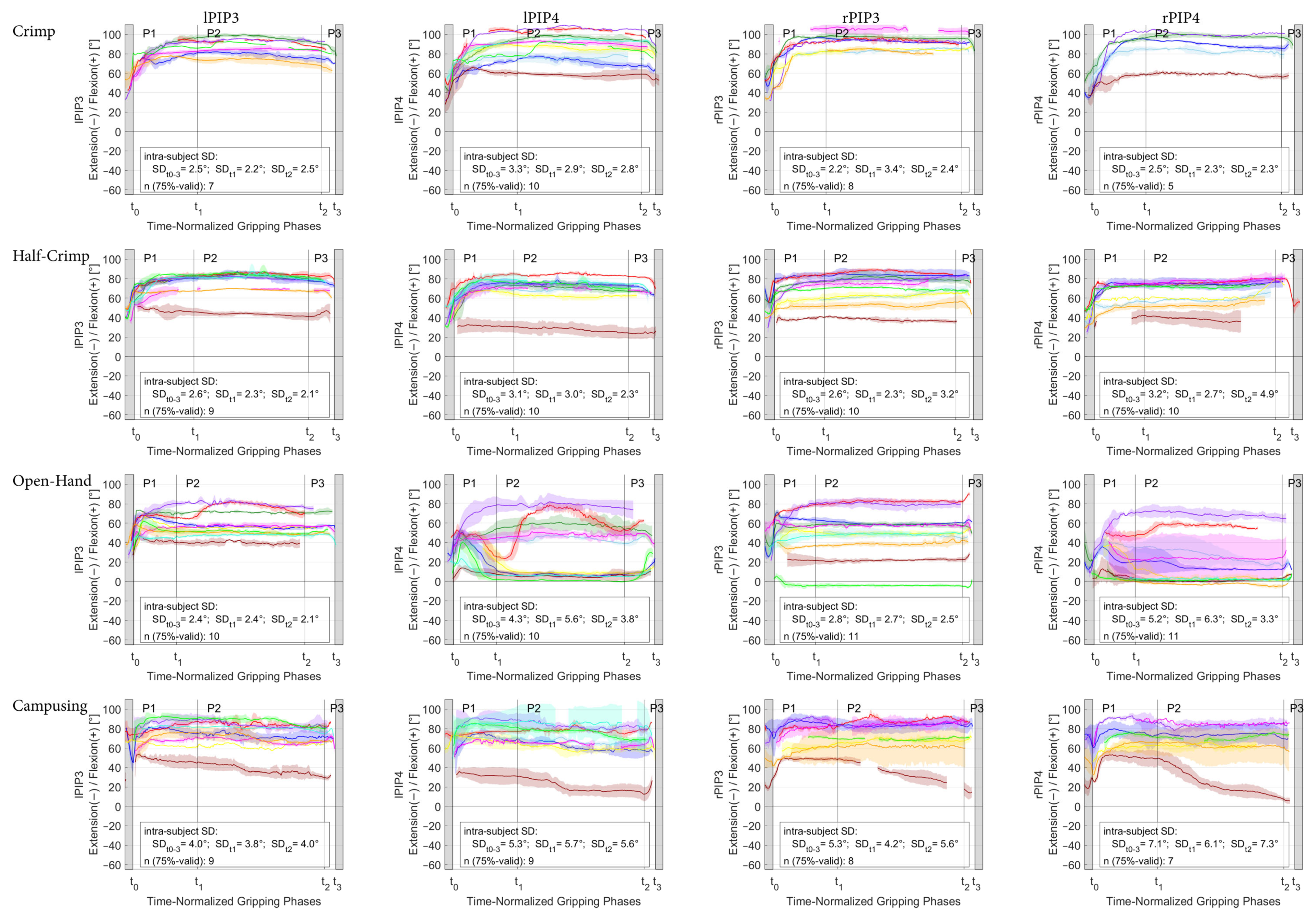
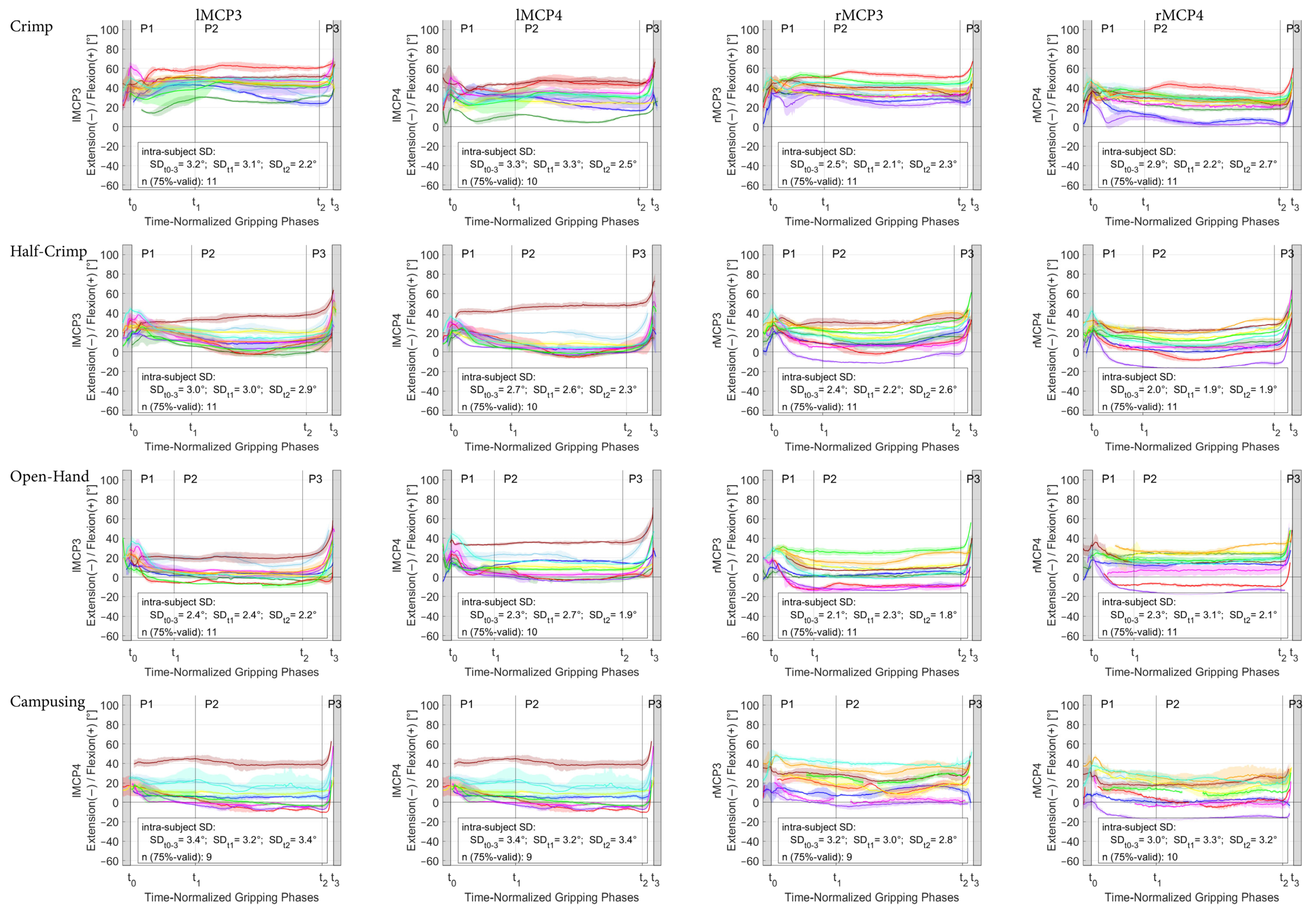
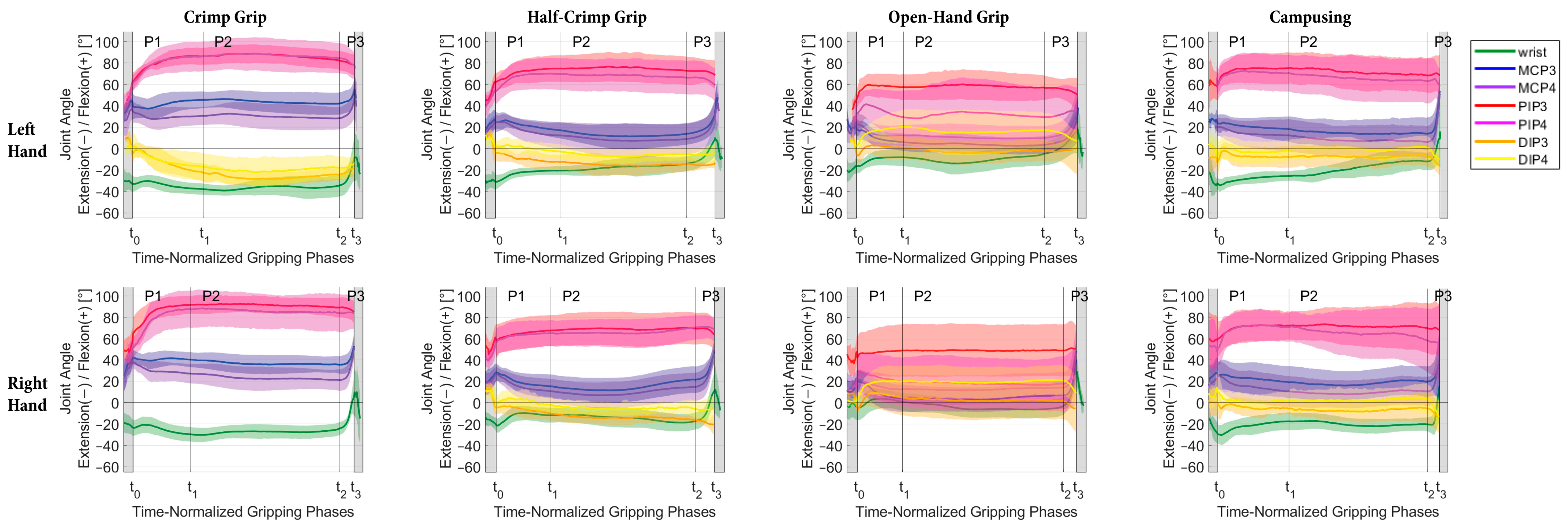
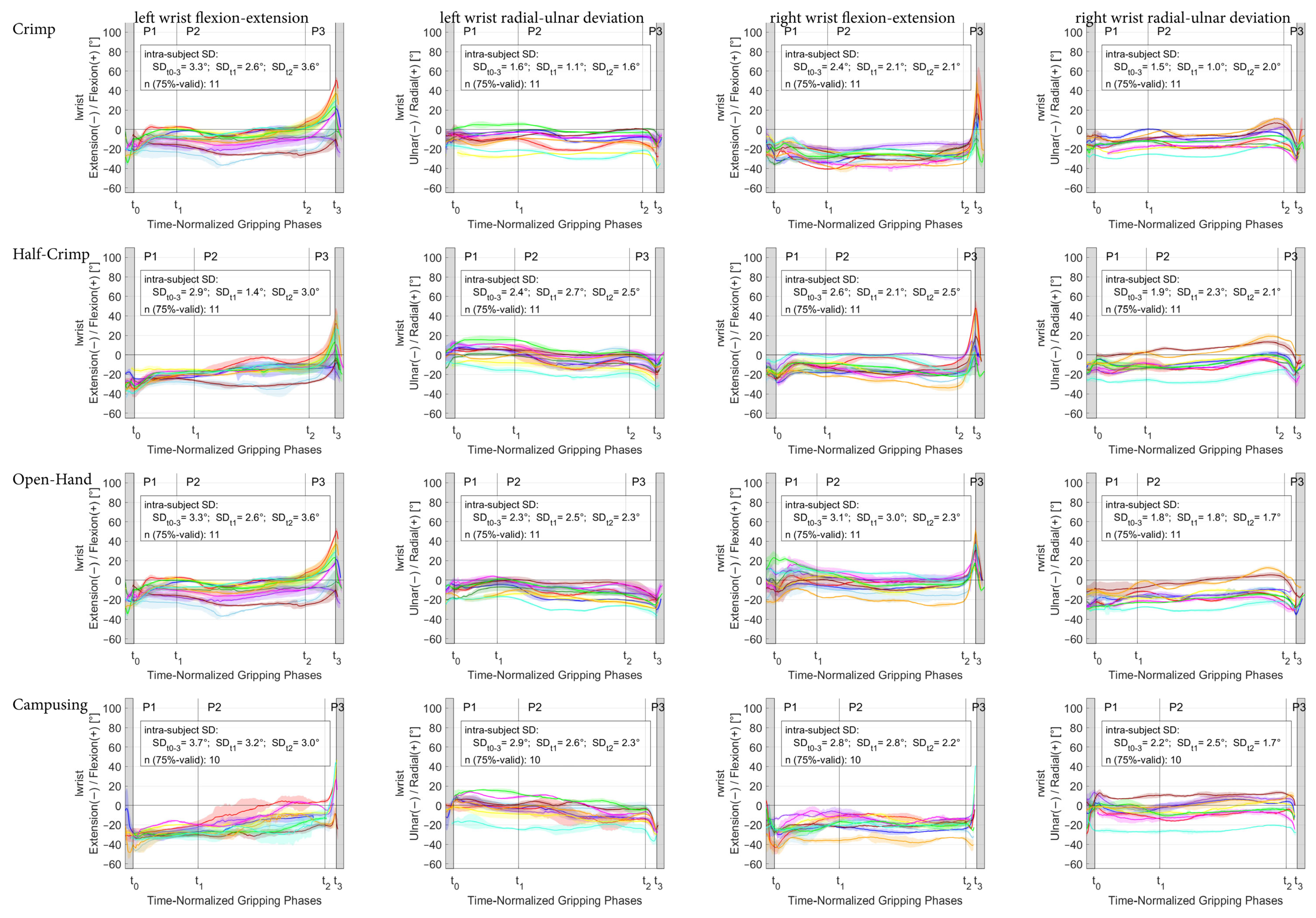
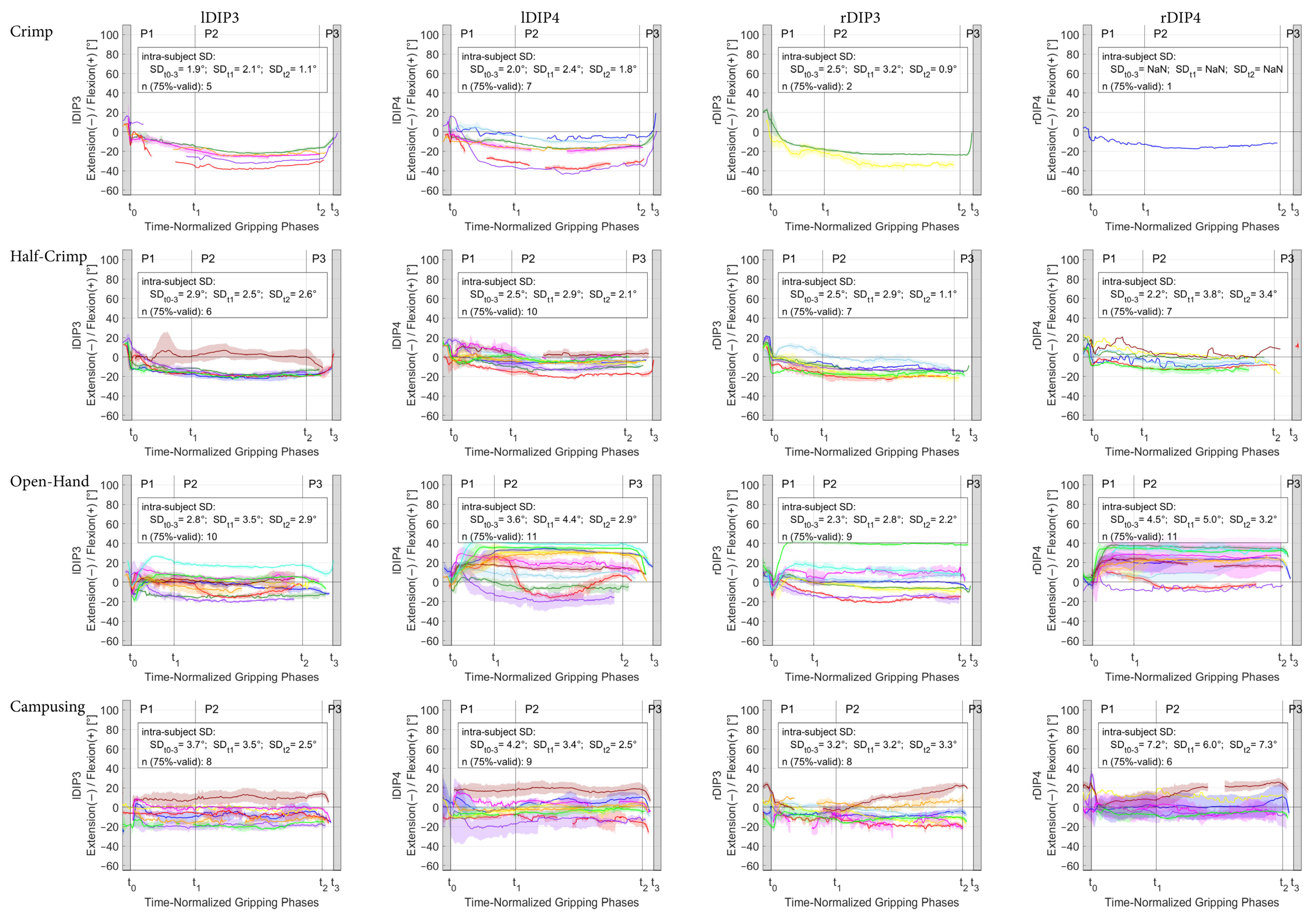
Figure 4.
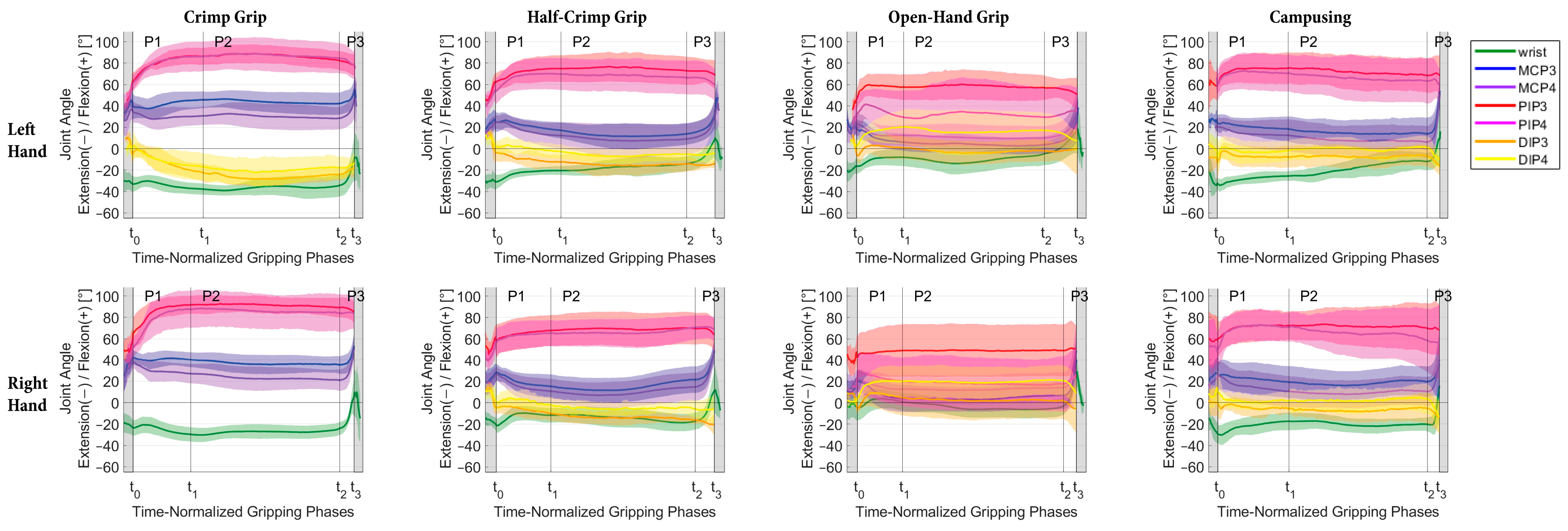
Mean and SD of flexion–extension angle progress over all participants during the time-normalized gripping phases (P1 = gripping, P2 = holding, P3 = releasing) for the joints of the left (top row) and right hand (bottom row) for the different grip positions (minimum n = 3 for mean and SD calculation).
Figure 4.
Mean and SD of flexion–extension angle progress over all participants during the time-normalized gripping phases (P1 = gripping, P2 = holding, P3 = releasing) for the joints of the left (top row) and right hand (bottom row) for the different grip positions (minimum n = 3 for mean and SD calculation).
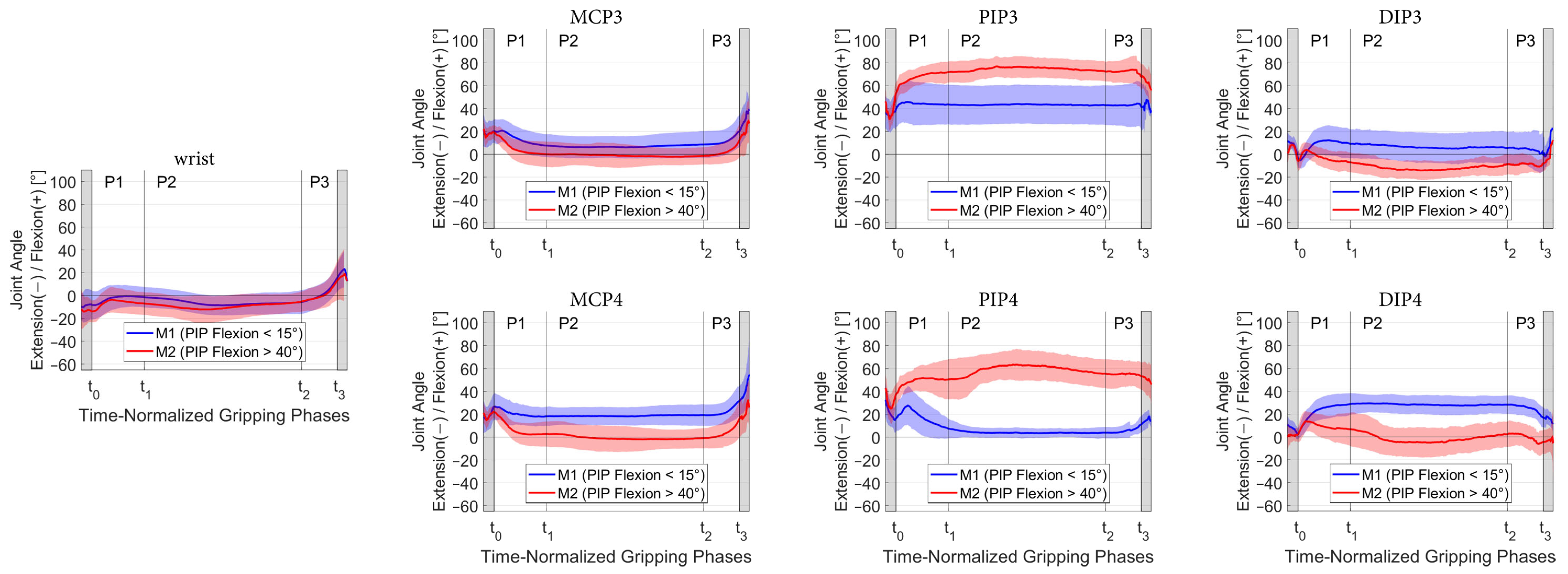
Figure 5.
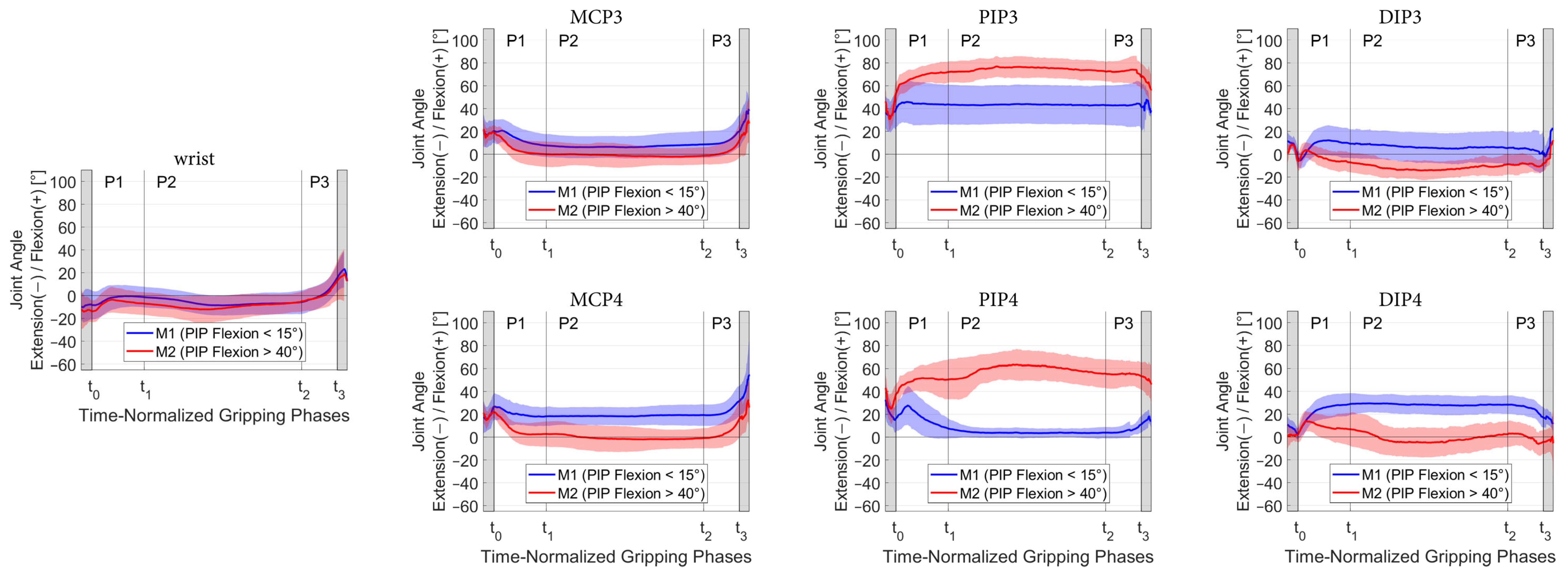
Mean and SD of the finger joint and wrist angles divided between the two methods during open-hand grip classified by PIP flexion angle, whereby trials with PIP flexion < 15° were assigned to group M1 (blue) and trials with PIP flexion > 40° to group M2 (red).
Figure 5.
Mean and SD of the finger joint and wrist angles divided between the two methods during open-hand grip classified by PIP flexion angle, whereby trials with PIP flexion < 15° were assigned to group M1 (blue) and trials with PIP flexion > 40° to group M2 (red).
Table 1.
Anthropometric data and redpoint (RP) climbing level of the participants according to IRCRA grading [
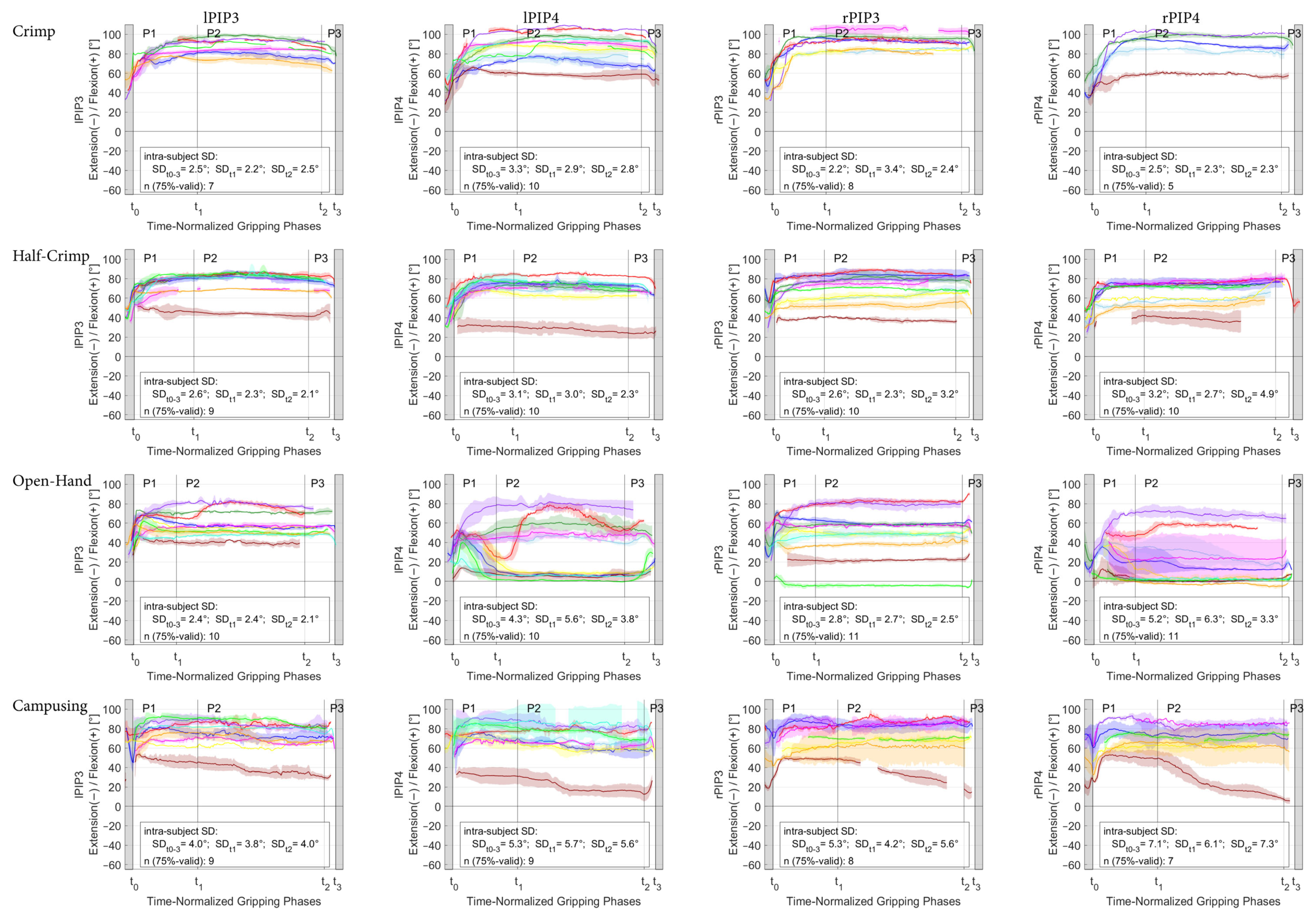
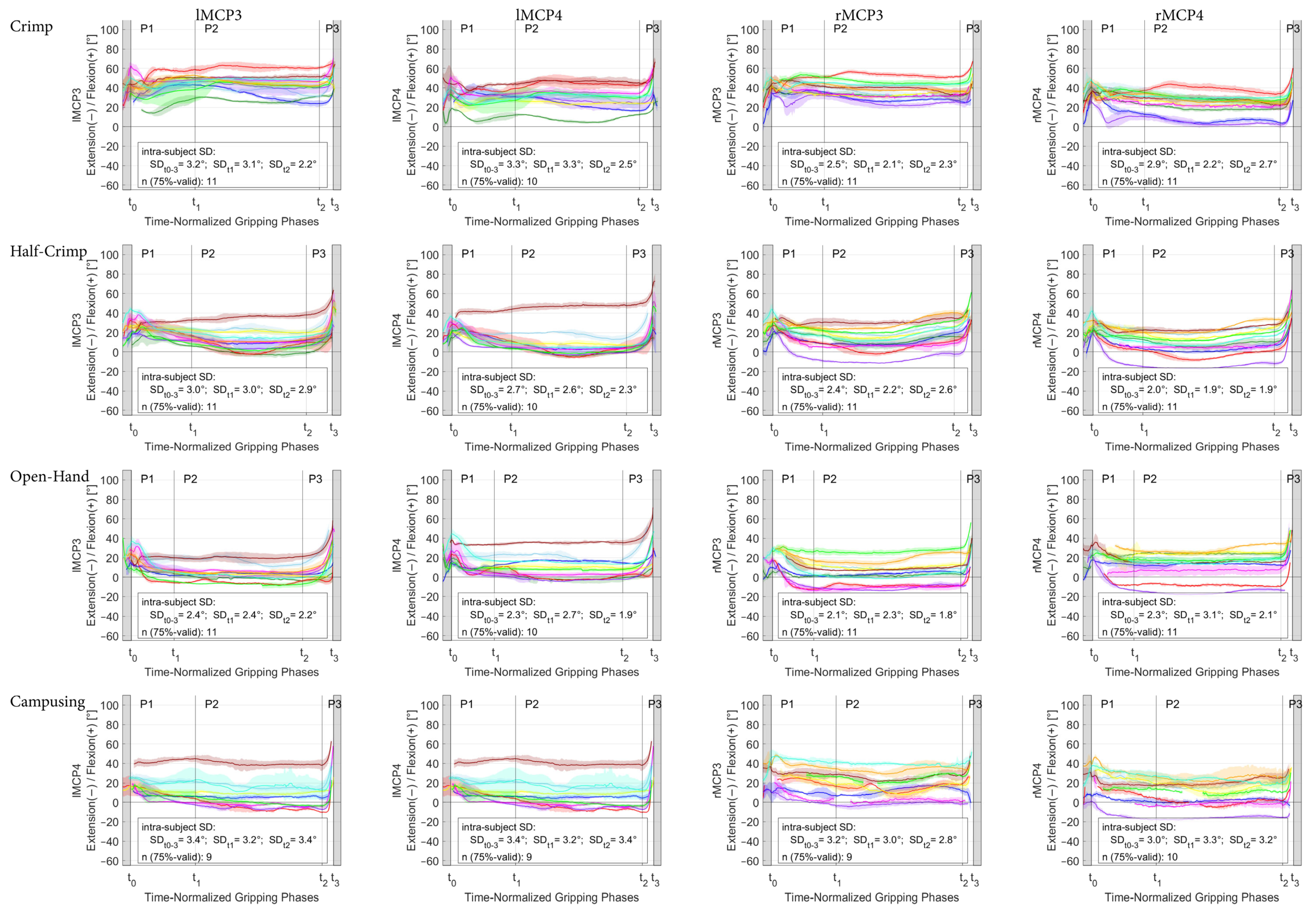
19]. Plot color refers to the color used for kinematic plots of individual climbers; hence, the climbers can be identified by this color in
Figure A4,
Figure A5 and
Figure A6. Participant “CLIM_0011” had to be excluded due to technical problems affecting kinetic data acquisition.
Table 1.
Anthropometric data and redpoint (RP) climbing level of the participants according to IRCRA grading [
19]. Plot color refers to the color used for kinematic plots of individual climbers; hence, the climbers can be identified by this color in
Figure A4,
Figure A5 and
Figure A6. Participant “CLIM_0011” had to be excluded due to technical problems affecting kinetic data acquisition.
| Participant | Sex | Age | Weight | Height | Climbing Experience | Training Hours Per Week | Max RP Bouldern IRCRA | Max RP Lead Climbing IRCRA | Plot
Color |
|---|
| | | [years] | [kg] | [cm] | [years] | [h] | [max] | [max] | |
|---|
| CLIM_0001 | F | 25 | 69 | 168 | 17 | 15 | 26.5 | 23 | |
| CLIM_0002 | M | 28 | 72 | 185 | 5 | 12 | 23.5 | n.a. | |
| CLIM_0003 | M | 31 | 67 | 174 | 10 | 6 | 26.5 | 23 | |
| CLIM_0004 | M | 32 | 66 | 174 | 12 | 12 | 28.5 | 29 | |
| CLIM_0005 | M | 38 | 75 | 174 | 15 | 6 | 23.5 | 21 | |
| CLIM_0006 | M | 45 | 65 | 179 | 27 | 6 | 27.5 | 27 | |
| CLIM_0007 | M | 51 | 70 | 180 | 30 | 3.5 | 26.5 | 27 | |
| CLIM_0008 | M | 30 | 74 | 185 | 15 | 3 | 24.5 | 25 | |
| CLIM_0009 | M | 20 | 70 | 176 | 10 | 14 | 26.5 | 23 | |
| CLIM_0010 | M | 23 | 69 | 179 | 6 | 10 | 25.5 | 18 | |
| CLIM_0012 | M | 36 | 73 | 187 | 20 | 8 | 27.5 | 25 | |
| Average | 1F 10M | 32.6 | 70.0 | 178.3 | 15.2 | 8.7 | 26.0 | 24.1 | |
| SD | | 9.1 | 3.0 | 5.5 | 7.6 | 4.0 | 1.6 | 3.0 | |
Table 2.
Flexion(+)–extension(-) ROM [°] (SD) during the grabbing (P1), holding (P2) and releasing (P3) phase averaged over all participants and conditions. Øn reflects the average number of participants with valid trials for ROM calculation; however, n might differ between conditions. It was specified with a footnote only if Øn < 11.
Table 2.
Flexion(+)–extension(-) ROM [°] (SD) during the grabbing (P1), holding (P2) and releasing (P3) phase averaged over all participants and conditions. Øn reflects the average number of participants with valid trials for ROM calculation; however, n might differ between conditions. It was specified with a footnote only if Øn < 11.
| | Wrist | MCP3 | MCP4 | PIP3 | PIP4 | DIP3 | DIP4 | Overall Mean |
|---|
| P1 | 14.2 (2.4) | 16.1 (2.3) | 16.8 (2.2) 1 | 20.5 (7.0) 1 | 25.3 (7.6) 1 | 19.2 (4.8) 1 | 18.1 (6.9) | 18.6 |
| P2 | 12.7 (3.1) | 9.2 (2.0) | 8.5 (1.2) 1 | 7.9 (2.6) 1 | 10.0 (2.8) 1 | 9.3 (3.0) 2 | 9.1 (2.4) 1 | 9.5 |
| P3 | 28.1 (2.5) | 22.3 (6.8) | 26.5 (6.0) 1 | 6.7 (1.0) 1 | 7.8 (3.3) 2 | 8.1 (3.9) 3 | 7.1 (4.5) 2 | 15.2 |
Table 3.
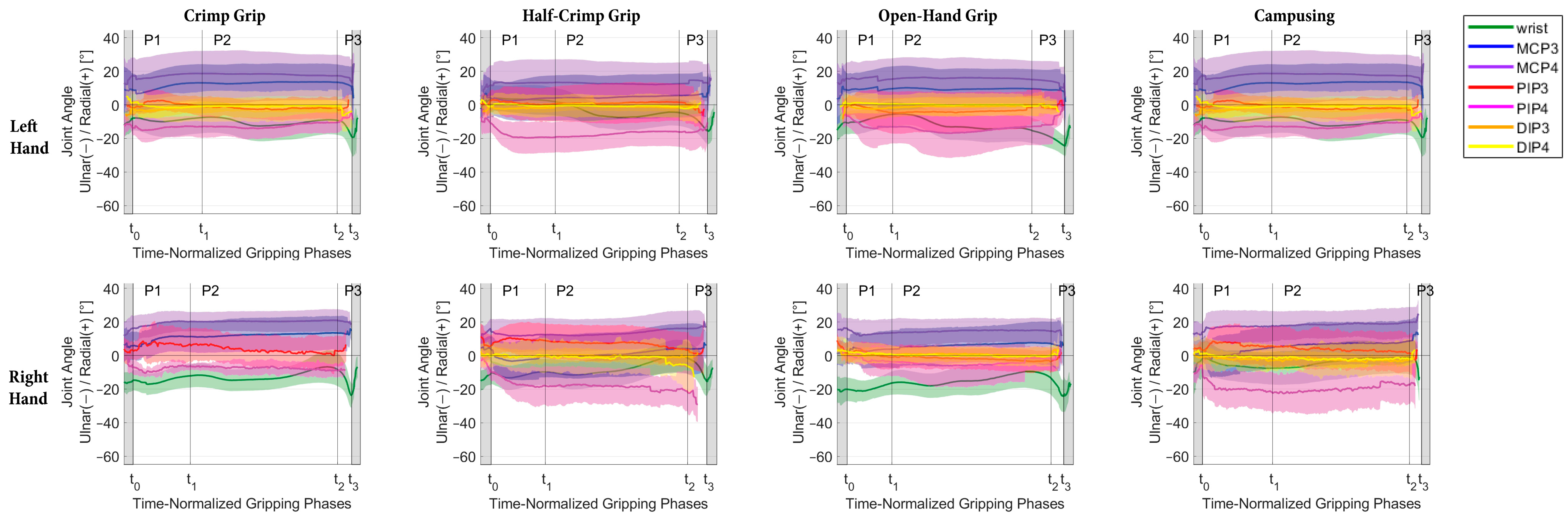
Radial(+)–ulnar(-) deviation ROM [°] (SD) during the grabbing (P1), holding (P2) and releasing (P3) phase averaged over all participants and conditions. Øn reflects the average number of participants with valid trials for ROM calculation; however, n might differ between conditions. It was specified with a footnote only if Øn < 11.
Table 3.
Radial(+)–ulnar(-) deviation ROM [°] (SD) during the grabbing (P1), holding (P2) and releasing (P3) phase averaged over all participants and conditions. Øn reflects the average number of participants with valid trials for ROM calculation; however, n might differ between conditions. It was specified with a footnote only if Øn < 11.
| | Wrist | MCP3 | MCP4 | PIP3 | PIP4 | DIP3 | DIP4 | Overall Mean |
|---|
| P1 | 8.5 (2.3) | 8.5 (1.6) | 7.9 (1.3) 1 | 10.4 (1.9) 1 | 12.2 (2.5) 1 | 6.0 (2.0) 1 | 5.5 (1.3) | 8.4 |
| P2 | 11.5 (1.9) | 5.4 (1.5) | 4.8 (1.3) 1 | 8.0 (2.3) 1 | 8.4 (2.0) 1 | 5.1 (2.6) 2 | 5.1 (1.7) 1 | 6.9 |
| P3 | 13.2 (2.4) | 4.9 (0.6) | 5.0 (1.3) 1 | 4.8 (0.6) 1 | 5.2 (1.3) 2 | 2.9 (1.2) 3 | 2.7 (1.1) 2 | 5.5 |
Table 4.
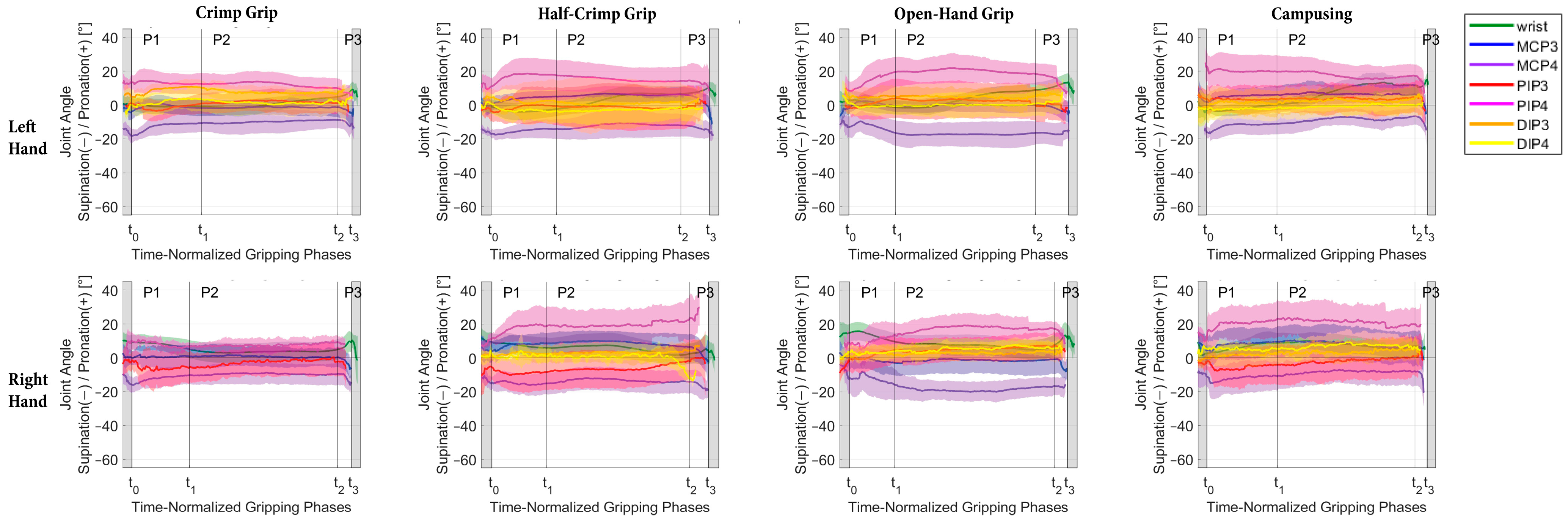
Pronation(+)–supination(-) ROM [°] (SD) during the grabbing (P1), holding (P2) and releasing (P3) phase averaged over all participants and conditions. Øn reflects the average number of participants with valid trials for ROM calculation; however, n might differ between conditions. It was specified with a footnote only if Øn < 11.
Table 4.
Pronation(+)–supination(-) ROM [°] (SD) during the grabbing (P1), holding (P2) and releasing (P3) phase averaged over all participants and conditions. Øn reflects the average number of participants with valid trials for ROM calculation; however, n might differ between conditions. It was specified with a footnote only if Øn < 11.
| | Wrist | MCP3 | MCP4 | PIP3 | PIP4 | DIP3 | DIP4 | Overall Mean |
|---|
| P1 | 7.2 (1.9) | 10.1 (2.1) | 12.8 (2.9) 1 | 11.5 (1.9) 1 | 13.4 (2.8) 1 | 10.3 (2.3) 1 | 10.6 (1.9) | 10.8 |
| P2 | 10.0 (3.6) | 7.3 (2.5) | 8.5 (2.0) 1 | 9.1 (2.6) 1 | 9.5 (2.4) 1 | 9.0 (3.1) 2 | 8.9 (2.2) 1 | 8.9 |
| P3 | 6.8 (1.3) | 9.7 (1.9) | 8.2 (1.6) 1 | 5.8 (1.2) 1 | 6.7 (2.2) 2 | 5.1 (1.4) 3 | 4.6 (1.5) 2 | 6.7 |
Table 5.
Mean (SD) flexion(+)–extension(-) joint angles [°] during the holding phase (P2) averaged over all climbers. N refers to the number of participants with at least one available value for the corresponding joint parameter. Superscripted letters refer to statistically significant differences between the left and right hand (A) as well as between corresponding joints of the middle and ring finger within the same hand (a–e).
Table 5.
Mean (SD) flexion(+)–extension(-) joint angles [°] during the holding phase (P2) averaged over all climbers. N refers to the number of participants with at least one available value for the corresponding joint parameter. Superscripted letters refer to statistically significant differences between the left and right hand (A) as well as between corresponding joints of the middle and ring finger within the same hand (a–e).
| Grip Type | Side | Wrist | MCP3 | MCP4 | PIP3 | PIP4 | DIP3 | DIP4 |
|---|
| Crimp | left | −36.6 | (7.1) | n = 11 A | 43.9 | (9.1) | n = 11 a | 30.2 | (10.9) | n = 10 a | 84.6 | (9.9) | n = 9 | 87.4 | (14.8) | n = 10 | −23.7 | (7.3) | n = 9 | −16.7 | (10.8) | n = 11 |
| | right | −27.6 | (5.8) | n = 11 A | 36.8 | (8.3) | n = 11 b | 23.2 | (10.2) | n = 11 b | 89.0 | (12.0) | n = 11 | 85.6 | (14.4) | n = 7 | −28.3 | (9.8) | n = 6 | −11.2 | (16.4) | n = 4 |
| Half-crimp | left | −17.4 | (6.9) | n = 11 | 12.8 | (10.4) | n = 11 | 8.7 | (14.6) | n = 10 | 75.0 | (13.3) | n = 9 | 68.3 | (15.2) | n = 10 | −13.0 | (7.2) | n = 9 | −5.8 | (6.0) | n = 11 |
| | right | −14.4 | (7.7) | n = 11 | 14.9 | (11.5) | n = 11 | 9.9 | (12.2) | n = 11 | 69.6 | (14.6) | n = 10 | 66.2 | (13.1) | n = 10 | −10.6 | (7.9) | n = 10 | −7.3 | (9.8) | n = 10 |
| Open-hand | left | −10.2 | (9.2) | n = 11 | 4.0 | (8.2) | n = 11 | 10.5 | (11.6) | n = 10 | 58.6 | (13.2) | n = 10 | 31.7 | (29.0) | n = 10 | −2.5 | (10.4) | n = 10 d | 16.5 | (18.8) | n = 11 d |
| | right | −4.4 | (7.6) | n = 11 | 4.3 | (11.9) | n = 11 | 12.7 | (13.6) | n = 11 | 49.4 | (24.7) | n = 11 c | 17.9 | (24.0) | n = 11 c | 3.8 | (16.1) | n = 11 e | 19.4 | (14.9) | n = 11 e |
| Campusing | left | −18.0 | (7.8) | n = 10 | 14.8 | (13.1) | n = 10 | 8.2 | (14.5) | n = 9 | 72.5 | (15.6) | n = 9 | 66.2 | (19.9) | n = 9 | −7.9 | (9.0) | n = 9 | −0.6 | (9.2) | n = 10 |
| | right | −20.0 | (6.5) | n = 10 | 18.0 | (12.9) | n = 10 | 9.4 | (13.1) | n = 10 | 70.7 | (17.2) | n = 9 | 68.6 | (19.1) | n = 10 | −7.3 | (8.8) | n = 8 | 0.5 | (9.0) | n = 9 |
Table 6.
Minimum and maximum within-participant average of the flexion(+)–extension(-) joint angles of the ring and middle finger PIPs during the holding phase.
Table 6.
Minimum and maximum within-participant average of the flexion(+)–extension(-) joint angles of the ring and middle finger PIPs during the holding phase.
| Grip Type | | lPIP3 | lPIP4 | rPIP3 | rPIP4 |
|---|
| Crimp | Min | 67.4 | 58.3 | 61.9 | 58.8 |
| | Max | 96.4 | 106.2 | 105.3 | 101.4 |
| Half-crimp | Min | 43.5 | 27.9 | 41.2 | 38.2 |
| | Max | 85.7 | 84.2 | 86.9 | 78.2 |
| Open-hand | Min | 39.9 | 0.8 | −4.3 | −2.9 |
| | Max | 79.9 | 78.5 | 82.0 | 69.1 |
| Campusing | Min | 37.6 | 20.0 | 34.5 | 23.6 |
| | Max | 87.7 | 87.8 | 88.8 | 91.4 |



 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}