

Current Role of Intra-Articular Injections of Platelet-Rich Plasma in Adhesive Capsulitis of Shoulder: A Systematic Review

 ,
,  ,
,  ,
,  , and
, and 
Abstract
1. Introduction
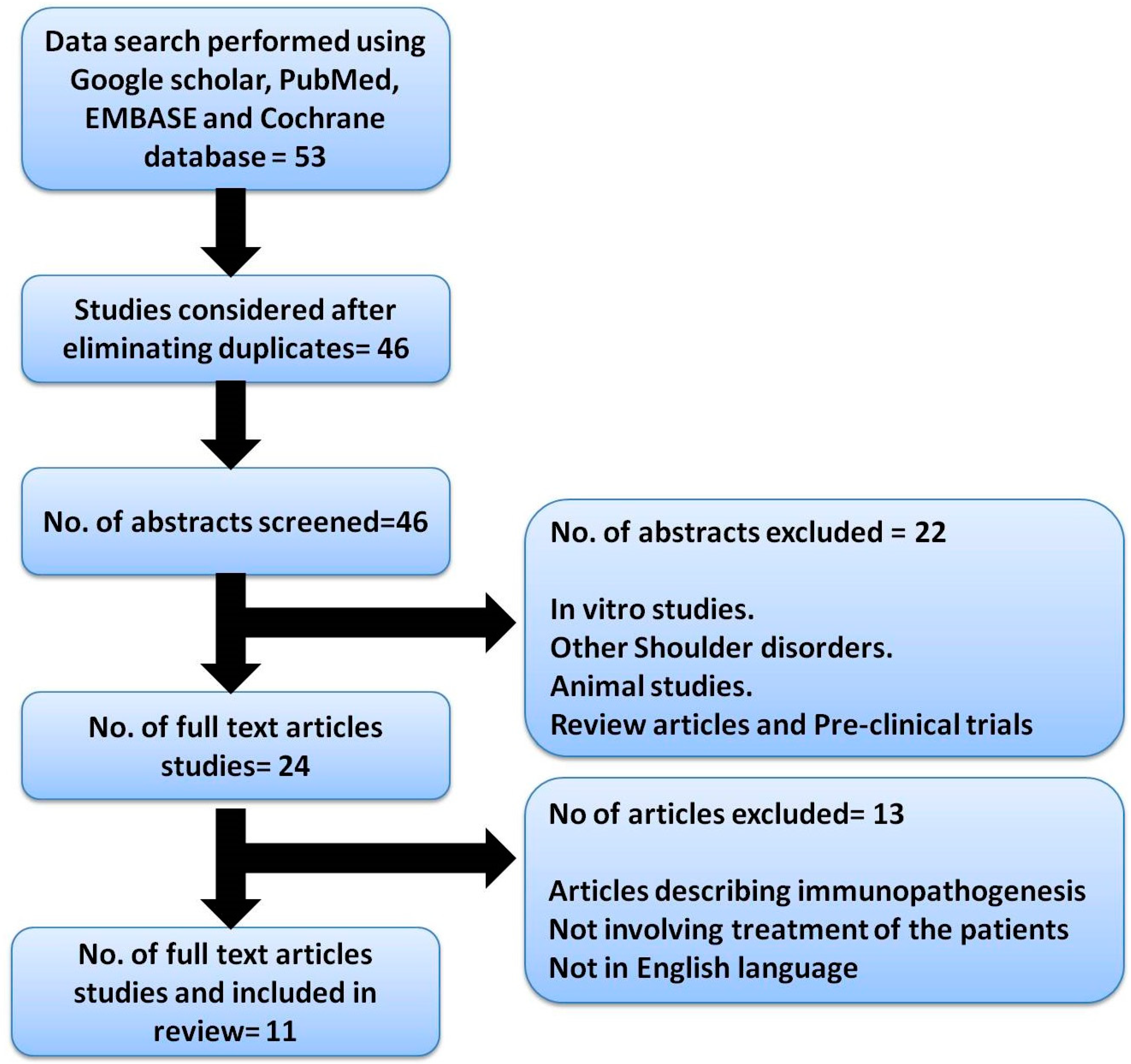
2. Materials and Methods Search Strategy
Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reeves, B. The Natural History of the Frozen Shoulder Syndrome. Scand. J. Rheumatol. 1975, 4, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Brue, S.; Valentin, A.; Forssblad, M.; Werner, S.; Mikkelsen, C.; Cerulli, G. Idiopathic Adhesive Capsulitis of the Shoulder: A Review. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Page, P.; Labbe, A. Adhesive Capsulitis: Use the Evidence to Integrate Your Interventions. N. Am. J. Sports Phys. Ther. 2010, 5, 266–273. [Google Scholar]
- Koh, K.H. Corticosteroid Injection for Adhesive Capsulitis in Primary Care: A Systematic Review of Randomised Clinical Trials. Singap. Med. J. 2016, 57, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Cvetanovich, G.L.; Leroux, T.; Hamamoto, J.T.; Higgins, J.D.; Romeo, A.A.; Verma, N.N. Arthroscopic 360° Capsular Release for Adhesive Capsulitis in the Lateral Decubitus Position. Arthrosc. Tech. 2016, 5, e1033–e1038. [Google Scholar] [CrossRef][Green Version]
- Mishra, A.; Woodall, J.; Vieira, A. Treatment of Tendon and Muscle Using Platelet-Rich Plasma. Clin. Sports Med. 2009, 28, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Aslani, M.A.; Mirzaee, F.; Baradaran, A.F.; Zafarani, Z.; Aslani, H. Clinical Results of Platelet-Rich Plasma in Frozen Shoulder. J. Cell. Mol. Anesth. 2020, 5, 74–78. [Google Scholar] [CrossRef]
- Barman, A.; Mukherjee, S.; Sahoo, J.; Maiti, R.; Rao, P.B.; Sinha, M.K.; Sahoo, D.; Tripathy, S.K.; Patro, B.K.; Bag, N.D. Single Intra-Articular Platelet-Rich Plasma Versus Corticosteroid Injections in the Treatment of Adhesive Capsulitis of the Shoulder: A Cohort Study. Am. J. Phys. Med. Rehabil. 2019, 98, 549–557. [Google Scholar] [CrossRef]
- Ünlü, B.; Çalış, F.A.; Karapolat, H.; Üzdü, A.; Tanıgör, G.; Kirazlı, Y. Efficacy of Platelet-Rich Plasma Injections in Patients with Adhesive Capsulitis of the Shoulder. Int. Orthop. 2021, 45, 181–190. [Google Scholar] [CrossRef]
- Upadhyay, S.; Jorule, K.; Varma, H.S.; Chansoria, M. Ongoing Efficacy of Platelet-Rich Plasma vs Corticosteroid Injection in Patients with Adhesive Capsulitis: A Prospective Randomized Assessor-Blind Comparative Analysis. J. Recent Adv. Pain 2020, 6, 10. [Google Scholar] [CrossRef]
- Agrawal, A.C.; Nayak, B.; Sakale, H. Management of Adhesive Capsulitis of Shoulder Joint by Single Platelet Rich Plasma Injection. J. Orthop. Traumatol. Rehabil. 2019, 11, 62. [Google Scholar] [CrossRef]
- Çalış, H.T.; Karabaş, Ç.; Güler, E. Effects of Platelet-rich Plasma Injection on Adhesive Capsulitis: An Interventional Case Series. Erciyes Med. J. /Erciyes Tip Derg. 2019, 41, 102–106. [Google Scholar]
- Kumar, S.; Singh, P.P. Comparative Analysis on Efficacy of Injection Methyl Prednisolone vs. Autologous PRP in Adhesive Capsulitis/Peri Arthritis/Frozen Shoulder. Int. J. Med. Res. Prof. 2019, 5, 278–281. [Google Scholar]
- Kothari, S.Y.; Srikumar, V.; Singh, N. Comparative efficacy of platelet rich plasma injection, corticosteroid injection and ultrasonic therapy in the treatment of periarthritis shoulder. J. Clin. Diagnos. Res. 2017, 11, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Jeyaraman, M.; Ramesh, R.; Prajwal, G.S.; Dhamsania, H.J. The comparative and prospective study on efficacy and functional outcome of autologous platelet rich plasma injection vs. hydrodissection in adhesive capsulitis of shoulder. Int. J. Res. Orthop. 2018, 4, 848–853. [Google Scholar] [CrossRef]
- Lin, J. Platelet-rich plasma injection in the treatment of frozen shoulder: A randomized controlled trial with 6-month follow-up. Int. J. Clin. Pharmacol. Ther. 2018, 56, 366. [Google Scholar] [CrossRef]
- Aslani, H.; Nourbakhsh, S.T.; Zafarani, Z.; Ahmadi-Bani, M.; Ananloo, M.E.S.; Beigy, M.; Salehi, S. Platelet-rich plasma for frozen shoulder: A case report. Arch. Bone Jt. Surg. 2016, 4, 90. [Google Scholar]
- Hagiwara, Y.; Ando, A.; Onoda, Y.; Takemura, T.; Minowa, T.; Hanagata, N.; Tsuchiya, M.; Watanabe, T.; Chimoto, E.; Suda, H.; et al. Coexistence of fibrotic and chondrogenic process in the capsule of idiopathic frozen shoulders. Osteoarthr. Cartil. 2012, 20, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Morén-Hybbinette, I.; Moritz, U.; Scherstén, B. The clinical picture of the painful diabetic shoulder—Natural history, social consequences and analysis of concomitant hand syndrome. Acta Med. Scand. 1987, 221, 73–82. [Google Scholar] [CrossRef]
- Molloy, T.; Wang, Y.; Murrell, G.A. The roles of growth factors in tendon and ligament healing. Sports Med. 2003, 33, 381–394. [Google Scholar] [CrossRef]
- Ebert, J.R.; Wang, A.; Smith, A.; Nairn, R.; Breidahl, W.; Zheng, M.H.; Ackland, T. A midterm evaluation of postoperative platelet-rich plasma injections on arthroscopic supraspinatus repair: A randomized controlled trial. Am. J. Sports Med. 2017, 45, 2965–2974. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, J.H. PRP treatment effects on degenerative tendinopathy-an in vitro model study. Muscles Ligaments Tendons J. 2014, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Scarpone, M.; Rabago, D.; Snell, E.; Demeo, P.; Ruppert, K.; Pritchard, P.; Arbogast, G.; Wilson, J.J.; Balzano, J.F. Effectiveness of platelet-rich plasma injection for rotator cuff tendinopathy: A prospective open-label study. Glob. Adv. Health Med. 2013, 2, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Feusi, O.; Karol, A.; Fleischmann, T.; von Rechenberg, B.; Bouaicha, S.; Werner, C.M.; Jentzsch, T. Platelet-rich plasma as a potential prophylactic measure against frozen shoulder in an in vivo shoulder contracture model. Arch. Orthop. Trauma Surg. 2020, 142, 363–372. [Google Scholar] [CrossRef]


{kind=link}
| S.No | Author | Year | Type of Study | Country | No of Patients | Study Details | Results | Complications |
|---|---|---|---|---|---|---|---|---|
| 1. | Aslani MA et al. [7] | 2020 | Case series | Iran | 44 | First stage: one PRP injection in each subacromial bursa and intra-articular space, repeated after 4 weeks. Second stage: one PRP injection only, in the glenohumeral joint. | Significant improvement in function: 51.6% in DASH and 100% in SF-12 health-survey questionnaire. Significant reduction in pain function (p < 0.001), 67% improvement in pain. Follow-up: 25 weeks. | None |
| 2. | Barman et al. [8] | 2019 | Comparative study | India | 28 | A total of 28 patients were given single intra-articular PRP, and 27 patients given single intra-articular corticosteroid. | PRP group: reduction in VAS score and total SPADI score, compared with corticosteroid group. Significant improvement in ROM in the PRP group. Follow-up: 12 weeks. | None |
| 3. | Unlu et al. [9] | 2020 | Randomized controlled trial | Turkey | 17 | Randomized into two groups: one group was given a 2 mL PRP injection three times every two weeks, while the control group was given a saline injection Intra-articularly. The same exercises were given to both groups. | Improvement in SPADI score and ROM in the PRP group, as compared to the control group. Significant decrease in VAS score in PRP group. There is no significant difference in the use of analgesics in both groups. | None |
| 4. | Upadhyaya et al. [10] | 2020 | Randomized comparative analysis | India | 60 | Patients received a single injection, either methylprednisolone (Group II) or PRP (Group I) with 1% lidocaine. The patients were randomized into these groups. | The mean pain scale, mean disability, and total SPADI score linearly improved in the PRP group, and final scores at the final follow-up were higher, compared with the steroid group (p < 0.05). | None |
| 5. | Agarwal et al. [11] | 2019 | Case series | India | 20 | Patients were given a single 4 mL PRP injection. | At 1 month, statistically significant improvements in the constant score. A few patients had increased pain on the third day of injection, which improved with time. | None |
| 6. | Kumar et al. [12] | 2019 | Comparative study | India | 30 | Patients were divided into two groups: one received the PRP injection, whereas the other was given methylprednisolone. | A significant difference in VAS between 1 month, 2 months, and 6 months. A significant difference in VAS between 2 months and 6 months. The outcome was excellent amongst 10% of subjects, good amongst 66.67% of subjects, fair amongst 13.33% of subjects, and poor amongst 10% of patients. Both PRP and steroids showed equal effectiveness in treating frozen shoulders. | None |
| 7. | Calis et al. [13] | 2019 | Case series | Turkey | 9 | One intra-articular PRP injection was given at presentation and 2 weeks. PRP injection was given under sonography guidance. | Significant improvements in ROM (p < 0.05), VAS scores (p < 0.05) and SPADI (p < 0.05) at the follow-up of 12 weeks. | None |
| 8. | Kothari et al. [14] | 2017 | Randomized comparative study | India | 62 | Patients were divided into the A, B, and C groups, and were given corticosteroid 80 mg, PRP(2 mL), and ultrasonic therapy (seven times in 2 weeks). | PRP injection depicted better results in terms of ROM, VAS score and QuickDASH score during the corticosteroid and ultrasonic therapy. Follow-up: 12 weeks. | None |
| 9. | Jeyaraman et al. [15] | 2018 | Comparative study | India | 46 | Group A: given 3 mL PRP intra-articularly. Group B: hydro-dissection (20 mL normal saline + 5 ml lignocaine) intra-articularly. | PRP group showed improved functional quality of life. Significant improvement in ROM (DASH score p < 0.01) and decrease in VAS score (p < 0.01). | None |
| 10. | Lin et al. [16] | 2018 | Randomized control trial | China | 30 | Group 1: 2 mL PRP intra-articularly. Group 2: Procaine injection intra-articularly. | VAS score decreased in both groups till 3 months but continued to decline in the PRP group whereas increased in the procaine group. The functional improvement (UCLA score) improved in the PRP group. | None |
| 11. | Aslani H et al. [17] | 2016 | Case report | Iran | 1 | PRP injections are given in the seventh and eighth month after the start of symptoms. | After the first injection: improvement was seen regarding diurnal shoulder pain and night pain. Improvement in ROM and function. | None |
| S.No | Author | Year | PRP System Used | Type of PRP Used | Spin Technique |
|---|---|---|---|---|---|
| 1. | Aslani M A et al. [7] | 2020 | Arthrex-ACP system | Not specified | 1500 rpm for 5 min |
| 2. | Barman et al. [8] | 2019 | Plasmamed PRP Kit | Not specified | 1800 rpm for 14 min |
| 3. | Unlu et al. [9] | 2020 | Manual method | Not specified | 1200 g for 5 min |
| 4. | Upadhyaya et al. [10] | 2020 | Manual method | Not specified | 1500 rpm for 15 min |
| 5. | Agarwal et al. [11] | 2019 | Manual method | LR-PRP | Not specified |
| 6. | Kumar et al. [12] | 2019 | Not specified | Not specified | Not specified |
| 7. | Calis et al. [13] | 2019 | Manual method | LP-PRP | 1195 rpm for 20 min followed by 1890 rpm for 15 min |
| 8. | Kothari et al. [14] | 2017 | Manual method | Not specified | Not specified |
| 9. | Jeyaraman et al. [15] | 2018 | Manual method | Not specified | 3000 rpm for 10 min followed by 5000 rpm for 10 min |
| 10. | Lin et al. [16] | 2018 | Manual method | Not specified | Not specified |
| 11. | Aslani H et al. [17] | 2016 | Arthrex-ACP system | Not specified | 5000 rpm for 5 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harna, B.; Gupta, V.; Arya, S.; Jeyaraman, N.; Rajendran, R.L.; Jeyaraman, M.; Gangadaran, P.; Khanna, M.; Hong, C.M.; Ahn, B.-C. Current Role of Intra-Articular Injections of Platelet-Rich Plasma in Adhesive Capsulitis of Shoulder: A Systematic Review. Bioengineering 2023, 10, 21. https://doi.org/10.3390/bioengineering10010021
Harna B, Gupta V, Arya S, Jeyaraman N, Rajendran RL, Jeyaraman M, Gangadaran P, Khanna M, Hong CM, Ahn B-C. Current Role of Intra-Articular Injections of Platelet-Rich Plasma in Adhesive Capsulitis of Shoulder: A Systematic Review. Bioengineering. 2023; 10(1):21. https://doi.org/10.3390/bioengineering10010021
Chicago/Turabian StyleHarna, Bushu, Vijay Gupta, Shivali Arya, Naveen Jeyaraman, Ramya Lakshmi Rajendran, Madhan Jeyaraman, Prakash Gangadaran, Manish Khanna, Chae Moon Hong, and Byeong-Cheol Ahn. 2023. "Current Role of Intra-Articular Injections of Platelet-Rich Plasma in Adhesive Capsulitis of Shoulder: A Systematic Review" Bioengineering 10, no. 1: 21. https://doi.org/10.3390/bioengineering10010021
APA StyleHarna, B., Gupta, V., Arya, S., Jeyaraman, N., Rajendran, R. L., Jeyaraman, M., Gangadaran, P., Khanna, M., Hong, C. M., & Ahn, B.-C. (2023). Current Role of Intra-Articular Injections of Platelet-Rich Plasma in Adhesive Capsulitis of Shoulder: A Systematic Review. Bioengineering, 10(1), 21. https://doi.org/10.3390/bioengineering10010021