
Urinary Polycyclic Aromatic Hydrocarbon Metabolites Are Associated with Biomarkers of Chronic Endocrine Stress, Oxidative Stress, and Inflammation in Adolescents: FLEHS-4 (2016–2020)

 , , , , , ,
, , , , , ,  , , ,
, , ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Analysis of Urinary PAH Metabolites and Urinary Specific Gravity
2.4. Analysis of 8-oxo-7,8-dihydro-2’-deoxyguanosine (8-oxodG) in Urine
2.5. Hair Sample Collection and Hair Cortisol Measurement
2.6. Total and Differential Leucocyte Count in Peripheral Blood
2.7. Statistical Analysis
3. Results
3.1. Study Population Characteristics
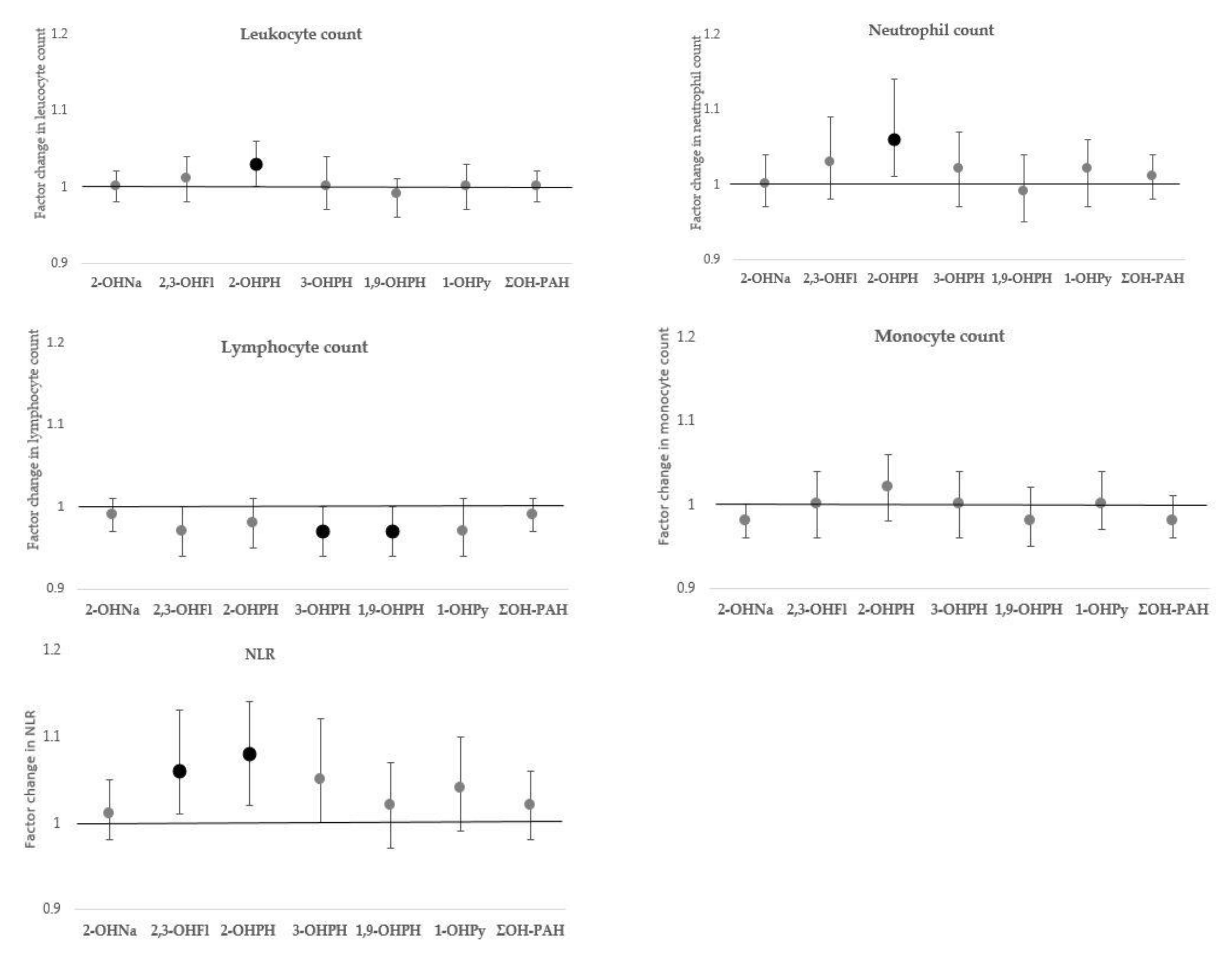
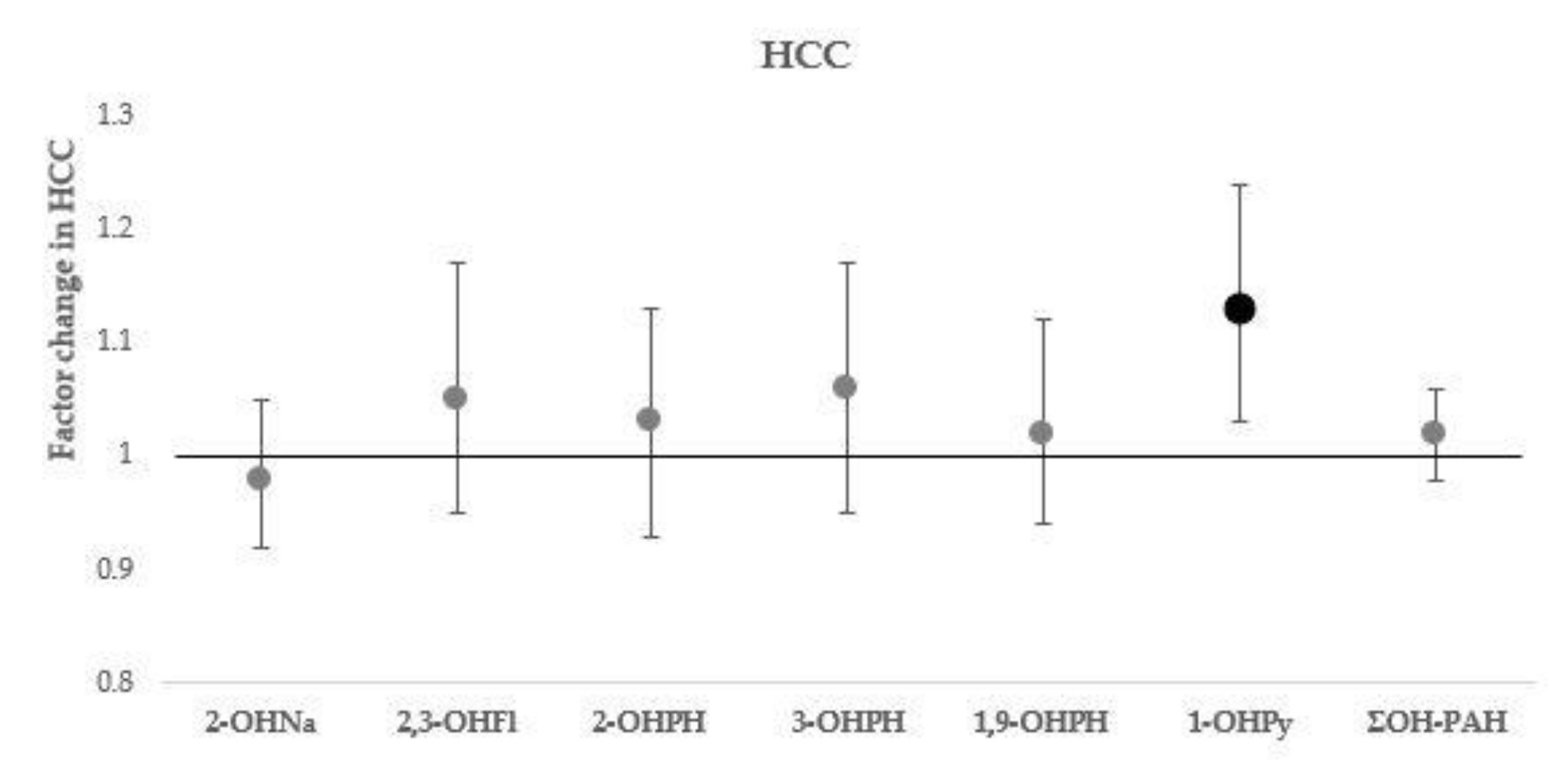
3.2. Associations between OH-PAHs and Effect Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vondráček, J.; Pivnička, J.; Machala, M. Polycyclic aromatic hydrocarbons and disruption of steroid signaling. Curr. Opin. Toxicol. 2018, 11–12, 27–34. [Google Scholar] [CrossRef]
- Zhang, H.; Han, Y.; Qiu, X.; Wang, Y.; Li, W.; Liu, J.; Chen, X.; Li, R.; Xu, F.; Chen, W.; et al. Association of internal exposure to polycyclic aromatic hydrocarbons with inflammation and oxidative stress in prediabetic and healthy individuals. Chemosphere 2020, 253, 126748. [Google Scholar] [CrossRef]
- Polanska, K.; Dettbarn, G.; Jurewicz, J.; Sobala, W.; Magnus, P.; Seidel, A.; Hanke, W. Effect of prenatal polycyclic aromatic hydrocarbons exposure on birth outcomes: The polish mother and child cohort study. Biomed Res. Int. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Murawski, A.; Roth, A.; Schwedler, G.; Schmied-Tobies, M.I.H.; Rucic, E.; Pluym, N.; Scherer, M.; Scherer, G.; Conrad, A.; Kolossa-Gehring, M. Polycyclic aromatic hydrocarbons (PAH) in urine of children and adolescents in Germany—Human biomonitoring results of the German Environmental Survey 2014–2017 (GerES V). Int. J. Hyg. Environ. Health 2020, 226, 113491. [Google Scholar] [CrossRef]
- Abdel-Shafy, H.I.; Mansour, M.S.M. A review on polycyclic aromatic hydrocarbons: Source, environmental impact, effect on human health and remediation. Egypt. J. Pet. 2016, 25, 107–123. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Deng, X.; Li, W.; Liu, S.; Chen, Y.; Yang, B.; Liu, Q. Internal exposure levels of polycyclic aromatic hydrocarbons in children and adolescents: A systematic review and meta-analysis. Environ. Health Prev. Med. 2019, 24, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Moorthy, B.; Chu, C.; Carlin, D.J. Polycyclic aromatic hydrocarbons: From metabolism to lung cancer. Toxicol. Sci. 2015, 1, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rengarajan, T.; Rajendran, P.; Nandakumar, N.; Lokeshkumar, B.; Rajendran, P.; Nishigaki, I. Exposure to polycyclic aromatic hydrocarbons with special focus on cancer. Asian Pac. J. Trop. Biomed. 2015, 5, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Kataria, A.; Trasande, L.; Trachtman, H. The effects of environmental chemicals on renal function. Nat. Rev. Nephrol. 2015, 11, 610–625. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Jahan, S.A.; Kabir, E.; Brown, R.J.C. A review of airborne polycyclic aromatic hydrocarbons (PAHs) and their human health effects. Environ. Int. 2013, 60, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.S.; Vuong, A.M.; Dietrich, K.N.; Chen, A. Proximity to traffic and exposure to polycyclic aromatic hydrocarbons in relation to Attention Deficit Hyperactivity Disorder and conduct disorder in U.S. children. Int. J. Hyg. Environ. Health 2021, 232. [Google Scholar] [CrossRef] [PubMed]
- Wang, I.J.; Karmaus, W.J.J.; Yang, C.C. Polycyclic aromatic hydrocarbons exposure, oxidative stress, and asthma in children. Int. Arch. Occup. Environ. Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Farzan, S.F.; Chen, Y.; Trachtman, H.; Trasande, L. Urinary polycyclic aromatic hydrocarbons and measures of oxidative stress, inflammation and renal function in adolescents: NHANES 2003-2008. Environ. Res. 2016, 144, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, M.; Slezakova, K.; Delerue-Matos, C.; Pereira, M.C.; Morais, S. Children environmental exposure to particulate matter and polycyclic aromatic hydrocarbons and biomonitoring in school environments: A review on indoor and outdoor exposure levels, major sources and health impacts. Environ. Int. 2019, 124, 180–204. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, K.K.; McElrath, T.F.; Pace, G.G.; Weller, D.; Zeng, L.; Pennathur, S.; Cantonwine, D.E.; Meeker, J.D. Urinary Polycyclic Aromatic Hydrocarbon Metabolite Associations with Biomarkers of Inflammation, Angiogenesis, and Oxidative Stress in Pregnant Women. Environ. Sci. Technol. 2017, 51, 4652–4660. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.; Pan, X.C.; Kim, S.Y.; Park, K.; Kim, Y.H.; Kim, H.; Hong, Y.C. Exposures to particulate matter and polycyclic aromatic hydrocarbons and oxidative stress in schoolchildren. Environ. Health Perspect. 2010, 118, 579–586. [Google Scholar] [CrossRef] [Green Version]
- Koppen, G.; Franken, C.; Den Hond, E.; Plusquin, M.; Reimann, B.; Leermakers, M.; Covaci, A.; Nawrot, T.; Van Larebeke, N.; Schoeters, G.; et al. Pooled analysis of genotoxicity markers in relation to exposure in the Flemish Environment and Health Studies (FLEHS) between 1999 and 2018. Environ. Res. 2020, 190, 110002. [Google Scholar] [CrossRef]
- Lu, S.-Y.; Li, Y.-X.; Zhang, J.-Q.; Zhang, T.; Liu, G.-H.; Huang, M.-Z.; Li, X.; Ruan, J.-J.; Kannan, K.; Qiu, R.-L. Associations between polycyclic aromatic hydrocarbon (PAH) exposure and oxidative stress in people living near e-waste recycling facilities in China. Environ. Int. 2016, 94, 161–169. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, Y.; Liu, W.; Schlenk, D.; Liu, J. Glucocorticoid and mineralocorticoid receptors and corticosteroid homeostasis are potential targets for endocrine-disrupting chemicals. Environ. Int. 2019, 133, 105133. [Google Scholar] [CrossRef]
- Odermatt, A.; Gumy, C. Glucocorticoid and mineralocorticoid action: Why should we consider influences by environmental chemicals? Biochem. Pharmacol. 2008, 76, 1184–1193. [Google Scholar] [CrossRef]
- Thomson, E.M.; Filiatreault, A.; Guénette, J. Stress hormones as potential mediators of air pollutant effects on the brain: Rapid induction of glucocorticoid-responsive genes. Environ. Res. 2019, 178, 108717. [Google Scholar] [CrossRef]
- Chrousos, G.P. Stress and disorders of the stress system. Nat. Rev. Endocrinol. 2009, 5, 374–381. [Google Scholar] [CrossRef]
- Brenhouse, H.C.; Schwarz, J.M. Immunoadolescence: Neuroimmune development and adolescent behavior. Neurosci. Biobehav. Rev. 2016, 70, 288–299. [Google Scholar] [CrossRef] [Green Version]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell. Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef] [Green Version]
- Şimşek, Ş.; Yüksel, T.; Kaplan, İ.; Uysal, C.; Aktaş, H. The levels of cortisol and oxidative stress and DNA damage in child and adolescent victims of sexual abuse with or without post-traumatic stress disorder. Psychiatry Investig. 2016, 13, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Golub, M.S. Adolescent health and the environment. Environ. Health Perspect. 2000, 108, 355. [Google Scholar] [CrossRef]
- Sheth, C.; McGlade, E.; Yurgelun-Todd, D. Chronic Stress in Adolescents and Its Neurobiological and Psychopathological Consequences: An RDoC Perspective. Chronic Stress 2017, 1, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Kim, E.; Choi, M.H. Technical and clinical aspects of cortisol as a biochemical marker of chronic stress. BMB Rep. 2015, 48, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abell, J.G.; Stalder, T.; Ferrie, J.E.; Shipley, M.J.; Kirschbaum, C.; Kivimäki, M.; Kumari, M. Assessing cortisol from hair samples in a large observational cohort: The Whitehall II study. Psychoneuroendocrinology 2016, 73, 148–156. [Google Scholar] [CrossRef] [Green Version]
- Gray, N.A.; Dhana, A.; Van Der Vyver, L.; Van Wyk, J.; Khumalo, N.P.; Stein, D.J. Determinants of hair cortisol concentration in children: A systematic review. Psychoneuroendocrinology 2018, 87, 204–214. [Google Scholar] [CrossRef]
- Wosu, A.C.; Valdimarsdóttir, U.; Shields, A.E.; Williams, D.R.; Williams, M.A. Correlates of cortisol in human hair: Implications for epidemiologic studies on health effects of chronic stress. Ann. Epidemiol. 2013, 23, 797–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-related and basic determinants of hair cortisol in humans: A meta-analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef]
- Davenport, M.D.; Tiefenbacher, S.; Lutz, C.K.; Novak, M.A.; Meyer, J.S. Analysis of endogenous cortisol concentrations in the hair of rhesus macaques. Gen. Comp. Endocrinol. 2006, 147, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Heimbürge, S.; Kanitz, E.; Otten, W. The use of hair cortisol for the assessment of stress in animals. Gen. Comp. Endocrinol. 2019, 270, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Manenschijn, L.; Koper, J.W.; Lamberts, S.W.J.; Van Rossum, E.F.C. Evaluation of a method to measure long term cortisol levels. Steroids 2011, 76, 1032–1036. [Google Scholar] [CrossRef]
- Vozarova, B.; Weyer, C.; Lindsay, R.S.; Pratley, R.E.; Bogardus, C.; Antonio Tataranni, P. High white blood cell count is associated with a worsening of insulin sensitivity and predicts the development of type 2 diabetes. Diabetes 2002, 51, 455–461. [Google Scholar] [CrossRef] [Green Version]
- Poursafa, P.; Kelishadi, R.; Amini, A.; Amini, A.; Amin, M.M.; Lahijanzadeh, M.; Modaresi, M. Association of air pollution and hematologic parameters in children and adolescents. J. Pediatr. 2011, 87, 350–356. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Liu, Q.; Liang, J.; Weng, Z.; Xu, J.; Jiang, Z.; Gu, A. Urinary biomarkers of polycyclic aromatic hydrocarbons and their associations with liver function in adolescents. Environ. Pollut. 2021, 278, 116842. [Google Scholar] [CrossRef]
- Oulhote, Y.; Shamim, Z.; Kielsen, K.; Weihe, P.; Grandjean, P.; Ryder, L.P.; Heilmann, C. Children’s white blood cell counts in relation to developmental exposures to methylmercury and persistent organic pollutants. Reprod. Toxicol. 2017, 68, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Afari, M.E.; Bhat, T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: An update. Expert Rev. Cardiovasc. Ther. 2016, 14, 573–577. [Google Scholar] [CrossRef]
- Gao, X.; Coull, B.; Lin, X.; Vokonas, P.; Sparrow, D.; Hou, L.; DeMeo, D.L.; Litonjua, A.A.; Schwartz, J.; Baccarelli, A.A. Association of Neutrophil to Lymphocyte Ratio With Pulmonary Function in a 30-Year Longitudinal Study of US Veterans. JAMA Netw. Open 2020, 3, e2010350. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki. Ethical principles for medical research involving human subjects. Bull. World Health Organ. 2001, 79(4), 373–374. [Google Scholar]
- Roelants, M.; Hauspie, R.; Hoppenbrouwers, K. References for growth and pubertal development from birth to 21 years in Flanders, Belgium. Ann. Hum. Biol. 2009, 36, 680–694. [Google Scholar] [CrossRef]
- Hofmann, M.; Young, C.; Binz, T.M.; Baumgartner, M.R.; Bauer, N. Contact to nature benefits health: Mixed effectiveness of different mechanisms. Int. J. Environ. Res. Public Health 2018, 15, 31. [Google Scholar] [CrossRef] [Green Version]
- Verheyen, V.J.; Remy, S.; Lambrechts, N.; Govarts, E.; Colles, A.; Poelmans, L.; Verachtert, E.; Lefebvre, W.; Monsieurs, P.; Vanpoucke, C.; et al. Residential exposure to air pollution and access to neighborhood greenspace in relation to hair cortisol concentrations during the second and third trimester of pregnancy. Environ. Health 2021, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Standards & Technology Standard. Reference Material 3672: Organic Contaminants in Smokers’ Urine. 2020; pp. 1–6. Available online: https://www-s.nist.gov/srmors/certificates/3672.pdf (accessed on 24 September 2021).
- Esteban López, M.; Göen, T.; Mol, H.; Nübler, S.; Haji-Abbas-Zarrabi, K.; Koch, H.M.; Kasper-Sonnenberg, M.; Dvorakova, D.; Hajslova, J.; Antignac, J.P.; et al. The European human biomonitoring platform - Design and implementation of a laboratory quality assurance/quality control (QA/QC) programme for selected priority chemicals. Int. J. Hyg. Environ. Health 2021, 234, 113740. [Google Scholar] [CrossRef] [PubMed]
- Toyokuni, S.; Tanaka, T.; Hattori, Y.; Nishiyama, Y.; Yoshida, A.; Uchida, K.; Hiai, H.; Ochi, H.; Osawa, T. Quantitative immunohistochemical determination of 8-hydroxy-2’- deoxyguanosine by a monoclonal antibody N45.1: Its application to ferric nitrilotriacetate-induced renal carcinogenesis model. Lab. Investig. 1997, 3, 365–374. [Google Scholar]
- Barregard, L.; Møller, P.; Henriksen, T.; Mistry, V.; Koppen, G.; Rossner, P.; Sram, R.; Weimann, A.; Poulsen, H.; Nataf, R.; et al. Human and methodological sources of variability in the measurement of urinary 8-oxo-7,8-dihydro-2’-deoxyguanosine. Antioxid. Redox Signal. 2013, 18, 2377–2391. [Google Scholar] [CrossRef] [PubMed]
- Greff, M.J.E.; Levine, J.M.; Abuzgaia, A.M.; Elzagallaai, A.A.; Rieder, M.J.; van Uum, S.H.M. Hair cortisol analysis: An update on methodological considerations and clinical applications. Clin. Biochem. 2019, 63, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nakul-Aquaronne, D.; Sudaka-Sammarcelli, I.; Ferrero-Vacher, C.; Starck, B.; Bayle, J. Evaluation of the Sysmex Xe-2100® hematology analyzer in hospital use. J. Clin. Lab. Anal. 2003, 17, 113–123. [Google Scholar] [CrossRef]
- Lubin, J.H.; Colt, J.S.; Camann, D.; Davis, S.; Cerhan, J.R.; Severson, R.K.; Bernstein, L.; Hartge, P. Epidemiologic Evaluation of Measurement Data in the Presence of Detection Limits. Environ. Health Perspect. 2004, 112, 1691. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.A.; Lu, C.; Schmotzer, B.J.; Waller, L.A.; Riederer, A.M. Evaluation of physiological measures for correcting variation in urinary output: Implications for assessing environmental chemical exposure in children. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 336–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.P.; Mehta, S.S.; White, A.J.; Niehoff, N.M.; Arroyave, W.D.; Wang, A.; Lunn, R.M. Urinary polycyclic aromatic hydrocarbon metabolites and mortality in the United States: A prospective analysis. PLoS ONE 2021, 16, e0252719. [Google Scholar] [CrossRef] [PubMed]
- De Craemer, S.; Croes, K.; van Larebeke, N.; Sioen, I.; Schoeters, G.; Loots, I.; Nawrot, T.; Nelen, V.; Campo, L.; Fustinoni, S.; et al. Investigating unmetabolized polycyclic aromatic hydrocarbons in adolescents’ urine as biomarkers of environmental exposure. Chemosphere 2016, 155, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Liu, Y.; Chen, Z.; Zhang, J.; Deng, H.; Gu, J. Interaction effects of life events and hair cortisol on perceived stress, anxiety, and depressive symptoms among Chinese adolescents: Testing the differential susceptibility and diathesis-stress models. Front. Psychol. 2019, 10, 297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penz, M.; Kirschbaum, C.; Buske-Kirschbaum, A.; Wekenborg, M.K.; Miller, R. Stressful life events predict one-year change of leukocyte composition in peripheral blood. Psychoneuroendocrinology 2018, 94, 17–24. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.M.; Upson, K.; Cook, N.R.; Weinberg, C.R. Environmental chemicals in urine and blood: Improving methods for creatinine and lipid adjustment. Environ. Health Perspect. 2016, 124, 220–227. [Google Scholar] [CrossRef]
- De Coster, S.; van Leeuwen, D.M.; Jennen, D.G.J.; Koppen, G.; Den Hond, E.; Nelen, V.; Schoeters, G.; Baeyens, W.; van Delft, J.H.M.; Kleinjans, J.C.S.; et al. Gender-specific transcriptomic response to environmental exposure in flemish adults. Environ. Mol. Mutagen. 2013, 54, 574–588. [Google Scholar] [CrossRef]
- Robert, S.A. SOCIOECONOMIC POSITION AND HEALTH: The Independent Contribution of Community Socioeconomic Context. Annu. Rev. Sociol. 1999, 25, 489–516. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regession Approach; Guilford Publ.: New York, NY, USA, 2018. [Google Scholar]
- Kindengezin Kansarmoede. 2018. Available online: https://www.statistiekvlaanderen.be/kansarmoede-index-van-kind-en-gezin (accessed on 5 April 2021).
- Steunpunt Milieu en Gezondheid Vlaamse Humane-Biomonitoringprogramma 2016–2020: Referentiewaarden Bij Jongeren. 2020. Available online: https://www.milieu-en-gezondheid.be/nl/onderzoeksresultaten (accessed on 3 February 2021).
- Schultz, T.W.; Sinks, G.D. Xenoestrogenic gene expression: Structural features of active polycyclic aromatic hydrocarbons. Environ. Toxicol. Chem. 2002, 21, 783–786. [Google Scholar] [CrossRef]
- Jaillon, S.; Berthenet, K.; Garlanda, C. Sexual Dimorphism in Innate Immunity. Clin. Rev. Allergy Immunol. 2017 563 2017, 56, 308–321. [Google Scholar] [CrossRef]
- Alshaarawy, O.; Zhu, M.; Ducatman, A.; Conway, B.; Andrew, M.E. Polycyclic aromatic hydrocarbon biomarkers and serum markers of inflammation. A positive association that is more evident in men. Environ. Res. 2013, 126, 98–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.L.; Moutinho, V.; Panageas, K.S.; Coit, D.G. A peripheral blood biomarker estimates probability of survival: The neutrophil-lymphocyte ratio in noncancer patients. Biomark. Med. 2016, 10, 953–957. [Google Scholar] [CrossRef] [Green Version]
- Furuta, C.; Noda, S.; Li, C.M.; Suzuki, A.K.; Taneda, S.; Watanabe, G.; Taya, K. Nitrophenols isolated from diesel exhaust particles regulate steroidogenic gene expression and steroid synthesis in the human H295R adrenocortical cell line. Toxicol. Appl. Pharmacol. 2008, 229, 109–120. [Google Scholar] [CrossRef]
- Schug, T.T.; Blawas, A.M.; Gray, K.; Heindel, J.J.; Lawler, C.P. Elucidating the links between endocrine disruptors and neurodevelopment. Endocrinology 2015, 156, 1941–1951. [Google Scholar] [CrossRef] [PubMed]
- John, C.D.; Buckingham, J.C. Cytokines: Regulation of the hypothalamo-pituitary-adrenocortical axis. Curr. Opin. Pharmacol. 2003, 3, 78–84. [Google Scholar] [CrossRef]
- Mortamais, M.; Pujol, J.; van Drooge, B.L.; Macià, D.; Martínez-Vilavella, G.; Reynes, C.; Sabatier, R.; Rivas, I.; Grimalt, J.; Forns, J.; et al. Effect of exposure to polycyclic aromatic hydrocarbons on basal ganglia and attention-deficit hyperactivity disorder symptoms in primary school children. Environ. Int. 2017, 105, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerlofs-Nijland, M.E.; Boere, A.J.F.; Leseman, D.L.; Dormans, J.A.; Sandström, T.; Salonen, R.O.; van Bree, L.; Cassee, F.R. Effects of particulate matter on the pulmonary and vascular system: Time course in spontaneously hypertensive rats. Part. Fibre Toxicol. 2005, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Thomson, E.M.; Vladisavljevic, D.; Mohottalage, S.; Kumarathasan, P.; Vincent, R. Mapping acute systemic effects of inhaled particulate matter and ozone: Multiorgan gene expression and glucocorticoid activity. Toxicol. Sci. 2013, 135, 169–181. [Google Scholar] [CrossRef] [Green Version]
- Schoeters, G.; Den Hond, E.; Colles, A.; Loots, I.; Morrens, B.; Keune, H.; Bruckers, L.; Nawrot, T.; Sioen, I.; De Coster, S.; et al. Concept of the Flemish human biomonitoring programme. Int. J. Hyg. Environ. Health 2012, 215, 102–108. [Google Scholar] [CrossRef]
- Scinicariello, F.; Buser, M.C. Urinary polycyclic aromatic hydrocarbons and childhood obesity: NHANES (2001–2006). Environ. Health Perspect. 2014, 122, 299–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Air Quality Guidelines for Europe. Chapter 5.9 Polycyclic Aromatic Hydrocarbons (PAHs), 2nd ed.; WHO Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Buekers, J.; Dons, E.; Elen, B.; Panis, I. Health impact model for modal shift from car use to cycling or walking in Flanders: Application to two bicycle highways. J. Transp. Health 2015, 2, 1–14. [Google Scholar] [CrossRef]
- Flanders Environment Agency. Jaarrapport Lucht – Emissies en concentraties van luchtverontreinigende stoffen. 2020. Available online: https://www.vmm.be/publicaties/lucht-2020/emissies-en-concentraties-luchtverontreinigende-stoffen (accessed on 24 November 2020).
- Bushnik, T.; Wong, S.L.; Holloway, A.C.; Thomson, E.M. Association of urinary polycyclic aromatic hydrocarbons and obesity in children aged 3–18: Canadian Health Measures Survey 2009–2015. J. Dev. Orig. Health Dis. 2020, 11, 623–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomasetig, F.; Tebby, C.; Graillot, V.; Zeman, F.; Pery, A.; Cravedi, J.P.; Audebert, M. Comparative genotoxic potential of 27 polycyclic aromatic hydrocarbons in three human cell lines. Toxicol. Lett. 2020, 326, 99–105. [Google Scholar] [CrossRef]
- Nisbet, I.C.T.; LaGoy, P.K. Toxic equivalency factors (TEFs) for polycyclic aromatic hydrocarbons (PAHs). Regul. Toxicol. Pharmacol. 1992, 16, 290–300. [Google Scholar] [CrossRef]
- EFSA Polycyclic Aromatic Hydrocarbons in Food - Scientific Opinion of the Panel on Contaminants in the Food Chain. EFSA J. 2008, 6, 1–114. [CrossRef]
- Jung, K.H.; Liu, B.; Lovinsky-Desir, S.; Yan, B.; Camann, D.; Sjodin, A.; Li, Z.; Perera, F.; Kinney, P.; Chillrud, S.; et al. Time trends of polycyclic aromatic hydrocarbon exposure in New York city from 2001 to 2012: Assessed by repeat air and urine samples. Environ. Res. 2014, 131, 95–103. [Google Scholar] [CrossRef] [Green Version]
- Health Canada, Results of the Canadian Health Measures Survey Cycle 4 (2014–2015). 2017. Available online: https://www.canada.ca/en/health-canada/services/environmental-workplace-health/reports-publications/environmental-contaminants/fourth-report-human-biomonitoring-environmental-chemicals-canada.html (accessed on 3 September 2020).
- Sunyer, J.; Muñoz, A.; Peng, Y.; Margolick, J.; Chmiel, J.S.; Oishi, J.; Kingsley, L.; Samet, J.M. Longitudinal relation between smoking and white blood cells. Am. J. Epidemiol. 1996, 144, 734–741. [Google Scholar] [CrossRef] [Green Version]
- Di Lorenzo, L.; Silvestroni, A.; Martino, M.G.; Gagliardi, T.; Corfiati, M.; Soleo, L. Evaluation of peripheral blood neutrophil leucocytes in lead-exposed workers. Int. Arch. Occup. Environ. Health 2006, 79, 491–498. [Google Scholar] [CrossRef]
- Kumar, J.; Lind, P.M.; Salihovic, S.; Van Bavel, B.; Ingelsson, E.; Lind, L. Persistent Organic Pollutants and Inflammatory Markers in a Cross-Sectional Study of Elderly Swedish People: The PIVUS Cohort. Environ. Health Perspect. 2014, 122, 977–983. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.C.; Schwartz, J. Metabolic syndrome and inflammatory responses to long-term particulate air pollutants. Environ. Health Perspect. 2008, 116, 612–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 393) | % | Boys (n = 183) | % | Girls (n = 210) | % | p-Value |
|---|---|---|---|---|---|---|---|
| Age (years) | 0.855 | ||||||
| <14.5 | 103 | 26.2 | 46 | 25.1 | 57 | 27.1 | |
| 14.5−15.5 | 258 | 65.6 | 121 | 66.1 | 137 | 65.2 | |
| >15.5 | 32 | 8.1 | 16 | 8.7 | 16 | 7.6 | |
| Perceived income adequacy | 0.668 | ||||||
| Difficult | 111 | 28.2 | 53 | 29 | 58 | 27.6 | |
| Rather easy | 125 | 31.8 | 61 | 33.3 | 64 | 30.5 | |
| Easy–very easy | 151 | 38.4 | 66 | 36.1 | 85 | 40.5 | |
| Missing | 6 | 1.5 | 3 | 1.6 | 3 | 1.4 | |
| Area Deprivation Index | 0.180 | ||||||
| 0−5.3% | 94 | 23.9 | 40 | 21.9 | 54 | 25.7 | |
| 5.4−9.3% | 99 | 25.2 | 41 | 22.4 | 58 | 27.6 | |
| 9.4−15.5% | 101 | 25.7 | 47 | 25.6 | 54 | 25.7 | |
| >15.5% | 99 | 25.2 | 55 | 30.1 | 44 | 21 | |
| Body Mass Index a | 0.053 | ||||||
| Underweight | 32 | 8.1 | 15 | 8.2 | 17 | 8.1 | |
| Normal weight | 285 | 72.5 | 142 | 77.6 | 143 | 68.1 | |
| Overweight, obese | 76 | 19.3 | 26 | 14.2 | 50 | 23.8 | |
| Smoking | 0.427 | ||||||
| No | 374 | 95.2 | 172 | 94 | 202 | 96.2 | |
| Yes | 18 | 4.6 | 10 | 5.5 | 8 | 3.8 | |
| Missing | 1 | 0.3 | 1 | 0.5 | 0 | 0 | |
| Residential exposure to ETS | 0.809 | ||||||
| No | 351 | 89.3 | 165 | 90.2 | 186 | 88.6 | |
| Yes | 40 | 10.2 | 18 | 9.8 | 22 | 10.5 | |
| Missing | 2 | 0.5 | 0 | 0 | 2 | 1 | |
| Recent health complaints | 0.297 | ||||||
| No | 277 | 70.5 | 134 | 73.2 | 143 | 68.1 | |
| Yes | 115 | 29.3 | 49 | 26.8 | 66 | 31.4 | |
| Missing | 1 | 0.3 | 0 | 0 | 1 | 0.5 | |
| Season of sampling | 0.001 | ||||||
| Winter | 123 | 31.3 | 48 | 26.2 | 75 | 35.7 | |
| Spring | 180 | 45.8 | 110 | 60.1 | 70 | 33.3 | |
| Summer | - | - | - | - | - | - | |
| Fall | 90 | 22.9 | 25 | 13.7 | 65 | 31 | |
| 2-day mean temperature (°C) | 0.001 | ||||||
| <6 | 145 | 36.9 | 51 | 27.9 | 94 | 44.8 | |
| 6−12 | 137 | 34.9 | 58 | 31.7 | 79 | 37.6 | |
| >12 | 111 | 28.2 | 74 | 40.4 | 37 | 17.6 |
| Biomarker | All (n = 393) | Boys (n = 183) | Girls (n = 210) | |||
|---|---|---|---|---|---|---|
| GM (95% CI) | p25 | p75 | GM (95% CI) | GM (95% CI) | p-Value | |
| OH-PAHs (µg/L) a | ||||||
| 2-OHNa * | 4.04 (3.70, 4.41) | 2.15 | 7.07 | 3.48 (3.07, 3.95) | 4.60 (4.08, 5.18) | 0.002 |
| 2,3-OHFl * | 0.209 (0.197, 0.221) | 0.144 | 0.277 | 0.207 (0.190, 0.224) | 0.211 (0.195, 0.228) | 0.743 |
| 2-OHPH | 0.074 (0.069, 0.078) | 0.051 | 0.101 | 0.078 (0.072, 0.085) | 0.070 (0.065, 0.076) | 0.06 |
| 3-OHPH | 0.073 (0.069, 0.078) | 0.052 | 0.099 | 0.077 (0.071, 0.084) | 0.070 (0.065, 0.075) | 0.056 |
| 1,9-OHPH | 0.111 (0.104, 0.118) | 0.074 | 0.149 | 0.107 (0.098, 0.116) | 0.115 (0.105, 0.126) | 0.252 |
| 1-OHPy ** | 0.067 (0.063, 0.074) | 0.048 | 0.096 | 0.065 (0.060, 0.071) | 0.069 (0.063, 0.074) | 0.342 |
| ΣOH-PAH (µmol/L) a,** | 0.032 (0.029, 0.035) | 0.018 | 0.052 | 0.028 (0.025, 0.032) | 0.036 (0.032, 0.040) | 0.004 |
| Effect biomarkers | ||||||
| HCC (pg/mg hair) | 3.07 (2.84, 3.31) | 2.09 | 4.38 | 2.85 (2.55, 3.19) | 3.26 (2.94, 3.62) | 0.083 |
| Leucocytes (cells/µL) | 6744 (6583, 6910) | 5675 | 7925 | 6471 (6236, 6715) | 6991 (6775, 7215) | 0.002 |
| Neutrophils (cells/µL) | 3535 (3403, 3672) | 2757 | 4636 | 3186 (3016, 3366) | 3870 (3682, 4068) | 0.002 |
| Lymphocytes (cells/µL) | 2250 (2195, 2307) | 1941 | 2627 | 2297 (2216, 2381) | 2210 (2136, 2287) | 0.124 |
| Monocytes (cells/µL) | 562 (546, 579) | 458 | 692 | 570 (547, 594) | 555 (533, 578) | 0.373 |
| NLR | 1.57 (1.50, 1.64) | 1.19 | 2.1 | 1.39 (1.31, 1.47) | 1.75 (1.65, 1.86) | <0.001 |
| 8-oxodG (µg/L) a | 16.90 (16.19, 17.65) | 13.41 | 21.43 | 16.80 (15.85, 17.80) | 17.00 (15.95, 18.10) | 0.790 |
| OH-PAHs | Model I | Model II | Model III | |||
|---|---|---|---|---|---|---|
| n | β (95% CI) | n | β (95% CI) | n | β (95% CI) | |
| 2-OHNa | 392 | 1.00 (0.94, 1.06) | 386 | 0.98 (0.92, 1.05) | 384 | 0.98 (0.92, 1.05) |
| 2,3-OHFl | 392 | 1.08 (0.98, 1.18) | 386 | 1.05 (0.95, 1.15) | 384 | 1.05 (0.95, 1.17) |
| 2-OHPH | 393 | 1.05 (0.96, 1.15) | 387 | 1.01 (0.92, 1.12) | 385 | 1.03 (0.93, 1.13) |
| 3-OHPH | 393 | 1.06 (0.96, 1.17) | 387 | 1.05 (0.95, 1.16) | 385 | 1.06 (0.95, 1.17) |
| 1,9-OHPH | 393 | 1.03 (0.95, 1.12) | 387 | 1.01 (0.93, 1.10) | 385 | 1.02 (0.94, 1.12) |
| 1-OHPy | 391 | 1.12 (1.02, 1.23) | 385 | 1.12 (1.02, 1.23) | 383 | 1.13 (1.03, 1.24) |
| ΣOH-PAH | 391 | 1.02 (0.98, 1.06) | 385 | 1.02 (0.98, 1.06) | 383 | 1.02 (0.98, 1.06) |
| OH-PAHs | Model I | Model II | Model III | |||
|---|---|---|---|---|---|---|
| n | β (95% CI) | n | β (95% CI) | n | β (95% CI) | |
| Leukocytes | ||||||
| 2-OHNa | 392 | 1.00 (0.98, 1.02) | 386 | 1.00 (0.98, 1.02) | 384 | 1.00 (0.98, 1.02) |
| 2,3-OHFl | 392 | 1.02 (0.99, 1.05) | 386 | 1.01 (0.98, 1.05) | 384 | 1.01 (0.98, 1.04) |
| 2-OHPH | 393 | 1.03 (1.00 1.07) | 387 | 1.03 (1.00, 1.07) | 385 | 1.03 (1.00, 1.06) |
| 3-OHPH | 393 | 1.01 (0.98, 1.04) | 387 | 1.01 (0.97, 1.04) | 385 | 1.00 (0.97, 1.04) |
| 1,9-OHPH | 393 | 0.99 (0.96, 1.02) | 387 | 0.99 (0.96, 1.01) | 385 | 0.99 (0.96, 1.01) |
| 1-OHPy | 391 | 1.00 (0.98, 1.03) | 385 | 1.00 (0.97, 1.03) | 383 | 1.00 (0.97, 1.03) |
| ΣOH-PAH | 391 | 1.00 (0.98, 1.06) | 385 | 1.00 (0.98, 1.02) | 383 | 1.00 (0.98, 1.02) |
| Neutrophils | ||||||
| 2-OHNa | 392 | 1.01 (0.98, 1.04) | 386 | 1.01 (0.98, 1.04) | 384 | 1.00 (0.97, 1.04) |
| 2,3-OHFl | 392 | 1.04 (1.00, 1.09) | 386 | 1.04 (0.99, 1.09) | 384 | 1.03 (0.98, 1.09) |
| 2-OHPH | 393 | 1.06 (1.02, 1.11) | 387 | 1.06 (1.01, 1.11) | 385 | 1.06 (1.01, 1.11) |
| 3-OHPH | 393 | 1.03 (0.98, 1.08) | 387 | 1.02 (0.98, 1.08) | 385 | 1.02 (0.97, 1.07) |
| 1,9-OHPH | 393 | 1.00 (0.96, 1.04) | 387 | 0.99 (0.95, 1.04) | 385 | 0.99 (0.95, 1.04) |
| 1-OHPy | 391 | 1.02 (0.98, 1.07) | 385 | 1.02 (0.97, 1.07) | 383 | 1.02 (0.97, 1.06) |
| ΣOH-PAH | 391 | 1.01 (0.98, 1.04) | 385 | 1.01 (0.98, 1.04) | 383 | 1.01 (0.98, 1.04) |
| Lymphocytes | ||||||
| 2-OHNa | 392 | 0.99 (0.97, 1.01) | 386 | 0.99 (0.97, 1.01) | 384 | 0.99 (0.97, 1.01) |
| 2,3-OHFl | 392 | 0.98 (0.95, 1.01) | 386 | 0.98 (0.95, 1.01) | 384 | 0.97 (0.94, 1.00) |
| 2-OHPH | 393 | 0.99 (0.96, 1.02) | 387 | 0.98 (0.95, 1.02) | 385 | 0.98 (0.95, 1.01) |
| 3-OHPH | 393 | 0.98 (0.94, 1.01) | 387 | 0.97 (0.94, 1.00) | 385 | 0.97 (0.94, 1.00) |
| 1,9-OHPH | 393 | 0.98 (0.95, 1.01) | 387 | 0.97 (0.94, 1.00) | 385 | 0.97 (0.94, 1.00) |
| 1-OHPy | 391 | 0.98 (0.95, 1.21) | 385 | 0.97 (0.94, 1.00) | 383 | 0.97 (0.94, 1.01) |
| ΣOH-PAH | 391 | 0.99 (0.97, 1.01) | 385 | 0.99 (0.97, 1.02) | 383 | 0.99 (0.97, 1.01) |
| Monocytes | ||||||
| 2-OHNa | 392 | 0.98 (0.96, 1.01) | 386 | 0.98 (0.96, 1.01) | 384 | 0.98 (0.96, 1.00) |
| 2,3-OHFl | 392 | 1.00 (0.96, 1.03) | 386 | 1.00 (0.96, 1.04) | 384 | 1.00 (0.96, 1.04) |
| 2-OHPH | 393 | 1.02 (0.98, 1.06) | 387 | 1.02 (0.98, 1.06) | 385 | 1.02 (0.98, 1.06) |
| 3-OHPH | 393 | 1.00 (0.97, 1.04) | 387 | 1.00 (0.96, 1.04) | 385 | 1.00 (0.96, 1.04) |
| 1,9-OHPH | 393 | 0.98 (0.95, 1.02) | 387 | 0.98 (0.95, 1.02) | 385 | 0.98 (0.95, 1.02) |
| 1-OHPy | 391 | 1.00 (0.97, 1.04) | 385 | 1.00 (0.97, 1.04) | 383 | 1.00 (0.97, 1.04) |
| ΣOH-PAH | 391 | 0.98 (0.96, 1.01) | 385 | 0.98 (0.96, 1.01) | 383 | 0.98 (0.96, 1.01) |
| Neutrophil–lymphocyte ratio (NLR) | ||||||
| 2-OHNa | 392 | 1.01 (0.98, 1.05) | 386 | 1.01 (0.98, 1.05) | 384 | 1.01 (0.98, 1.05) |
| 2,3-OHFl | 392 | 1.06 (1.01, 1.12) | 386 | 1.06 (1.01, 1.12) | 384 | 1.06 (1.01, 1.13) |
| 2-OHPH | 393 | 1.08 (1.02, 1.13) | 387 | 1.08 (1.02, 1.14) | 385 | 1.08 (1.02, 1.14) |
| 3-OHPH | 393 | 1.05 (0.99, 1.11) | 387 | 1.05 (1.00, 1.11) | 385 | 1.05 (1.00, 1.12) |
| 1,9-OHPH | 393 | 1.02 (0.97, 1.06) | 387 | 1.02 (0.98, 1.07) | 385 | 1.02 (0.97, 1.07) |
| 1-OHPy | 391 | 1.04 (0.99, 1.10) | 385 | 1.04 (0.99, 1.09) | 383 | 1.04 (0.99, 1.10) |
| ΣOH-PAH | 391 | 1.02 (0.98, 1.06) | 385 | 1.02 (0.98, 1.06) | 383 | 1.02 (0.98, 1.06) |
| OH_PAHs | Model I | Model II | Model III | |||
|---|---|---|---|---|---|---|
| n | β (95% CI) | n | β (95% CI) | n | β (95% CI) | |
| 2-OHNa | 392 | 1.02 (0.99, 1.05) | 386 | 1.02 (0.99, 1.05) | 384 | 1.02 (0.98, 1.05) |
| 2,3-OHFl | 392 | 1.04 (0.99, 1.10) | 386 | 1.04 (1.00, 1.11) | 384 | 1.04 (0.98, 1.10) |
| 2-OHPH | 393 | 1.07 (1.02, 1.12) | 387 | 1.08 (1.03, 1.14) | 385 | 1.08 (1.02, 1.14) |
| 3-OHPH | 393 | 1.05 (1.00, 1.11) | 387 | 1.06 (1.01, 1.12) | 385 | 1.06 (1.00, 1.12) |
| 1,9-OHPH | 393 | 1.00 (0.96, 1.05) | 387 | 1.01 (0.97, 1.06) | 385 | 1.01 (0.96, 1.06) |
| 1-OHPy | 391 | 1.07 (1.02, 1.12) | 385 | 1.08 (1.03, 1.13) | 383 | 1.07 (1.02, 1.13) |
| ΣOH-PAH | 391 | 1.02 (0.99, 1.06) | 385 | 1.02 (0.99, 1.06) | 383 | 1.02 (0.98, 1.06) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verheyen, V.J.; Remy, S.; Govarts, E.; Colles, A.; Rodriguez Martin, L.; Koppen, G.; Voorspoels, S.; Bruckers, L.; Bijnens, E.M.; Vos, S.; et al. Urinary Polycyclic Aromatic Hydrocarbon Metabolites Are Associated with Biomarkers of Chronic Endocrine Stress, Oxidative Stress, and Inflammation in Adolescents: FLEHS-4 (2016–2020). Toxics 2021, 9, 245. https://doi.org/10.3390/toxics9100245
Verheyen VJ, Remy S, Govarts E, Colles A, Rodriguez Martin L, Koppen G, Voorspoels S, Bruckers L, Bijnens EM, Vos S, et al. Urinary Polycyclic Aromatic Hydrocarbon Metabolites Are Associated with Biomarkers of Chronic Endocrine Stress, Oxidative Stress, and Inflammation in Adolescents: FLEHS-4 (2016–2020). Toxics. 2021; 9(10):245. https://doi.org/10.3390/toxics9100245
Chicago/Turabian StyleVerheyen, Veerle J., Sylvie Remy, Eva Govarts, Ann Colles, Laura Rodriguez Martin, Gudrun Koppen, Stefan Voorspoels, Liesbeth Bruckers, Esmée M. Bijnens, Stijn Vos, and et al. 2021. "Urinary Polycyclic Aromatic Hydrocarbon Metabolites Are Associated with Biomarkers of Chronic Endocrine Stress, Oxidative Stress, and Inflammation in Adolescents: FLEHS-4 (2016–2020)" Toxics 9, no. 10: 245. https://doi.org/10.3390/toxics9100245
APA StyleVerheyen, V. J., Remy, S., Govarts, E., Colles, A., Rodriguez Martin, L., Koppen, G., Voorspoels, S., Bruckers, L., Bijnens, E. M., Vos, S., Morrens, B., Coertjens, D., De Decker, A., Franken, C., Den Hond, E., Nelen, V., Covaci, A., Loots, I., De Henauw, S., ... Schoeters, G. (2021). Urinary Polycyclic Aromatic Hydrocarbon Metabolites Are Associated with Biomarkers of Chronic Endocrine Stress, Oxidative Stress, and Inflammation in Adolescents: FLEHS-4 (2016–2020). Toxics, 9(10), 245. https://doi.org/10.3390/toxics9100245