
Preoperative Planning Framework for Robot-Assisted Dental Implant Surgery: Finite-Parameter Surrogate Model and Optimization of Instrument Placement


Abstract
1. Introduction
1.1. Background and Task
1.2. Related Works
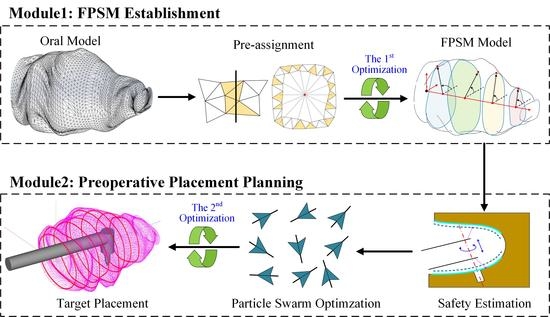
- A new finite-parameter surrogate model (FPSM) is proposed, in which the oral cavity is replaced by a group of closed curves described in the polar coordinate system. All the parameters of closed curves can be optimized to fit the oral structure. This can significantly increase the real-time performance and reduce the computational burden for most of the planning tasks in which complex 3D oral structures should be involved.
- Based on the FPSM, an efficient collision-detection method can be determined through cylinder-to-line simplification of the instrument’s rod.
- The feeding target is automatically placed through the particle swarm optimization (PSO) algorithm, which is the second stage of optimization, forming the preoperative planning framework.
- The framework is an essential expansion of the previous work on VF. With the VF and the planning framework combined, a full strategy is established.
2. System, Task, and Framework
2.1. System Constitution
2.2. Planning Task for Virtual Fixture
2.3. Overview of Two-Stage Optimization Framework
3. Finite-Parameter Surrogate Model
3.1. Parameterization of Closed Curves
3.2. Parameter Optimization of Closed Curves
- The area of the closed curve should be as large as possible to better-simulate the boundary of the oral structure, and the maximum possible area is when the closed curve exactly coincides with the boundary. This point aims to provide accessible spaces for preoperative planning as much as possible.
- The closed curve should not collide with the triangular mesh, or should only allow very slight collisions to be accepted. This point aims to prevent collisions and ensure safety.
3.3. Establishment of FPSM
4. Automatic Placement of Feeding Target
4.1. Collision Detection and Safety Estimation
4.2. Establishment of Objective Function
4.3. Optimization of Preoperative Placement
5. Tests, Results, and Discussion
5.1. Test of FPSM Establishment
5.2. Test of Optimization for Instrument Placement
5.3. Discussion
6. Conclusions and Future Work
- A new finite parameter surrogate model for the oral cavity, also called the FPSM, is designed using an array of closed curves in polar coordinates. After pre-assignment of the triangular mesh of the oral cavity, the model is solved during the first stage of optimization through gradient descent and penalty function methods.
- The placement for the implanting instrument is solved using the PSO algorithm in the second stage of optimization, during which the FPSM serves as a safety estimator to drive the iteration to converge to the optimal solution.
- The FPSM solver, the PSO solver, and a 3D visualization software are developed, and the performance of the entire framework is tested, preliminarily verifying the effectiveness of the proposed framework.
- The FPSM has the feature of high real-time quality, accuracy, flexibility, and multifunctionality, which has great potential to play a role in preoperative planning, online trajectory planning, intraoperative motion regulating, and collision alarming. Combined with the PSO solver, the framework is an important expansion of the previously proposed work.
- The FPSM will be used for other tasks and applications, including preoperative planning, online trajectory planning, intraoperative motion regulating, and collision alarming, which can bring more safety for other modes of surgical operation.
- The proposed framework will be seamlessly integrated with master-salve control, virtual fixture, vision system, and system hardware. When all the modules are combined, a complete master-slave teleoperation test can be conducted, during which some control aspects including some non-linearities will be investigated and addressed.
- Some artificial intelligence models, such as objective encoding and predicting networks, that are being studied in mobile robot navigation can be adopted and applied to the aspect of traditional robotic manipulators, which can bring more methods or approaches for robot-assisted oral surgery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mihara, Y.; Matsuda, K.; Takahashi, T.; Hatta, K.; Fukutake, M.; Sato, H.; Gondo, Y.; Masui, Y.; Kamide, K.; Sugimoto, K.; et al. Occlusal support predicts tooth loss in older Japanese people. Community Dent. Oral Epidemiol. 2020, 48, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Kusama, T.; Nakazawa, N.; Kiuchi, S.; Kondo, K.; Osaka, K.; Aida, J. Dental prosthetic treatment reduced the risk of weight loss among older adults with tooth loss. Ournal Am. Geriatr. Soc. 2021, 69, 2498–2506. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, R.; Botelho, J.; Machado, V.; Mascarenhas, P.; Alcoforado, G.; Mendes, J.; Chambrone, L. Predictors of tooth loss during long-term periodontal maintenance: An updated systematic review. J. Clin. Periodontol. 2021, 48, 1019–1036. [Google Scholar] [CrossRef]
- Kudsi, Z.; Fenlon, M.; Johal, A.; Baysan, A. Assessment of Psychological Disturbance in Patients with Tooth Loss: A Systematic Review of Assessment Tools. J. Prosthodont.-Implant. Esthet. Reconstr. Dent. 2020, 29, 193–200. [Google Scholar] [CrossRef]
- Hosadurga, R.; Soe, H.; Lim, A.; Adl, A.; Mathew, M. Association between tooth loss and hypertension: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 925–932. [Google Scholar] [CrossRef]
- Flanagan, D. Rationale for Mini Dental Implant Treatment. J. Oral Implantol. 2020, 47, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Trullenque-Eriksson, A.; Guisado-Moya, B. Retrospective Long-term Evaluation of Dental Implants in Totally and Partially Edentulous Patients. Part I: Survival and Marginal Bone Loss. Implant. Dent. 2014, 23, 732–737. [Google Scholar] [CrossRef]
- Trullenque-Eriksson, A.; Guisado-Moya, B. Retrospective Long-Term Evaluation of Dental Implants in Totally and Partially Edentulous Patients: Part II: Periimplant Disease. Implant. Dent. 2015, 24, 217–221. [Google Scholar] [CrossRef]
- Ahmad, P.; Alam, M.K.; Aldajani, A.; Alahmari, A.; Alanazi, A.; Stoddart, M.; Sghaireen, M.G. Dental Robotics: A Disruptive Technology. Sensors 2021, 21, 3308. [Google Scholar] [CrossRef]
- Riet, T.; Sem, K.; Ho, J.; Spijker, R.; Kober, J.; Lange, J. Robot technology in dentistry, part one of a systematic review: Literature characteristics. Dent. Mater. 2021, 37, 1217–1226. [Google Scholar] [CrossRef]
- Riet, T.; Sem, K.; Ho, J.; Spijker, R.; Kober, J.; Lange, J. Robot technology in dentistry, part two of a systematic review: An overview of initiatives. Dent. Mater. 2021, 37, 1227–1236. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, W.; Cai, Y.; Zhao, Q.; Wang, Y.; Hu, Y.; Wang, S. A Guiding and Positioning Motion Strategy Based on a New Conical Virtual Fixture for Robot-Assisted Oral Surgery. Machines 2023, 11, 3. [Google Scholar] [CrossRef]
- Sun, X.; McKenzie, F.; Bawab, S.; Li, J.; Yoon, Y.; Huang, J. Automated dental implantation using image-guided robotics: Registration results. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Yoon, Y.; Li, J.; McKenzie, F. Automated image-guided surgery for common and complex dental implants. J. Med. Eng. Technol. 2014, 38, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.; Uozumi, S.; Ohnishi, K.; Usuda, S.; Kawana, H. Stereo Vision based Robot Navigation System Using Modulated Potential Field for Implant Surgery. In Proceedings of the 2015 IEEE International Conference on Industrial Technology, Seville, Spain, 17–19 March 2015; pp. 493–498. [Google Scholar]
- Li, J.; Lam, W.; Hsung, R.; Pow, E.; Wang, Z. A Customizable, Compact Robotic Manipulator for Assisting Multiple Dental Procedures. In Proceedings of the 2018 3rd IEEE International Conference on Advanced Robotics and Mechatronics, Singapore, 18–20 July 2018; pp. 720–725. [Google Scholar]
- Li, J.; Shen, Z.; Xu, W.; Lam, W.; Hsung, R.; Pow, E.; Kosuge, K.; Wang, Z. A Compact Dental Robotic System Using Soft Bracing Technique. IEEE Robot. Autom. Lett. 2019, 4, 1271–1278. [Google Scholar] [CrossRef]
- Li, J.; Lam, J.; Liu, M.; Wang, Z. Compliant Control and Compensation for A Compact Cable-Driven Robotic Manipulator. IEEE Robot. Autom. Lett. 2020, 5, 5417–5424. [Google Scholar] [CrossRef]
- Feng, Y.; Fan, J.; Tao, B.; Wang, S.; Mo, J.; Wu, Y.; Liang, Q.; Chen, X. An image-guided hybrid robot system for dental implant surgery. Int. J. Comput. Assist. Radiol. Surg. 2021, 17, 15–26. [Google Scholar] [CrossRef]
- Tao, B.; Feng, Y.; Fan, X.; Lan, K.; Lan, K.; Zhuang, M.; Wang, S.; Wang, F.; Chen, X.; Wu, Y. The accuracy of a novel image-guided hybrid robotic system for dental implant placement: An in vitro study. Int. J. Med. Robot. Comput. Assist. Surg. 2023, 19, e2452. [Google Scholar] [CrossRef]
- Hu, Y.; Li, J.; Chen, Y.; Wang, Q.; Chi, C.; Zhang, H.; Gao, Q.; Lan, Y.; Li, Z.; Mu, Z.; et al. Design and Control of a Highly Redundant Rigid-flexible Coupling Robot to Assist the COVID-19 Oropharyngeal-Swab Sampling. IEEE Robot. Autom. Lett. 2022, 7, 1856–1863. [Google Scholar] [CrossRef]
- Rosenberg, L. Virtual fixtures: Perceptual tools for telerobotic manipulation. In Proceedings of the 12th International Symposium on Robotics Research, Seattle, WA, USA, 18–22 September 1993; pp. 76–82. [Google Scholar]
- Abbott, J.; Marayong, P.; Okamura, A. Haptic virtual fixtures for robot-assisted manipulation. In Proceedings of the 12th International Symposium on Robotics Research, San Francisco, CA, USA, 12–15 October 2005; pp. 49–64. [Google Scholar]
- Abbott, J.; Okamura, A. Stable forbidden-region virtual fixtures for bilateral telemanipulation. J. Dyn. Syst. Meas. Control.-Trans. ASME 2006, 128, 53–64. [Google Scholar] [CrossRef]
- Bettini, A.; Marayong, P.; Lang, S.; Okamura, A.; Hager, G. Vision-assisted control for manipulation using virtual fixtures. IEEE Trans. Robot. Autom. 2004, 20, 953–966. [Google Scholar] [CrossRef]
- Abbott, J.; Okamura, A. Pseudo-admittance bilateral telemanipulation with guidance virtual fixtures. Int. J. Robot. Res. 2007, 26, 865–884. [Google Scholar] [CrossRef]
- Tang, A.; Cao, Q.; Pan, T. Spatial motion constraints for a minimally invasive surgical robot using customizable virtual fixtures. Int. J. Med. Robot. Comput. Assist. Surg. 2014, 10, 447–460. [Google Scholar] [CrossRef]
- Xu, C.; Lin, L.; Aung, Z.; Chai, G.; Xie, L. Research on spatial motion safety constraints and cooperative control of robot-assisted craniotomy: Beagle model experiment verification. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, 1–13. [Google Scholar] [CrossRef]
- Ren, J.; Patel, R.; McIsaac, K.; Guiraudon, G.; Peters, T. Dynamic 3-D virtual fixtures for minimally invasive beating heart procedures. IEEE Trans. Med. Imaging 2008, 27, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Yang, E.; McIsaac, K.; Patel, N.; Ebrahimi, A.; Shahbazi, M.; Gehlbach, P.; Iordachita, I. Automatic Light Pipe Actuating System for Bimanual Robot-Assisted Retinal Surgery. IEEE Trans. Mechatron. 2020, 25, 2846–2857. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Yu, X.; Chen, X.; Zhang, F. Laparoscope arm automatic positioning for robot-assisted surgery based on reinforcement learning. Mech. Sci. 2019, 10, 119–131. [Google Scholar] [CrossRef]
- Liang, K.; Xing, Y.; Li, J.; Wang, S.; Li, A.; Li, J. Motion control skill assessment based on kinematic analysis of robotic end-effector movements. Int. J. Med. Robot. Comput. Assist. Surg. 2018, 14, e1845. [Google Scholar] [CrossRef]
- Xing, Y.; Liang, K.; Wang, S.; Li, J.; Wang, X.; Li, A. Safety Oriented Evaluation (SOE) of Robot-assisted Minimally Invasive Surgery (MIS) Performance Skill. In Proceedings of the 2014 IEEE International Conference on Robotics and Biomimetics IEEE-ROBIO, Bali, Indonesia, 5–10 December 2014; pp. 619–624. [Google Scholar]
- Preda, S.; Ciobirca, C.; Gruionu, G.; Lacob, A.; Sapalidis, K.; Gruionu, L.; Castravete, S.; Patrascu, S.; Surlin, V. Preoperative Computer-Assisted Laparoscopy Planning for the Minimally Invasive Surgical Repair of Hiatal Hernia. Diagnostics 2020, 10, 621. [Google Scholar] [CrossRef]
- Badani, K.; Muhletaler, F.; Fumo, M.; Kaul, S.; Peabody, J.; Bhandari, M.; Menon, M. Optimizing robotic placement renal surgery: The lateral camera port technique and current results. J. Endourol. 2008, 22, 507–510. [Google Scholar] [CrossRef]
- Banez, J.; Caro, S.; Schwaitzberg, S.; Classe, J.; Cao, C. Modeling Patients for Optimized Port Placement in Robot-Assisted Surgery. In Proceedings of the ASME 11th Biennial Conference on Engineering Systems Design and Analysis, Nantes, France, 2–4 July 2012; pp. 821–826. [Google Scholar]
- Tian, C.P.; Xu, Z.Y.; Wang, L.K.; Liu, Y.J. Arc fault detection using artificial intelligence: Challenges and benefits. Math. Biosci. Eng. 2023, 20, 12404–12432. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Li, L.; Yang, J.; Wang, Y.X.; Hao, S.H. Center-based Transfer Feature Learning With Classifier Adaptation for surface defect recognition. Mech. Syst. Signal Process. 2023, 188, 110001. [Google Scholar] [CrossRef]
- Lin, C.; Zheng, Y.; Guang, C.H.; Ma, K.; Yang, Y. Precision forceps tracking and localisation using a Kalman filter for continuous curvilinear capsulorhexis. Int. J. Med. Robot. Comput. Assist. Surg. 2022, 18, e2432. [Google Scholar] [CrossRef] [PubMed]
- He, C.Y.; Patel, N.; Ebrahimi, A.; Kobilarov, M.; Iordachita, I. Preliminary study of an RNN-based active interventional robotic system (AIRS) in retinal microsurgery. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 945–954. [Google Scholar] [CrossRef]
- He, C.Y.; Patel, N.; Shahbazi, M.; Yang, Y.; Gehlbach, P.; Kobilarov, M.; Iordachita, I. Toward Safe Retinal Microsurgery: Development and Evaluation of an RNN-Based Active Interventional Control Framework. IEEE Trans. Biomed. Eng. 2020, 64, 966–977. [Google Scholar] [CrossRef]
- Lin, C.; Yang, Y.; Gao, H.D.; Zhang, Y.; Ma, K.; Guang, C.H. Evaluation of continuous curvilinear capsulorhexis based on a neural-network. Int. J. Comput. Assist. Radiol. Surg. 2023, 1–10. [Google Scholar] [CrossRef]
- Liu, Z.W.; Yang, D.; Wang, Y.J.; Lu, M.J.; Li, R.R. EGNN: Graph structure learning based on evolutionary computation helps more in graph neural networks. Appl. Soft Comput. 2023, 135, 110040. [Google Scholar] [CrossRef]
- Wang, Y.X.; Liu, Z.W.; Xu, J.D.; Yan, W.Q. Heterogeneous Network Representation Learning Approach for Ethereum Identity Identification. IEEE Trans. Comput. Soc. Syst. 2022, 10, 890–899. [Google Scholar] [CrossRef]
- Shi, Y.; Li, H.R.; Fu, X.P.; Luan, R.F.; Wang, Y.X.; Wang, N.; Sun, Z.B.; Niu, Y.X.; Wang, C.H.; Zhang, C.; et al. Self-powered difunctional sensors based on sliding contact-electrification and tribovoltaic effects for pneumatic monitoring and controlling. Nano Energy 2023, 110, 108339. [Google Scholar] [CrossRef]
- Haidegger, T. Autonomy for Surgical Robots: Concepts and Paradigms. IEEE Trans. Med. Robot. Bionics 2019, 1, 65–76. [Google Scholar] [CrossRef]
- Nagy, T.; Haidegger, T. Performance and Capability Assessment in Surgical Subtask Automation. Sensors 2022, 22, 2501. [Google Scholar] [CrossRef] [PubMed]





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Coverage (%) | Time (s) | N | Coverage (%) | Time (s) |
|---|---|---|---|---|---|
| 3 | 59.24 | 0.171 | 12 | 90.30 | 1.161 |
| 4 | 71.09 | 0.262 | 13 | 87.29 | 1.247 |
| 5 | 60.14 | 0.215 | 14 | 91.28 | 1.255 |
| 6 | 82.31 | 0.303 | 15 | 88.23 | 1.926 |
| 7 | 79.11 | 0.346 | 16 | 91.42 | 1.860 |
| 8 | 79.98 | 0.459 | 17 | 92.05 | 3.098 |
| 9 | 82.63 | 0.406 | 18 | 90.92 | 3.969 |
| 10 | 84.07 | 0.665 | 19 | 93.17 | 4.867 |
| 11 | 86.24 | 0.653 | 20 | 90.87 | 4.911 |
| Objective Function | ||
|---|---|---|
| Equation (14) | 65.500 | 0.000 |
| Equation (21) | 55.304 | 0.000 |
| Equation (22) | 81.000 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Wang, W.; Cai, Y.; Zhao, Q.; Wang, Y. Preoperative Planning Framework for Robot-Assisted Dental Implant Surgery: Finite-Parameter Surrogate Model and Optimization of Instrument Placement. Bioengineering 2023, 10, 952. https://doi.org/10.3390/bioengineering10080952
Wang Y, Wang W, Cai Y, Zhao Q, Wang Y. Preoperative Planning Framework for Robot-Assisted Dental Implant Surgery: Finite-Parameter Surrogate Model and Optimization of Instrument Placement. Bioengineering. 2023; 10(8):952. https://doi.org/10.3390/bioengineering10080952
Chicago/Turabian StyleWang, Yan, Wei Wang, Yueri Cai, Qiming Zhao, and Yuyang Wang. 2023. "Preoperative Planning Framework for Robot-Assisted Dental Implant Surgery: Finite-Parameter Surrogate Model and Optimization of Instrument Placement" Bioengineering 10, no. 8: 952. https://doi.org/10.3390/bioengineering10080952
APA StyleWang, Y., Wang, W., Cai, Y., Zhao, Q., & Wang, Y. (2023). Preoperative Planning Framework for Robot-Assisted Dental Implant Surgery: Finite-Parameter Surrogate Model and Optimization of Instrument Placement. Bioengineering, 10(8), 952. https://doi.org/10.3390/bioengineering10080952