
Biomaterials for Alveolar Ridge Preservation as a Preoperative Procedure for Implant Treatment: History and Current Evidence

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Alveolar Ridge Changes following Tooth Extraction
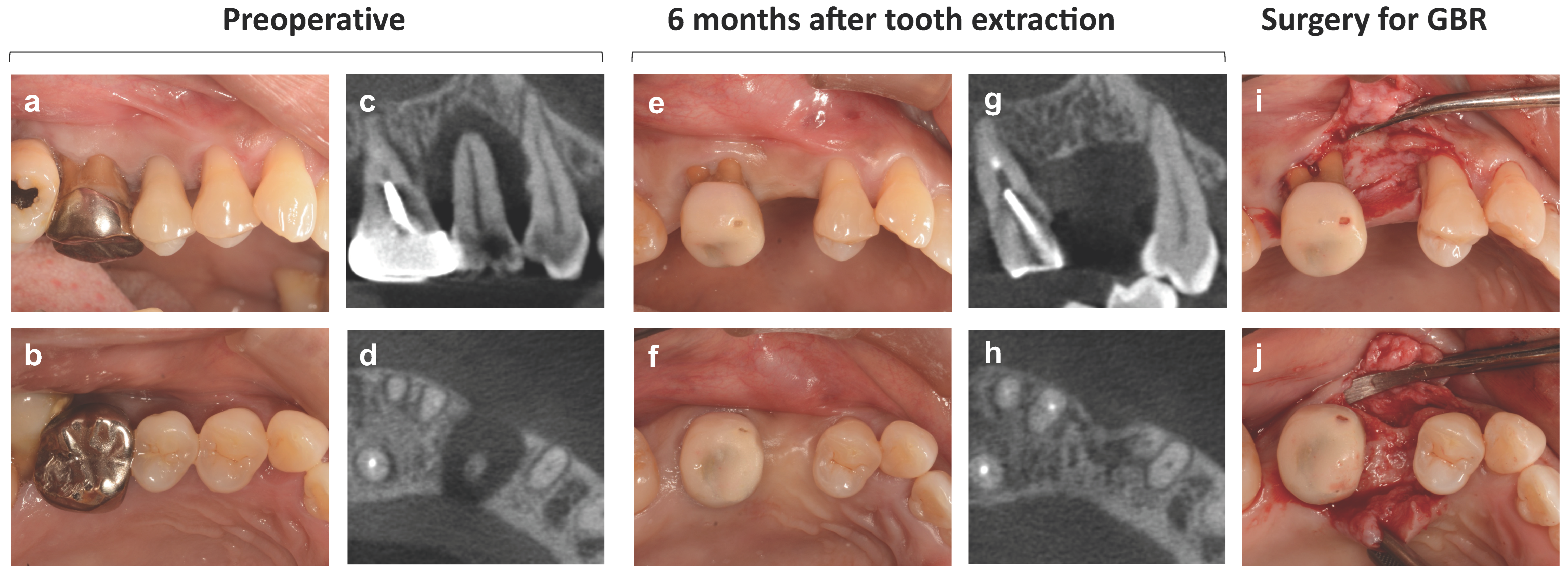
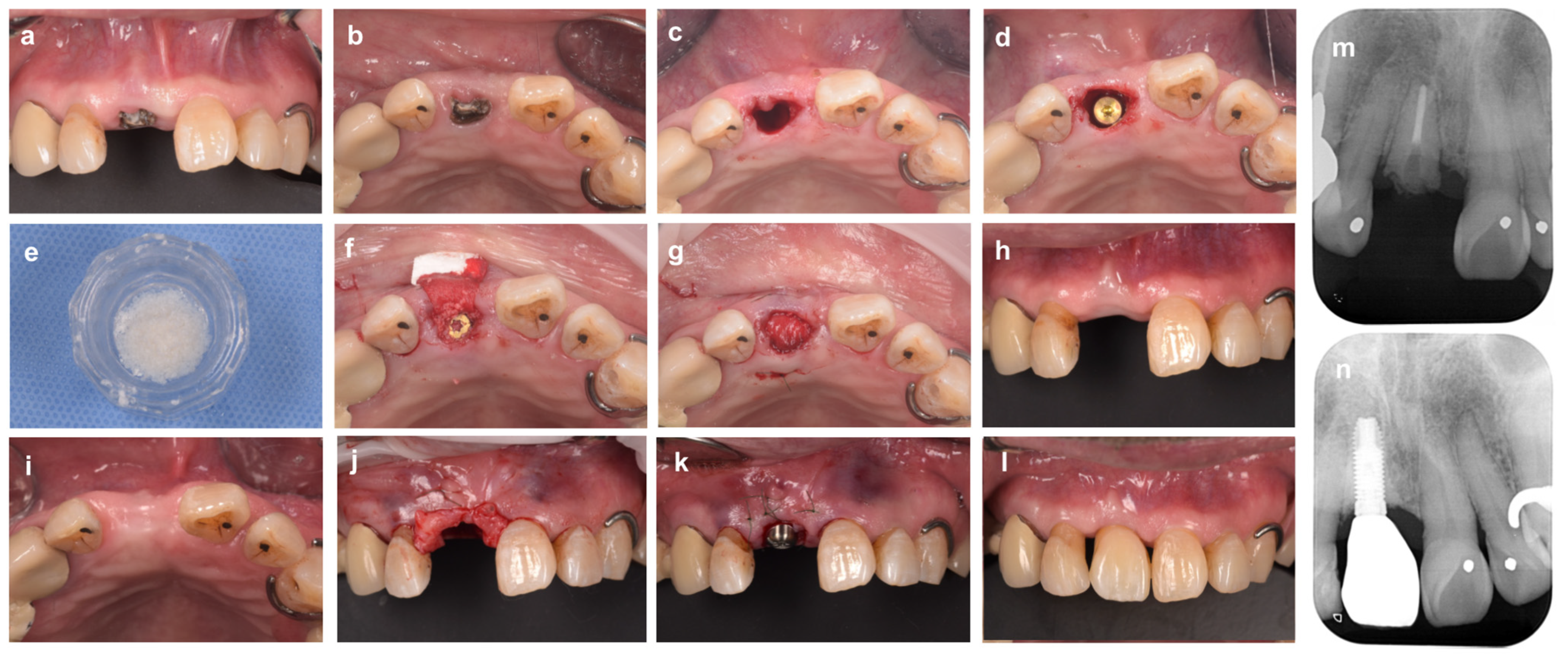
3. Immediate Implant Placement after Tooth Extraction
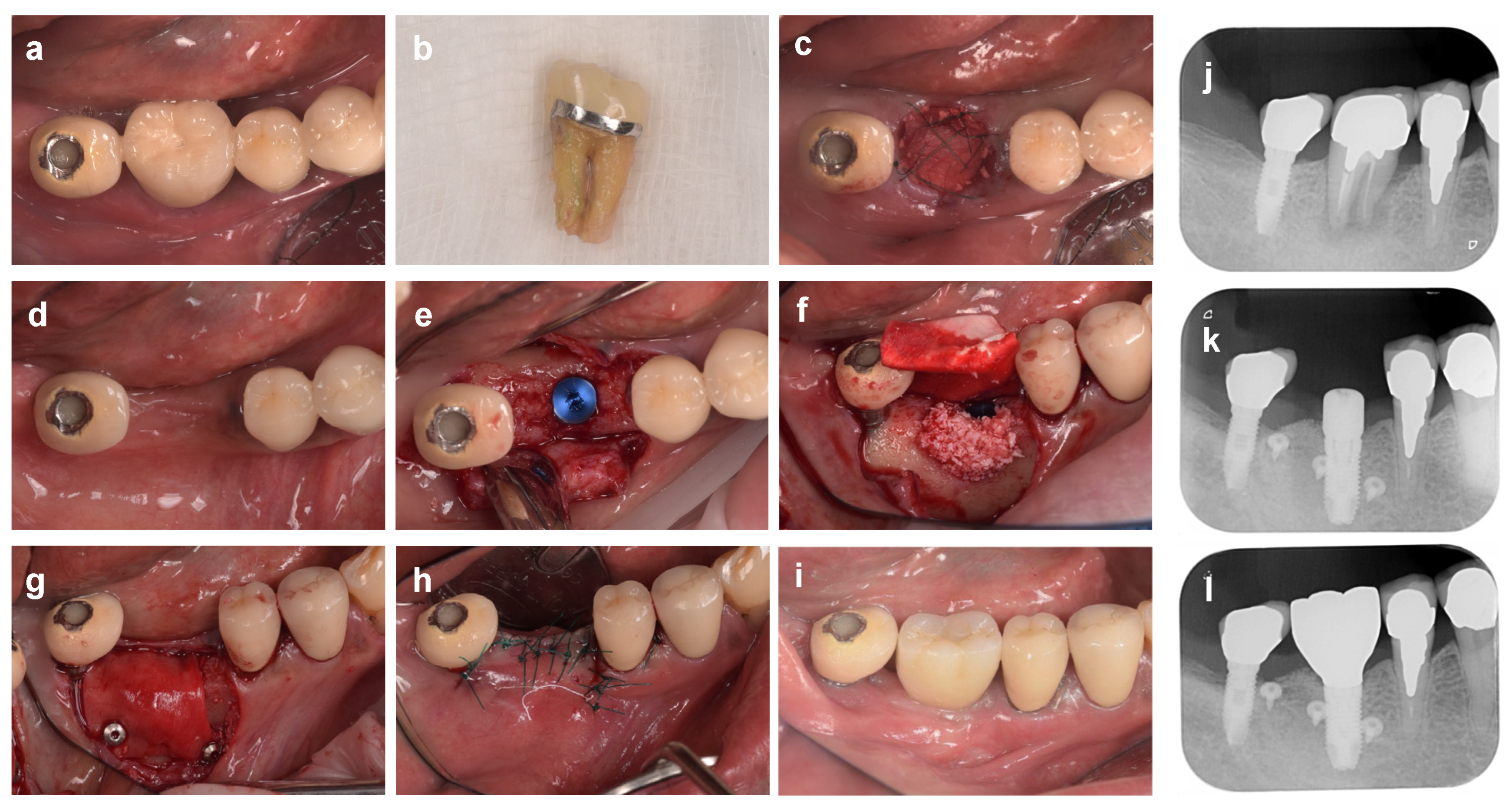
Clinical Case of Immediate Extraction Implant Placement with Bone Grafting
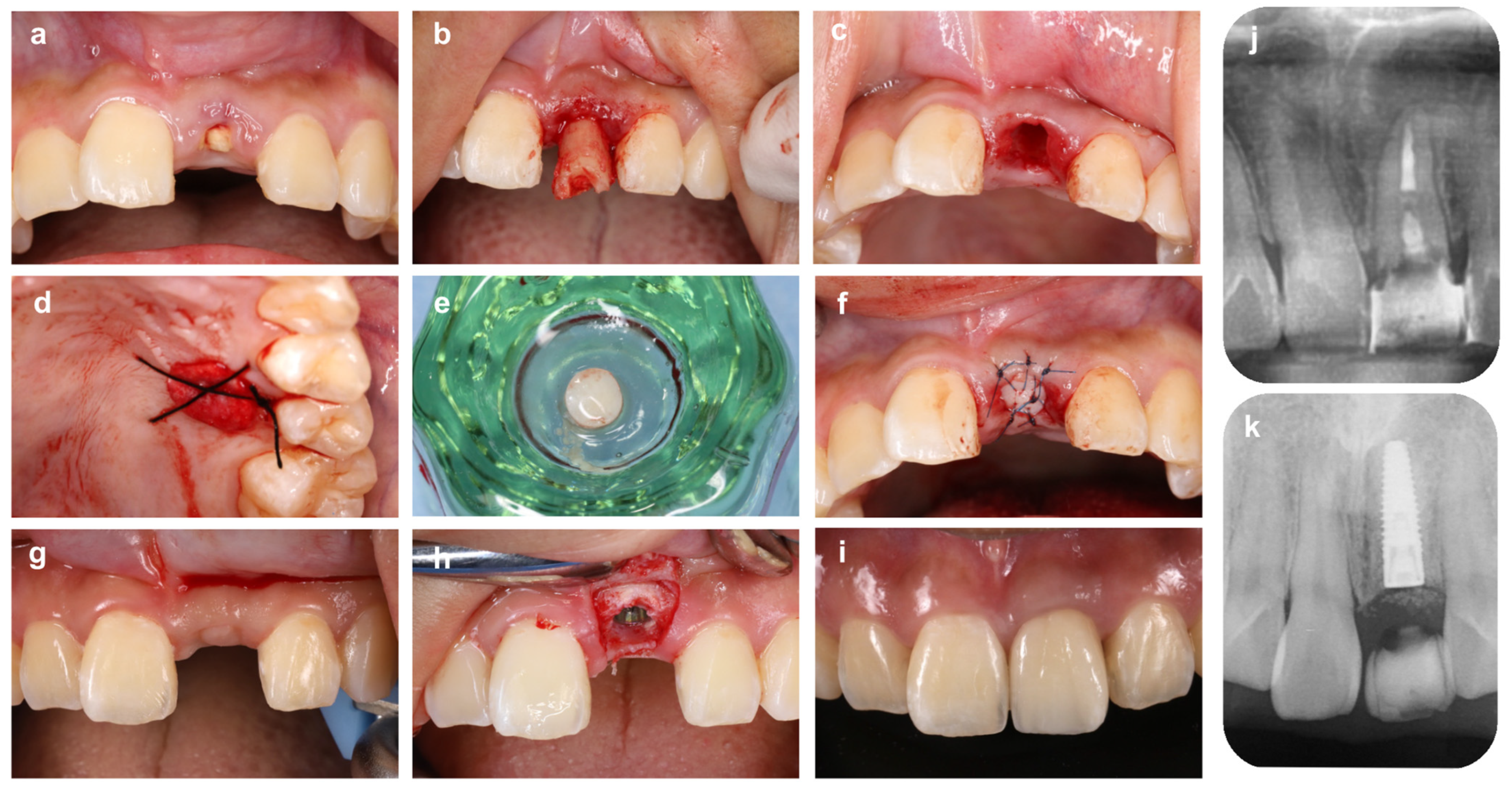
4. Alveolar Ridge Preservation
4.1. Alveolar Ridge Preservation with Soft Tissue or Alternative Graft Materials
Clinical Cases of Alveolar Ridge Preservation Using Soft Tissue or Alternative Membrane Material
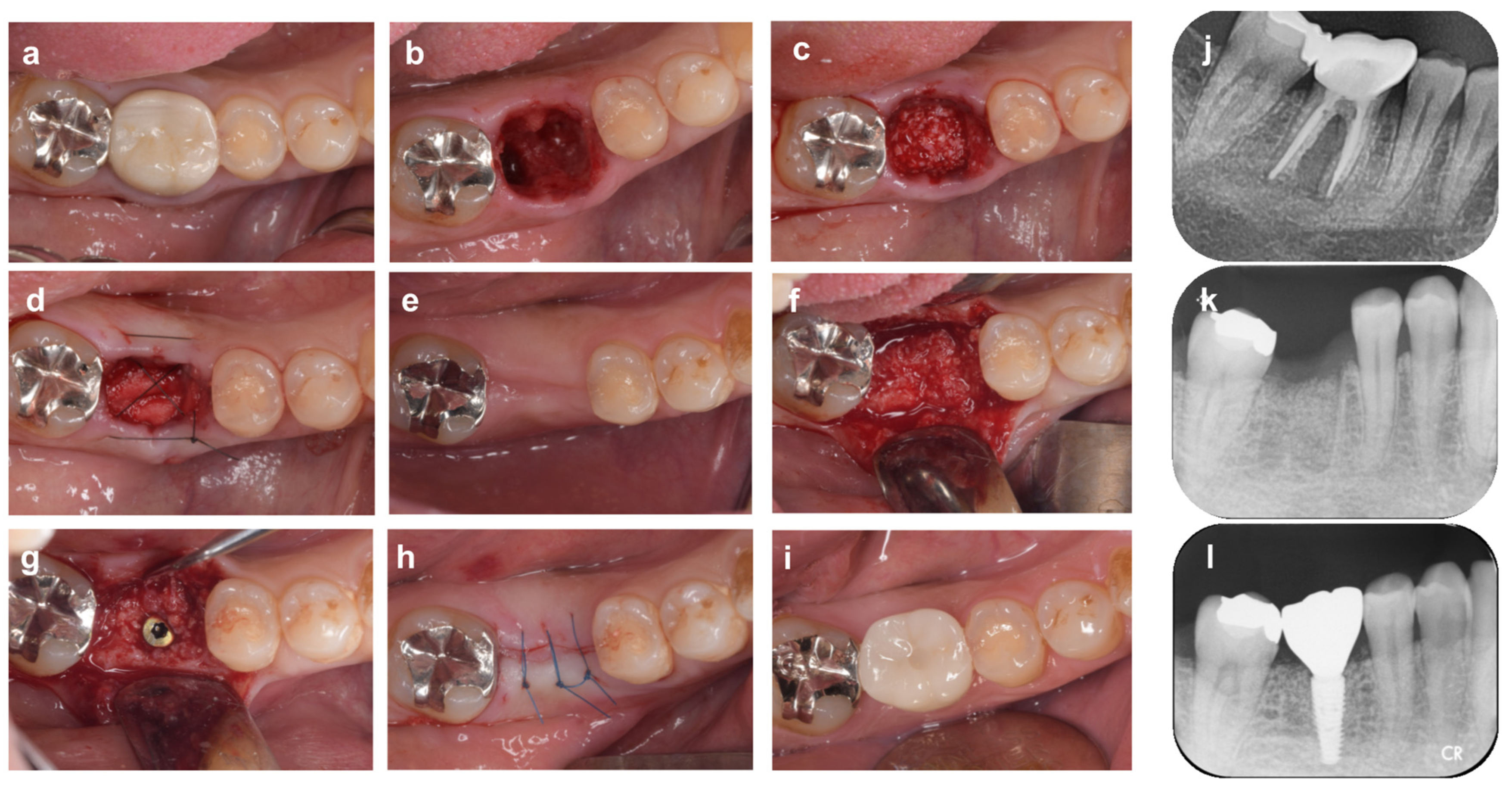
4.2. Alveolar Ridge Preservation with Non-Absorbable d-PTFE Membrane
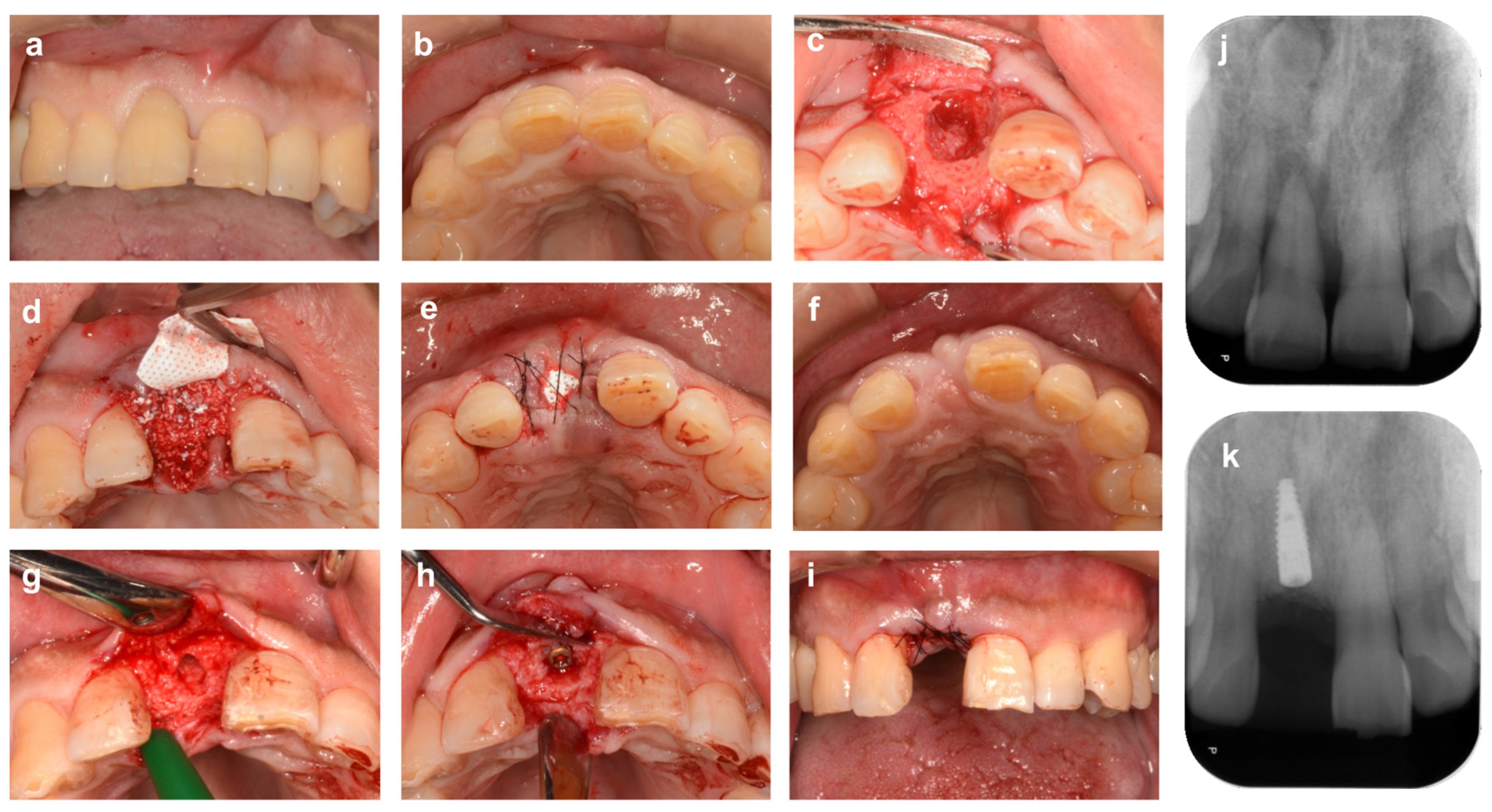
Clinical Cases of Alveolar Ridge Preservation with the Open Membrane Approach Using Non-Absorbable Membranes
5. The Need for Primary Closure of Extraction Sockets by Gingival Flaps
6. Bone Grafts for Alveolar Ridge Preservation
6.1. Biomaterials Science of Bone Graft Materials
6.2. Scientific Considerations for Bone Grafts Based on Clinical Studies
6.3. Criteria for the Use of Bone Grafts in Alveolar Ridge Preservation
7. Potential Risk Factors That Affect the Clinical Outcomes of Alveolar Ridge Preservation
8. Concluding Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Atwood, D.A. Reduction of residual ridges: A major oral disease entity. J. Prosthet. Dent. 1971, 26, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Pietrokovski, J.; Massler, M. Alveolar ridge resorption following tooth extraction. J. Prosthet. Dent. 1967, 17, 21–27. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- John, V.; De Poi, R.; Blanchard, S. Socket preservation as a precursor of future implant placement: Review of the literature and case reports. Compend. Contin. Educ. Dent. 2007, 28, 646–653, quiz 654, 671. [Google Scholar] [PubMed]
- Chatzopoulos, G.S.; Koidou, V.P.; Sonnenberger, M.; Johnson, D.; Chu, H.; Wolff, L.F. Postextraction ridge preservation by using dense PTFE membranes: A systematic review and meta-analysis. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 195–223. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Elangovan, S.; Kramer, K.W.; Blanchette, D.; Dawson, D.V. Effect of alveolar ridge preservation after tooth extraction: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 950–958. [Google Scholar] [CrossRef]
- Ashman, A.; Bruins, P. A new immediate hard tissue replacement (HTR)TM for bone in the oral cavity. J. Oral Implantol. 1982, 10, 419–452. [Google Scholar]
- Avila-Ortiz, G.; Gubler, M.; Romero-Bustillos, M.; Nicholas, C.L.; Zimmerman, M.B.; Barwacz, C.A. Efficacy of Alveolar Ridge Preservation: A Randomized Controlled Trial. J. Dent. Res. 2020, 99, 402–409. [Google Scholar] [CrossRef]
- Chavda, S.; Levin, L. Human Studies of Vertical and Horizontal Alveolar Ridge Augmentation Comparing Different Types of Bone Graft Materials: A Systematic Review. J. Oral Implantol. 2018, 44, 74–84. [Google Scholar] [CrossRef]
- Casarez-Quintana, A.; Mealey, B.L.; Kotsakis, G.; Palaiologou, A. Comparing the histological assessment following ridge preservation using a composite bovine-derived xenograft versus an alloplast hydroxyapatite-sugar cross-linked collagen matrix. J. Periodontol. 2022, 93, 1691–1700. [Google Scholar] [CrossRef] [PubMed]
- Myeroff, C.; Archdeacon, M. Autogenous bone graft: Donor sites and techniques. J. Bone Jt. Surg. Am. 2011, 93, 2227–2236. [Google Scholar] [CrossRef] [PubMed]
- Lazzara, R.J. Immediate implant placement into extraction sites: Surgical and restorative advantages. Int. J. Periodontics Restor. Dent. 1989, 9, 12. [Google Scholar]
- Becker, W.; Becker, B.E. Guided tissue regeneration for implants placed into extraction sockets and for implant dehiscences: Surgical techniques and case report. Int. J. Periodontics Restor. Dent. 1990, 10, 376–391. [Google Scholar]
- Lekovic, V.; Klokkevold, P.R.; Camargo, P.M.; Kenney, E.B.; Nedic, M.; Weinlaender, M. Evaluation of periosteal membranes and coronally positioned flaps in the treatment of Class II furcation defects: A comparative clinical study in humans. J. Periodontol. 1998, 69, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Stimmelmayr, M.; Guth, J.F.; Iglhaut, G.; Beuer, F. Preservation of the ridge and sealing of the socket with a combination epithelialised and subepithelial connective tissue graft for management of defects in the buccal bone before insertion of implants: A case series. Br. J. Oral Maxillofac. Surg. 2012, 50, 550–555. [Google Scholar] [CrossRef]
- Bartee, B.K. The use of high-density polytetrafluoroethylene membrane to treat osseous defects: Clinical reports. Implant Dent. 1995, 4, 21–26. [Google Scholar] [CrossRef]
- Oguic, M.; Candrlic, M.; Tomas, M.; Vidakovic, B.; Blaskovic, M.; Jerbic Radetic, A.T.; Zoricic Cvek, S.; Kuis, D.; Cvijanovic Peloza, O. Osteogenic Potential of Autologous Dentin Graft Compared with Bovine Xenograft Mixed with Autologous Bone in the Esthetic Zone: Radiographic, Histologic and Immunohistochemical Evaluation. Int. J. Mol. Sci. 2023, 24, 6440. [Google Scholar] [CrossRef]
- Sapoznikov, L.; Haim, D.; Zavan, B.; Scortecci, G.; Humphrey, M.F. A novel porcine dentin-derived bone graft material provides effective site stability for implant placement after tooth extraction: A randomized controlled clinical trial. Clin. Oral Investig. 2023, 27, 2899–2911. [Google Scholar] [CrossRef]
- Kutkut, A.; Andreana, S.; Kim, H.L.; Monaco, E., Jr. Extraction socket preservation graft before implant placement with calcium sulfate hemihydrate and platelet-rich plasma: A clinical and histomorphometric study in humans. J. Periodontol. 2012, 83, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Brahma Prasad Chary, N.O.; Raju, M.S.; Suresh Sajjan, M.C.; Gottumukkala, S.N.; Manyam, R. Comparison of quality of bone and insertion torque values of early implants placed at 6 and 8 weeks in sockets preserved with advanced platelet-rich fibrin: A randomized controlled trial. J. Indian Prosthodont. Soc. 2021, 21, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Alsabeeha, N.H.; Payne, A.G.; Ali, S.; Faggion, C.M.J.; Esposito, M. Interventions for replacing missing teeth: Alveolar ridge preservation techniques for dental implant site development. Cochrane Database Syst. Rev. 2021, 4, CD010176. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23 (Suppl. S5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K. A study of the dimensional changes occurring in the maxilla following tooth extraction. Aust. Dent. J. 1969, 14, 241–244. [Google Scholar] [CrossRef]
- Lam, R.V. Contour changes of the alveolar processes following extractions. J. Prosthet. Dent. 1960, 10, 25–32. [Google Scholar] [CrossRef]
- Araujo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontol 2000 2015, 68, 122–134. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Shahim, K.; Reyes, M.; Katsaros, C.; Buser, D. Soft Tissue Alterations in Esthetic Postextraction Sites: A 3-Dimensional Analysis. J. Dent. Res. 2015, 94, 187S–193S. [Google Scholar] [CrossRef]
- Chappuis, V.; Engel, O.; Reyes, M.; Shahim, K.; Nolte, L.P.; Buser, D. Ridge alterations post-extraction in the esthetic zone: A 3D analysis with CBCT. J. Dent. Res. 2013, 92, 195S–201S. [Google Scholar] [CrossRef]
- Misawa, M.; Lindhe, J.; Araujo, M.G. The alveolar process following single-tooth extraction: A study of maxillary incisor and premolar sites in man. Clin. Oral Implant. Res. 2016, 27, 884–889. [Google Scholar] [CrossRef]
- Schulte, W.; Kleineikenscheidt, H.; Lindner, K.; Schareyka, R.; Heimke, G.; Gerlach, C.; Hardegg, W. Animal experiments on the question of healing around the Tubingen immediate implant. Dtsch. Zahnarztl. Z. 1978, 33, 326–331. [Google Scholar] [PubMed]
- Barzilay, I.; Graser, G.N.; Iranpour, B.; Natiella, J.R. Immediate implantation of a pure titanium implant into an extraction socket: Report of a pilot procedure. Int. J. Oral Maxillofac. Implant. 1991, 5, 8. [Google Scholar]
- Lang, N.P.; Bragger, U.; Hammerle, C.H.; Sutter, F. Immediate transmucosal implants using the principle of guided tissue regeneration. I. Rationale, clinical procedures and 30-month results. Clin. Oral Implant. Res. 1994, 5, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Denissen, H.W.; Kalk, W.; Veldhuis, H.A.; van Waas, M.A. Anatomic consideration for preventive implantation. Int. J. Oral Maxillofac. Implant. 1993, 8, 191–196. [Google Scholar]
- Paolantonio, M.; Dolci, M.; Scarano, A.; d’Archivio, D.; di Placido, G.; Tumini, V.; Piattelli, A. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J. Periodontol. 2001, 72, 1560–1571. [Google Scholar] [CrossRef] [PubMed]
- Watzek, G.; Haider, R.; Mensdorff-Pouilly, N.; Haas, R. Immediate and delayed implantation for complete restoration of the jaw following extraction of all residual teeth: A retrospective study comparing different types of serial immediate implantation. Int. J. Oral Maxillofac. Implant. 1995, 10, 7. [Google Scholar]
- Araujo, M.G.; Sukekava, F.; Wennstrom, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implant. Res. 2006, 17, 615–624. [Google Scholar] [CrossRef]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Sanz, M.; Cecchinato, D.; Ferrus, J.; Pjetursson, E.B.; Lang, N.P.; Lindhe, J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin. Oral Implant. Res. 2010, 21, 13–21. [Google Scholar] [CrossRef]
- Araujo, M.G.; Sukekava, F.; Wennstrom, J.L.; Lindhe, J. Ridge alterations following implant placement in fresh extraction sockets: An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 645–652. [Google Scholar] [CrossRef]
- Araujo, M.G.; Wennstrom, J.L.; Lindhe, J. Modeling of the buccal and lingual bone walls of fresh extraction sites following implant installation. Clin. Oral Implant. Res. 2006, 17, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Ferrus, J.; Cecchinato, D.; Pjetursson, E.B.; Lang, N.P.; Sanz, M.; Lindhe, J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin. Oral Implant. Res. 2010, 21, 22–29. [Google Scholar] [CrossRef]
- Matarasso, S.; Salvi, G.E.; Iorio Siciliano, V.; Cafiero, C.; Blasi, A.; Lang, N.P. Dimensional ridge alterations following immediate implant placement in molar extraction sites: A six-month prospective cohort study with surgical re-entry. Clin. Oral Implant. Res. 2009, 20, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C. A prospective clinical study of non-submerged immediate implants: Clinical outcomes and esthetic results. Clin. Oral Implant. Res. 2007, 18, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Hammerle, C.H.; Araujo, M.G.; Simion, M.; Osteology Consensus, G. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin. Oral Implant. Res. 2012, 23 (Suppl. S5), 80–82. [Google Scholar] [CrossRef] [PubMed]
- Artzi, Z.; Nemcovsky, C.E. The application of deproteinized bovine bone mineral for ridge preservation prior to implantation. Clinical and histological observations in a case report. J. Periodontol. 1998, 69, 1062–1067. [Google Scholar] [CrossRef]
- De Risi, V.; Clementini, M.; Vittorini, G.; Mannocci, A.; De Sanctis, M. Alveolar ridge preservation techniques: A systematic review and meta-analysis of histological and histomorphometrical data. Clin. Oral Implant. Res. 2015, 26, 50–68. [Google Scholar] [CrossRef]
- Horvath, A.; Mardas, N.; Mezzomo, L.A.; Needleman, I.G.; Donos, N. Alveolar ridge preservation. A systematic review. Clin. Oral Investig. 2013, 17, 341–363. [Google Scholar] [CrossRef]
- Canellas, J.; Soares, B.N.; Ritto, F.G.; Vettore, M.V.; Vidigal Junior, G.M.; Fischer, R.G.; Medeiros, P.J.D. What grafting materials produce greater alveolar ridge preservation after tooth extraction? A systematic review and network meta-analysis. J. Craniomaxillofac. Surg. 2021, 49, 1064–1071. [Google Scholar] [CrossRef]
- Landsberg, C.J. Socket seal surgery combined with immediate implant placement: A novel approach for single-tooth replacement. Int. J. Periodontics Restor. Dent. 1997, 17, 140–149. [Google Scholar]
- Landsberg, C.J.; Bichacho, N. A modified surgical/prosthetic approach for optimal single implant supported crown. Part I—The socket seal surgery. Pract. Periodontics Aesthet. Dent. 1994, 6, 11–17, quiz 19. [Google Scholar] [PubMed]
- Jung, R.E.; Siegenthaler, D.W.; Hammerle, C.H. Postextraction tissue management: A soft tissue punch technique. Int. J. Periodontics Restor. Dent. 2004, 24, 545–553. [Google Scholar]
- Stimmelmayr, M.; Allen, E.P.; Reichert, T.E.; Iglhaut, G. Use of a combination epithelized-subepithelial connective tissue graft for closure and soft tissue augmentation of an extraction site following ridge preservation or implant placement: Description of a technique. Int. J. Periodontics Restor. Dent. 2010, 30, 375–381. [Google Scholar]
- Papace, C.; Busch, C.; Ristow, O.; Keweloh, M.; Hoffmann, J.; Mertens, C. The effect of different soft-tissue management techniques for alveolar ridge preservation: A randomized controlled clinical trial. Int. J. Implant. Dent. 2021, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Segnini, B.; Borges-Filho, F.F.; Nicoli, L.G.; Goncalves, M.; Marcantonio, C.; Oliveira, G.J.; Marcantonio, E., Jr. Impact of soft tissue graft on the preservation of compromised sockets: A randomized controlled clinical pilot study. Acta Odontol. Latinoam. 2021, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Sukekava, F.; Araujo, M.G.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Root-coverage procedures for the treatment of localized recession-type defects: A Cochrane systematic review. J. Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef]
- Oates, T.W.; Robinson, M.; Gunsolley, J.C. Surgical therapies for the treatment of gingival recession. A systematic review. Ann. Periodontol. 2003, 8, 303–320. [Google Scholar] [CrossRef]
- McGuire, M.K.; Scheyer, E.T. Randomized, controlled clinical trial to evaluate a xenogeneic collagen matrix as an alternative to free gingival grafting for oral soft tissue augmentation. J. Periodontol. 2014, 85, 1333–1341. [Google Scholar] [CrossRef]
- Lim, H.C.; Jung, U.W.; You, H.; Lee, J.S. Randomized clinical trial of ridge preservation using porcine bone/cross-linked collagen vs. bovine bone/non-cross-linked collagen: Cone beam computed tomographic analysis. Clin. Oral Implant. Res. 2017, 28, 1492–1500. [Google Scholar] [CrossRef]
- Barber, H.D.; Lignelli, J.; Smith, B.M.; Bartee, B.K. Using a dense PTFE membrane without primary closure to achieve bone and tissue regeneration. J. Oral Maxillofac. Surg. 2007, 65, 748–752. [Google Scholar] [CrossRef]
- Simion, M.; Baldoni, M.; Rossi, P.; Zaffe, D. A comparative study of the effectiveness of e-PTFE membranes with and without early exposure during the healing period. Int. J. Periodontics Restor. Dent. 1994, 14, 166–180. [Google Scholar]
- Bartee, B.K. Extraction site reconstruction for alveolar ridge preservation. Part 2: Membrane-assisted surgical technique. J. Oral Implantol. 2001, 27, 194–197. [Google Scholar] [CrossRef]
- Bartee, B.K. Evaluation of a new polytetrafluoroethylene guided tissue regeneration membrane in healing extraction sites. Compend. Contin. Educ. Dent. 1998, 19, 1256–1258+1260+1262–1264. [Google Scholar] [PubMed]
- Arbab, H.; Greenwell, H.; Hill, M.; Morton, D.; Vidal, R.; Shumway, B.; Allan, N.D. Ridge Preservation Comparing a Nonresorbable PTFE Membrane to a Resorbable Collagen Membrane: A Clinical and Histologic Study in Humans. Implant Dent. 2016, 25, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.J.; Lim, H.C.; Lee, D.W. Alveolar ridge preservation using an open membrane approach for sockets with bone deficiency: A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lee, J.B.; Koo, K.T.; Seol, Y.J.; Lee, Y.M. Flap Management in Alveolar Ridge Preservation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 613–621. [Google Scholar] [CrossRef]
- Engler-Hamm, D.; Cheung, W.S.; Yen, A.; Stark, P.C.; Griffin, T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: A comparative clinical trial. J. Periodontol. 2011, 82, 377–387. [Google Scholar] [CrossRef]
- Barone, A.; Borgia, V.; Covani, U.; Ricci, M.; Piattelli, A.; Iezzi, G. Flap versus flapless procedure for ridge preservation in alveolar extraction sockets: A histological evaluation in a randomized clinical trial. Clin. Oral Implant. Res. 2015, 26, 806–813. [Google Scholar] [CrossRef]
- Martins, J.R.; Wagner, T.P.; Vallim, A.C.; Konflanz, W.; Schwendicke, F.; Celeste, R.K.; Haas, A.N. Comparison of the efficacy of different techniques to seal the alveolus during alveolar ridge preservation: Meta-regression and network meta-analysis. J. Clin. Periodontol. 2022, 49, 694–705. [Google Scholar] [CrossRef]
- Brkovic, B.M.; Prasad, H.S.; Rohrer, M.D.; Konandreas, G.; Agrogiannis, G.; Antunovic, D.; Sandor, G.K. Beta-tricalcium phosphate/type I collagen cones with or without a barrier membrane in human extraction socket healing: Clinical, histologic, histomorphometric, and immunohistochemical evaluation. Clin. Oral Investig. 2012, 16, 581–590. [Google Scholar] [CrossRef]
- Lim, H.C.; Shin, H.S.; Cho, I.W.; Koo, K.T.; Park, J.C. Ridge preservation in molar extraction sites with an open-healing approach: A randomized controlled clinical trial. J. Clin. Periodontol. 2019, 46, 1144–1154. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Couso-Queiruga, E.; Shiau, H.J.; Stuhr, S.; Prasad, H.; Allareddy, T.V.; Reynolds, M.A.; Avila-Ortiz, G. Evaluation of poly lactic-co-glycolic acid-coated beta-tricalcium phosphate for alveolar ridge preservation: A multicenter randomized controlled trial. J. Periodontol. 2021, 92, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Philipp, A.; Annen, B.M.; Signorelli, L.; Thoma, D.S.; Hammerle, C.H.; Attin, T.; Schmidlin, P. Radiographic evaluation of different techniques for ridge preservation after tooth extraction: A randomized controlled clinical trial. J. Clin. Periodontol. 2013, 40, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Jamjoom, A.; Cohen, R.E. Grafts for Ridge Preservation. J. Funct. Biomater. 2015, 6, 833–848. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, V.M.; Stevenson, S. Natural history of autografts and allografts. Clin. Orthop. Relat. Res. 1987, 225, 7–16. [Google Scholar] [CrossRef]
- Zhao, R.; Yang, R.; Cooper, P.R.; Khurshid, Z.; Shavandi, A.; Ratnayake, J. Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments. Molecules 2021, 26, 3007. [Google Scholar] [CrossRef]
- Dias, R.R.; Sehn, F.P.; de Santana Santos, T.; Silva, E.R.; Chaushu, G.; Xavier, S.P. Corticocancellous fresh-frozen allograft bone blocks for augmenting atrophied posterior mandibles in humans. Clin. Oral Implant. Res. 2016, 27, 39–46. [Google Scholar] [CrossRef]
- Quattlebaum, J.B.; Mellonig, J.T.; Hensel, N.F. Antigenicity of freeze-dried cortical bone allograft in human periodontal osseous defects. J. Periodontol. 1988, 59, 394–397. [Google Scholar] [CrossRef]
- The Committee on Research, Science and Therapy of the American Academy of Periodontology. Position Paper; Tissue Banking of Bone Allografts Used in Periodontal Regeneration. J. Periodontol. 2001, 72, 834–838. [Google Scholar] [CrossRef]
- Russell, J.; Scarborough, N.; Chesmel, K. Re: Ability of commercial demineralized freeze-dried bone allograft to induce new bone formation (1996, 67, 918–926). J. Periodontol. 1997, 68, 804–806. [Google Scholar]
- Mellonig, J.T.; Bowers, G.M.; Bailey, R.C. Comparison of bone graft materials. Part I. New bone formation with autografts and allografts determined by Strontium-85. J. Periodontol. 1981, 52, 291–296. [Google Scholar] [CrossRef] [PubMed]
- McAllister, B.S.; Margolin, M.D.; Cogan, A.G.; Buck, D.; Hollinger, J.O.; Lynch, S.E. Eighteen-month radiographic and histologic evaluation of sinus grafting with anorganic bovine bone in the chimpanzee. Int. J. Oral Maxillofac. Implant. 1999, 14, 361–368. [Google Scholar]
- Sogal, A.; Tofe, A.J. Risk assessment of bovine spongiform encephalopathy transmission through bone graft material derived from bovine bone used for dental applications. J. Periodontol. 1999, 70, 1053–1063. [Google Scholar] [CrossRef] [PubMed]
- Shetty, V.; Han, T.J. Alloplastic materials in reconstructive periodontal surgery. Dent. Clin. N. Am. 1991, 35, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, Y.; Zuo, Y.; Li, J.; Ma, S.; Cheng, L. Biocompatibility and osteogenesis of biomimetic nano-hydroxyapatite/polyamide composite scaffolds for bone tissue engineering. Biomaterials 2007, 28, 3338–3348. [Google Scholar] [CrossRef] [PubMed]
- Osborn, J.F.; Newesely, H. The material science of calcium phosphate ceramics. Biomaterials 1980, 1, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.P.; Driessen, A.A.; de Groot, K.; van den Hooff, A. Biodegradation behavior of various calcium phosphate materials in bone tissue. J. Biomed. Mater. Res. 1983, 17, 769–784. [Google Scholar] [CrossRef]
- Rabalais, M.L., Jr.; Yukna, R.A.; Mayer, E.T. Evaluation of durapatite ceramic as an alloplastic implant in periodontal osseous defects. I. Initial six-month results. J. Periodontol. 1981, 52, 680–689. [Google Scholar] [CrossRef]
- Schepers, E.; de Clercq, M.; Ducheyne, P.; Kempeneers, R. Bioactive glass particulate material as a filler for bone lesions. J. Oral Rehabil. 1991, 18, 439–452. [Google Scholar] [CrossRef]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int. J. Mol. Sci. 2019, 20, 5960. [Google Scholar] [CrossRef]
- Carvalho, S.M.; Oliveira, A.A.; Jardim, C.A.; Melo, C.B.; Gomes, D.A.; de Fatima Leite, M.; Pereira, M.M. Characterization and induction of cementoblast cell proliferation by bioactive glass nanoparticles. J. Tissue Eng. Regen. Med. 2012, 6, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Jeong, S.N. Effect of enamel matrix derivative on alveolar ridge preservation in the posterior maxilla: A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2020, 22, 622–630. [Google Scholar] [CrossRef]
- Mercado, F.; Vaquette, C.; Hamlet, S.; Ivanovski, S. Enamel matrix derivative promotes new bone formation in xenograft assisted maxillary anterior ridge preservation-A randomized controlled clinical trial. Clin. Oral Implant. Res. 2021, 32, 732–744. [Google Scholar] [CrossRef] [PubMed]
- Eeckhout, C.; Ackerman, J.; Glibert, M.; Cosyn, J. A randomized controlled trial evaluating hyaluronic acid gel as wound healing agent in alveolar ridge preservation. J. Clin. Periodontol. 2022, 49, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Orlando, B.; Cingano, L.; Marconcini, S.; Derchi, G.; Covani, U. A randomized clinical trial to evaluate and compare implants placed in augmented versus non-augmented extraction sockets: 3-year results. J. Periodontol. 2012, 83, 836–846. [Google Scholar] [CrossRef] [PubMed]
- Festa, V.M.; Addabbo, F.; Laino, L.; Femiano, F.; Rullo, R. Porcine-derived xenograft combined with a soft cortical membrane versus extraction alone for implant site development: A clinical study in humans. Clin. Implant Dent. Relat. Res. 2013, 15, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.K.; Song, Y.W.; Park, S.H.; Jung, R.E.; Jung, U.W.; Thoma, D.S. Alveolar ridge preservation in the posterior maxilla reduces vertical dimensional change: A randomized controlled clinical trial. Clin. Oral Implant. Res. 2019, 30, 515–523. [Google Scholar] [CrossRef]
- Iorio-Siciliano, V.; Ramaglia, L.; Blasi, A.; Bucci, P.; Nuzzolo, P.; Riccitiello, F.; Nicolo, M. Dimensional changes following alveolar ridge preservation in the posterior area using bovine-derived xenografts and collagen membrane compared to spontaneous healing: A 6-month randomized controlled clinical trial. Clin. Oral Investig. 2020, 24, 1013–1023. [Google Scholar] [CrossRef]
- Santana, R.; Gyurko, R.; Kanasi, E.; Xu, W.P.; Dibart, S. Synthetic polymeric barrier membrane associated with blood coagulum, human allograft, or bovine bone substitute for ridge preservation: A randomized, controlled, clinical and histological trial. Int. J. Oral Maxillofac. Surg. 2019, 48, 675–683. [Google Scholar] [CrossRef]
- Scheyer, E.T.; Heard, R.; Janakievski, J.; Mandelaris, G.; Nevins, M.L.; Pickering, S.R.; Richardson, C.R.; Pope, B.; Toback, G.; Velasquez, D.; et al. A randomized, controlled, multicentre clinical trial of post-extraction alveolar ridge preservation. J. Clin. Periodontol. 2016, 43, 1188–1199. [Google Scholar] [CrossRef]
- Serrano Mendez, C.A.; Lang, N.P.; Caneva, M.; Ramirez Lemus, G.; Mora Solano, G.; Botticelli, D. Comparison of allografts and xenografts used for alveolar ridge preservation. A clinical and histomorphometric RCT in humans. Clin. Implant Dent. Relat. Res. 2017, 19, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Chisci, G.; Hatia, A.; Chisci, E.; Chisci, D.; Gennaro, P.; Gabriele, G. Socket Preservation after Tooth Extraction: Particulate Autologous Bone vs. Deproteinized Bovine Bone. Bioengineering 2023, 10, 421. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.Y.; Lee, Y.; Lim, J.H.; Jin, M.U.; Lee, J.M.; Suh, J.Y.; Kim, Y.G. Comparative Evaluation of Recombinant Human Bone Morphogenetic Protein-2/Hydroxyapatite and Bovine Bone for New Bone Formation in Alveolar Ridge Preservation. Implant Dent. 2018, 27, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Bonta, H.; Galli, F.G.; Gualtieri, A.; Renou, S.; Caride, F. The Effect of an Alloplastic Bone Substitute and Enamel Matrix Derivative on the Preservation of Single Anterior Extraction Sockets: A Histologic Study in Humans. Int. J. Periodontics Restor. Dent. 2022, 42, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Mayer, Y.; Zigdon-Giladi, H.; Machtei, E.E. Ridge Preservation Using Composite Alloplastic Materials: A Randomized Control Clinical and Histological Study in Humans. Clin. Implant Dent. Relat. Res. 2016, 18, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Noronha Oliveira, M.; Rau, L.H.; Marodin, A.; Correa, M.; Correa, L.R.; Aragones, A.; Magini, R.S. Ridge Preservation After Maxillary Third Molar Extraction Using 30% Porosity PLGA/HA/beta-TCP Scaffolds With and Without Simvastatin: A Pilot Randomized Controlled Clinical Trial. Implant Dent. 2017, 26, 832–840. [Google Scholar] [CrossRef]
- Cortellini, P. Minimally invasive surgical techniques in periodontal regeneration. J. Evid. Based Dent. Pract. 2012, 12, 89–100. [Google Scholar] [CrossRef]
- Becker, W.; Clokie, C.; Sennerby, L.; Urist, M.R.; Becker, B.E. Histologic findings after implantation and evaluation of different grafting materials and titanium micro screws into extraction sockets: Case reports. J. Periodontol. 1998, 69, 414–421. [Google Scholar] [CrossRef]
- Carmagnola, D.; Adriaens, P.; Berglundh, T. Healing of human extraction sockets filled with Bio-Oss. Clin. Oral Implant. Res. 2003, 14, 137–143. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sano, T.; Kuraji, R.; Miyashita, Y.; Yano, K.; Kawanabe, D.; Numabe, Y. Biomaterials for Alveolar Ridge Preservation as a Preoperative Procedure for Implant Treatment: History and Current Evidence. Bioengineering 2023, 10, 1376. https://doi.org/10.3390/bioengineering10121376
Sano T, Kuraji R, Miyashita Y, Yano K, Kawanabe D, Numabe Y. Biomaterials for Alveolar Ridge Preservation as a Preoperative Procedure for Implant Treatment: History and Current Evidence. Bioengineering. 2023; 10(12):1376. https://doi.org/10.3390/bioengineering10121376
Chicago/Turabian StyleSano, Tetsuya, Ryutaro Kuraji, Yukihiro Miyashita, Kosei Yano, Dai Kawanabe, and Yukihiro Numabe. 2023. "Biomaterials for Alveolar Ridge Preservation as a Preoperative Procedure for Implant Treatment: History and Current Evidence" Bioengineering 10, no. 12: 1376. https://doi.org/10.3390/bioengineering10121376
APA StyleSano, T., Kuraji, R., Miyashita, Y., Yano, K., Kawanabe, D., & Numabe, Y. (2023). Biomaterials for Alveolar Ridge Preservation as a Preoperative Procedure for Implant Treatment: History and Current Evidence. Bioengineering, 10(12), 1376. https://doi.org/10.3390/bioengineering10121376