
High Risk Subgroups Sensitive to Air Pollution Levels Following an Emergency Medical Admission

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collation
2.2. Deprivation Indices
2.3. Air Quality
2.4. Risk Predictors and Statistical Methods
3. Results
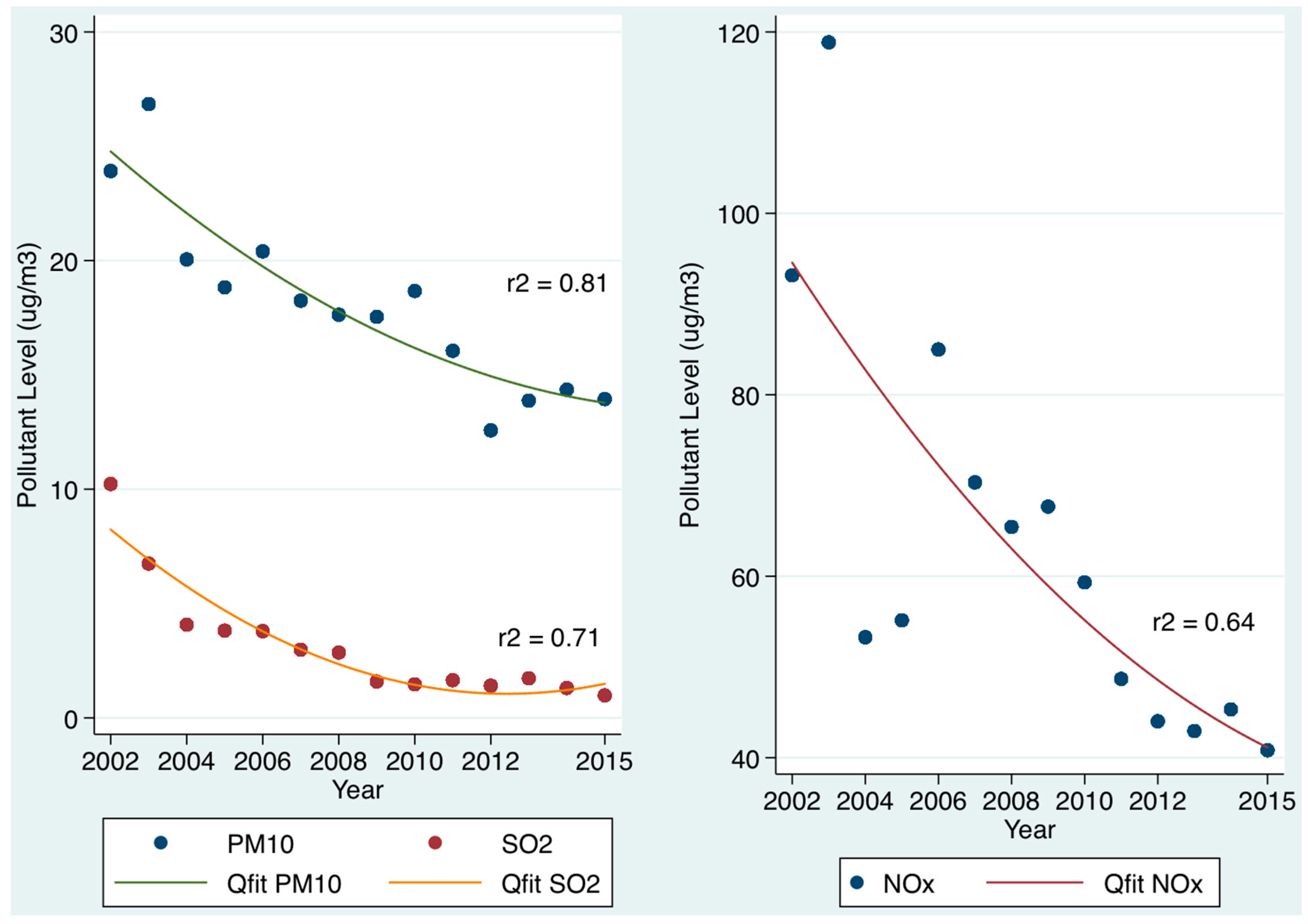
3.1. Admission PM10, SO2, and NOx Levels and 30-Day Hospital Mortality (Figure 1, Table 1)
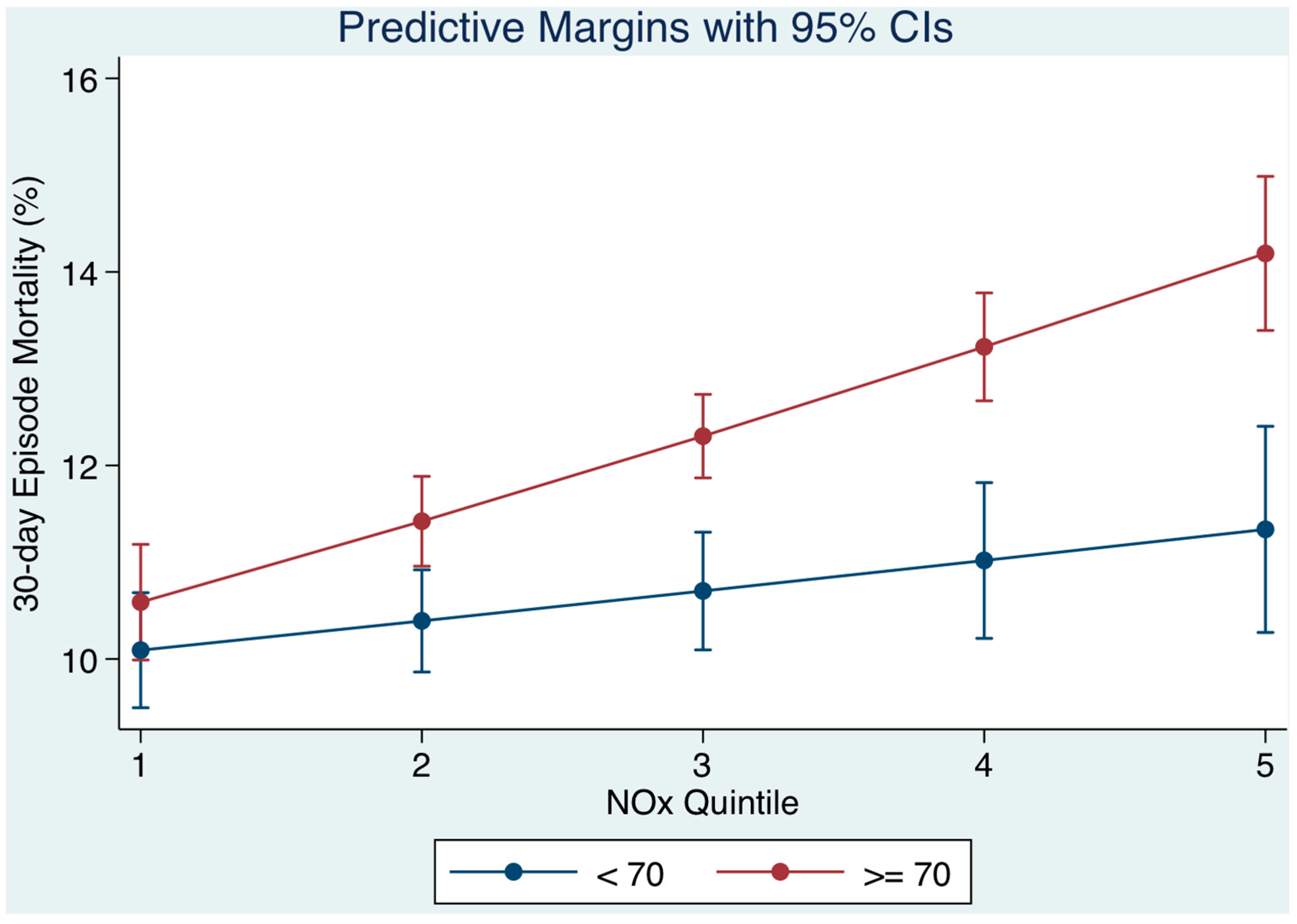
3.2. Air Pollution on Day of Admission and Patient Age (Figure 2)
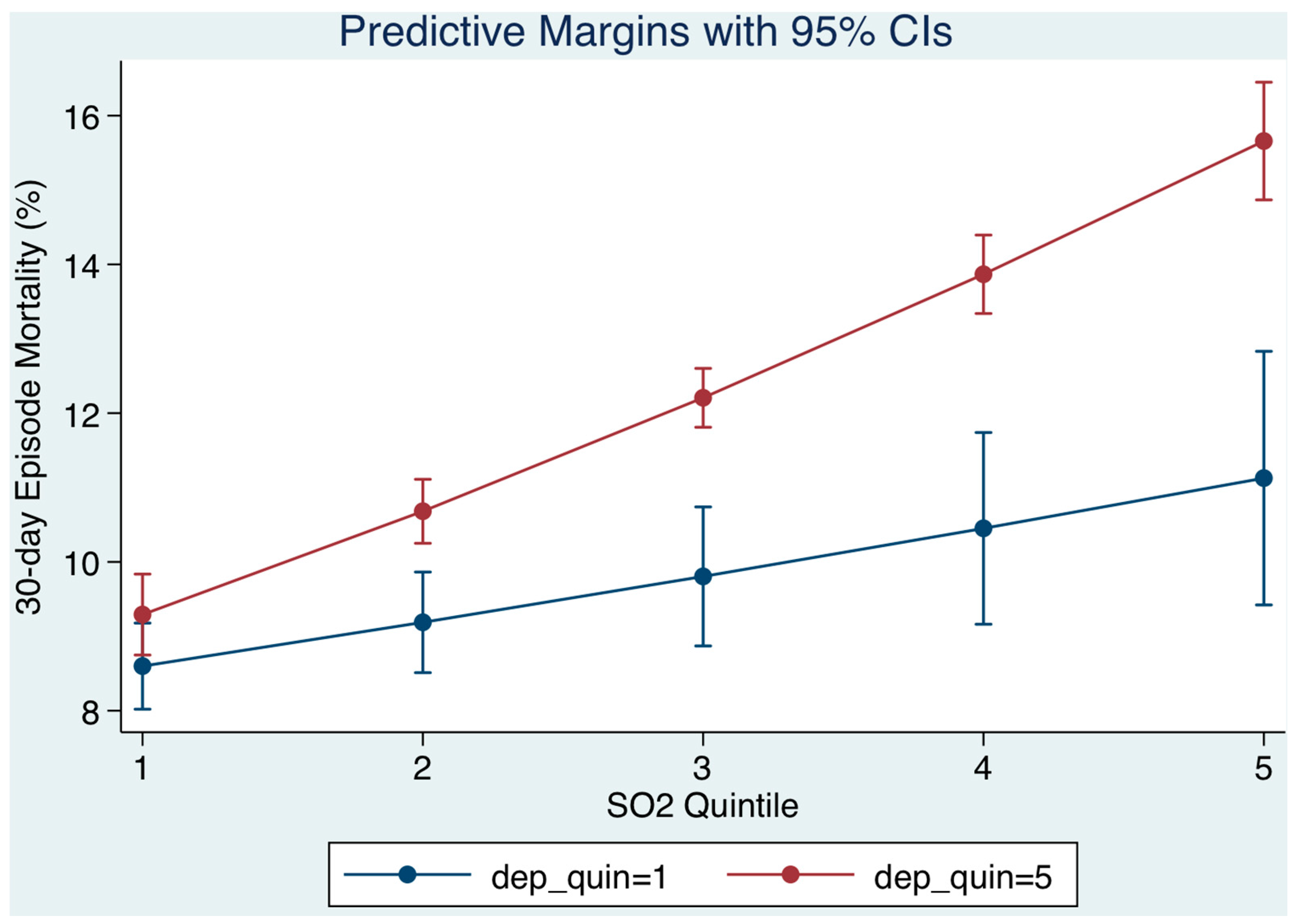
3.3. Relation of Socio-Economic Status on Day of Admission (Figure 3)
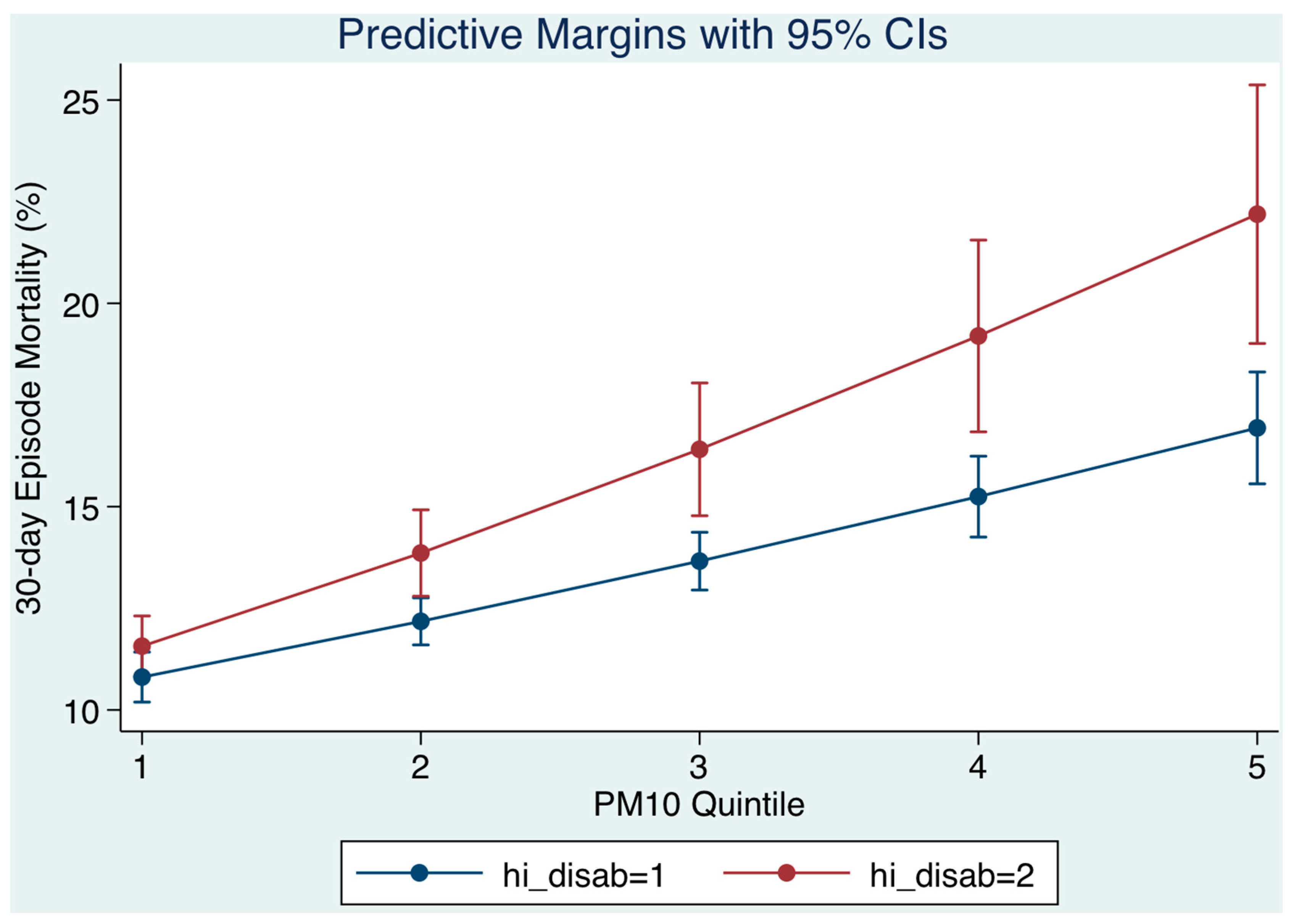
3.4. Relation of Disabling Disease Status on Day of Admission (Figure 4)
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the Air: A Review of the Effects of Particulate Matter Air Pollution on Human Health. J. Med. Toxicol. 2011, 8, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Samet, J.M.; Dominici, F.; Curriero, F.C.; Coursac, I.; Zeger, S.L. Fine particulate air pollution and mortality in 20 U.S. cities, 1987–1994. N. Engl. J. Med. 2000, 343, 1742–1749. [Google Scholar] [CrossRef] [PubMed]
- Katsouyanni, K.; Touloumi, G.; Spix, C.; Schwartz, J.; Balducci, F.; Medina, S.; Rossi, G.; Wojtyniak, B.; Sunyer, J.; Bacharova, L.; et al. Short-term effects of ambient sulphur dioxide and particulate matter on mortality in 12 European cities: Results from time series data from the APHEA project. Air Pollution and Health: A European Approach. BMJ 1997, 314, 1658–1663. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.W.; Pope, C.A. Acute respiratory effects of particulate air pollution. Annu. Rev. Public Health 1994, 15, 107–132. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Kanner, R.E. Acute Effects of PM10 Pollution on Pulmonary Function of Smokers with Mild to Moderate Chronic Obstructive Pulmonary Disease. Am. Rev. Respir. Dis. 1993, 147, 1336–1340. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, R.W.; Anderson, H.R.; Sunyer, J.; Ayearses, J.; Baccini, M.; Vonk, J.M.; Boumghar, A.; Forastiere, F.; Forsberg, B.; Touloumi, G.; et al. Acute effects of particulate air pollution on respiratory admissions: Results from APHEA 2 project. Air Pollution and Health: A European Approach. Am. J. Respir. Crit. Care Med. 2001, 164, 1860–1866. [Google Scholar] [CrossRef] [PubMed]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Jonathan, M.; Samet, M.D. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Kelly, I.; Clancy, L. Mortality in a general hospital and urban air pollution. Ir. Med. J. 1984, 77, 322–324. [Google Scholar] [PubMed]
- Clancy, L.; Goodman, P.; Sinclair, H.; Dockery, D.W. Effect of air-pollution control on death rates in Dublin, Ireland: An intervention study. Lancet 2002, 360, 1210–1214. [Google Scholar] [CrossRef]
- Schwartz, J. Air pollution and daily mortality: a review and meta analysis. Environ. Res. 1994, 64, 36–52. [Google Scholar] [CrossRef] [PubMed]
- Katsouyanni, K.; Zmirou, D.; Spix, C.; Sunyer, J.; Schouten, J.P.; Ponka, A.; Anderson, H.R.; Le Moullec, Y.; Wojtyniak, B.; Vigotti, M.A.; et al. Short-term effects of air pollution on health: A European approach using epidemiological time-series data. The APHEA project: background, objectives, design. Eur. Respir. J. 1995, 8, 1030–1038. [Google Scholar] [PubMed]
- Walsh, J.B.; Coakley, D.; Murphy, C.; Coakley, J.D.; Boyle, E.; Johnson, H. Demographic profile of the elderly population in Dublin accident and emergency hospital catchment areas. Ir. Med. J. 2004, 97, 84–86. [Google Scholar] [PubMed]
- Weuve, J.; Puett, R.C.; Schwartz, J.; Yanosky, J.D.; Laden, F.; Grodstein, F. Exposure to particulate air pollution and cognitive decline in older women. Arch. Intern. Med. 2012, 172, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Havard, S.; Deguen, S.; Zmirou-Navier, D.; Schillinger, C.; Bard, D. Traffic-Related Air Pollution and Socioeconomic Status. Epidemiology 2009, 20, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Chotirmall, S.H.; Picardo, S.; Lyons, J.; D’Alton, M.; O’Riordan, D.; Silke, B. Disabling disease codes predict worse outcomes for acute medical admissions. Intern. Med. J. 2014, 44, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Lodovici, M.; Bigagli, E. Oxidative stress and air pollution exposure. J. Toxicol. 2011, 2011, 4870–4874. [Google Scholar] [CrossRef] [PubMed]
- Bar-Or, D.; Bar-Or, R.; Rael, L.T.; Brody, E.N. Oxidative stress in severe acute illness. Redox Biol. 2015, 4, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Rooney, T.; Moloney, E.D.; Bennett, K.; O’Riordan, D.; Silke, B. Impact of an acute medical admission unit on hospital mortality: A 5-year prospective study. QJM 2008, 101, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; O’Riordan, D.; Silke, B. Long-term outcome of an AMAU—A decade’s experience. Q. J. Med. 2014, 107, 43–49. [Google Scholar] [CrossRef] [PubMed]
- O’Loughlin, R.; Allwright, S.; Barry, J.; Kelly, A.; Teljeur, C. Using HIPE data as a research and planning tool: Limitations and opportunities. Ir. J. Med. Sci. 2005, 174, 40–45. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, A.; Colgan, M.P.; McGuigan, C.; Smyth, F.; Haider, N.; O’Neill, S.; Moore, D.; Madhavan, P. A critical evaluation of HIPE data. Ir. Med. J. 2012, 105, 21–23. [Google Scholar] [PubMed]
- Kelly, A.; Teljeur, C. SAHRU National Deprivation Index Trinity College, Dublin, 2007. Available online: http://www.sahru.tcd.ie/services/ deprivation/DeprivationFiles/WebReport07.pdf (accessed on 7 July 2007).
- Conway, R.; Galvin, S.; Coveney, S.; O’Riordan, D.; Silke, B. Deprivation as an outcome determinant in emergency medical admissions. QJM 2013, 106, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Shimrat, M. Algorithm 112: Position of point relative to polygon. Commun. ACM 1962, 5, 434. [Google Scholar] [CrossRef]
- Keary, J.; Jennings, S.G.; O’Connor, T.C.; McManus, B.; Lee, M. PM10 concentration measurements in Dublin city. Environ. Monit. Assess. 1998, 52, 3–18. [Google Scholar] [CrossRef]
- Silke, B.; Kellett, J.; Rooney, T.; Bennett, K.; O’Riordan, D. An improved medical admissions risk system using multivariable fractional polynomial logistic regression modelling. Q. J. Med. 2010, 103, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Moreno, R. Clinical review: Scoring systems in the critically ill. Crit. Care 2010, 14, 207. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.; Greenslade, J.H.; Chu, K.; Brown, A.F.; Lipman, J. Severity Scores in Emergency Department Patients With Presumed Infection: A Prospective Validation Study. Crit. Care Med. 2016, 44, 539–547. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Courtney, D.; Conway, R.; Kavanagh, J.; O’Riordan, D.; Silke, B. High-sensitivity troponin as an outcome predictor in acute medical admissions. Postgrad. Med. J. 2014, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Chotirmall, S.H.; Callaly, E.; Lyons, J.; O’Connell, B.; Kelleher, M.; Byearsne, D.; O’Riordan, D.; Silke, B. Blood cultures in emergency medical admissions: A key patient cohort. Eur. J. Emerg. Med. 2016, 23, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.; Teljeur, C. SAHRU National Deprivation Index; Small Area Health Research Unit (SAHRU), Department of Public Health & Primary Care, Trinity College Dublin: Dublin, Ireland, 2007. [Google Scholar]
- Di, Q.; Wang, Y.; Zanobetti, A.; Wang, Y.; Koutrakis, P.; Choirat, C.; Dominici, F.; Schwartz, J.D. Air Pollution and Mortality in the Medicare Population. N. Engl. J. Med. 2017, 376, 2513–2522. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Schindler, C.; Liu, L.J.; Keidel, D.; Bayer-Oglesby, L.; Brutsche, M.H.; Gerbase, M.W.; Keller, R.; Künzli, N.; Leuenberger, P.; et al. Reduced exposure to PM10 and attenuated age-related decline in lung function. N. Engl. J. Med. 2007, 357, 2338–2347. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.; Schikowski, T.; Carsin, A.E.; Cai, Y.; Jacquemin, B.; Sanchez, M. Adult lung function and long-term air pollution exposure. ESCAPE: A multicentre cohort study and meta-analysis. Eur. Respir. J. 2015, 45, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.-M.; Ou, C.-Q.; Chan, K.-P.; Chau, Y.-K.; Thach, T.-Q.; Yang, L.; Chung, R.Y.-N.; Thomas, G.N.; Peiris, J.S.M.; Wong, T.-W.; et al. The Effects of Air Pollution on Mortality in Socially Deprived Urban Areas in Hong Kong, China. Environ. Health Perspect. 2008, 116, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Sloggett, A.; Joshi, H. Higher mortality in deprived areas: Community or personal disadvantage? BMJ 1994, 309, 1470–1474. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Z.J.; B nnelykke, K.; Hvidberg, M.; Jensen, S.S.; Ketzel, M.; Loft, S.; Mette, S.; Anne, T.; Kim, O.; Ole, R.-N. Long-term exposure to air pollution and asthma hospitalisations in older adults: A cohort study. Thorax 2011, 67, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.; Baldacci, S.; Maio, S.; Cerrai, S.; Sarno, G.; Viegi, G. Adverse effects of outdoor pollution in the elderly. J. Thorac Dis. 2015, 7, 34–45. [Google Scholar] [PubMed]
- Ozminkowski, R.J.; Smith, M.W.; Coffey, R.M.; Mark, T.L.; Neslusan, C.A.; Drabek, J. Private Payers Serving Individuals with Disabilities and Chronic Conditions; Department of Health and Human Services: Washington, DC, USA, 2000.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Group | OR | 95% CI | p < |
|---|---|---|---|---|
| SO2 (µg/m3) | Q II | 1.30 | 1.12, 1.50 | 0.001 |
| Q III | 1.54 | 1.33, 1.78 | 0.001 | |
| Q IV | 1.92 | 1.66, 2.22 | 0.001 | |
| Q V | 1.88 | 1.60, 2.21 | 0.001 | |
| PM10 (µg/m3) | 1.04 | 1.01, 1.08 | 0.02 | |
| Illness Severity | 3.97 | 3.58, 4.41 | 0.001 | |
| Charlson Index | 1.56 | 1.47, 1.66 | 0.001 | |
| Disabling Score | 1.19 | 1.14, 1.25 | 0.001 | |
| Sepsis | 2.44 | 2.28, 2.63 | 0.001 | |
| MDC Respiratory | 1.98 | 1.77, 2.22 | 0.001 | |
| MDC Cardiac | 1.72 | 1.51, 1.96 | 0.001 | |
| MDC Neurology | 2.13 | 1.84, 2.48 | 0.001 | |
| Deprivation—ED | 1.09 | 1.05, 1.14 | 0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cournane, S.; Conway, R.; Byrne, D.; O’Riordan, D.; Coveney, S.; Silke, B. High Risk Subgroups Sensitive to Air Pollution Levels Following an Emergency Medical Admission. Toxics 2017, 5, 27. https://doi.org/10.3390/toxics5040027
Cournane S, Conway R, Byrne D, O’Riordan D, Coveney S, Silke B. High Risk Subgroups Sensitive to Air Pollution Levels Following an Emergency Medical Admission. Toxics. 2017; 5(4):27. https://doi.org/10.3390/toxics5040027
Chicago/Turabian StyleCournane, Seán, Richard Conway, Declan Byrne, Deirdre O’Riordan, Seamus Coveney, and Bernard Silke. 2017. "High Risk Subgroups Sensitive to Air Pollution Levels Following an Emergency Medical Admission" Toxics 5, no. 4: 27. https://doi.org/10.3390/toxics5040027
APA StyleCournane, S., Conway, R., Byrne, D., O’Riordan, D., Coveney, S., & Silke, B. (2017). High Risk Subgroups Sensitive to Air Pollution Levels Following an Emergency Medical Admission. Toxics, 5(4), 27. https://doi.org/10.3390/toxics5040027