
A Systematic Review of the Long-Term Effects of Using Smartphone- and Tablet-Based Rehabilitation Technology for Balance and Gait Training and Exercise Programs




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
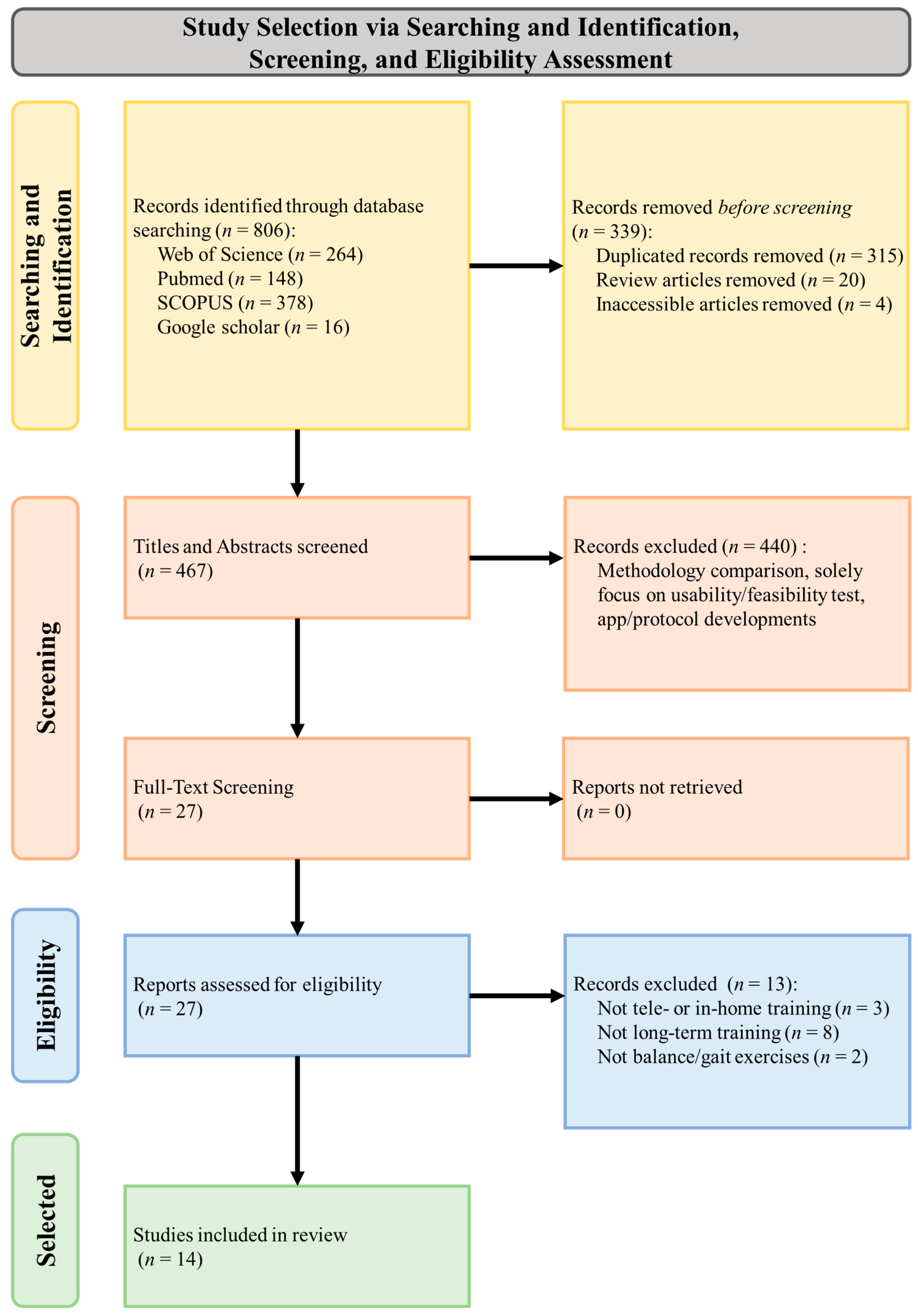
2.3. Study Selection
2.4. Data Extraction and Tabulation
2.5. Methodological Quality
3. Results
3.1. Study Quality
3.2. Study Analysis
3.2.1. Participant Cohort
3.2.2. Telerehabilitation Technology
3.2.3. Training Type, Period, and Location
3.2.4. Effects of Real-Time Biofeedback
3.2.5. Effects of Pre-Recorded or Real-Time Demonstration
3.2.6. Effects of Gamification
4. Discussion
4.1. Increased Accessibility and Convenience
4.2. Data Tracking and Analysis
4.3. Enhanced Engagement and Motivation
4.4. Improved Outcomes
4.5. Limitations, Future Work, and Implications of Included Studies
- Rehabilitation exercises that challenge balance and gait, activate neural pathways, and promote neuroplasticity are more likely to generalize the learned skills to similar functional activities.
- Sensory-augmented or gamified rehabilitation combining balance or gait exercises with cognitive or motor tasks improves the ability to perform activities that require multitasking.
- Balance and gait rehabilitation exercises with sensory integration challenge the brain to process information from vision, vestibular, proprioception, and other systems, enhancing stability and navigation, particularly in uncertain environments.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Konrad, H.R.; Girardi, M.; Helfert, R. Balance and aging. Laryngoscope 1999, 109, 1454–1460. [Google Scholar] [CrossRef]
- Berg, W.P.; Alessio, H.M.; Mills, E.M.; Tong, C. Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing 1997, 26, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Timsina, L.R.; Willetts, J.L.; Brennan, M.J.; Marucci-Wellman, H.; Lombardi, D.A.; Courtney, T.K.; Verma, S.K. Circumstances of fall-related injuries by age and gender among community-dwelling adults in the United States. PLoS ONE 2017, 12, e0176561. [Google Scholar] [CrossRef]
- Vaishya, R.; Vaish, A. Falls in older adults are serious. Indian J. Orthop. 2020, 54, 69–74. [Google Scholar] [CrossRef]
- Arnold, C.M.; Sran, M.M.; Harrison, E.L. Exercise for fall risk reduction in community-dwelling older adults: A systematic review. Physiother. Can. 2008, 60, 358–372. [Google Scholar] [CrossRef] [PubMed]
- Geohagen, O.; Hamer, L.; Lowton, A.; Guerra, S.; Milton-Cole, R.; Ellery, P.; Martin, F.C.; Lamb, S.E.; Sackley, C.; Sheehan, K.J. The effectiveness of rehabilitation interventions including outdoor mobility on older adults’ physical activity, endurance, outdoor mobility and falls-related self-efficacy: Systematic review and meta-analysis. Age Ageing 2022, 51, afac120. [Google Scholar] [CrossRef] [PubMed]
- Hackney, M.E.; Wolf, S.L. Impact of Tai Chi Chu’an practice on balance and mobility in older adults: An integrative review of 20 years of research. J. Geriatr. Phys. Ther. 2014, 37, 127–135. [Google Scholar] [CrossRef]
- Selves, C.; Stoquart, G.; Lejeune, T. Gait rehabilitation after stroke: Review of the evidence of predictors, clinical outcomes and timing for interventions. Acta Neurol. Belg. 2020, 120, 783–790. [Google Scholar] [CrossRef] [PubMed]
- Arienti, C.; Lazzarini, S.G.; Pollock, A.; Negrini, S. Rehabilitation interventions for improving balance following stroke: An overview of systematic reviews. PLoS ONE 2019, 14, e0219781. [Google Scholar] [CrossRef]
- Dutta, A.; Lahiri, U.; Das, A.; Nitsche, M.A.; Guiraud, D. Post-stroke balance rehabilitation under multi-level electrotherapy: A conceptual review. Front. Neurosci. 2014, 8, 403. [Google Scholar] [CrossRef]
- De Freitas Tb Ms, P.T.; Leite, P.B.; Doná, F.P.T.; Pompeu, J.P.T.; Swarowsky, A.P.T.; Torriani-Pasin, C.P.T. The effects of dual task gait and balance training in Parkinson’s disease: A systematic review. Physiother. Theory Pract. 2020, 36, 1088–1096. [Google Scholar] [CrossRef]
- Coelho, D.B.; de Oliveira, C.E.N.; Guimarães, M.V.C.; Ribeiro de Souza, C.; Dos Santos, M.L.; de Lima-Pardini, A.C. A systematic review on the effectiveness of perturbation-based balance training in postural control and gait in Parkinson’s disease. Physiotherapy 2022, 116, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Gilat, M.; Ginis, P.; Zoetewei, D.; De Vleeschhauwer, J.; Hulzinga, F.; D’Cruz, N.; Nieuwboer, A. A systematic review on exercise and training-based interventions for freezing of gait in Parkinson’s disease. NPJ Park. Dis. 2021, 7, 81. [Google Scholar] [CrossRef]
- Martino Cinnera, A.; Bisirri, A.; Leone, E.; Morone, G.; Gaeta, A. Effect of dual-task training on balance in patients with multiple sclerosis: A systematic review and meta-analysis. Clin. Rehabil. 2021, 35, 1399–1412. [Google Scholar] [CrossRef] [PubMed]
- Corrini, C.; Gervasoni, E.; Perini, G.; Cosentino, C.; Putzolu, M.; Montesano, A.; Pelosin, E.; Prosperini, L.; Cattaneo, D. Mobility and balance rehabilitation in multiple sclerosis: A systematic review and dose-response meta-analysis. Mult. Scler. Relat. Disord. 2023, 69, 104424. [Google Scholar] [CrossRef] [PubMed]
- Iodice, R.; Aceto, G.; Ruggiero, L.; Cassano, E.; Manganelli, F.; Dubbioso, R. A review of current rehabilitation practices and their benefits in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2023, 69, 104460. [Google Scholar] [CrossRef]
- Lee, B.-C. Design and Assessment of Vibrotactile Biofeedback and Instructional Systems for Balance Rehabilitation Applications; University of Michigan: Ann Arbor, MI, USA, 2012. [Google Scholar]
- Dobkin, B.H. A rehabilitation-internet-of-things in the home to augment motor skills and exercise training. Neurorehabil Neural Repair. 2017, 31, 217–227. [Google Scholar] [CrossRef]
- Nakae, H.; Tsushima, H. Effects of home exercise on physical function and activity in home care patients with Parkinson’s disease. J. Phys. Ther. Sci. 2014, 26, 1701–1706. [Google Scholar] [CrossRef]
- Kao, C.L.; Chen, L.K.; Chern, C.M.; Hsu, L.C.; Chen, C.C.; Hwang, S.J. Rehabilitation outcome in home-based versus supervised exercise programs for chronically dizzy patients. Arch. Gerontol. Geriatr. 2010, 51, 264–267. [Google Scholar] [CrossRef]
- Forkan, R.; Pumper, B.; Smyth, N.; Wirkkala, H.; Ciol, M.A.; Shumway-Cook, A. Exercise adherence following physical therapy intervention in older adults with impaired balance. Phys. Ther. 2006, 86, 401–410. [Google Scholar] [CrossRef]
- Sluijs, E.M.; Kok, G.J.; van der Zee, J. Correlates of exercise compliance in physical therapy. Phys. Ther. 1993, 73, 771–782, discussion 783–786. [Google Scholar] [CrossRef]
- Appleby, E.; Gill, S.T.; Hayes, L.K.; Walker, T.L.; Walsh, M.; Kumar, S. Effectiveness of telerehabilitation in the management of adults with stroke: A systematic review. PLoS ONE 2019, 14, e0225150. [Google Scholar] [CrossRef] [PubMed]
- Dalmazane, M.; Gallou-Guyot, M.; Compagnat, M.; Magy, L.; Montcuquet, A.; Billot, M.; Daviet, J.C.; Perrochon, A. Effects on gait and balance of home-based active video game interventions in persons with multiple sclerosis: A systematic review. Mult. Scler. Relat. Disord. 2021, 51, 102928. [Google Scholar] [CrossRef]
- Gandolfi, M.; Geroin, C.; Dimitrova, E.; Boldrini, P.; Waldner, A.; Bonadiman, S.; Picelli, A.; Regazzo, S.; Stirbu, E.; Primon, D.; et al. Virtual reality telerehabilitation for postural instability in parkinson’s disease: A multicenter, single-blind, randomized, controlled trial. BioMed Res. Int. 2017, 2017, 7962826. [Google Scholar] [CrossRef] [PubMed]
- Truijen, S.; Abdullahi, A.; Bijsterbosch, D.; van Zoest, E.; Conijn, M.; Wang, Y.; Struyf, N.; Saeys, W. Effect of home-based virtual reality training and telerehabilitation on balance in individuals with Parkinson disease, multiple sclerosis, and stroke: A systematic review and meta-analysis. Neurol. Sci. 2022, 43, 2995–3006. [Google Scholar] [CrossRef] [PubMed]
- Moral-Munoz, J.A.; Zhang, W.; Cobo, M.J.; Herrera-Viedma, E.; Kaber, D.B. Smartphone-based systems for physical rehabilitation applications: A systematic review. Assist. Technol. 2021, 33, 223–236. [Google Scholar] [CrossRef]
- Reyes, A.; Qin, P.; Brown, C.A. A standardized review of smartphone applications to promote balance for older adults. Disabil. Rehabil. 2018, 40, 690–696. [Google Scholar] [CrossRef]
- Peters, J.; Abou, L.; Wong, E.; Dossou, M.S.; Sosnoff, J.J.; Rice, L.A. Smartphone-based gait and balance assessment in survivors of stroke: A systematic review. Disabil. Rehabil. Assist. Technol. 2022, 1–11. [Google Scholar] [CrossRef]
- Di Lorito, C.; Long, A.; Byrne, A.; Harwood, R.H.; Gladman, J.R.F.; Schneider, S.; Logan, P.; Bosco, A.; van der Wardt, V. Exercise interventions for older adults: A systematic review of meta-analyses. J. Sport Health Sci. 2021, 10, 29–47. [Google Scholar] [CrossRef]
- Granacher, U.; Muehlbauer, T.; Gruber, M. A qualitative review of balance and strength performance in healthy older adults: Impact for testing and training. J. Aging Res. 2012, 2012, 708905. [Google Scholar] [CrossRef]
- Lesinski, M.; Hortobágyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Effects of balance training on balance performance in healthy older adults: A systematic review and meta-analysis. Sports Med. 2015, 45, 1721–1738. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Chen, W.; Chen, Q.; Li, F.; Chen, C.; Li, P.; Li, F.; Guo, S.; Chen, P.; Yuan, W.; et al. Effects of resistance and balance exercises for athletic ability and quality of life in people with osteoporotic vertebral fracture: Systematic review and meta-analysis of randomized control trials. Front. Med. 2023, 10, 1135063. [Google Scholar] [CrossRef] [PubMed]
- Zech, A.; Hübscher, M.; Vogt, L.; Banzer, W.; Hänsel, F.; Pfeifer, K. Balance training for neuromuscular control and performance enhancement: A systematic review. J. Athl. Train. 2010, 45, 392–403. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health, Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 2017.
- Abou, L.; Alluri, A.; Fliflet, A.; Du, Y.; Rice, L.A. Effectiveness of physical therapy interventions in reducing fear of falling among individuals with neurologic diseases: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2021, 102, 132–154. [Google Scholar] [CrossRef] [PubMed]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson’s disease: A pilot randomized controlled trial. Park. Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef]
- Silveira, P.; van de Langenberg, R.; van Het Reve, E.; Daniel, F.; Casati, F.; de Bruin, E.D. Tablet-based strength-balance training to motivate and improve adherence to exercise in independently living older people: A phase II preclinical exploratory trial. J. Med. Internet Res. 2013, 15, e159. [Google Scholar] [CrossRef]
- An, J.; Kim, J.; Lai, E.C.; Lee, B.C. Effects of a smartphone-based wearable telerehabilitation system for in-home dynamic weight-shifting balance exercises by individuals with parkinson’s disease. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 5678–5681. [Google Scholar] [CrossRef]
- Lee, B.C.; An, J.; Kim, J.; Lai, E.C. Performing dynamic weight-shifting balance exercises with a smartphone-based wearable telerehabilitation system for home use by individuals with parkinson’s disease: A proof-of-concept study. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 456–463. [Google Scholar] [CrossRef]
- Jabri, S.; Bushart, D.D.; Kinnaird, C.; Bao, T.; Bu, A.; Shakkottai, V.G.; Sienko, K.H. Preliminary study of vibrotactile feedback during home-based balance and coordination training in individuals with cerebellar ataxia. Sensors 2022, 22, 3512. [Google Scholar] [CrossRef]
- Callisaya, M.L.; Jayakody, O.; Vaidya, A.; Srikanth, V.; Farrow, M.; Delbaere, K. A novel cognitive-motor exercise program delivered via a tablet to improve mobility in older people with cognitive impairment—StandingTall Cognition and Mobility. Exp. Gerontol. 2021, 152, 111434. [Google Scholar] [CrossRef]
- Cochen De Cock, V.; Dotov, D.; Damm, L.; Lacombe, S.; Ihalainen, P.; Picot, M.C.; Galtier, F.; Lebrun, C.; Giordano, A.; Driss, V.; et al. BeatWalk: Personalized music-based gait rehabilitation in parkinson’s disease. Front. Psychol. 2021, 12, 655121. [Google Scholar] [CrossRef]
- Campbell, K.R.; Peterka, R.J.; Fino, P.C.; Parrington, L.; Wilhelm, J.L.; Pettigrew, N.C.; King, L.A. The effects of augmenting traditional rehabilitation with audio biofeedback in people with persistent imbalance following mild traumatic brain injury. Front. Neurol. 2022, 13, 926691. [Google Scholar] [CrossRef]
- Bao, T.; Carender, W.J.; Kinnaird, C.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Kabeto, M.; Seidler, R.D.; Sienko, K.H. Effects of long-term balance training with vibrotactile sensory augmentation among community-dwelling healthy older adults: A randomized preliminary study. J. Neuroeng. Rehabil. 2018, 15, 5. [Google Scholar] [CrossRef]
- Bao, T.; Noohi, F.; Kinnaird, C.; Carender, W.J.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Seidler, R.D.; Sienko, K.H. Retention effects of long-term balance training with vibrotactile sensory augmentation in healthy older adults. Sensors 2022, 22, 3014. [Google Scholar] [CrossRef]
- Hong, J.; Kong, H.J.; Yoon, H.J. Web-based telepresence exercise program for community-dwelling elderly women with a high risk of falling: Randomized controlled trial. JMIR Mhealth Uhealth 2018, 6, e132. [Google Scholar] [CrossRef] [PubMed]
- Wakasa, M.; Odashima, T.; Saito, A.; Kimoto, M.; Saito, I.; Handa, S.; Syukunobe, K.; Kume, Y.; Okada, K. Telerehabilitation with tablet computers replaces face-to-face rehabilitation. Phys. Occup. Ther. Geriatr. 2020, 38, 85–97. [Google Scholar] [CrossRef]
- Burgos, P.I.; Lara, O.; Lavado, A.; Rojas-Sepúlveda, I.; Delgado, C.; Bravo, E.; Kamisato, C.; Torres, J.; Castañeda, V.; Cerda, M. Exergames and telerehabilitation on smartphones to improve balance in stroke patients. Brain Sci. 2020, 10, 773. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Mishra, R.K.; York, M.K.; Enriquez, A.; Lindsay, A.; Barchard, G.; Vaziri, A.; Najafi, B. Tele-medicine based and self-administered interactive exercise program (Tele-exergame) to improve cognition in older adults with mild cognitive impairment or dementia: A feasibility, acceptability, and proof-of-concept study. Int. J. Environ. Res. Public Health 2022, 19, 16361. [Google Scholar] [CrossRef] [PubMed]
- Kairy, D.; Lehoux, P.; Vincent, C.; Visintin, M. A systematic review of clinical outcomes, clinical process, healthcare utilization and costs associated with telerehabilitation. Disabil. Rehabil. 2009, 31, 427–447. [Google Scholar] [CrossRef]
- Delgoshaei, B.; Mobinizadeh, M.; Mojdekar, R.; Afzal, E.; Arabloo, J.; Mohamadi, E. Telemedicine: A systematic review of economic evaluations. Med. J. Islam. Repub. Iran 2017, 31, 113. [Google Scholar] [CrossRef]
- Brennan, D.M.; Mawson, S.; Brownsell, S. Telerehabilitation: Enabling the remote delivery of healthcare, rehabilitation, and self management. Stud. Health Technol. Inform. 2009, 145, 231–248. [Google Scholar]
- Dozza, M.; Wall, C., 3rd; Peterka, R.J.; Chiari, L.; Horak, F.B. Effects of practicing tandem gait with and without vibrotactile biofeedback in subjects with unilateral vestibular loss. J. Vestib. Res. 2007, 17, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Wolf, S.L.; He, J. Recent developments in biofeedback for neuromotor rehabilitation. J. Neuroeng. Rehabil. 2006, 3, 11. [Google Scholar] [CrossRef]
- Wong, M.S.; Mak, A.F.; Luk, K.D.; Evans, J.H.; Brown, B. Effectiveness of audio-biofeedback in postural training for adolescent idiopathic scoliosis patients. Prosthet. Orthot. Int. 2001, 25, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Janssen, J.; Verschuren, O.; Renger, W.J.; Ermers, J.; Ketelaar, M.; van Ee, R. Gamification in physical therapy: More than using games. Pediatr. Phys. Ther. 2017, 29, 95–99. [Google Scholar] [CrossRef]


{kind=link}
| Web of Science | Title: (“Smartphone” OR “Tablet”) AND (“*rehabilitation” OR “Training” OR “exergame” OR “exer-game”) AND (“balance” OR “gait”) Abstract: (“Smartphone” OR “Tablet”) AND (“rehabilitation” OR “Training” OR “exergame” OR “exer-game”) AND (“balance” OR “gait”) Topic: (“Smartphone” OR “Tablet”) AND (“*rehabilitation” OR “Training” OR “exergame” OR “exer-game”) AND (“balance” OR “gait”) |
| Pubmed | Title/Abstract: (“Smartphone” OR “Tablet”) AND (“*rehabilitation” OR “Training” OR “exergame” OR “exer-game”) AND (“balance” OR “gait”) |
| Scopus | Article title, Abstract, Keywords: (“Smartphone” OR “Tablet”) AND (“*rehabilitation” OR “Training”) AND (“balance” OR “gait”) |
| Google Scholar | With all of the words: (“Smartphone” OR “Tablet”) AND (“rehabilitation” OR “Training” OR “exergame” OR “exer-game”) AND (“balance” OR “gait”) |
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Overall Quality | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ginis et al. (2016) [37] | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | Good |
| Silveira et al. (2013) [38] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| An et al. (2020) [39] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | NA | No | Good |
| Lee et al. (2023) [40] | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| Jabri et al. (2022) [41] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| Callisay et al. (2021) [42] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | Good |
| Cochen et al. (2021) [43] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | Good |
| Campbell et al. (2022) [44] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| Bao et al. (2018) [45] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | Good |
| Bao et al. (2022) [46] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| Hong et al. (2018) [47] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| Wakasa et al. (2020) [48] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | Good |
| Burgos et al. (2020) [49] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | No | Yes | Good |
| Park et al. (2022) [50] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | N/A | Yes | Yes | Good |
| Study | Participant Cohort | Age (Years) | Sample Size (Groups) |
|---|---|---|---|
| Ginis et al. (2016) [37] | Parkinson’s disease | Not specified | 38 (IG = 20; CG = 18) |
| Silveira et al. (2013) [38] | Older adults | 75 ± 6 | 33 (Individual IG = 11; Social IG = 12; CG = 10) |
| An et al. (2020) [39] | Parkinson’s disease | 75.5 ± 4.9 | 2 (N/A) |
| Lee et al. (2023) [40] | Parkinson’s disease | 50–75 | 7 (N/A) |
| Jabri et al. (2022) [41] | Hereditary cerebellar ataxia | 47 ± 12 | 7 (N/A) |
| Callisay et al. (2021) [42] | Older adults | 72.8 ± 7 | 77 (N/A) |
| Cochen et al. (2021) [43] | Parkinson’s disease | 65 ± 9 | 39 (N/A) |
| Campbell et al. (2022) [44] | Chronic mild traumatic brain injury (mTBI) | 40.9 ± 11 | 31 (IG = 16; CG = 15) |
| Bao et al. (2018) [45] | Older adults | 75.6 ± 4.9 | 12 (IG = 6; CG = 6) |
| Bao et al. (2022) [46] | Older adults | 75.4 ± 4.7 | 15 (IG = 8; CG = 7) |
| Hong et al. (2018) [47] | Older adults (with Fall Risk Assessment scores > 14) | 68–91 | 23 (IG = 10; CG = 13) |
| Wakasa et al. (2020) [48] | Older adults | 76.3 ± 3.3 | 9 (N/A) |
| Burgos et al. (2020) [49] | Early subacute stroke | 46–79 | 10 (IG = 6; CG = 4) |
| Park et al. (2022) [50] | Older adults (with mild cognitive impairment or dementia) | 68.1 ± 5.4 | 14 (N/A) |
| Study | Technology and Additional Sensors | Training Type | Delivery Modality | Training and Assessment Periods | Training Location | Outcome Measures |
|---|---|---|---|---|---|---|
| Ginis et al. (2016) [37] | Smartphone IMU sensors | Gait | Real-time visual and auditory biofeedback | Six weeks Three times/week Pre-, Post-, and Retention 1 month | In and around the home | (1) Gait parameters (gait speed, stride length, DS time) (2) Balance (MiniBESTest, FSST, FES-I) (3) Endurance and physical capacity (2MWT, PASE) (4) FOG severity (NFOG-Q, Ziegler protocol) (5) Disease severity (UPDRS III) (6) Cognitive assessments (CTT A and B, VF scores in sitting and walking) (7) Quality of life (SF-36) |
| Silveira et al. (2013) [38] | Tablet No additional sensors | Balance, Strength | Pre-recorded demonstration | Twelve weeks Five times/week; Balance training Two times/week; Strength training Pre-, Post- | In-home | (1) Adherence and attrition (2) Preferred and fast gait speed (3) Motivation instruments (self-reported 7-point Likert scale questionnaire) (4) Change of behavior (self-reported TTM questionnaire) |
| An et al. (2020) [39] | Smartphone IMU sensors and four vibration units | Balance | Real-time visual and vibrotactile biofeedback | Six weeks Three times/week Pre-, Post-, and Retention 1 month | In-home | (1) Exercise performance (XCORR, PE) (2) Regression analysis using linear and exponential models were conducted to estimate average XCORR and PE trends (3) Balance and gait performance and level of fear of falling (LOS, SOT, FES, ABC, DGI) |
| Lee et al. (2023) [40] | Smartphone IMU sensors and four vibration units | Balance | Real-time visual and vibrotactile biofeedback | Six weeks Three times/week Pre-, Post- | In-home | (1) Exercise performance (XCORR, PE) (2) Regression analysis using linear and exponential models were conducted to estimate the trends of the average XCORR and PE (3) TAM questionnaire (8-point Likert scale questionnaire averaged across the participants) |
| Jabri et al. (2022) [41] | Smartphone Built-in gyroscope and four vibration units | Balance, Coordination | Real-time vibrotactile biofeedback | Six weeks with biofeedback Five times/week Six weeks without biofeedback Five times/week Pre-, Per- (6 weeks), Post- | In and around-home | Balance and coordination assessments (SARA scores, SARA posture & gait subscores, mCTSIB, DGI, TUG, TUG-m, 5×STS, lower-body strength) |
| Callisay et al. (2021) [42] | Tablet No additional sensors | Balance, Strength, Cognition | Pre-recorded demonstration | Six months Two h/week Pre-, Post- | In-home | (1) Gait parameters (gait speed, dual-task gait speed) (2) Balance (15s step test, FISCIT-4) (3) Muscle strength (5×STS) (4) Cognition (executive function, memory, attention), mood, and balance confidence (5) Adherence, safety, usability, and feedback |
| Cochen et al. (2021) [43] | Smartphone IMU sensors | Gait | Real-time auditory biofeedback | Four weeks Five times/week Pre-, Post- | In and around the home | (1) Disease severity (Hoehn and Yahr scale) (2) Fall risk (FES) (3) Balance (MiniBESTest) (4) Global cognitive function (MoCA), depressive symptoms (BDI), anxiety (Parkinson’s anxiety scale), apathy (Lille apathy rating scale), fatigue (fatigue severity scale), and quality of life (EQ-5D) (5) Safety and tolerance (daily survey on the number of falls, fatigue, and pain) (6) Observance, usability, and enjoyment (7) Physical activity evaluation (CHAMPS) (8) Gait parameters (6MWT) |
| Campbell et al. (2022) [44] | Smartphone Built-in acceleration sensor and headphone | Balance | Real-time auditory biofeedback | Six weeks 45 min biweekly Pre-, Post- | In-home | (1) PCSS (2) Balance (SOT, central sensorimotor integration test) |
| Bao et al. (2018) [45] | Smartphone Built-in gyroscope and four vibration units | Balance | Real-time vibrotactile biofeedback | Eight weeks Three times/week Pre-, Per (4 weeks), Post- | In-home | Balance performance (ABC, SOT, MiniBEST, 5×STS, FSST, FRT, Gait Speed Test, TUG, TUG-COG) |
| Bao et al. (2022) [46] | Smartphone Built-in gyroscope and four vibration units | Balance | Real-time vibrotactile biofeedback | Eight weeks Three times/week Pre-, Retention 1 (1 week), Retention 2 (1 month), Retention 3 (6 months) fMRI assessment Pre-, Retention (1 week) | In-home | Balance performance (ABC, SOT, MiniBEST, 5×STS, FSST, FRT, Gait Speed Test, TUG, TUG-COG, MDC) |
| Hong et al. (2018) [47] | Tablet No additional sensors | Balance, Resistance | Real-time demonstration | Twelve weeks (3 times/week) Pre-, Post- | In-home | (1) Body composition (2) Physical function parameters (SFT, BBS) (3) Psychological factors (Korean Falls Efficacy Scale scores, Fear of Falling Questionnaire scores) |
| Wakasa et al. (2020) [48] | Tablet No additional sensors | Balance, Strength, Flexibility | Real-time demonstration | Six months (60–70 min biweekly) Pre-, Post- | Community center | (1) Motor function–balance and gait (LES, TUG, BBS) (2) Maximal isotonic strengthening of the knee extensors (3) Health status (SF-36) (4) Questionnaire on motivation and perceptions of benefits from participation |
| Burgos et al. (2020) [49] | Smartphone No additional sensors | Balance | Gamification | Four weeks Nine times/week Pre-, Post- | In-home | (1) Balance performance (BBS, MiniBESTest) (2) Functional independence (BI) (3) System Usability Scale |
| Park et al. (2022) [50] | Tablet No additional sensors | Balance, Cognition | Gamification | Six weeks Two times/week Pre-, Post- | In-home | (1) Acceptance (TAM questionnaire) (2) Cognition and anxiety level (MoCA, BAI) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.; Ahn, J.; Lee, B.-C. A Systematic Review of the Long-Term Effects of Using Smartphone- and Tablet-Based Rehabilitation Technology for Balance and Gait Training and Exercise Programs. Bioengineering 2023, 10, 1142. https://doi.org/10.3390/bioengineering10101142
Lee C, Ahn J, Lee B-C. A Systematic Review of the Long-Term Effects of Using Smartphone- and Tablet-Based Rehabilitation Technology for Balance and Gait Training and Exercise Programs. Bioengineering. 2023; 10(10):1142. https://doi.org/10.3390/bioengineering10101142
Chicago/Turabian StyleLee, Chihyeong, Jooeun Ahn, and Beom-Chan Lee. 2023. "A Systematic Review of the Long-Term Effects of Using Smartphone- and Tablet-Based Rehabilitation Technology for Balance and Gait Training and Exercise Programs" Bioengineering 10, no. 10: 1142. https://doi.org/10.3390/bioengineering10101142
APA StyleLee, C., Ahn, J., & Lee, B.-C. (2023). A Systematic Review of the Long-Term Effects of Using Smartphone- and Tablet-Based Rehabilitation Technology for Balance and Gait Training and Exercise Programs. Bioengineering, 10(10), 1142. https://doi.org/10.3390/bioengineering10101142