

Optimizing Spinal Fusion Cage Design to Improve Bone Substitute Filling on Varying Disc Heights: A 3D Printing Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
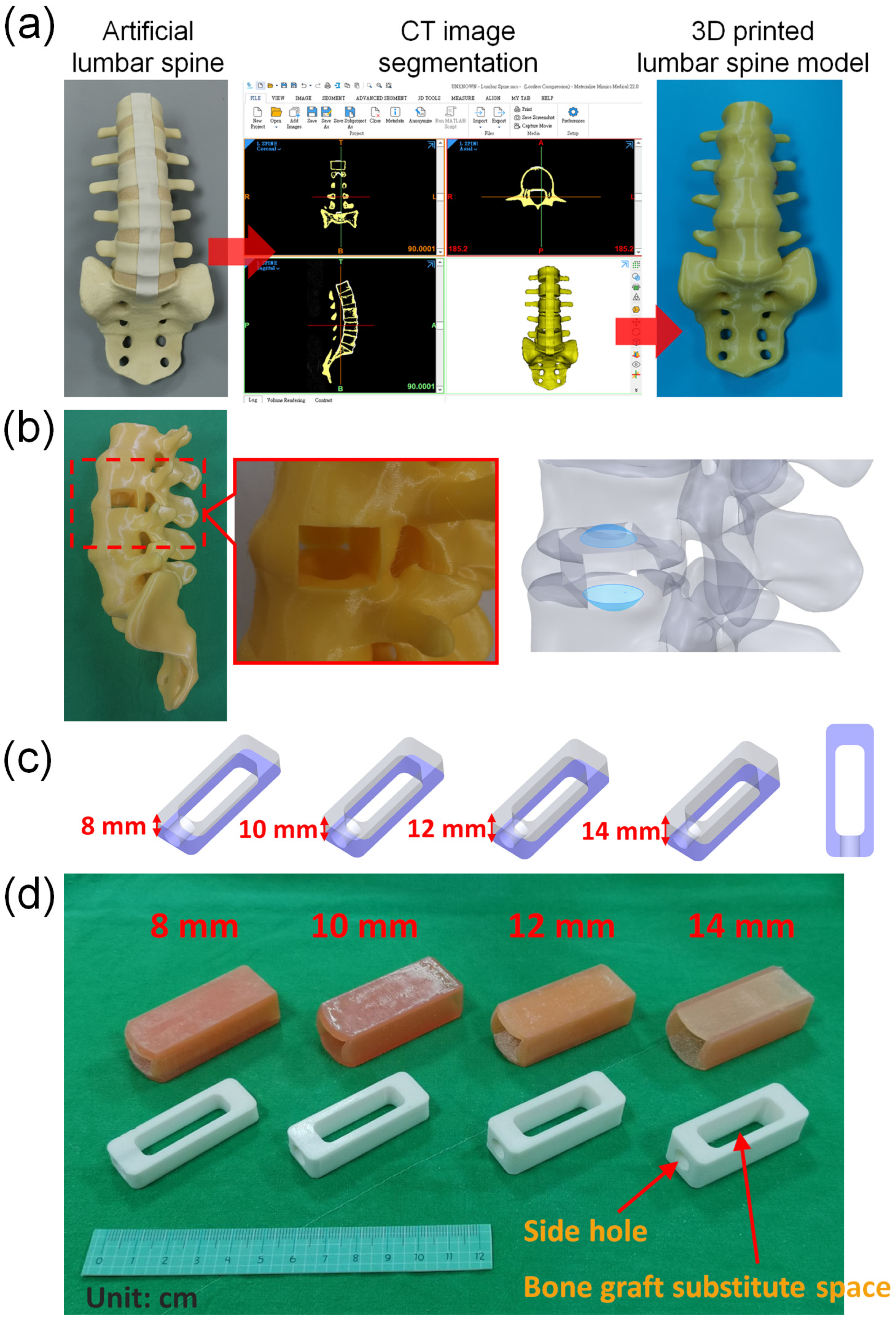
2.1. Model of Spine
2.2. Model of Cage
2.3. Model of Disc
2.4. Preparation of Bone Substitute
2.5. Experimental Methods
- A model with an internal volume of one cubic centimeter was created and weighed using a high-precision balance. The prepared bone substitute was then filled into the cubic centimeter using the finger-packing technique and weighed again to determine the density of the bone substitute after finger packing.
- The cages produced by 3D printing were placed into soft material-printed intervertebral disc simulators of corresponding height, and their total weight was measured using a high-precision balance. It was observed that the cages with heights of 8 mm, 10 mm, 12 mm, and 14 mm had total weights of 17.901 g, 16.779 g, 16.070 g, and 15.535 g, respectively.
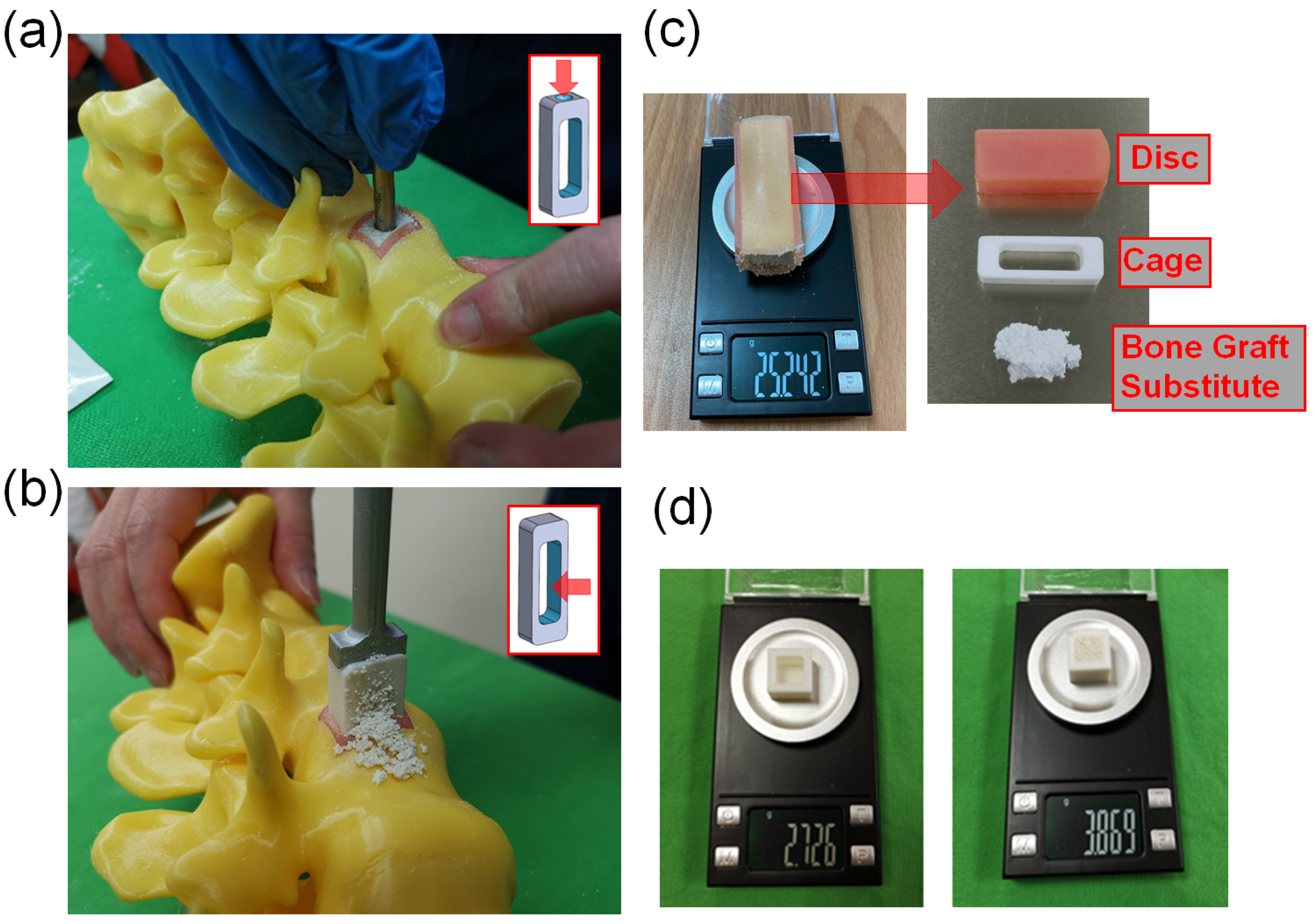
- In this study, we used two methods to place bone substitute into cages. The SG cage group (side hole for grafting group) involved using a cage with a side hole to fill it with bone substitute after implantation (Figure 2a). The FP cage group (finger-packing group) involved filling the cage with bone substitute before implantation using finger packing (Figure 2b).
- a.
- SG cage group: This study employed a cage with filling side holes (a specially designed innovative cage with “side hole for grafting”). Firstly, a soft-material printed intervertebral disc was placed into a 3D-printed spinal model, followed by the implantation of the specially designed cage into the soft-material printed intervertebral disc. Bone substitute was then filled into the cage through the side holes until it was completely filled. Subsequently, the intervertebral disc substitute, cage, and bone substitute were removed together and weighed using a high-precision scale (Figure 2c). This step was repeated 10 times for each group based on the different heights of the cage.
- b.
- FP cage group: Traditional methods were used in this study. Firstly, a soft 3D-printed intervertebral disc was placed into a 3D-printed spine model. Next, bone substitute was packed into the interior space of the 3D-printed cage using the finger-packing technique. An inserter was then employed to connect the 3D-printed cage, and a hammer was used to aid the implantation of the 3D-printed cage into the soft intervertebral disc within the spine model. After implantation, the weight of the 3D-printed intervertebral disc, cage, and internal bone substitute was measured using a high-precision scale and recorded. This step was repeated 10 times for each group based on the height of the cage.
- c.
- After each use of the high-precision scale, it must be recalibrated to zero before subsequent measurements can be taken.
- A 3D-printed cube with a 1-cubic centimeter internal space was fabricated for measurement purposes. The weight of the empty 3D-printed cube was initially determined. Subsequently, the 1-cubic centimeter space within the cube was filled with the bone substitute material, and the total weight was measured. This enabled the calculation of the weight of the bone substitute when occupying a volume of 1 cubic centimeter, which was found to be approximately 1.143 g (Figure 2d).
2.6. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, G.X.; Akbary, K.; Kotheeranurak, V.; Quillo-Olvera, J.; Jo, H.J.; Yang, X.W.; Mahatthanatrakul, A.; Kim, J.S. Clinical and Radiologic Outcomes of Direct Versus Indirect Decompression with Lumbar Interbody Fusion: A Matched-Pair Comparison Analysis. World Neurosurg. 2018, 119, e898–e909. [Google Scholar] [CrossRef]
- Han, X.G.; Tang, G.Q.; Han, X.; Xing, Y.G.; Zhang, Q.; He, D.; Tian, W. Comparison of Outcomes between Robot-Assisted Minimally Invasive Transforaminal Lumbar Interbody Fusion and Oblique Lumbar Interbody Fusion in Single-Level Lumbar Spondylolisthesis. Orthop. Surg. 2021, 13, 2093–2101. [Google Scholar] [CrossRef] [PubMed]
- Bydon, M.; De la Garza-Ramos, R.; Abt, N.B.; Macki, M.; Sciubba, D.M.; Wolinsky, J.P.; Bydon, A.; Gokaslan, Z.L.; Witham, T.F. Durotomy is associated with pseudoarthrosis following lumbar fusion. J. Clin. Neurosci. 2015, 22, 544–548. [Google Scholar] [CrossRef]
- Woods, K.R.; Billys, J.B.; Hynes, R.A. Technical description of oblique lateral interbody fusion at L1-L5 (OLIF25) and at L5-S1 (OLIF51) and evaluation of complication and fusion rates. Spine J. 2017, 17, 545–553. [Google Scholar] [CrossRef]
- Zhang, B.; Hu, Y.; Kong, Q.; Feng, P.; Liu, J.; Ma, J. Comparison of Oblique Lumbar Interbody Fusion Combined with Posterior Decompression (OLIF-PD) and Posterior Lumbar Interbody Fusion (PLIF) in the Treatment of Adjacent Segmental Disease (ASD). J. Pers. Med. 2023, 13, 368. [Google Scholar] [CrossRef]
- Lee, H.-J.; Ryu, K.-S.; Hur, J.-W.; Seong, J.-H.; Cho, H.-J.; Kim, J.-S. Safety of lateral interbody fusion surgery without intraoperative monitoring. Turk. Neurosurg. 2018, 28, 428–433. [Google Scholar]
- Ozgur, B.M.; Gillard, D.M.; Wood, E.E.; Truong, F.; Wendel, T.G. Can the use of a novel bone graft delivery system significantly increase the volume of bone graft material in a lumbar in situ cage, beyond volumes normally achieved via standard cage filling methodology? Results from a cadaveric pilot study. Interdiscip. Neurosurg. 2018, 14, 32–36. [Google Scholar] [CrossRef]
- Shi, Y.; Deng, T.; Peng, Y.; Qin, Z.; Ramalingam, M.; Pan, Y.; Chen, C.; Zhao, F.; Cheng, L.; Liu, J. Effect of Surface Modification of PEEK Artificial Phalanx by 3D Printing on its Biological Activity. Coatings 2023, 13, 400. [Google Scholar] [CrossRef]
- Hecker, A.; Tax, L.; Giese, B.; Schellnegger, M.; Pignet, A.-L.; Reinbacher, P.; Watzinger, N.; Kamolz, L.-P.; Lumenta, D.B. Clinical Applications of Three-Dimensional Printing in Upper Extremity Surgery: A Systematic Review. J. Pers. Med. 2023, 13, 294. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Ahn, S.H.; Choi, S.H.; Ahn, W.S.; Jung, I.-H. Clinical Application of a Customized 3D-Printed Bolus in Radiation Therapy for Distal Extremities. Life 2023, 13, 362. [Google Scholar] [CrossRef]
- Odom, M.; Gomez, J.R.; Danelson, K.A.; Sarwal, A. Development of a homemade spinal model for simulation to teach ultrasound guidance for lumbar puncture. Neurocrit. Care 2019, 31, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Heidari, A.; Nourbakhsh, S.; Mohammadi, R.; Semiromi, D. Design and fabrication of elastic two-component polymer-metal disks using a 3D printer under different loads for the lumbar spine. Polym. Test 2022, 112, 107633. [Google Scholar] [CrossRef]
- Pullen, M.W.; Pooley, R.A.; Kofler, J.M., Jr.; Valero-Moreno, F.; Ramos-Fresnedo, A.; Domingo, R.A.; Perez-Vega, C.; Fox, W.C.; Sandhu, S.J.S.; Quinones-Hinojosa, A. A radiographic analysis of common 3D print materials and assessment of their fidelity within vertebral models. J. 3D Print. Med. 2022, 8, 100080. [Google Scholar] [CrossRef]
- Fernandes, R.J.R.; Gee, A.; Kanawati, A.J.; Siddiqi, F.; Rasoulinejad, P.; Zdero, R.; Bailey, C. Evaluation of the contact surface between vertebral endplate and 3D printed patient-specific cage vs commercial cage. Sci. Rep. 2022, 12, 12505. [Google Scholar] [CrossRef] [PubMed]
- Adl Amini, D.; Okano, I.; Oezel, L.; Zhu, J.; Chiapparelli, E.; Shue, J.; Sama, A.A.; Cammisa, F.P.; Girardi, F.P.; Hughes, A.P. Evaluation of cage subsidence in standalone lateral lumbar interbody fusion: Novel 3D-printed titanium versus polyetheretherketone (PEEK) cage. Eur. Spine J. 2021, 30, 2377–2384. [Google Scholar] [CrossRef]
- Wu, J.; Feng, Q.; Yang, D.; Xu, H.; Wen, W.; Xu, H.; Miao, J. Biomechanical evaluation of different sizes of 3D printed cage in lumbar interbody fusion-a finite element analysis. BMC Musculoskelet. Disord. 2023, 24, 85. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Pao, J.L.; Chen, C.S.; Chen, Y.C.; Chang, C.C.; Hung, F.M.; Chang, C.H. Evaluation of New Biphasic Calcium Phosphate Bone Substitute: Rabbit Femur Defect Model and Preliminary Clinical Results. J. Med. Biol. Eng. 2017, 37, 85–93. [Google Scholar] [CrossRef]
- Yoo, J.S.; Min, S.H.; Yoon, S.H. Fusion rate according to mixture ratio and volumes of bone graft in minimally invasive transforaminal lumbar interbody fusion: Minimum 2-year follow-up. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 183–189. [Google Scholar] [CrossRef]
- Kanat, A.; Tsianaka, E.; Gasenzer, E.R.; Drosos, E. Some Interesting points of competition of X-ray using during the Greco-Ottoman War in 1897 and development of neurosurgical radiology: A reminiscence. Turk. Neurosurg. 2022, 32, 877–881. [Google Scholar] [CrossRef]
- Yu, Y.; Robinson, D.L.; Ackland, D.C.; Yang, Y.; Lee, P.V.S. Influence of the geometric and material properties of lumbar endplate on lumbar interbody fusion failure: A systematic review. J. Orthop. Surg. Res. 2022, 17, 224. [Google Scholar] [CrossRef]
- Xie, T.; Pu, L.; Zhao, L.; Lu, Y.; Yang, Z.; Wang, X.; Song, Y.; Zeng, J. Influence of coronal-morphology of endplate and intervertebral space to cage subsidence and fusion following oblique lumbar interbody fusion. BMC Musculoskelet. Disord. 2022, 23, 633. [Google Scholar] [CrossRef] [PubMed]
- Muthiah, N.; Yolcu, Y.U.; Alan, N.; Agarwal, N.; Hamilton, D.K.; Ozpinar, A. Evolution of polyetheretherketone (PEEK) and titanium interbody devices for spinal procedures: A comprehensive review of the literature. Eur. Spine J. 2022, 31, 2547–2556. [Google Scholar] [CrossRef]
- Tan, J.-H.; Cheong, C.K.; Hey, H.W.D. Titanium (Ti) cages may be superior to polyetheretherketone (PEEK) cages in lumbar interbody fusion: A systematic review and meta-analysis of clinical and radiological outcomes of spinal interbody fusions using Ti versus PEEK cages. Eur. Spine J. 2021, 30, 1285–1295. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.-C.; Chou, P.-H.; Lin, H.-H.; Wang, S.-T.; Chang, M.-C. Outcome of Ti/PEEK versus PEEK cages in minimally invasive transforaminal lumbar interbody fusion. Glob. Spine J. 2023, 13, 472–478. [Google Scholar] [CrossRef]
- Sheha, E.D.; Gandhi, S.D.; Colman, M.W. 3D printing in spine surgery. Ann. Transl. Med. 2019, 7, S164. [Google Scholar] [CrossRef]
- Garg, B.; Mehta, N. Current status of 3D printing in spine surgery. J. Clin. Orthop. Trauma 2018, 9, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.; Liao, Z.; Zeng, Q.; Chen, H.; Huang, W.; Liu, Z.; Chen, Y.; Zhong, J.; Huang, G. Customized three-dimensional-printed orthopedic close contact casts for the treatment of stable ankle fractures: Finite element analysis and a pilot study. ACS Omega 2021, 6, 3418–3426. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Lin, C.-L.; Yu, C.-H.; Chang, H.-C.; Lin, Y.-M.; Lin, J.-W. Biomechanical Analysis of Mandibular Implant-Assisted Removable Partial Denture with Distal Extension. J. Med. Biol. Eng. 2022, 42, 534–543. [Google Scholar] [CrossRef]
- Mayer, R.; Liacouras, P.; Thomas, A.; Kang, M.; Lin, L.; Simone, C.B. 3D printer generated thorax phantom with mobile tumor for radiation dosimetry. Rev. Sci. Instrum. 2015, 86, 074301. [Google Scholar] [CrossRef]
- Hong, J.-k.; Bae, I.-S.; Kang, H.I.; Kim, J.H.; Jwa, C. Development of a Pedicle Screw Fixation Simulation Model for Surgical Training Using a 3-Dimensional Printer. World Neurosurg. 2023, 171, e554–e559. [Google Scholar] [CrossRef]
- Cramer, J.; Quigley, E.; Hutchins, T.; Shah, L. Educational material for 3D visualization of spine procedures: Methods for creation and dissemination. J. Digit. Imaging 2017, 30, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Galvez, M.; Montoya, C.E.; Fuentes, J.; Rojas, G.M.; Asahi, T.; Currie, W.; Kuflik, M.; Chahin, A. Error measurement between anatomical porcine spine, CT images, and 3D printing. Acad. Radiol. 2020, 27, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-T.; Lee, C.-H.; Chen, K.-H.; Yen, Y.-C.; Wang, C.-H.; Wang, S.-P.; Su, K.-C. Trochanteric Nails for the Reduction of Intertrochanteric Fractures: A Biomechanical Analysis Based on Finite Element Analysis and DIC System. J. Med. Biol. Eng. 2022, 42, 459–468. [Google Scholar] [CrossRef]
- Liao, Y.; Yan, Y.; Kang, Y.; Wang, W.; Song, X.; Peng, W.; Fu, H.; Chen, H.; Wang, C. Biomechanical Analysis of the External Fixation in a Lumbar Fracture Model: A Finite Element Study. J. Med. Biol. Eng. 2022, 42, 469–478. [Google Scholar] [CrossRef]
- Tseng, B.-T.; Yen, Y.-C.; Cheng, C.-S.; Wang, C.-H.; Lien, K.-H.; Huang, C.-M.; Su, K.-C. Biomechanical Effects of Different Miniplate Thicknesses and Fixation Methods Applied in BSSO Surgery Under Two Occlusal Conditions. J. Med. Biol. Eng. 2022, 42, 445–458. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cage Height | 8 mm | 10 mm | 12 mm | 14 mm | |
|---|---|---|---|---|---|
| volume (cm3) | 1 | 2.930 | 3.662 | 4.395 | 5.128 |
| Estimated weight (g) | 1.143 | 3.349 | 4.187 | 5.024 | 5.861 |
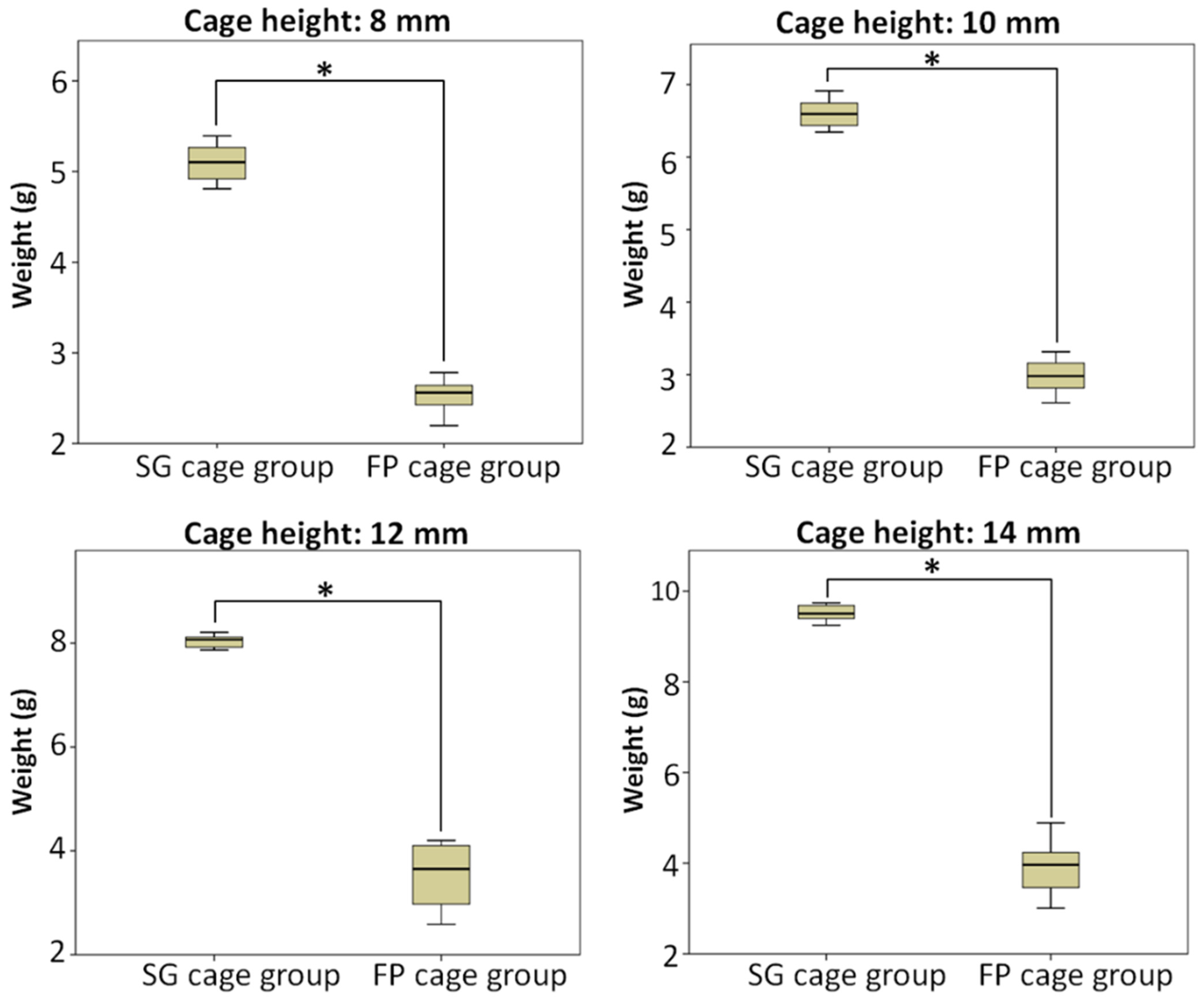
| Average weight (g) of SG cage group ± SD (average weight/estimated weight) | 5.101 ± 2.003 (152%) | 6.603 ± 0.190 (158%) | 8.040 ± 0.118 (160%) | 9.516 ± 0.169 (162%) | |
| Average weight (g) of FP cage group ± SD (average weight/excepted weight) | 2.540 ± 0.175 (76%) | 2.980 ± 0.224 (71%) | 3.535 ± 0.585 (71%) | 3.928 ± 0.552 (67%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shih, C.-M.; Lee, C.-H.; Chen, K.-H.; Pan, C.-C.; Yen, Y.-C.; Wang, C.-H.; Su, K.-C. Optimizing Spinal Fusion Cage Design to Improve Bone Substitute Filling on Varying Disc Heights: A 3D Printing Study. Bioengineering 2023, 10, 1250. https://doi.org/10.3390/bioengineering10111250
Shih C-M, Lee C-H, Chen K-H, Pan C-C, Yen Y-C, Wang C-H, Su K-C. Optimizing Spinal Fusion Cage Design to Improve Bone Substitute Filling on Varying Disc Heights: A 3D Printing Study. Bioengineering. 2023; 10(11):1250. https://doi.org/10.3390/bioengineering10111250
Chicago/Turabian StyleShih, Cheng-Min, Cheng-Hung Lee, Kun-Hui Chen, Chien-Chou Pan, Yu-Chun Yen, Chun-Hsiang Wang, and Kuo-Chih Su. 2023. "Optimizing Spinal Fusion Cage Design to Improve Bone Substitute Filling on Varying Disc Heights: A 3D Printing Study" Bioengineering 10, no. 11: 1250. https://doi.org/10.3390/bioengineering10111250
APA StyleShih, C.-M., Lee, C.-H., Chen, K.-H., Pan, C.-C., Yen, Y.-C., Wang, C.-H., & Su, K.-C. (2023). Optimizing Spinal Fusion Cage Design to Improve Bone Substitute Filling on Varying Disc Heights: A 3D Printing Study. Bioengineering, 10(11), 1250. https://doi.org/10.3390/bioengineering10111250