1. Introduction
There has been considerable attention and discourse in clinical medicine, especially regarding the repair of critical-sized bone defects. This is particularly pertinent to invasive implant biocompatibility and wound-healing outcomes post-surgery. Historical constraints in materials and processing techniques have traditionally led to the use of biocompatible medical-grade titanium alloys and straightforward porous structure designs when addressing extensive bone defects. However, the substantial rigidity disparity between titanium alloys and bone tissue and the non-degradable nature of these materials hampers the short-term regeneration of the surrounding bone [
1,
2]. This limitation results in stress concentration at the interface between implants and bone, inducing stress shielding effects. Consequently, the regenerative efficacy of bone tissue is compromised, posing significant risks such as implant migration and collapse during the recovery period [
3]. This study addresses this concern by incorporating a gradient porosity bone scaffold. By varying the porosity at different levels, we aim to eliminate stress concentration points while ensuring that the mechanical strength of other parts remains relatively unchanged.
Bone transplantation surgery involves surgically replacing existing bone tissue with substitute materials. This procedure can be categorized into autografts, allografts, and synthetic bone grafts based on the type of substitute employed. Autografts utilize bone fragments obtained from other parts of the patient’s body, while allografts involve using bone from donors of the same type (allogeneic bone). Synthetic bone grafts are crafted from various materials. Artificial bone replacement materials commonly include bioceramics, metal alloys, and composite materials [
4,
5]. Historically, traditional medical techniques predominantly relied on autografts and allografts. Despite exhibiting superior bone formation rates and regenerated bone volume during bone growth [
6], the search for suitable substitutes persists. Moreover, autograft and allograft bone transplants carry inherent risks of complications, such as rejection and infection [
7]. Allografts require the careful consideration of factors like potential virus infections from the transplant source, the presence of immune disorders, and the impact of human leukocyte antigen compatibility [
8,
9]. In recent years, artificial bone transplantation surgeries with a stable supply of replacement sites and sources have been employed for treatment, significantly reducing patient wait times for replacement sites.
In past structural design studies, researchers drew inspiration from the architecture of bone tissue by incorporating porous structures into materials. Through in vivo experiments, implants made of the same material with added porous structures demonstrated advantages such as increased tissue permeability, thereby promoting a faster bone tissue growth rate [
10,
11]. Hulbert and their research team conducted experiments using ceramic materials, testing discs with and without pores. Their observations indicated a more rapid healing process around the porous discs made of the same material, with tissue fibers better enveloping the porous structure [
12]. Naoya Taniguchi et al. proposed the fabrication of porous implants using titanium alloy material and observed favorable bone tissue growth in pores ranging from 300 to 600 μm in diameter [
13]. Furthermore, the titanium scaffold with a 50% porosity exhibited lower maximum von Mises stress [
14], while the scaffold with a 70% porosity demonstrated optimal cell proliferation and bone ingrowth capacity [
15].
Selecting substitute materials is crucial for the success of artificial bone transplantation procedures. Presently, the prevalent materials utilized in medical substitutes comprise bioceramics and metal alloys. Bioceramics, represented by hydroxyapatite (HAp), are esteemed for their robust biocompatibility, non-toxicity, and osteoconductive properties. HAp is notable for its ability to control degradation in the presence of biological entities [
16], contributing to its widespread utilization in artificial bone replacements. Its exceptional biocompatibility significantly accelerates the bone-healing process. However, findings from tensile testing conducted by Kutz et al. [
17] reported a yield strength of 0.043 GPa, limiting the application of HAp to low-load-bearing scenarios. Experimental studies by Arcos et al. [
18] revealed that a synergistic combination of HAp and metal in bone defect replacement notably enhances tissue growth efficiency. Furthermore, the results of studies by Shah et al. [
19] underscored the remarkable adaptability of titanium structures to natural bone tissue. Titanium alloys, depending on the composition of different metallic elements and their lattice arrangements at room temperature, can be classified into three main categories: (1) α (hexagonal close-packed) phase alloys, (2) β (body-centered cubic) phase alloys, and (3) α + β phase alloys [
20]. This study uses the third type of Ti64 ELI. It combines the high-temperature creep and oxidation resistance of α phase alloys with the high strength and flexibility of β phase alloys [
21]. Conforming to the international to ASTM F136 material specifications for use in medical implants, the main components of the Ti64 ELI material, expressed in weight percentage (wt.%), include approximately 88.9% titanium, 6.5% aluminum, and 4.5% vanadium. The low-modulus alloy of Ti has also been employed in scaffold research. Luo et al. investigated the mechanical properties, biocompatibility, and proteinomics of the low-modulus alloy Ti-Nb-Ta-Zr [
22]. Song et al. achieved low-modulus radial gradient gyroid porous Ta structures via laser powder bed fusion [
23].
In addition to excellent biocompatibility, some alloys possess the appropriate combination of properties for use in high-load-bearing applications in the body, an example being medical-grade titanium alloy (Ti64 ELI). It boasts superior tensile strength without structural limitations (elastic modulus = 80–130 GPa [
24]) and excellent corrosion resistance and wear resistance [
25]. A study by Zhang et al. [
26] highlighted the practical support provided by artificial bone replacements fabricated from Ti alloy during the healing process. Rigorous sterilization procedures significantly mitigate issues such as infections. However, subsequent studies found that the elastic modulus of the alloy is substantially higher than that of cortical bone (17 GPa) and bone (5 GPa) of the distal tibia in non-osteoporotic middle-aged men [
27,
28]. This discrepancy results in uneven force distribution post-implantation, leading to excessive stress concentration and the formation of a stress shielding effect. This phenomenon diminishes the regenerative efficacy of bone tissue and heightens the risk of implant slippage and collapse during the recovery process [
29].
Li et al. introduced an innovative topology optimization methodology that concurrently considers mechanical and fluidic properties in the design of porous scaffolds [
30]. Wang et al. investigated the effects of porosity, pore size, and radial pore size distribution on compressive mechanical properties, cellular responses, and bone regeneration outcomes [
31]. This study introduces an optimized scaffold design approach for addressing critical-sized tibial defects. This study employs Ansys-Workbench for simulating post-implantation stress distribution and utilizes selective laser melting (SLM) to streamline the production of various structures by manufacturing physical prototypes. Subsequently, automated testing verifies the scaffold’s mechanical performance to ensure robust support provision.
The chosen manufacturing material is medical-grade Ti64 ELI alloy, integrating a gradient porous structure and bone plate into the overall formation. To promote bone tissue growth, HAp was selected for the central part of the scaffold. Utilizing Ti alloy with a gradient porous structure minimizes interface stress concentration between the scaffold and bone defect during bone growth. This design facilitates optimal bone support while safeguarding the HAp material from excessive compression and potential fractures during the initial implantation process. The scaffold is securely affixed using interconnected bone plates, aiding surgeons in achieving swift positioning during surgery and installing the scaffold at bone-cutting sites. This mitigates the risk of post-operative migration and significantly reduces the likelihood of complications. Our team has conducted previous studies on bone defects [
32,
33].
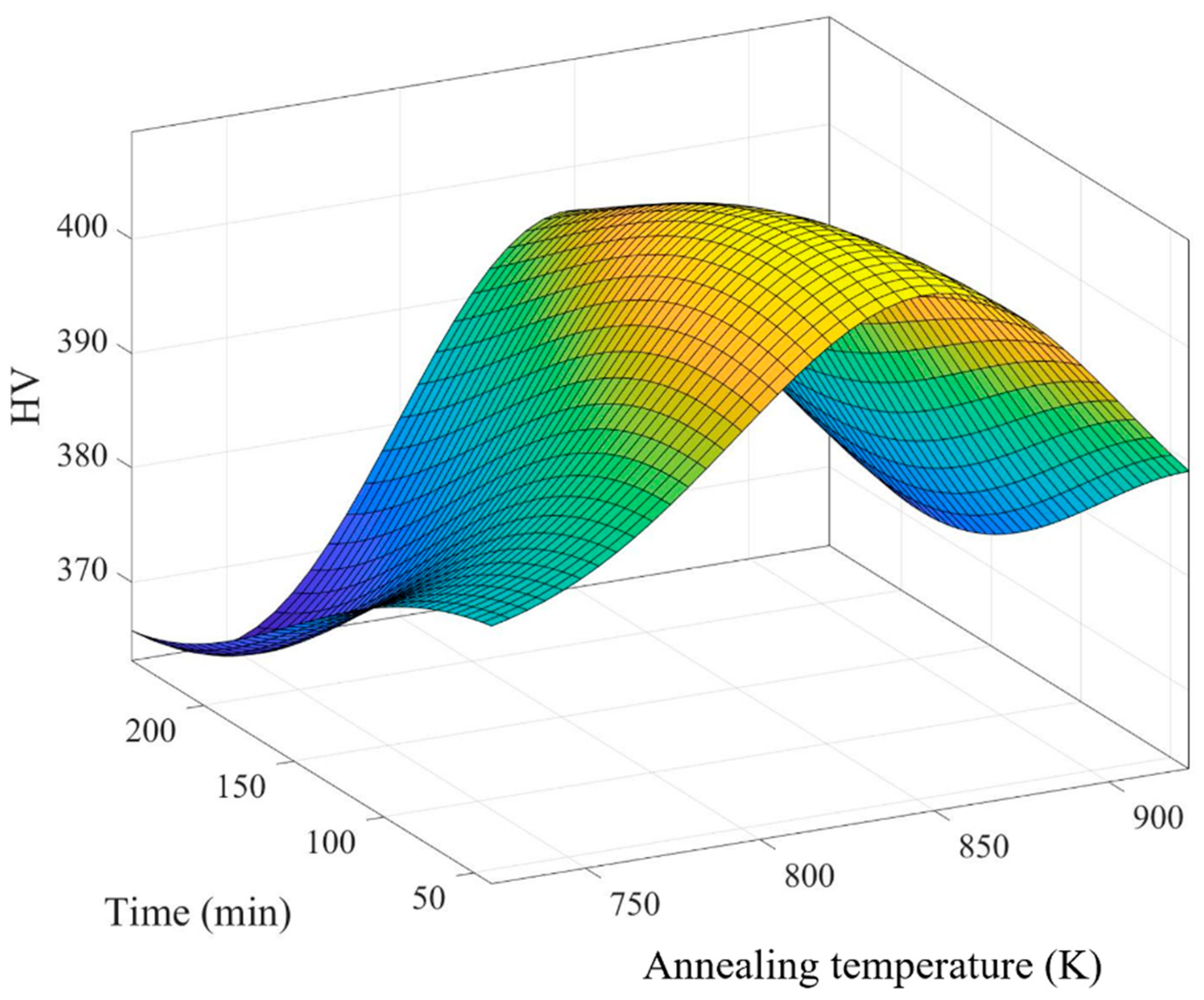
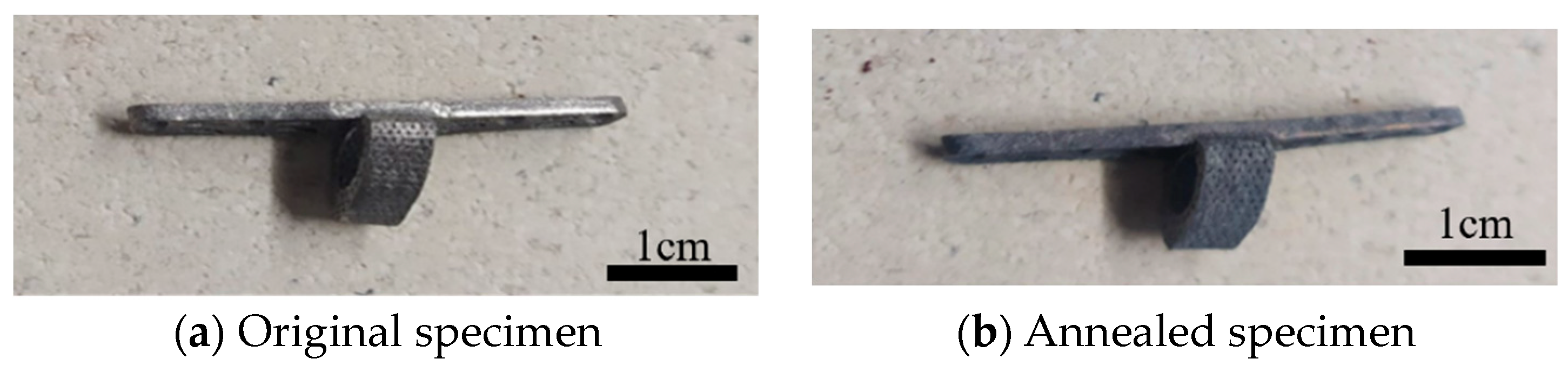
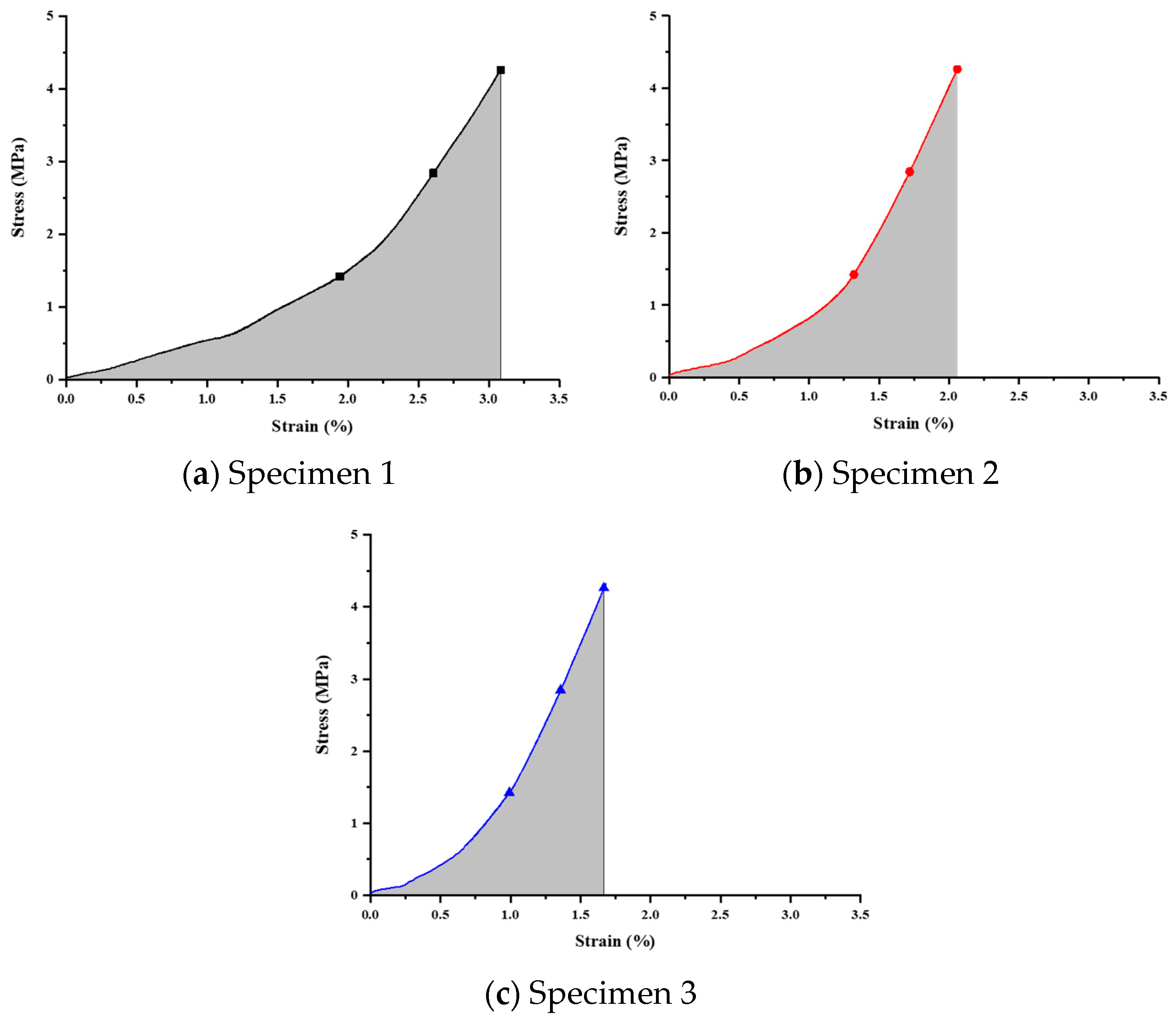
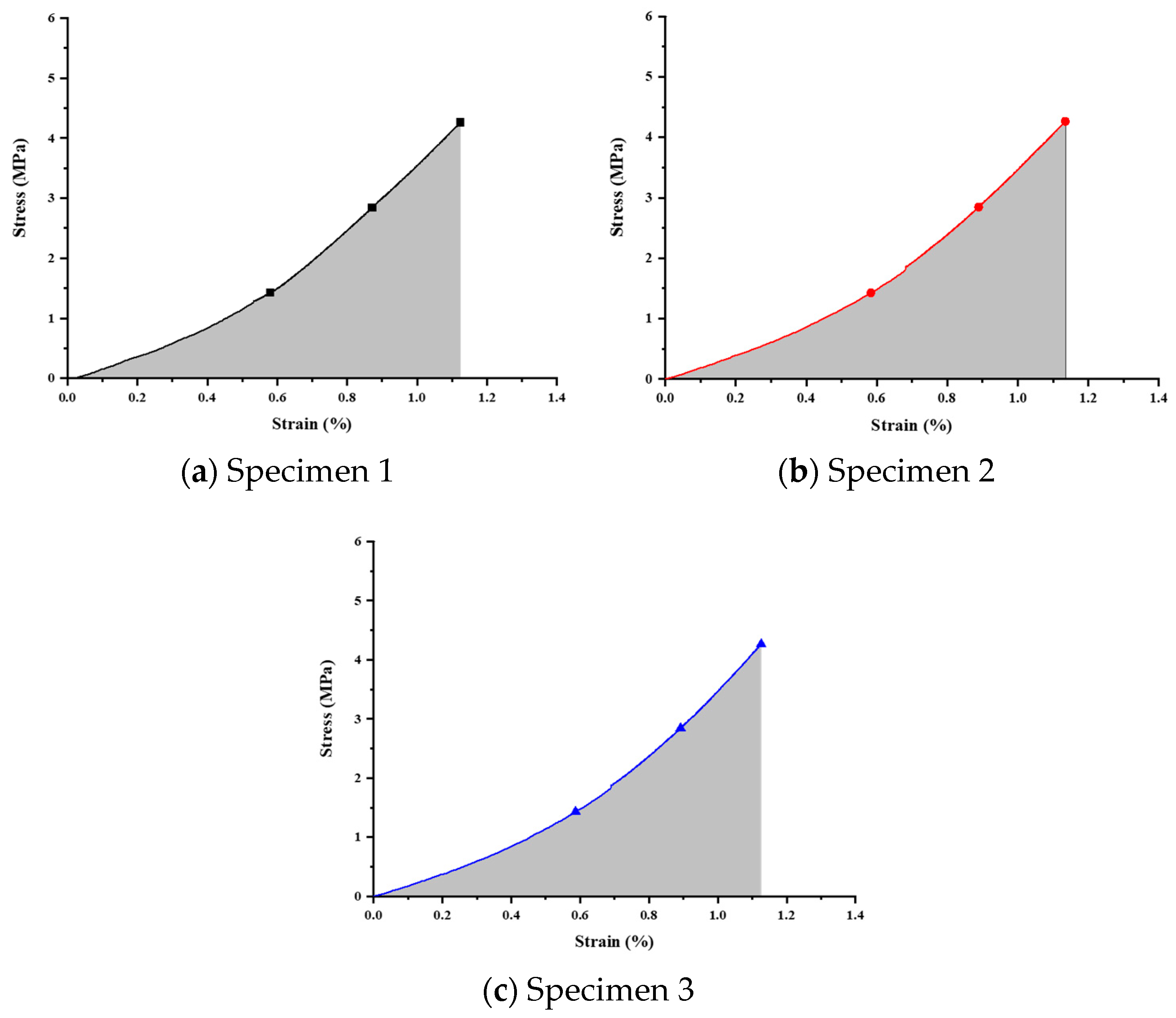
The current work comprises three main components. Firstly, finite element analysis (FEA) is employed to simulate the mechanical responses of scaffolds with different porosities and materials under high-activity conditions in rabbits. Secondly, a uniform design method (UDM) significantly reduces the experimental iterations required to explore the optimal annealing temperature and duration. The structures are manufactured using SLM to address various locations of bone defects, significantly reducing manufacturing time compared to traditional processes. Subsequently, annealing is performed at the optimal temperature and duration parameters to reduce stress concentration in the scaffold and achieve homogenization. Thirdly, nanoindentation tests are conducted on the prototype scaffold to obtain three mechanical properties (modulus, hardness, and strain energy) and investigate the scaffold’s structural strength and stress concentration.



 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}