

Effects of rTMS Intervention on Functional Neuroimaging Activities in Adolescents with Major Depressive Disorder Measured Using Resting-State fMRI
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. rTMS Procedure
2.3. Clinical Assessment
2.4. fMRI Data Acquisition
2.5. fMRI Data Preprocessing
2.6. ReHo and ALFF Calculation
2.7. sgACC-Based Whole-Brain FC Analysis
2.8. Statistical Analysis
3. Results
3.1. Demographic and Clinical Outcomes
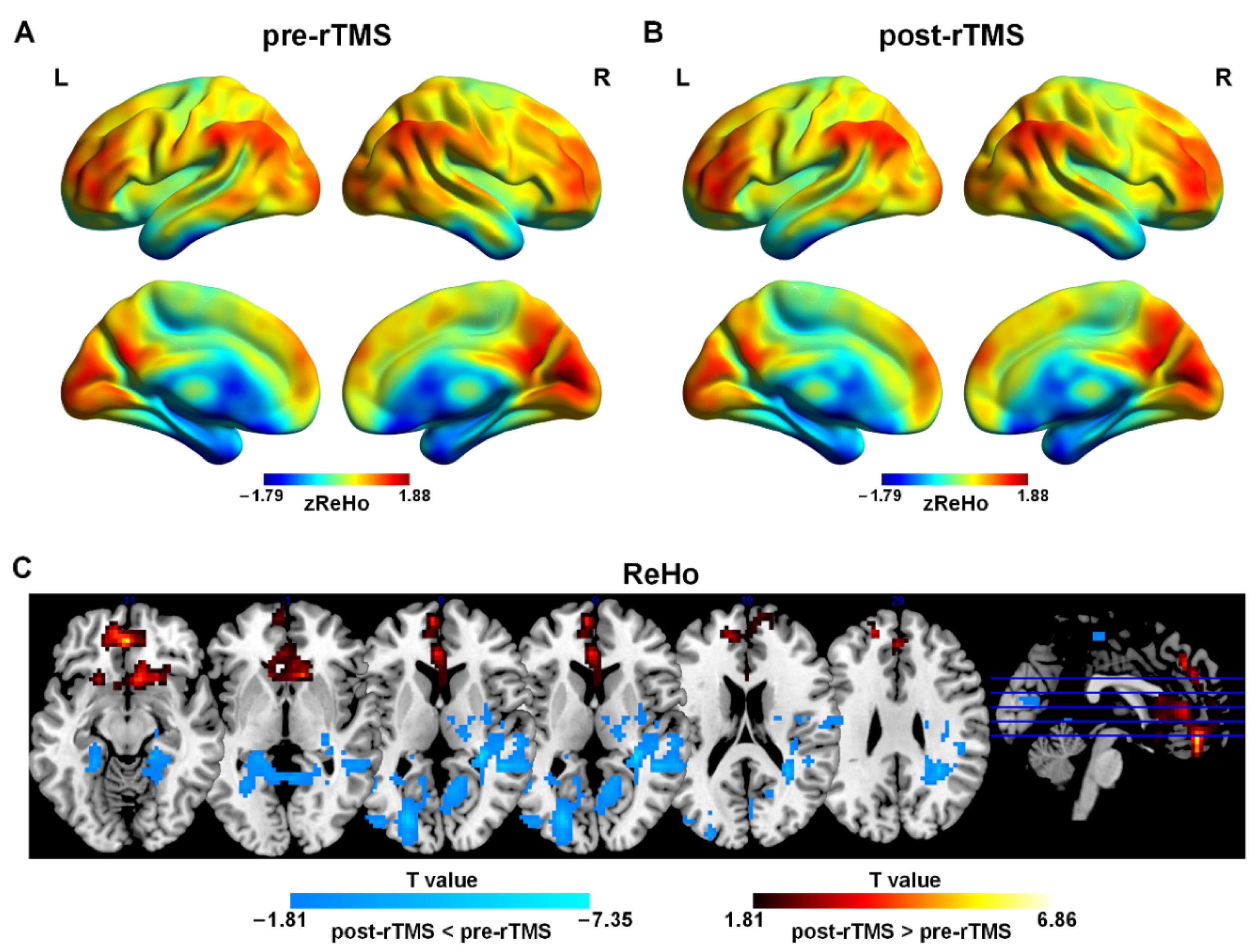
3.2. rTMS-Induced ReHo Changes between Pre-rTMS and Post-rTMS
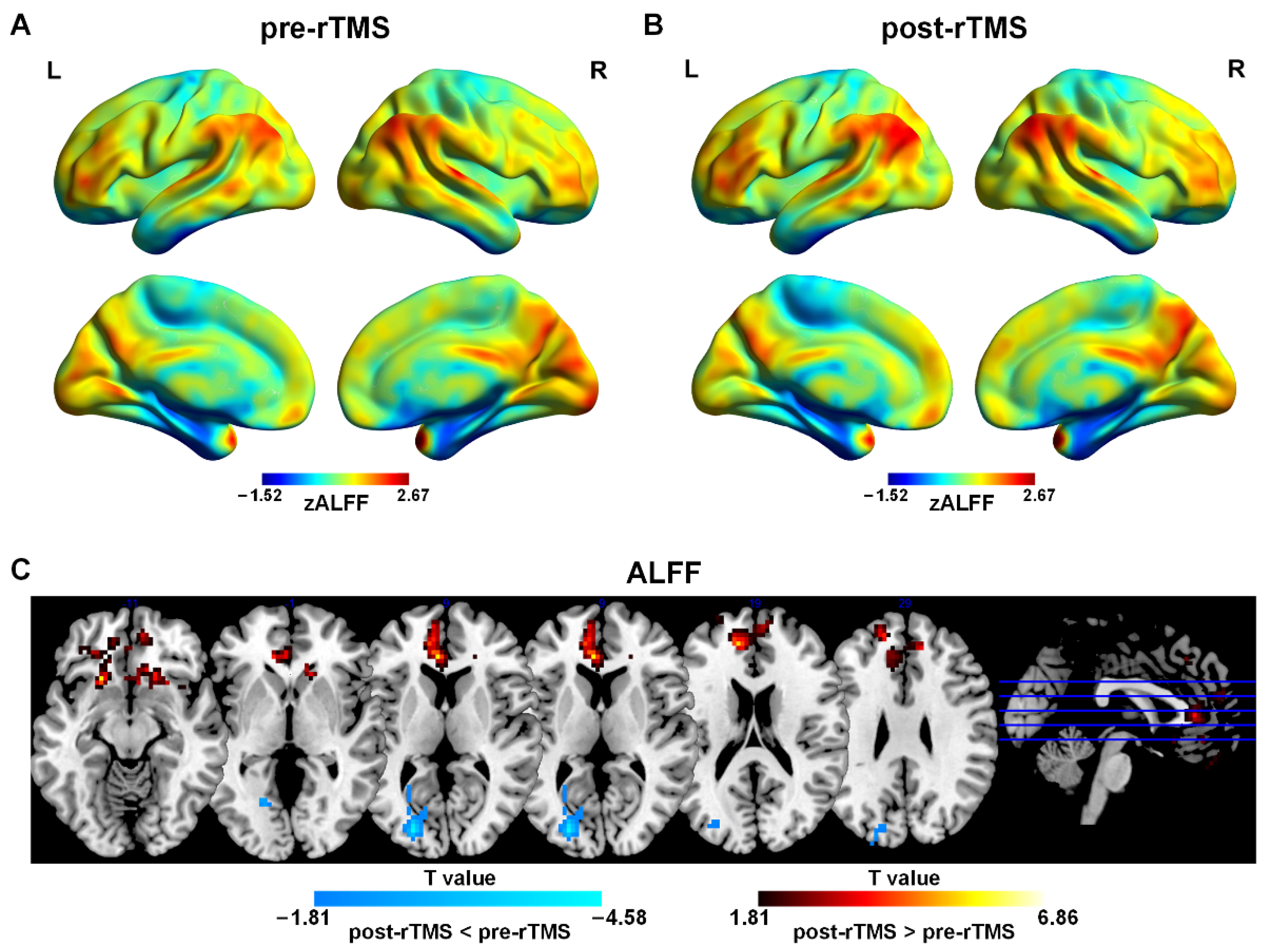
3.3. rTMS-Induced ALFF Changes between Pre-rTMS and Post-rTMS
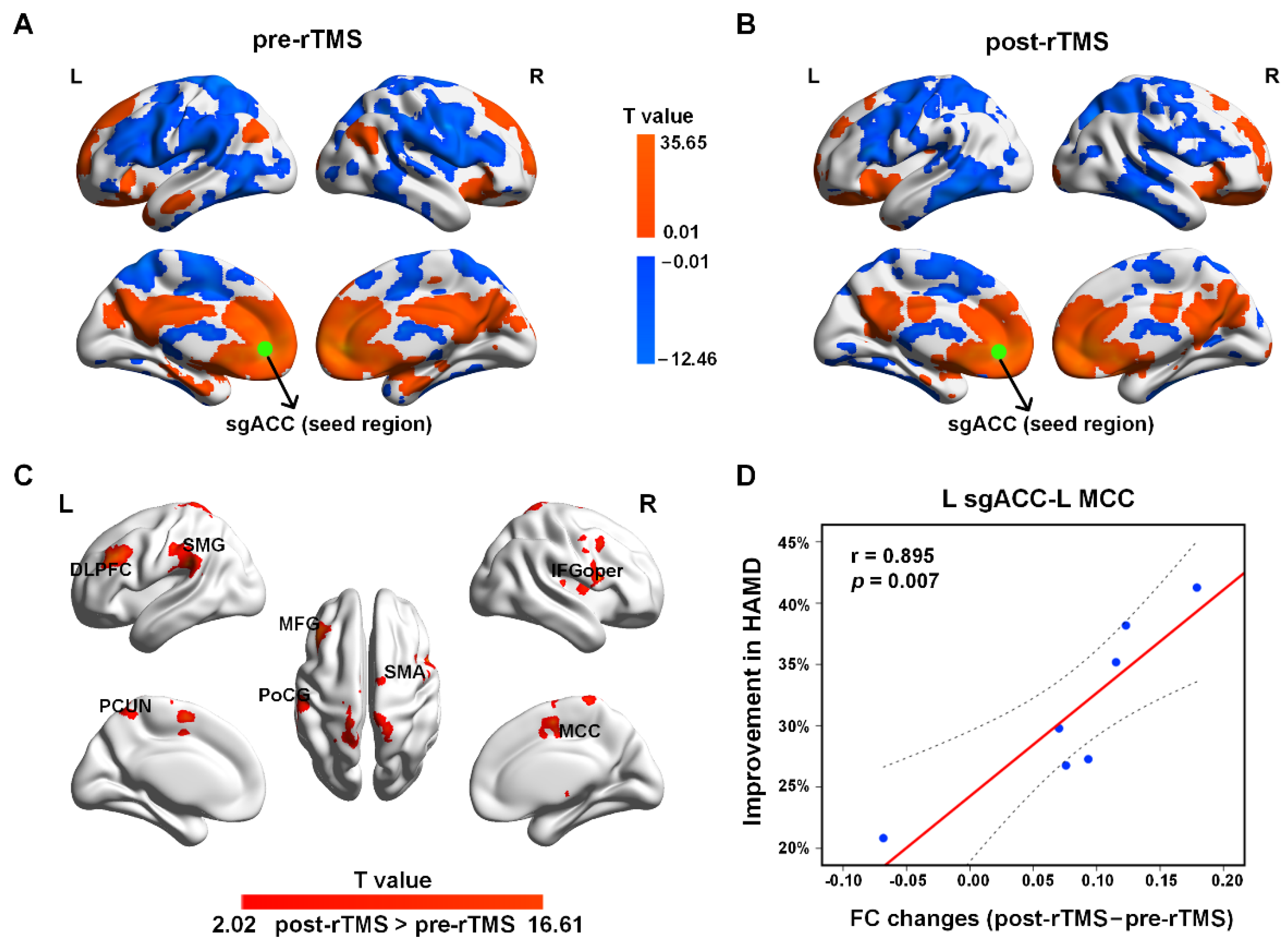
3.4. rTMS-Induced FC Changes between Pre-rTMS and Post-rTMS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, Y.; Wang, Y.; Wang, H.; Liu, Z.; Yu, X.; Yan, J.; Yu, Y.; Kou, C.; Xu, X.; Lu, J.; et al. Prevalence of mental disorders in China: A cross-sectional epidemiological study. Lancet Psychiatry 2019, 6, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Cui, Q.; Chen, Y.; He, Z.; Sheng, W.; Tang, Q.; Yang, Y.; Luo, W.; Yu, Y.; Chen, J. Insular-associated causal network of structural covariance evaluating progressive gray matter changes in major depressive disorder. Cereb. Cortex 2023, 33, 831–843. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Chen, Y.; Cui, Q.; Guo, Y.; Pang, Y.; Luo, W.; Yu, Y.; Chen, J.; Gao, J.; Sheng, W.; et al. Shared and distinct patterns of dynamic functional connectivity variability of thalamo-cortical circuit in bipolar depression and major depressive disorder. Cereb. Cortex 2023, 33, 6681–6692. [Google Scholar] [CrossRef] [PubMed]
- Thapar, A.; Collishaw, S.; Pine, D.S.; Thapar, A.K. Depression in adolescence. Lancet 2012, 379, 1056–1067. [Google Scholar] [CrossRef] [PubMed]
- Avenevoli, S.; Swendsen, J.; He, J.P.; Burstein, M.; Merikangas, K.R. Major depression in the national comorbidity survey-adolescent supplement: Prevalence, correlates, and treatment. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 37–44.e32. [Google Scholar] [CrossRef] [PubMed]
- March, J.S.; Silva, S.; Petrycki, S.; Curry, J.; Wells, K.; Fairbank, J.; Burns, B.; Domino, M.; McNulty, S.; Vitiello, B.; et al. The Treatment for Adolescents With Depression Study (TADS): Long-term effectiveness and safety outcomes. Arch. Gen. Psychiatry 2007, 64, 1132–1143. [Google Scholar] [PubMed]
- March, J.; Silva, S.; Curry, J.; Wells, K.; Fairbank, J.; Burns, B.; Domino, M.; Vitiello, B.; Severe, J.; Riedal, K.; et al. The Treatment for Adolescents With Depression Study (TADS): Outcomes over 1 year of naturalistic follow-up. Am. J. Psychiatry 2009, 166, 1141–1149. [Google Scholar] [CrossRef]
- Hetrick, S.E.; McKenzie, J.E.; Bailey, A.P.; Sharma, V.; Moller, C.I.; Badcock, P.B.; Cox, G.R.; Merry, S.N.; Meader, N. New generation antidepressants for depression in children and adolescents: A network meta-analysis. Cochrane Database Syst. Rev. 2021, 5, Cd013674. [Google Scholar]
- Feeney, A.; Hock, R.S.; Fava, M.; Hernández Ortiz, J.M.; Iovieno, N.; Papakostas, G.I. Antidepressants in children and adolescents with major depressive disorder and the influence of placebo response: A meta-analysis. J. Affect. Disord. 2022, 305, 55–64. [Google Scholar] [CrossRef]
- Reeves, R.R.; Ladner, M.E. Antidepressant-induced suicidality: An update. CNS Neurosci. Ther. 2010, 16, 227–234. [Google Scholar] [CrossRef]
- Umetsu, R.; Abe, J.; Ueda, N.; Kato, Y.; Matsui, T.; Nakayama, Y.; Kinosada, Y.; Nakamura, M. Association between Selective Serotonin Reuptake Inhibitor Therapy and Suicidality: Analysis of U.S. Food and Drug Administration Adverse Event Reporting System Data. Biol. Pharm. Bull. 2015, 38, 1689–1699. [Google Scholar] [CrossRef] [PubMed]
- Baeken, C.; Brem, A.-K.; Arns, M.; Brunoni, A.R.; Filipčić, I.; Ganho-Ávila, A.; Langguth, B.; Padberg, F.; Poulet, E.; Rachid, F. Repetitive transcranial magnetic stimulation treatment for depressive disorders: Current knowledge and future directions. Curr. Opin. Psychiatry 2019, 32, 409. [Google Scholar] [CrossRef] [PubMed]
- Ontario, H.Q. Repetitive transcranial magnetic stimulation for treatment-resistant depression: A systematic review and meta-analysis of randomized controlled trials. Ont. Health Technol. Assess. Ser. 2016, 16, 1. [Google Scholar]
- Lefaucheur, J.-P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef] [PubMed]
- Croarkin, P.E.; MacMaster, F.P. Transcranial Magnetic Stimulation for Adolescent Depression. Child Adolesc. Psychiatr. Clin. N. Am. 2019, 28, 33–43. [Google Scholar] [CrossRef]
- Dunner, D.L.; Aaronson, S.T.; Sackeim, H.A.; Janicak, P.G.; Carpenter, L.L.; Boyadjis, T.; Brock, D.G.; Bonneh-Barkay, D.; Cook, I.A.; Lanocha, K.; et al. A multisite, naturalistic, observational study of transcranial magnetic stimulation for patients with pharmacoresistant major depressive disorder: Durability of benefit over a 1-year follow-up period. J. Clin. Psychiatry 2014, 75, 1394–1401. [Google Scholar] [CrossRef] [PubMed]
- Schutter, D.J. Antidepressant efficacy of high-frequency transcranial magnetic stimulation over the left dorsolateral prefrontal cortex in double-blind sham-controlled designs: A meta-analysis. Psychol. Med. 2009, 39, 65–75. [Google Scholar] [CrossRef]
- Slotema, C.W.; Blom, J.D.; Hoek, H.W.; Sommer, I.E. Should we expand the toolbox of psychiatric treatment methods to include Repetitive Transcranial Magnetic Stimulation (rTMS)? A meta-analysis of the efficacy of rTMS in psychiatric disorders. J. Clin. Psychiatry 2010, 71, 873–884. [Google Scholar] [CrossRef]
- Biswal, B.; Yetkin, F.Z.; Haughton, V.M.; Hyde, J.S. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn. Reson. Med. 1995, 34, 537–541. [Google Scholar] [CrossRef]
- Canario, E.; Chen, D.; Biswal, B. A review of resting-state fMRI and its use to examine psychiatric disorders. Psychoradiology 2021, 1, 42–53. [Google Scholar] [CrossRef]
- Phillips, M.L.; Chase, H.W.; Sheline, Y.I.; Etkin, A.; Almeida, J.R.; Deckersbach, T.; Trivedi, M.H. Identifying predictors, moderators, and mediators of antidepressant response in major depressive disorder: Neuroimaging approaches. Am. J. Psychiatry 2015, 172, 124–138. [Google Scholar] [CrossRef] [PubMed]
- Zang, Y.; Jiang, T.; Lu, Y.; He, Y.; Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage 2004, 22, 394–400. [Google Scholar] [CrossRef]
- Liu, F.; Guo, W.; Liu, L.; Long, Z.; Ma, C.; Xue, Z.; Wang, Y.; Li, J.; Hu, M.; Zhang, J. Abnormal amplitude low-frequency oscillations in medication-naive, first-episode patients with major depressive disorder: A resting-state fMRI study. J. Affect. Disord. 2013, 146, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.D.; Buckner, R.L.; White, M.P.; Greicius, M.D.; Pascual-Leone, A. Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biol. Psychiatry 2012, 72, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Weigand, A.; Horn, A.; Caballero, R.; Cooke, D.; Stern, A.P.; Taylor, S.F.; Press, D.; Pascual-Leone, A.; Fox, M.D. Prospective Validation that Subgenual Connectivity Predicts Antidepressant Efficacy of Transcranial Magnetic Stimulation Sites. Biol. Psychiatry 2018, 84, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Cash, R.F.H.; Zalesky, A.; Thomson, R.H.; Tian, Y.; Cocchi, L.; Fitzgerald, P.B. Subgenual Functional Connectivity Predicts Antidepressant Treatment Response to Transcranial Magnetic Stimulation: Independent Validation and Evaluation of Personalization. Biol. Psychiatry 2019, 86, e5–e7. [Google Scholar] [CrossRef] [PubMed]
- Ge, R.; Downar, J.; Blumberger, D.M.; Daskalakis, Z.J.; Vila-Rodriguez, F. Functional connectivity of the anterior cingulate cortex predicts treatment outcome for rTMS in treatment-resistant depression at 3-month follow-up. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2020, 13, 206–214. [Google Scholar] [CrossRef]
- Drevets, W.C.; Savitz, J.; Trimble, M. The subgenual anterior cingulate cortex in mood disorders. CNS Spectr. 2008, 13, 663–681. [Google Scholar] [CrossRef]
- Mayberg, H.S.; Lozano, A.M.; Voon, V.; McNeely, H.E.; Seminowicz, D.; Hamani, C.; Schwalb, J.M.; Kennedy, S.H. Deep brain stimulation for treatment-resistant depression. Neuron 2005, 45, 651–660. [Google Scholar] [CrossRef]
- Georgiev, D.; Akram, H.; Jahanshahi, M. Deep brain stimulation for psychiatric disorders: Role of imaging in identifying/confirming DBS targets, predicting, and optimizing outcome and unravelling mechanisms of action. Psychoradiology. 2021, 1, 118–151. [Google Scholar] [CrossRef]
- Mi, Y.; Ji, Y.; Lou, Z.; Hou, Y.; Ruan, L. Left intermittent theta burst stimulation combined with right low-frequency rTMS as an additional treatment for major depression: A retrospective study. Indian J. Psychiatry 2022, 64, 364–369. [Google Scholar] [PubMed]
- Zheng, A.; Yu, R.; Du, W.; Liu, H.; Zhang, Z.; Xu, Z.; Xiang, Y.; Du, L. Two-week rTMS-induced neuroimaging changes measured with fMRI in depression. J. Affect. Disord. 2020, 270, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Liu, H.; Du, W.; Chao, F.; Zhang, L.; Wang, K.; Huang, C.; Gao, Y.; Tang, Y. Stimulated left DLPFC-nucleus accumbens functional connectivity predicts the anti-depression and anti-anxiety effects of rTMS for depression. Transl. Psychiatry 2018, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A.; Avanzini, G.; Bestmann, S.; Berardelli, A.; Brewer, C.; Canli, T.; Cantello, R.; et al. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef] [PubMed]
- Croarkin, P.E.; Elmaadawi, A.Z.; Aaronson, S.T.; Schrodt, G.R., Jr.; Holbert, R.C.; Verdoliva, S.; Heart, K.L.; Demitrack, M.A.; Strawn, J.R. Left prefrontal transcranial magnetic stimulation for treatment-resistant depression in adolescents: A double-blind, randomized, sham-controlled trial. Neuropsychopharmacology 2021, 46, 462–469. [Google Scholar] [CrossRef] [PubMed]
- O’Reardon, J.P.; Solvason, H.B.; Janicak, P.G.; Sampson, S.; Isenberg, K.E.; Nahas, Z.; McDonald, W.M.; Avery, D.; Fitzgerald, P.B.; Loo, C.; et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: A multisite randomized controlled trial. Biol. Psychiatry 2007, 62, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Croarkin, P.E.; Nakonezny, P.A.; Deng, Z.D.; Romanowicz, M.; Voort, J.L.V.; Camsari, D.D.; Schak, K.M.; Port, J.D.; Lewis, C.P. High-frequency repetitive TMS for suicidal ideation in adolescents with depression. J. Affect. Disord. 2018, 239, 282–290. [Google Scholar] [CrossRef]
- Zhao, Y.; He, Z.; Luo, W.; Yu, Y.; Chen, J.; Cai, X.; Gao, J.; Li, L.; Gao, Q.; Chen, H.; et al. Effect of intermittent theta burst stimulation on suicidal ideation and depressive symptoms in adolescent depression with suicide attempt: A randomized sham-controlled study. J. Affect. Disord. 2023, 325, 618–626. [Google Scholar] [CrossRef]
- Hamilton, M. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Lu, F.; Wang, M.; Xu, S.; Chen, H.; Yuan, Z.; Luo, L.; Wang, X.; Zhang, J.; Dai, J.; Wang, X. Decreased interhemispheric resting-state functional connectivity in male adolescents with conduct disorder. Brain Imaging Behav. 2021, 15, 1201–1210. [Google Scholar] [CrossRef]
- Lu, F.; Cui, Q.; Huang, X.; Li, L.; Duan, X.; Chen, H.; Pang, Y.; He, Z.; Sheng, W.; Han, S. Anomalous intrinsic connectivity within and between visual and auditory networks in major depressive disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 100, 109889. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.M.; Zhou, J.S.; Wang, X.P.; Xiang, Y.T.; Yuan, Z. Short- and long-range functional connectivity density alterations in adolescents with pure conduct disorder at resting-state. Neuroscience 2017, 351, 96–107. [Google Scholar] [CrossRef]
- Lu, F.; Liu, P.; Chen, H.; Wang, M.; Xu, S.; Yuan, Z.; Wang, X.; Wang, S.; Zhou, J. More than just statics: Abnormal dynamic amplitude of low-frequency fluctuation in adolescent patients with pure conduct disorder. J. Psychiatr. Res. 2020, 131, 60–68. [Google Scholar] [CrossRef]
- Lu, F.; Guo, Y.; Luo, W.; Yu, Y.; Zhao, Y.; Ni, S.; Chen, J.; Cai, X.; Shen, C.; Wang, X.; et al. Disrupted functional networks within white-matter served as neural features in adolescent patients with conduct disorder. Behav. Brain Res. 2023, 447, 114422. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Guo, W.; Fouche, J.-P.; Wang, Y.; Wang, W.; Ding, J.; Zeng, L.; Qiu, C.; Gong, Q.; Zhang, W. Multivariate classification of social anxiety disorder using whole brain functional connectivity. Brain Struct. Funct. 2015, 220, 101–115. [Google Scholar] [CrossRef]
- Liu, F.; Wang, Y.; Li, M.; Wang, W.; Li, R.; Zhang, Z.; Lu, G.; Chen, H. Dynamic functional network connectivity in idiopathic generalized epilepsy with generalized tonic-clonic seizure. Hum. Brain Mapp. 2017, 38, 957–973. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Liu, C.-H.; Lu, S.-L.; Tang, L.-R.; Tie, C.-L.; Zhang, J.; Yuan, Z. Disrupted Topology of Frontostriatal Circuits Is Linked to the Severity of Insomnia. Front. Neurosci. 2017, 11, 214. [Google Scholar] [CrossRef]
- Zhang, J.; Xu, D.; Cui, H.; Zhao, T.; Chu, C.; Wang, J. Group-guided individual functional parcellation of the hippocampus and application to normal aging. Hum. Brain Mapp. 2021, 42, 5973–5984. [Google Scholar] [CrossRef]
- Yan, C.-G.; Wang, X.-D.; Zuo, X.-N.; Zang, Y.-F. DPABI: Data processing & analysis for (resting-state) brain imaging. Neuroinformatics 2016, 14, 339–351. [Google Scholar]
- Sheline, Y.I.; Price, J.L.; Yan, Z.; Mintun, M.A. Resting-state functional MRI in depression unmasks increased connectivity between networks via the dorsal nexus. Proc. Natl. Acad. Sci. USA 2010, 107, 11020–11025. [Google Scholar] [CrossRef]
- Chao-Gan, Y.; Yu-Feng, Z. DPARSF: A MATLAB Toolbox for “Pipeline” Data Analysis of Resting-State fMRI. Front. Syst. Neurosci. 2010, 4, 13. [Google Scholar] [PubMed]
- Zald, D.; Kim, S.; Salloway, S.; Malloy, P.; Duffy, J. The Frontal Lobes and Neuropsychiatric Illness; American Psychiatric Pub: Washington, DC, USA, 2011; pp. 33–69. [Google Scholar]
- Drevets, W.C. Orbitofrontal cortex function and structure in depression. Ann. N. Y. Acad. Sci. 2007, 1121, 499–527. [Google Scholar] [CrossRef] [PubMed]
- Pizzagalli, D.A.; Roberts, A.C. Prefrontal cortex and depression. Neuropsychopharmacology 2022, 47, 225–246. [Google Scholar] [CrossRef]
- Zhou, X.T.; Bao, W.D.; Liu, D.; Zhu, L.Q. Targeting the Neuronal Activity of Prefrontal Cortex: New Directions for the Therapy of Depression. Curr. Neuropharmacol. 2020, 18, 332–346. [Google Scholar] [CrossRef]
- Yao, Z.; Wang, L.; Lu, Q.; Liu, H.; Teng, G. Regional homogeneity in depression and its relationship with separate depressive symptom clusters: A resting-state fMRI study. J. Affect. Disord. 2009, 115, 430–438. [Google Scholar] [CrossRef]
- Drevets, W.C. Neuroimaging and neuropathological studies of depression: Implications for the cognitive-emotional features of mood disorders. Curr. Opin. Neurobiol. 2001, 11, 240–249. [Google Scholar] [CrossRef]
- Beevers, C.G.; Clasen, P.; Stice, E.; Schnyer, D. Depression symptoms and cognitive control of emotion cues: A functional magnetic resonance imaging study. Neuroscience 2010, 167, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Chen, X.; Chen, J.; Ai, M.; Gan, Y.; Wang, W.; Lv, Z.; Zhang, S.; Wang, S.; Kuang, L.; et al. Resting-state functional MRI of abnormal baseline brain activity in young depressed patients with and without suicidal behavior. J. Affect. Disord. 2016, 205, 252–263. [Google Scholar] [CrossRef]
- Palomero-Gallagher, N.; Eickhoff, S.B.; Hoffstaedter, F.; Schleicher, A.; Mohlberg, H.; Vogt, B.A.; Amunts, K.; Zilles, K. Functional organization of human subgenual cortical areas: Relationship between architectonical segregation and connectional heterogeneity. Neuroimage 2015, 115, 177–190. [Google Scholar] [CrossRef]
- Beckmann, M.; Johansen-Berg, H.; Rushworth, M.F. Connectivity-based parcellation of human cingulate cortex and its relation to functional specialization. J. Neurosci. 2009, 29, 1175–1190. [Google Scholar] [CrossRef]
- Haber, S.N.; Behrens, T.E. The neural network underlying incentive-based learning: Implications for interpreting circuit disruptions in psychiatric disorders. Neuron 2014, 83, 1019–1039. [Google Scholar] [CrossRef] [PubMed]
- Botvinick, M.M.; Cohen, J.D.; Carter, C.S. Conflict monitoring and anterior cingulate cortex: An update. Trends Cogn. Sci. 2004, 8, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Klomjai, W.; Katz, R.; Lackmy-Vallée, A. Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS). Ann. Phys. Rehabil. Med. 2015, 58, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Pizzagalli, D.A. Frontocingulate dysfunction in depression: Toward biomarkers of treatment response. Neuropsychopharmacology 2011, 36, 183–206. [Google Scholar] [CrossRef] [PubMed]
- Drysdale, A.T.; Grosenick, L.; Downar, J.; Dunlop, K.; Mansouri, F.; Meng, Y.; Fetcho, R.N.; Zebley, B.; Oathes, D.J.; Etkin, A.; et al. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat. Med. 2017, 23, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Mayberg, H.S.; Riva-Posse, P.; Crowell, A.L. Deep Brain Stimulation for Depression: Keeping an Eye on a Moving Target. JAMA Psychiatry 2016, 73, 439–440. [Google Scholar] [CrossRef]
- McGrath, C.L.; Kelley, M.E.; Holtzheimer, P.E.; Dunlop, B.W.; Craighead, W.E.; Franco, A.R.; Craddock, R.C.; Mayberg, H.S. Toward a neuroimaging treatment selection biomarker for major depressive disorder. JAMA Psychiatry 2013, 70, 821–829. [Google Scholar] [CrossRef]
- Cullen, K.R.; Gee, D.G.; Klimes-Dougan, B.; Gabbay, V.; Hulvershorn, L.; Mueller, B.A.; Camchong, J.; Bell, C.J.; Houri, A.; Kumra, S.; et al. A preliminary study of functional connectivity in comorbid adolescent depression. Neurosci. Lett. 2009, 460, 227–231. [Google Scholar] [CrossRef]
- Davey, C.G.; Harrison, B.J.; Yücel, M.; Allen, N.B. Regionally specific alterations in functional connectivity of the anterior cingulate cortex in major depressive disorder. Psychol Med. 2012, 42, 2071–2081. [Google Scholar] [CrossRef]
- Connolly, C.G.; Wu, J.; Ho, T.C.; Hoeft, F.; Wolkowitz, O.; Eisendrath, S.; Frank, G.; Hendren, R.; Max, J.E.; Paulus, M.P.; et al. Resting-state functional connectivity of subgenual anterior cingulate cortex in depressed adolescents. Biol. Psychiatry 2013, 74, 898–907. [Google Scholar] [CrossRef]
- Greicius, M.D.; Flores, B.H.; Menon, V.; Glover, G.H.; Solvason, H.B.; Kenna, H.; Reiss, A.L.; Schatzberg, A.F. Resting-state functional connectivity in major depression: Abnormally increased contributions from subgenual cingulate cortex and thalamus. Biol. Psychiatry 2007, 62, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Apps, M.A.; Lockwood, P.L.; Balsters, J.H. The role of the midcingulate cortex in monitoring others’ decisions. Front. Neurosci. 2013, 7, 251. [Google Scholar] [CrossRef] [PubMed]
- Shackman, A.J.; Salomons, T.V.; Slagter, H.A.; Fox, A.S.; Winter, J.J.; Davidson, R.J. The integration of negative affect, pain and cognitive control in the cingulate cortex. Nat. Rev. Neurosci. 2011, 12, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions’ of DSM-IV disorders in the national comorbidity survey replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Kornstein, S.G.; Schatzberg, A.F.; Thase, M.E.; Yonkers, K.A.; McCullough, J.P.; Keitner, G.I.; Gelenberg, A.J.; Ryan, C.E.; Hess, A.L.; Harrison, W.; et al. Gender differences in chronic major and double depression. J. Affect. Disord. 2000, 60, 1–11. [Google Scholar] [CrossRef]
- Wu, W.; Zhang, Y.; Jiang, J.; Lucas, M.V.; Fonzo, G.A.; Rolle, C.E.; Cooper, C.; Chin-Fatt, C.; Krepel, N.; Cornelssen, C.A.; et al. An electroencephalographic signature predicts antidepressant response in major depression. Nat. Biotechnol. 2020, 38, 439–447. [Google Scholar] [CrossRef]
- Zhang, Y.; Wu, W.; Toll, R.T.; Naparstek, S.; Maron-Katz, A.; Watts, M.; Gordon, J.; Jeong, J.; Astolfi, L.; Shpigel, E.; et al. Identification of psychiatric disorder subtypes from functional connectivity patterns in resting-state electroencephalography. Nat. Biomed. Eng. 2021, 5, 309–323. [Google Scholar] [CrossRef]
- Goldstein-Piekarski, A.N.; Staveland, B.R.; Ball, T.M.; Yesavage, J.; Korgaonkar, M.S.; Williams, L.M. Intrinsic functional connectivity predicts remission on antidepressants: A randomized controlled trial to identify clinically applicable imaging biomarkers. Transl. Psychiatry 2018, 8, 57. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | pre-rTMS (n = 11) | post-rTMS (n = 11) | t/F | p |
|---|---|---|---|---|
| Age (years) | 16.18 ± 2.36 | 16.18 ± 2.36 | ||
| Education (years) | 10.05 ± 2.39 | 10.05 ± 2.39 | ||
| Gender (M:F) | 1:10 | 1:10 | ||
| Age of first onset (years) | 13.73 ± 1.95 | 13.73 ± 1.95 | ||
| Number of depressive episodes | 1.64 ± 1.21 | 1.64 ± 1.21 | ||
| Duration of single depressive episode (months) | 10.82 ± 9.53 | 10.82 ± 9.53 | ||
| Mean FD (mm) | 0.09 ± 0.03 | 0.08 ± 0.04 | 0.78 | 0.453 * |
| HAMD score | 51.55 ± 16.59 | 36.73 ± 11.31 | 26.04 | <0.001 # |
| HAMA score | 31.09 ± 9.76 | 21.55 ± 5.35 | 24.17 | 0.001 # |
| Brain Region | MNI Coordinates | Cluster Size | T-Value | ||
|---|---|---|---|---|---|
| x | y | z | (Voxels) | ||
| ReHo | |||||
| post-rTMS > pre-rTMS | |||||
| Rectus_L | −3 | 45 | −15 | 84 | 6.86 |
| mPFC_L | −3 | 36 | 39 | 167 | 5.21 |
| mOFC_L | −3 | 45 | −12 | 96 | 5.03 |
| mOFC_R | 9 | 42 | −6 | 77 | 3.61 |
| ACC_L | −3 | 36 | 6 | 103 | 3.81 |
| post-rTMS < pre-rTMS | |||||
| MOG_L | −24 | −81 | 12 | 161 | −4.54 |
| CUN_L | −21 | −78 | 12 | 150 | −7.35 |
| MCC_R | 21 | −15 | 63 | 94 | −4.42 |
| CAL_L | −18 | −75 | 12 | 114 | −3.69 |
| CAL_R | 9 | −60 | 9 | 126 | −3.45 |
| ALFF | |||||
| post-rTMS > pre-rTMS | |||||
| mPFC_L | −12 | 45 | 15 | 150 | 6.86 |
| DLPFC_L | −15 | 51 | 27 | 82 | 5.75 |
| ACC_L | −9 | 45 | 15 | 118 | 4.64 |
| post-rTMS < pre-rTMS | |||||
| MOG_L | −21 | −81 | 12 | 140 | −4.58 |
| SOG_L | −21 | −87 | 27 | 66 | −2.22 |
| Brain Region | MNI Coordinates | Cluster Size | T-Value | ||
|---|---|---|---|---|---|
| x | y | z | (Voxels) | ||
| post-rTMS > pre-rTMS | |||||
| DLPFC_L | −46 | 38 | 30 | 172 | 10.31 |
| IFGoper_R | 51 | 9 | 27 | 75 | 6.48 |
| MCC_L | −3 | −3 | 45 | 44 | 16.61 |
| MFG_R | 45 | 12 | 42 | 59 | 5.38 |
| PCUN_L | −15 | −57 | 60 | 105 | 3.23 |
| PoCG_L | −18 | −42 | 75 | 67 | 4.04 |
| PoCG_R | 36 | −24 | 45 | 54 | 3.47 |
| SMA_L | −9 | −12 | 78 | 105 | 6.6 |
| SMG_L | −51 | −36 | 27 | 229 | 13.86 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, F.; Cui, Q.; Zou, Y.; Guo, Y.; Luo, W.; Yu, Y.; Gao, J.; Cai, X.; Fu, L.; Yuan, S.; et al. Effects of rTMS Intervention on Functional Neuroimaging Activities in Adolescents with Major Depressive Disorder Measured Using Resting-State fMRI. Bioengineering 2023, 10, 1374. https://doi.org/10.3390/bioengineering10121374
Lu F, Cui Q, Zou Y, Guo Y, Luo W, Yu Y, Gao J, Cai X, Fu L, Yuan S, et al. Effects of rTMS Intervention on Functional Neuroimaging Activities in Adolescents with Major Depressive Disorder Measured Using Resting-State fMRI. Bioengineering. 2023; 10(12):1374. https://doi.org/10.3390/bioengineering10121374
Chicago/Turabian StyleLu, Fengmei, Qian Cui, Yang Zou, Yuanhong Guo, Wei Luo, Yue Yu, Jingjing Gao, Xiao Cai, Linna Fu, Shuai Yuan, and et al. 2023. "Effects of rTMS Intervention on Functional Neuroimaging Activities in Adolescents with Major Depressive Disorder Measured Using Resting-State fMRI" Bioengineering 10, no. 12: 1374. https://doi.org/10.3390/bioengineering10121374
APA StyleLu, F., Cui, Q., Zou, Y., Guo, Y., Luo, W., Yu, Y., Gao, J., Cai, X., Fu, L., Yuan, S., Huang, J., Zhang, Y., Xie, J., Sheng, W., Tang, Q., Gao, Q., He, Z., & Chen, H. (2023). Effects of rTMS Intervention on Functional Neuroimaging Activities in Adolescents with Major Depressive Disorder Measured Using Resting-State fMRI. Bioengineering, 10(12), 1374. https://doi.org/10.3390/bioengineering10121374