
Bacterial Flora in Screw-Fixed Superstructures with Different Sealing Materials: A Comparative Clinical Trial



Abstract
1. Introduction
2. Materials and Methods
2.1. Participant Selection
2.1.1. Superstructure
2.1.2. Placement of the Final Superstructures and Sealing Materials (Figure 1)
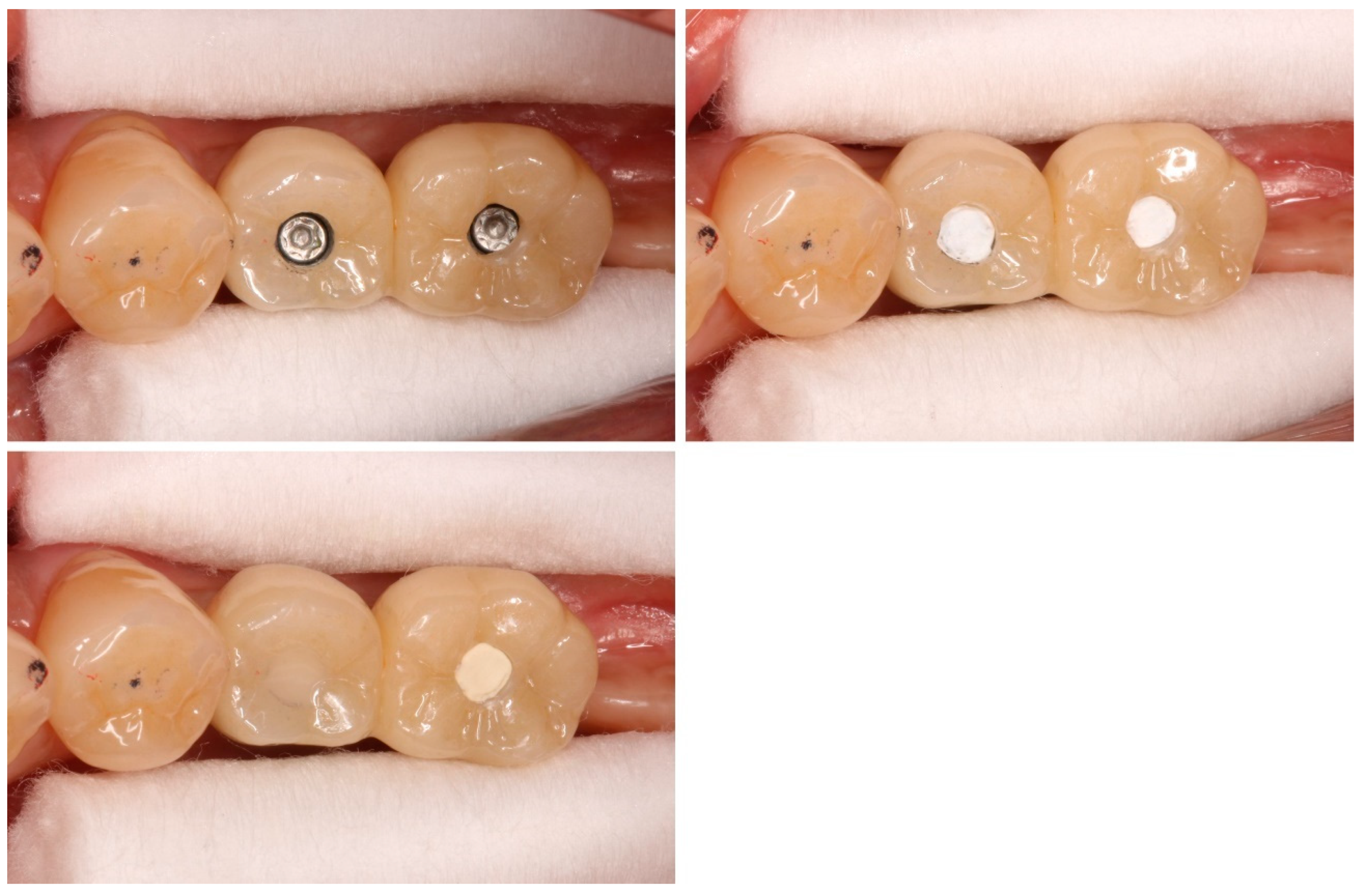
2.1.3. Zinc-containing Glass Ionomer (GI) Cement
2.2. Sampling
2.3. DNA Hybridization
2.4. Items for Investigation
2.5. Date Analysis
3. Results
3.1. Differences between Sealing Materials
3.1.1. Bacterial Count (Table 3)

{kind=link}
{kind=link}
{kind=link}
| Control | Test | |
|---|---|---|
| Total Bacteria | 13.0 × 106 | 4.3 × 106 ** |
| Porphyromonas gingivalis | 57,920 | 107,953 |
| Tannerella forsythia | 134,959 | 61,406 |
| Treponema denticola | 193,136 | 46,575 * |
| Red Complex | 386,014 | 215,934 * |
| Campylobacter rectus | 151,445 | 36,014 |
| Fusobacterium nucleatum subsp. polymorphum | 76,099 | 43,432 |
| Fusobacterium nucleatum subsp. animalis | 434,247 | 157,379 |
| Fusobacterium nucleatum subsp. nucleatum | 112,125 | 88,747 |
| Fusobacterium periodonticum | 114,794 | 48,227 |
| Fusobacterium nucleatum subsp. vincentii | 42,976 | 18,606 * |
| Prevotella nigrescens | 110,071 | 40,947 |
| Prevotella intermedia | 70,909 | 123,354 |
| Streptococcus constellatus | 25,113 | 37,062 |
| Campylobacter showae | 17,134 | 3481 |
| Campylobacter gracilis | 40,177 | 3371 * |
| Orange Complex | 1,195,088 | 600,620 * |
| Aggregatibacter actinomycetemcomitans | 462 | 66 |
| Campylobacter concisus | 28,056 | 3503 * |
| Capnocytophaga gingivalis | 5081 | 1624 |
| Capnocytophaga ochracea | 28,994 | 1410 |
| Capnocytophaga sputigena | 54,692 | 6540 |
| Eikenella corrodens | 3004 | 4051 |
| Green Complex | 120,290 | 17,194 * |
| Streptococcus intermedius | 6942 | 189 |
| Streptococcus gordonii | 104,047 | 17,282 ** |
| Streptococcus mitis | 22,251 | 23,349 |
| Streptococcus mitis bv 2 | 19,752 | 20,367 |
| Yellow Complex | 152,992 | 61,186 * |
| Actinomyces odontolyticus | 1707 | 1529 |
| Veillonella parvula | 110,860 | 46,849 * |
| Purple Complex | 112,567 | 48,377 ** |
| Actinomyces naeslundii II | 77,696 | 44,997 |
| Selenomonas noxia | 22,013 | 2144 |
3.1.2. Bacterial Ratio (Table 4)
| Control | Test | |
|---|---|---|
| Total Bacteria | ||
| Porphyromonas gingivalis | 0.24 | 0.23 |
| Tannerella forsythia | 0.50 | 0.00 |
| Treponema denticola | 0.64 | 0.00 |
| Red Complex | 4.36 | 0.23 |
| Campylobacter rectus | 0.48 | 0.00 |
| Fusobacterium nucleatum subsp. polymorphum | 0.38 | 0.19 |
| Fusobacterium nucleatum subsp. animalis | 1.46 | 0.00 |
| Fusobacterium nucleatum subsp. nucleatum | 0.35 | 0.00 |
| Fusobacterium periodonticum | 0.49 | 0.27 |
| Fusobacterium nucleatum subsp. vincentii | 0.18 | 0.01 |
| Prevotella nigrescens | 0.40 | 0.02 |
| Prevotella intermedia | 0.18 | 0.00 |
| Streptococcus constellatus | 0.11 | 0.00 |
| Campylobacter showae | 0.08 | 0.00 |
| Campylobacter gracilis | 0.24 | 0.05 * |
| Orange Complex | 4.36 | 0.54 |
| Aggregatibacter actinomycetemcomitans | 0.00 | 0.00 |
| Campylobacter concisus | 0.24 | 0.00 * |
| Capnocytophaga gingivalis | 0.03 | 0.01 |
| Capnocytophaga ochracea | 0.18 | 0.00 |
| Capnocytophaga sputigena | 0.25 | 0.43 |
| Eikenella corrodens | 0.02 | 0.00 |
| Green Complex | 0.72 | 0.44 * |
| Streptococcus intermedius | 0.05 | 1.51 |
| Streptococcus gordonii | 1.01 | 0.55 |
| Streptococcus mitis | 0.20 | 0.00 |
| Streptococcus mitis bv 2 | 0.19 | 1.34 * |
| Yellow Complex | 1.45 | 3.40 |
| Actinomyces odontolyticus | 0.02 | 2.91 * |
| Veillonella parvula | 2.32 | 0.16 |
| Purple Complex | 2.34 | 3.07 |
| Actinomyces naeslundii II | 0.93 | 2.31 |
| Selenomonas noxia | 0.09 | 1.00 |
3.1.3. Implant Positivity Rate (Table 5)
| Control | Test | |
|---|---|---|
| Total Bacteria | ||
| Porphyromonas gingivalis | 26.3% | 15.8% |
| Tannerella forsythia | 78.9% | 78.9% |
| Treponema denticola | 84.2% | 63.2% |
| Red Complex | 63.2% | 52.6% |
| Campylobacter rectus | 26.3% | 26.3% |
| Fusobacterium nucleatum subsp. polymorphum | 42.1% | 15.8% |
| Fusobacterium nucleatum subsp. animalis | 47.4% | 15.8% * |
| Fusobacterium nucleatum subsp. nucleatum | 57.9% | 31.6% |
| Fusobacterium periodonticum | 47.4% | 15.8% * |
| Fusobacterium nucleatum subsp. vincentii | 52.6% | 15.8% * |
| Prevotella nigrescens | 31.6% | 21.1% |
| Prevotella intermedia | 26.3% | 15.8% |
| Streptococcus constellatus | 42.1% | 36.8% |
| Campylobacter showae | 31.6% | 10.5% |
| Campylobacter gracilis | 42.1% | 10.5% * |
| Orange Complex | 40.7% | 19.6% ** |
| Aggregatibacter actinomycetemcomitans | 10.5% | 5.3% |
| Campylobacter concisus | 57.9% | 21.1% * |
| Capnocytophaga gingivalis | 36.8% | 15.8% |
| Capnocytophaga ochracea | 31.6% | 10.5% |
| Capnocytophaga sputigena | 36.8% | 21.1% |
| Eikenella corrodens | 21.1% | 10.5% |
| Green Complex | 32.5% | 14.0% ** |
| Streptococcus intermedius | 42.1% | 15.8% |
| Streptococcus gordonii | 89.5% | 78.9% |
| Streptococcus mitis | 89.5% | 84.2% |
| Streptococcus mitis bv 2 | 94.7% | 89.5% |
| Yellow Complex | 78.9% | 67.1% * |
| Actinomyces odontolyticus | 89.5% | 89.5% |
| Veillonella parvula | 73.7% | 47.4% * |
| Purple Complex | 81.6% | 68.4% |
| Actinomyces naeslundii II | 89.5% | 89.5% |
| Selenomonas noxia | 36.8% | 15.8% |
3.2. Differences between Patients
3.2.1. Bacterial Count (Table 6)
| Bacterial Count | Bacterial Ratio | |
|---|---|---|
| Total Bacteria | 0.000091 ** | |
| Porphyromonas gingivalis | 0.68 | 0.344 |
| Tannerella forsythia | 0.068 | 0.159 |
| Treponema denticola | 0.003 ** | 0.398 |
| Red Complex | 0.029 * | 0.621 |
| Campylobacter rectus | 0.368 | 0.368 |
| Fusobacterium nucleatum subsp. polymorphum | 0.0058 ** | 0.288 |
| Fusobacterium nucleatum subsp. animalis | 0.011 * | 0.043 * |
| Fusobacterium nucleatum subsp. nucleatum | 0.025 * | 0.628 |
| Fusobacterium periodonticum | 0.0038 ** | 0.26 |
| Fusobacterium nucleatum subsp. vincentii | 0.0026 ** | 0.194 |
| Prevotella nigrescens | 0.046 * | 0.252 |
| Prevotella intermedia | 0.681 | 0.344 |
| Streptococcus constellatus | 0.297 | 0.054 |
| Campylobacter showae | 0.014 * | 0.014 * |
| Campylobacter gracilis | 0.0058 ** | 0.0086 ** |
| Orange Complex | 0.025 * | 0.943 |
| Aggregatibacter actinomycetemcomitans | 0.328 | 0.328 |
| Campylobacter concisus | 0.017 * | 0.123 |
| Capnocytophaga gingivalis | 0.104 | 0.338 |
| Capnocytophaga ochracea | 0.015 * | 0.014 * |
| Capnocytophaga sputigena | 0.034 | 0.2 |
| Eikenella corrodens | 0.68 | 0.344 |
| Green Complex | 0.018 * | 0.127 |
| Streptococcus intermedius | 0.0086 ** | 0.288 |
| Streptococcus gordonii | 0.0005 ** | 0.128 |
| Streptococcus mitis | 0.293 | 0.0049 ** |
| Streptococcus mitis bv 2 | 0.357 | 0.0033 ** |
| Yellow Complex | 0.0069 ** | 0.188 |
| Actinomyces odontolyticus | 0.043 * | 0.0078 ** |
| Veillonella parvula | 0.00061 ** | 0.018 * |
| Purple Complex | 0.000091 ** | 0.063 |
| Actinomyces naeslundii II | 0.043 ** | 0.099 |
| Selenomonas noxia | 0.0086 ** | 0.018 * |
3.2.2. Bacterial Ratio (Table 6)
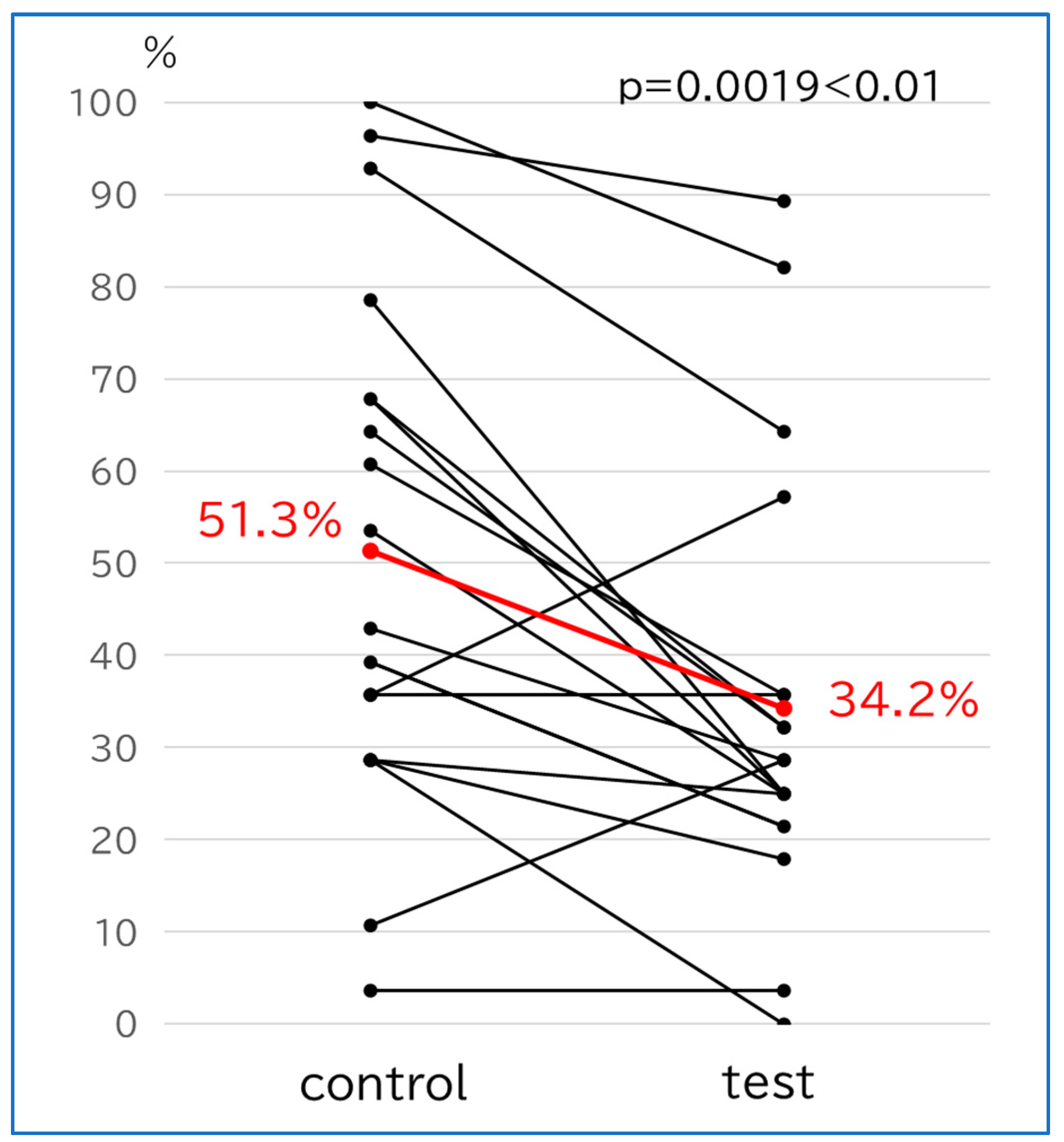
3.2.3. Implant Positivity Rate (Figure 3)
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A Systematic Review of the Survival and Complication Rates of Implant-Supported Fixed Dental Prostheses (FDPs) after a Mean Observation Period of at Least 5 Years. Clin. Oral Implants Res. 2012, 23 (Suppl. 6), 22–38. [Google Scholar] [CrossRef] [PubMed]
- Goiato, M.C.; dos Santos, D.M.; Santiago, J.F.; Moreno, A.; Pellizzer, E.P. Longevity of Dental Implants in Type IV Bone: A Systematic Review. Int. J. Oral Maxillofac. Surg. 2014, 43, 1108–1116. [Google Scholar] [CrossRef]
- Jimbo, R.; Albrektsson, T. Long-Term Clinical Success of Minimally and Moderately Rough Oral Implants: A Review of 71 Studies with 5 Years or More of Follow-Up. Implant. Dent. 2015, 24, 62–69. [Google Scholar] [CrossRef]
- Kofron, M.D.; Carstens, M.; Fu, C.; Wen, H.B. In Vitro Assessment of Connection Strength and Stability of Internal Implant-Abutment Connections. Clin. Biomech. 2019, 65, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Rismanchian, M.; Hatami, M.; Badrian, H.; Khalighinejad, N.; Goroohi, H. Evaluation of Microgap Size and Microbial Leakage in the Connection Area of 4 Abutments with Straumann (ITI) Implant. J. Oral Implantol. 2012, 38, 677–685. [Google Scholar] [CrossRef]
- Apatzidou, D.; Lappin, D.F.; Hamilton, G.; Papadopoulos, C.A.; Konstantinidis, A.; Riggio, M.P. Microbiome of Peri-Implantitis Affected and Healthy Dental Sites in Patients with a History of Chronic Periodontitis. Arch. Oral Biol. 2017, 83, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Martin, I.; Doolittle-Hall, J.; Teles, R.P.; Patel, M.; Belibasakis, G.N.; Hämmerle, C.H.F.; Jung, R.E.; Teles, F.R.F. Exploring the Microbiome of Healthy and Diseased Peri-Implant Sites Using Illumina Sequencing. J. Clin. Periodontol. 2017, 44, 1274–1284. [Google Scholar] [CrossRef]
- Sahrmann, P.; Gilli, F.; Wiedemeier, D.B.; Attin, T.; Schmidlin, P.R.; Karygianni, L. The Microbiome of Peri-Implantitis: A Systematic Review and Meta-Analysis. Microorganisms 2020, 8, 661. [Google Scholar] [CrossRef]
- Belibasakis, G.N.; Manoil, D. Microbial Community-Driven Etiopathogenesis of Peri-Implantitis. J. Dent. Res. 2021, 100, 21–28. [Google Scholar] [CrossRef]
- Quirynen, M.; van Steenberghe, D. Bacterial colonization of the internal part of two-stage implants. An in vivo study. Clin. Oral Implants Res. 1993, 4, 158–161. [Google Scholar] [CrossRef]
- Sasada, Y.; Cochran, D.L. Implant-Abutment Connections: A Review of Biologic Consequences and Peri-implantitis Implications. Int. J. Oral Maxillofac. Implants 2017, 32, 1296–1307. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, C.D.; Pita, M.S.; Santos Ede, S.; Monesi, N.; Pedrazzi, V.; Albuquerque Junior, R.F.; Ribeiro, R.F. Microbiome of titanium and zirconia dental implants abutments. Dent. Mater. 2016, 32, 93–101. [Google Scholar] [CrossRef] [PubMed]
- El Haddad, E.; Giannì, A.B.; Mancini, G.E.; Cura, F.; Carinci, F. Implant-abutment leaking of replace conical connection nobel biocare® implant system. An in vitro study of the microbiological penetration from external environment to implant-abutment space. Oral Implantol. 2016, 9, 76–82. [Google Scholar] [CrossRef]
- Jervøe-Storm, P.M.; Jepsen, S.; Jöhren, P.; Mericske-Stern, R.; Enkling, N. Internal Bacterial Colonization of Implants: Association with Peri-Implant Bone Loss. Clin. Oral Implants Res. 2015, 26, 957–963. [Google Scholar] [CrossRef]
- do Nascimento, C.; Pita, M.S.; Calefi, P.L.; de Oliveira Silva, T.S.; Dos Santos, J.B.; Pedrazzi, V. Different Sealing Materials Preventing the Microbial Leakage into the Screw-Retained Implant Restorations: An In Vitro Analysis by DNA Checkerboard Hybridization. Clin. Oral Implants Res. 2017, 28, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Park, S.D.; Lee, Y.; Kim, Y.L.; Yu, S.H.; Bae, J.M.; Cho, H.W. Microleakage of Different Sealing Materials in Access Holes of Internal Connection Implant. Systems. J. Prosthet. Dent. 2012, 108, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, L.F.; Watt, R.M.; Mattheos, N.; Si, M.S.; Lai, H.C.; Lang, N.P. Periodontal and Peri-Implant Microbiota in Patients with Healthy and Inflamed Periodontal and Peri-Implant Tissues. Clin. Oral Implants Res. 2016, 27, 13–21. [Google Scholar] [CrossRef]
- He, G.; Pearce, E.I.; Sissons, C.H. Inhibitory Effect of ZnCl2 on Glycolysis in Human Oral Microbes. Arch. Oral Biol. 2002, 2, 117–129. [Google Scholar] [CrossRef]
- Mohammed, N.R.; Mneimne, M.; Hill, R.G.; Al-Jawad, M.; Lynch, R.J.; Anderson, P. Physical Chemical Effects of Zinc on In Vitro Enamel Demineralization. J. Dent. 2014, 42, 1096–1104. [Google Scholar] [CrossRef]
- Toledano, M.; Yamauti, M.; Osorio, E.; Osorio, R. Zinc-Inhibited MMP Mediated Collagen Degradation After Different Dentine Demineralization Procedures. Caries Res. 2012, 46, 201–207. [Google Scholar] [CrossRef]
- Liu, Y.; Kohno, T.; Tsuboi, R.; Thongthai, P.; Fan, D.; Sakai, H.; Kitagawa, H.; Imazato, S. Antibacterial Effects and Physical Properties of a Glass Ionomer Cement Containing BioUnion Filler with Acidity-Induced Ability to Release Zinc Ion. Dent. Mater. J. 2021, 40, 1418–1427. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Takenaka, S.; Ohsumi, T.; Ida, T.; Ohshima, H.; Terao, Y.; Naksagoon, T.; Maeda, T.; Noiri, Y. Effect of a Novel Glass Ionomer Cement Containing Fluoro-Zinc-Silicate Fillers on Biofilm Formation and Dentin Ion Incorporation. Clin. Oral Investig. 2020, 24, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Yazawa, A.; Kamitani, S.; Togawa, N. Method for Absolute Quantification of Microbial Communities by Using Both Microarrays and Competitive PCR. J. Microbiol. Methods 2019, 165, 105718. [Google Scholar] [CrossRef] [PubMed]
- Moritani, K.; Takeshita, T.; Shibata, Y.; Ninomiya, T.; Kiyohara, Y.; Yamashita, Y. Acetaldehyde Production by Major Oral Microbes. Oral Dis. 2015, 21, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Cortelli, S.C.; Cortelli, J.R.; Romeiro, R.L.; Costa, F.O.; Aquino, D.R.; Orzechowski, P.R.; Araújo, V.C.; Duarte, P.M. Frequency of Periodontal Pathogens in Equivalent Peri-Implant and Periodontal Clinical Statuses. Arch. Oral Biol. 2013, 58, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Peñarrocha-Oltra, D.; Covani, U.; Rossetti, P.H. Microbiologic and Clinical Findings of Implants in Healthy Condition and with Peri-Implantitis. Int. J. Oral Maxillofac. Implants 2015, 30, 834–842. [Google Scholar] [CrossRef]
- Pérez-Chaparro, P.J.; Duarte, P.M.; Shibli, J.A.; Montenegro, S.; Lacerda Heluy, S.; Figueiredo, L.C.; Faveri, M.; Feres, M. The Current Weight of Evidence of the Microbiologic Profile Associated with Peri-Implantitis: A Systematic Review. J. Periodontol. 2016, 87, 1295–1304. [Google Scholar] [CrossRef]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and Microbial Biofilm Profiles of Peri-Implantitis: A Systematic Review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef]
- Zhou, H.; Ye, S.; Lyu, X.; Feng, H.; Liu, M.; Wen, C. Evaluation of Sealing Efficacy and Removal Convenience of Sealing Materials for Implant Abutment Screw Access Holes. BMC Oral Health 2022, 22, 362. [Google Scholar] [CrossRef]
- Moráguez, O.D.; Belser, U.C. The Use of Polytetrafluoroethylene Tape for the Management of Screw Access Channels in Implant-Supported Prostheses. J. Prosthet. Dent. 2010, 103, 189–191. [Google Scholar] [CrossRef]
- Cakan, U.; Gultekin, P.; Guncu, M.B.; Canay, S. Effect of Screw Access Channel Filling Materials on Uniaxial Retentive Force of Cement-Retained Implant Restorations. Aust. Dent. J. 2014, 59, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, A.G.; Fonseca, F.T.; Zago, C.D.; Brito Junior, R.B.; França, F.M. Efficacy of Gutta-Percha and Polytetrafluoroethylene Tape to Microbiologically Seal the Screw Access Channel of Different Prosthetic Implant Abutments. Clin. Implant. Dent. Relat. Res. 2016, 18, 778–787. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, M.; Albaqiah, H. Antimicrobial Efficacy of Materials Used for Sealing the Implant Abutment Screw Hole: An In Vitro Evaluation. Implant. Dent. 2017, 26, 911–914. [Google Scholar] [CrossRef] [PubMed]

| Inclusion Criteria |
| Implants placed and superstructures was inserted at this hospital |
| Age: between 20 and 80 years |
| Written consent to participate in the research was obtained from the individual. |
| Two implants are adjacent to each other. |
| Connected superstructure inserted. |
| Exclusion criteria |
| Fully edentulous patients |
| Bone grafting was performed at the time of implant placement |
| Periodontal disease or diabetes mellitus |
| Undergoing or previously undergoing radiation therapy to the head and neck |
| Bruxism |
| Pregnancy, possible pregnancy, breastfeeding, or considering pregnancy |
| Patients requiring prophylactic antibiotics or who were taking steroid medications |
| Marginal bone loss at the time of superstructure attachment |
| Prosthetic devices without intervening abutments were inserted |
| Gender | |
| Male | 13 |
| Female | 6 |
| Age (y) | |
| 40–49 | 2 |
| 50–59 | 3 |
| 60–69 | 7 |
| 70–79 | 7 |
| Mean ± SD | 65.7 ± 10.87 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, K.; Munakata, M.; Ishii, K.; Uesugi, T. Bacterial Flora in Screw-Fixed Superstructures with Different Sealing Materials: A Comparative Clinical Trial. Bioengineering 2024, 11, 195. https://doi.org/10.3390/bioengineering11020195
Yamaguchi K, Munakata M, Ishii K, Uesugi T. Bacterial Flora in Screw-Fixed Superstructures with Different Sealing Materials: A Comparative Clinical Trial. Bioengineering. 2024; 11(2):195. https://doi.org/10.3390/bioengineering11020195
Chicago/Turabian StyleYamaguchi, Kikue, Motohiro Munakata, Kota Ishii, and Takashi Uesugi. 2024. "Bacterial Flora in Screw-Fixed Superstructures with Different Sealing Materials: A Comparative Clinical Trial" Bioengineering 11, no. 2: 195. https://doi.org/10.3390/bioengineering11020195
APA StyleYamaguchi, K., Munakata, M., Ishii, K., & Uesugi, T. (2024). Bacterial Flora in Screw-Fixed Superstructures with Different Sealing Materials: A Comparative Clinical Trial. Bioengineering, 11(2), 195. https://doi.org/10.3390/bioengineering11020195