
Fighting Lead Poisoning: Effective Conditions for Home-Based Education, Housing Remediation, and Relocation †

 ,
,
Abstract

1. Introduction
2. Materials and Methods
3. Results
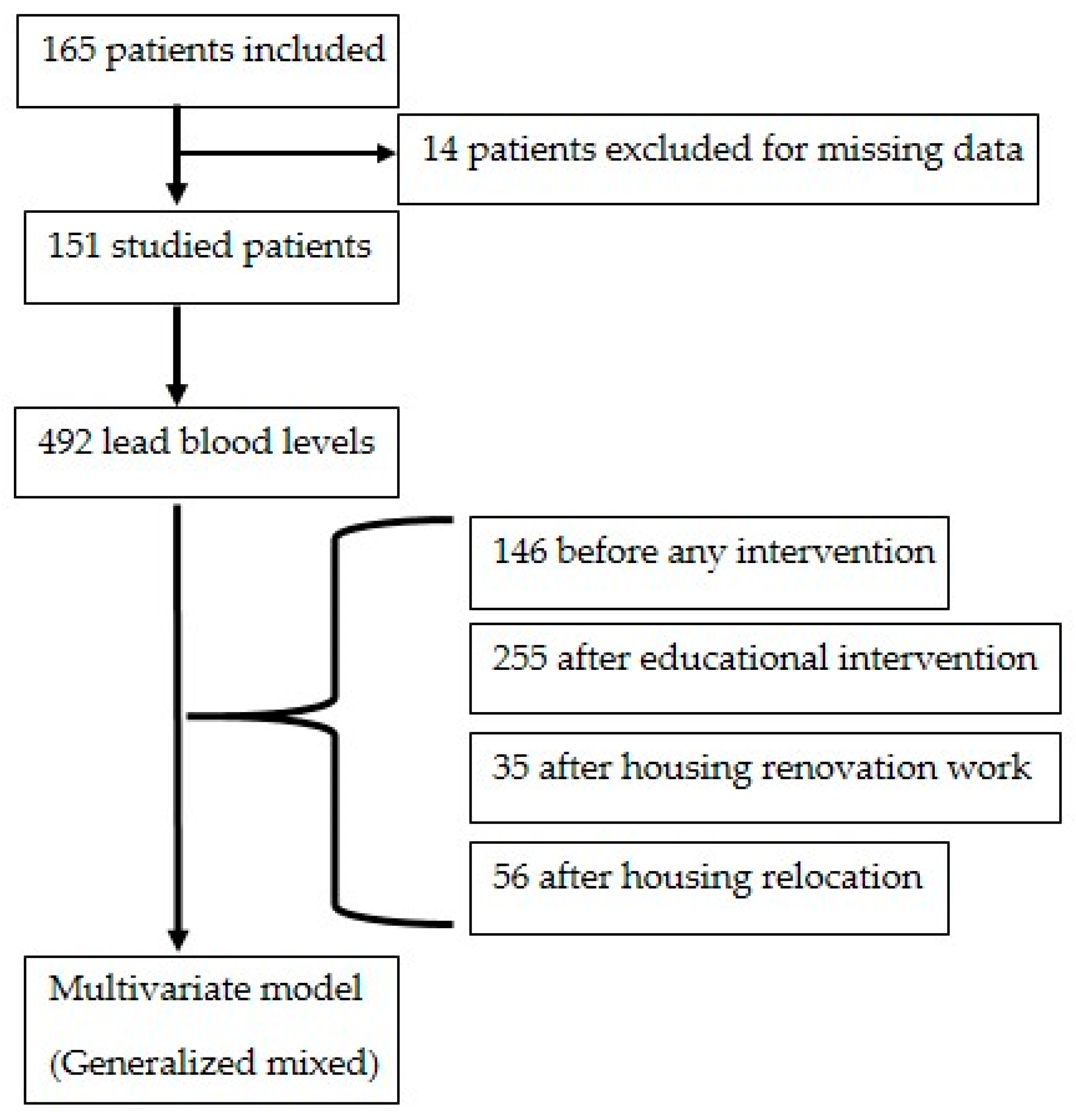
3.1. Initial Situation
3.2. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HEPA | High-Efficiency Particulate Air |
| RCT | Randomized Controlled Trial |
References
- Environmental Burden of Disease Associated with Inadequate Housing: A Method Guide to the Quantification of Health Effects of Selected Housing Risks in the WHO European Region. Available online: https://www.who.int/publications/i/item/9789289057899 (accessed on 27 June 2025).
- Saturnisme de L’enfant. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/maladies-de-la-mere-et-de-l-enfant/saturnisme-de-l-enfant (accessed on 27 June 2025).
- Détermination de Nouveaux Objectifs de Gestion des Expositions Au Plomb. Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=444 (accessed on 27 June 2025).
- Rollin, L.; Carré, N.; Garnier, R. Greater Paris lead poisoning monitoring system (système de surveillance du saturnisme en Ile-de-France [SSSILF]). Follow-up of children suffering from lead poisoning or at risk of lead poisoning in Greater Paris, 1992--2002. Rev. Epidemiol. Sante Publique 2008, 56, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Solet, J.L.; Renault, P.; Denys, J.C.; Teulé, G.; Dennemont, R.M.; Domonte, F.; Garnier, C.; Aubert, L.; Filleul, L.; Polycarpe, D. Discovery and follow-up of a lead-poisoning outbreak in a shantytown of Le Port, Reunion Island. Rev. Epidemiol. Sante Publique 2013, 61, 329–337. [Google Scholar] [CrossRef]
- Chapitre IV: Lutte Contre la Présence de Plomb ou D’amiante. (Articles L1334-1 à L1334-17)-Légifrance. Available online: https://www.legifrance.gouv.fr/codes/section_lc/LEGITEXT000006072665/LEGISCTA000006171529/#LEGISCTA000050703003 (accessed on 27 June 2025).
- HCSP Mise à jour du Guide Pratique de Dépistage et de Prise en Charge des Expositions au Plomb chez L’enfant Mineur et la Femme Enceinte. Haut Conseil de la Santé Publique. 2017. Available online: https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=643 (accessed on 27 June 2025).
- Amitai, Y.; Graef, J.W.; Brown, M.J.; Gerstle, R.S.; Kahn, N.; Cochrane, P.E. Hazards of “deleading” homes of children with lead poisoning. Am. J. Dis. Child. 1987, 141, 758–760. [Google Scholar] [CrossRef]
- Shani, Z.; Scott, R.G.; Schofield, L.S.; Johnson, J.H.; Williams, E.R.; Hampton, J.; Ramprasad, V. Effect of a home intervention program on pediatric asthma in an environmental justice community. Health Promot. Pract. 2015, 16, 291–298. [Google Scholar] [CrossRef]
- de Blay, F.; Fourgaut, G.; Hedelin, G.; Vervloet, D.; Michel, F.; Godard, P.; Charpin, D.; Pauli, G.; the Scientific Committee of the MIEC Study. Medical Indoor Environment Counselor (MIEC): Role in compliance with advice on mite allergen avoidance and on mite allergen exposure. Allergy 2003, 58, 27–33. [Google Scholar] [CrossRef]
- Montaudié-Dumas, I.; Giovannini-Chami, L.; Debai, C.; Collomp, R.; Bailly-Piccini, C.; Berlioz, M.; Albertini, M.; Bourrier, T. Impact on the indoor environment of allergic children of the medical counselor on indoor environment, after two successive visits at 6 months interval. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 2013, 20, 1288–1295. [Google Scholar] [CrossRef]
- Yeoh, B.; Woolfenden, S.; Wheeler, D.; Alperstein, G.; Lanphear, B. Household interventions for prevention of domestic lead exposure in children. Cochrane Database Syst Rev. 2008, 2, CD006047. [Google Scholar] [CrossRef]
- Nussbaumer-Streit, B.; Mayr, V.; Dobrescu, A.I.; Wagner, G.; Chapman, A.; Pfadenhauer, L.M.; Lohner, S.; Lhachimi, S.K.; Busert, L.K.; Gartlehner, G. Household interventions for secondary prevention of domestic lead exposure in children. Cochrane Database Syst. Rev. 2020, 10, CD006047. [Google Scholar] [CrossRef]
- USEPAO Lead Laws and Regulations. 2013. Available online: https://www.epa.gov/lead/lead-laws-and-regulations (accessed on 27 June 2025).
- Ministère de la Santé et des Solidarités. L’intoxication par le Plomb de L’enfant et la Femme Enceinte: Guide Pratique. 2006. Available online: https://sante.gouv.fr/IMG/pdf/guide_depistage_saturnisme-3.pdf (accessed on 27 June 2025).
- Décret n°2002-120 du 30 Janvier 2002 Relatif aux Caractéristiques du Logement Décent Pris pour L’application de L’article 187 de la loi n° 2000-1208 du 13 Décembre 2000 Relative à la Solidarité et au Renouvellement Urbains—Légifrance. Available online: https://www.legifrance.gouv.fr/loda/id/JORFTEXT000000217471/ (accessed on 27 June 2025).
- The Challenge of Slums—Global Report on Human Settlements 2003 UN-Habitat. Available online: https://unhabitat.org/the-challenge-of-slums-global-report-on-human-settlements-2003 (accessed on 27 June 2025).
- Les Conseillers (CMEI/CHS), APPA. Available online: https://www.appa.asso.fr/habitat-sante/les-conseillers/ (accessed on 27 June 2025).
- Laporte, R. Against lead poisoning: Effectiveness of housing first and counselling in the home. In Proceeding of the European Public Health Congress, Marseille, France, 20–23 November 2019. [Google Scholar]
- Jordan, C.M.; Yust, B.L.; Robison, L.L.; Hannan, P.; Deinard, A.S. A randomized trial of education to prevent lead burden in children at high risk for lead exposure: Efficacy as measured by blood lead monitoring. Environ. Health Perspect. 2003, 111, 1947–1951. [Google Scholar] [CrossRef]
- Shen, X.M.; Yan, C.H.; Wu, S.H.; Shi, R. Parental education to reduce blood lead levels in children with mild and moderate lead poisoning: A randomized controlled study. Zhonghua Er Ke Za Zhi Chin. J. Pediatr. 2004, 42, 892–897. [Google Scholar]
- Alcock, G.; Das, S.; More, N.S.; Hate, K.; More, S.; Pantvaidya, S.; Osrin, D.; Houweling, T.A. Examining inequalities in uptake of maternal health care and choice of provider in underserved urban areas of Mumbai, India: A mixed methods study. BMC Pregnancy Childbirth 2015, 15, 231. [Google Scholar] [CrossRef] [PubMed]
- Levesque, J.F.; Harris, M.F.; Russell, G. Patient-centred access to health care: Conceptualising access at the interface of health systems and populations. Int. J. Equity Health 2013, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Dixon, S.L.; Jacobs, D.E.; Wilson, J.W.; Akoto, J.Y.; Nevin, R.; Scott Clark, C. Window replacement and residential lead paint hazard control 12 years later. Environ. Res. 2012, 113, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Sarigiannis, D.A.; Hansen, U. Considering the cumulative risk of mixtures of chemicals—A challenge for policy makers. Environ. Health Glob. Access Sci. Source 2012, 11 (Suppl. 1), S18. [Google Scholar] [CrossRef]
- Braun, J.M.; Hornung, R.; Chen, A.; Dietrich, K.N.; Jacobs, D.E.; Jones, R.; Khoury, J.C.; Liddy-Hicks, S.; Morgan, S.; VanderBeek, S.B.; et al. Effect of Residential Lead-Hazard Interventions on Childhood Blood Lead Concentrations and Neurobehavioral Outcomes: A Randomized Clinical Trial. JAMA Pediatr. 2018, 172, 934–942. [Google Scholar] [CrossRef]
- Campbell, C.; Tran, M.; Gracely, E.; Starkey, N.; Kersten, H.; Palermo, P.; Rothman, N.; Line, L.; Hansen-Turton, T. Primary prevention of lead exposure: The Philadelphia lead safe homes study. Public Health Rep. Wash DC 2011, 126 (Suppl. 1), 76–88. [Google Scholar] [CrossRef]
- Hilts, S.R.; Hertzman, C.; Marion, S.A. A controlled trial of the effect of HEPA vacuuming on childhood lead exposure. Can. J. Public. Health Rev. Can. Sante Publique 1995, 86, 345–350. [Google Scholar]
- Rhoads, G.G.; Ettinger, A.S.; Weisel, C.P.; Buckley, T.J.; Goldman, K.D.; Adgate, J.; Lioy, P.J. The effect of dust lead control on blood lead in toddlers: A randomized trial. Pediatrics 1999, 103, 551–555. [Google Scholar] [CrossRef]
- Krezanoski, P.J.; Comfort, A.B.; Hamer, D.H. Effect of incentives on insecticide-treated bed net use in sub-Saharan Africa: A cluster randomized trial in Madagascar. Malar. J. 2010, 9, 186. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Howard, C.; Eberly, S.; Auinger, P.; Kolassa, J.; Weitzman, M.; Schaffer, S.J.; Alexander, K. Primary prevention of childhood lead exposure: A randomized trial of dust control. Pediatrics 1999, 103, 772–777. [Google Scholar] [CrossRef]
- Farrell, K.P.; Brophy, M.C.; Chisolm, J.J.; Rohde, C.A.; Strauss, W.J. Soil lead abatement and children’s blood lead levels in an urban setting. Am. J. Public Health 1998, 88, 1837–1839. [Google Scholar] [CrossRef]
- Miller, F.G.; Brody, H. Clinical equipoise and the incoherence of research ethics. J. Med. Philos. 2007, 32, 151–165. [Google Scholar] [CrossRef]
- Article L1334-1-Code de la Santé Publique—Légifrance. Available online: https://www.legifrance.gouv.fr/codes/article_lc/LEGIARTI000031928008 (accessed on 27 June 2025).
- Mal-logement en France: La Bombe Sociale a Explosé Fondation pour le Logement. Available online: http://www.fondationpourlelogement.fr/nos-publications/communiques-de-presse/mal-logement-en-france-la-bombe-sociale-explose (accessed on 27 June 2025).
- Section 1: Conditions D’attribution des Logements et Plafonds de Ressources. (Articles L441 à L441-2-9)—Légifrance. Available online: https://www.legifrance.gouv.fr/codes/id/LEGISCTA000006176320/ (accessed on 27 June 2025).
- Chapitre V: Autorisation préalable de mise en location (Articles L635-1 à L635-11)—Légifrance. Available online: https://www.legifrance.gouv.fr/codes/section_lc/LEGITEXT000006074096/LEGISCTA000028781374/ (accessed on 27 June 2025).
- Ajay, S.V.; Kirankumar, P.S.; Sanath, K.; Prathish, K.P.; Haridas, A. An experimental simulation study of conventional waste burning practices in India for the assessment and inventorisation of PCDD/F/dl-PCB emissions. J. Environ. Manag. 2022, 303, 114109. [Google Scholar] [CrossRef] [PubMed]
- Akortia, E.; Olukunle, O.I.; Daso, A.P.; Okonkwo, J.O. Soil concentrations of polybrominated diphenyl ethers and trace metals from an electronic waste dump site in the Greater Accra Region, Ghana: Implications for human exposure. Ecotoxicol. Environ. Saf. 2017, 137, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Z.; Mott, S.; Magwood, O.; Mathew, C.; Mclellan, A.; Kpade, V.; Gaba, P.; Kozloff, N.; Pottie, K.; Andermann, A. The impact of interventions for youth experiencing homelessness on housing, mental health, substance use, and family cohesion: A systematic review. BMC Public Health 2019, 19, 1528. [Google Scholar] [CrossRef]
- Boreland, F.; Lesjak, M.; Lyle, D. Evaluation of home lead remediation in an Australian mining community. Sci. Total Environ. 2009, 408, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Seth, R.; Girotra, T.G.; Mohammad, I.; Qaiyum, Y.; Taneja, I.; Raman, S. Mobile health van as an intervention to provide clinical support and health promotion to street children and marginalised populations in the National Capital Region of Delhi: A mixed-methods evaluation. BMJ Paediatr. Open 2025, 9, e002988. [Google Scholar] [CrossRef]
- Stormacq, C.; Van den Broucke, S.; Wosinski, J. Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health Promot. Int. 2019, 34, e1–e17. [Google Scholar] [CrossRef]
- Reviving Health Mediation During the COVID-19 Crisis and Beyond: An Implementation Study in Deprived Neighbourhoods of Marseille, France—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/39022414/ (accessed on 27 June 2025).
- Laporte, R.; Babe, P.; Jouve, E.; Daguzan, A.; Mazoue, F.; Minodier, P.; Noel, G.; Urbina, D.; Gentile, S. Developing and Validating an Individual-Level Deprivation Index for Children’s Health in France. Int. J. Environ. Res. Public Health 2022, 19, 16949. [Google Scholar] [CrossRef]
- SPF Un Programme National de Médiation en Santé Auprès et Avec les Gens du Voyage et les Habitants de Bidonvilles et Squats. Available online: https://www.santepubliquefrance.fr/import/un-programme-national-de-mediation-en-sante-aupres-et-avec-les-gens-du-voyage-et-les-habitants-de-bidonvilles-et-squats (accessed on 27 June 2025).
- Hill, A.B. The Environment and Disease: Association or Causation? Proc. R Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef]
- Cantor, A.G.; Hendrickson, R.; Blazina, I.; Griffin, J.; Grusing, S.; McDonagh, M.S. Screening for Elevated Blood Lead Levels in Childhood and Pregnancy: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2019, 321, 1510–1526. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.E. Lead screening update from the US Preventive Services Task Force. J. Pediatr. 2019, 212, 243. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.; Hill, S.; Guyatt, G.; Akl, E.A.; Ahmed, F. The GRADE approach and Bradford Hill’s criteria for causation. J. Epidemiol. Community Health 2011, 65, 392–395. [Google Scholar] [CrossRef]
- Hall, W. Austin Bradford Hill’s “Environment and disease: Association or causation. ” Addict. Abingdon Engl. 2024, 119, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Loke, Y.K.; Mattishent, K. Propensity score methods in real-world epidemiology: A practical guide for first-time users. Diabetes. Obes. Metab. 2020, 22 (Suppl. 3), 13–20. [Google Scholar] [CrossRef]
- Jardé, L. LOI N° 2012-300 Du 5 Mars 2012 Relative Aux Recherches Impliquant La Personne Humaine. J. Off. 2012, 56. Available online: https://www.legifrance.gouv.fr/jorf/id/JORFTEXT000025441587 (accessed on 27 June 2025).

{kind=link}
{kind=link}
| Legal Housing | Slum | p | ||
|---|---|---|---|---|
| N (%) | 85 (56.3) | 66 (43.7) | ||
| Boys | 52 (61.2) | 41 (62.1) | 0.13 | |
| Age at diagnosis (years) * | 4.9 (1.7) | 5.9 (2.0) | 0.14 | |
| Sources of lead exposure | ||||
| Decayed paint | 63 (74.1) | 7 (10.6) | <0.0005 | |
| Smoke and dust (burning, recycling) | 21 (24.7) | 63 (95.5) | <0.0005 | |
| Polluted water (leaded pipes) | 2 (3.0) | 0 (0.0) | 0.51 | |
| Risk co-factors | ||||
| Pica–geophagy behavior | 10 (11.8) | 0 (0.0) | 0.005 | |
| Surrounding cases | 77 (90.6) | 63 (95.5) | 0.35 | |
| Associated housing substandard criteria | 44 (51.8) | 57 (86.4) | <0.0005 | |
| Parental at-risk occupation | 15 (17.6) | 54 (81.8) | <0.0005 | |
| Blood lead level at diagnosis (μg/L) * | 110.7 (34.5) | 138.4 (32.2) | 0.01 | |
| Housing Type | Legal | Slum | |||
|---|---|---|---|---|---|
| Coefficient (Standard Error) | p | Coefficient (Standard Error) | p | ||
| Intercept | 71.4 (12.9) | <0.0001 | 105.8 (11.4) | <0.0001 | |
| Inclusion age < 7 years | 19.2 (12.0) | 0.11 | 47.7 (13.7) | 0.001 | |
| Associated housing substandard criteria | 36.6 (11.3) | <0.005 | - | ||
| Time (months) | 4.3 (1.54) | <0.01 | 1.0 (0.94) | 0.29 | |
| Interaction time x intervention, after: | |||||
| Home-based educational intervention | −5.4 (1.52) | <0.001 | −2.1 (0.82) | 0.01 | |
| Housing remediation | −6.0 (1.57) | <0.001 | - | ||
| Housing relocation | −5.7 (1.56) | <0.001 | −4.5 (1.0) | <0.0001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Barberin-Barberini, H.; Jouve, E.; Dubus, J.-C.; Hadji, K.; Laporte, R. Fighting Lead Poisoning: Effective Conditions for Home-Based Education, Housing Remediation, and Relocation. Toxics 2025, 13, 552. https://doi.org/10.3390/toxics13070552
de Barberin-Barberini H, Jouve E, Dubus J-C, Hadji K, Laporte R. Fighting Lead Poisoning: Effective Conditions for Home-Based Education, Housing Remediation, and Relocation. Toxics. 2025; 13(7):552. https://doi.org/10.3390/toxics13070552
Chicago/Turabian Stylede Barberin-Barberini, Hugues, Elisabeth Jouve, Jean-Christophe Dubus, Karine Hadji, and Remi Laporte. 2025. "Fighting Lead Poisoning: Effective Conditions for Home-Based Education, Housing Remediation, and Relocation" Toxics 13, no. 7: 552. https://doi.org/10.3390/toxics13070552
APA Stylede Barberin-Barberini, H., Jouve, E., Dubus, J.-C., Hadji, K., & Laporte, R. (2025). Fighting Lead Poisoning: Effective Conditions for Home-Based Education, Housing Remediation, and Relocation. Toxics, 13(7), 552. https://doi.org/10.3390/toxics13070552