

Reduced Isocyanate Release Using a Waterproof, Resin-Based Cast Alternative Relative to Fiberglass Casts



Abstract
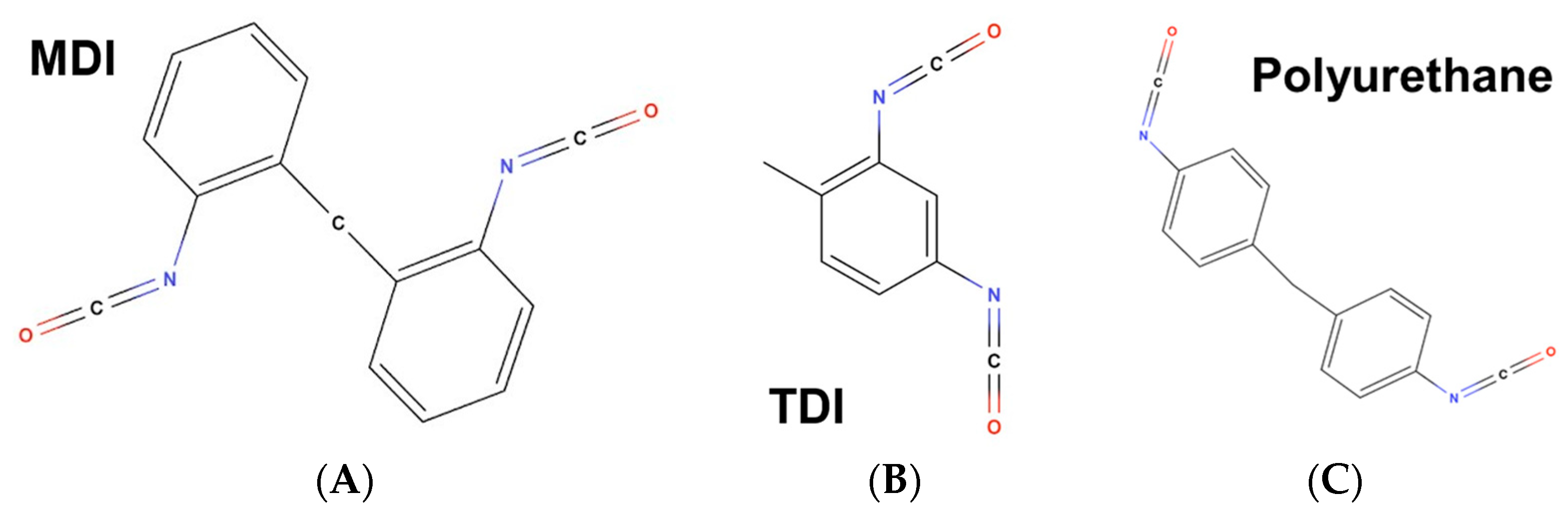
1. Introduction
2. Materials and Methods
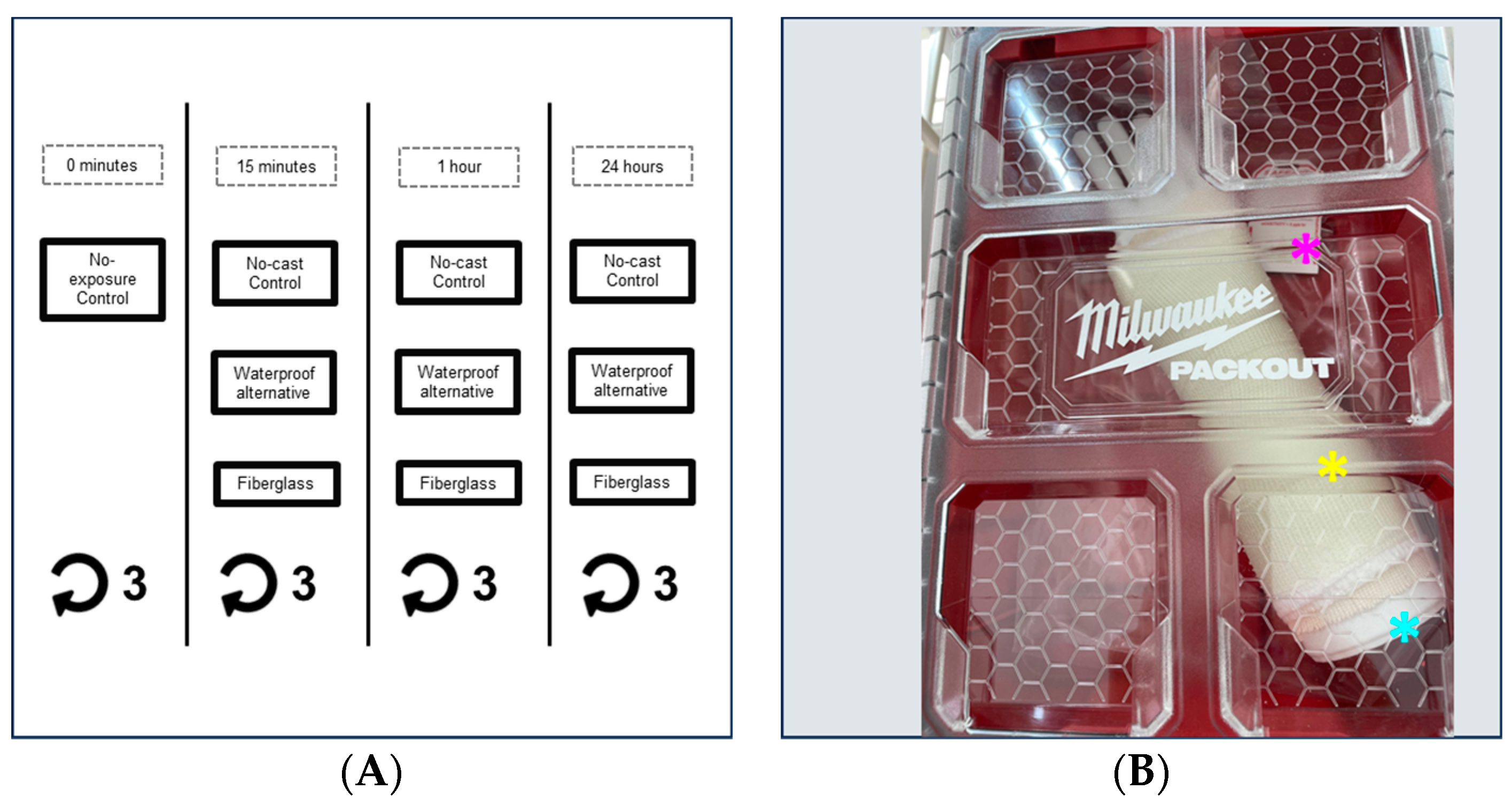
2.1. Waterproof Alternative and Fiberglass Testing
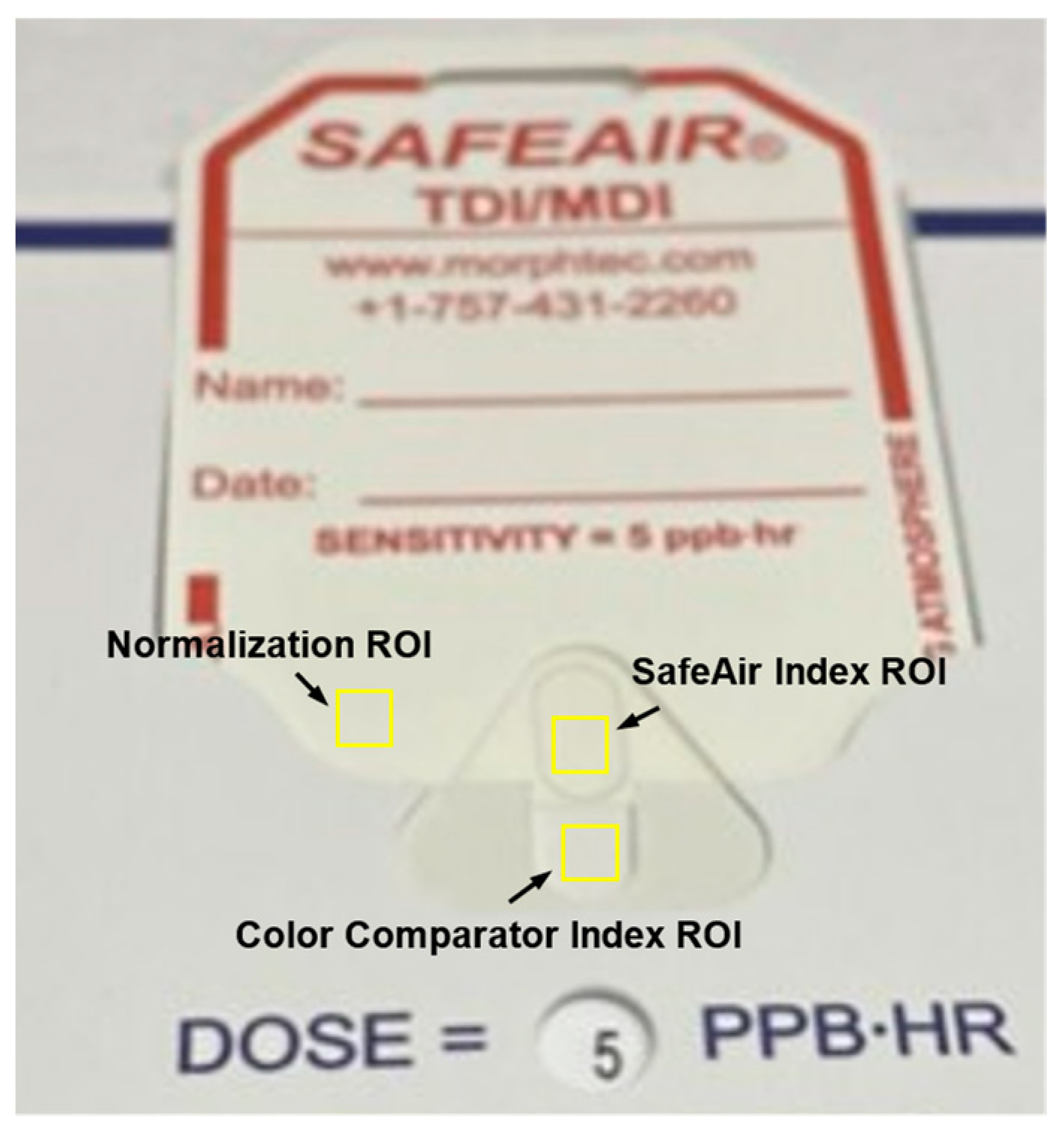
2.2. Image Collection
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
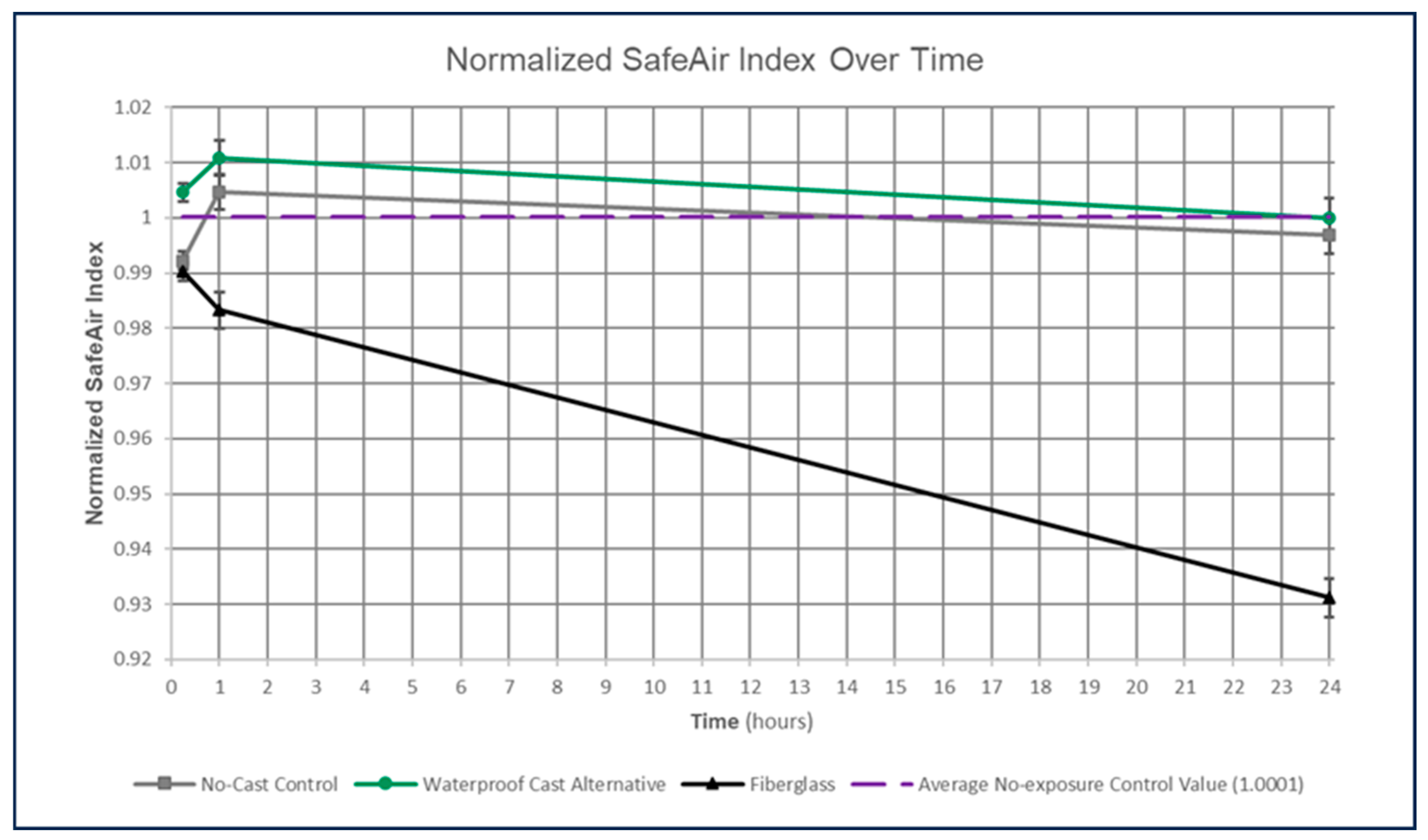
3.1. Normalized SafeAir Index Values
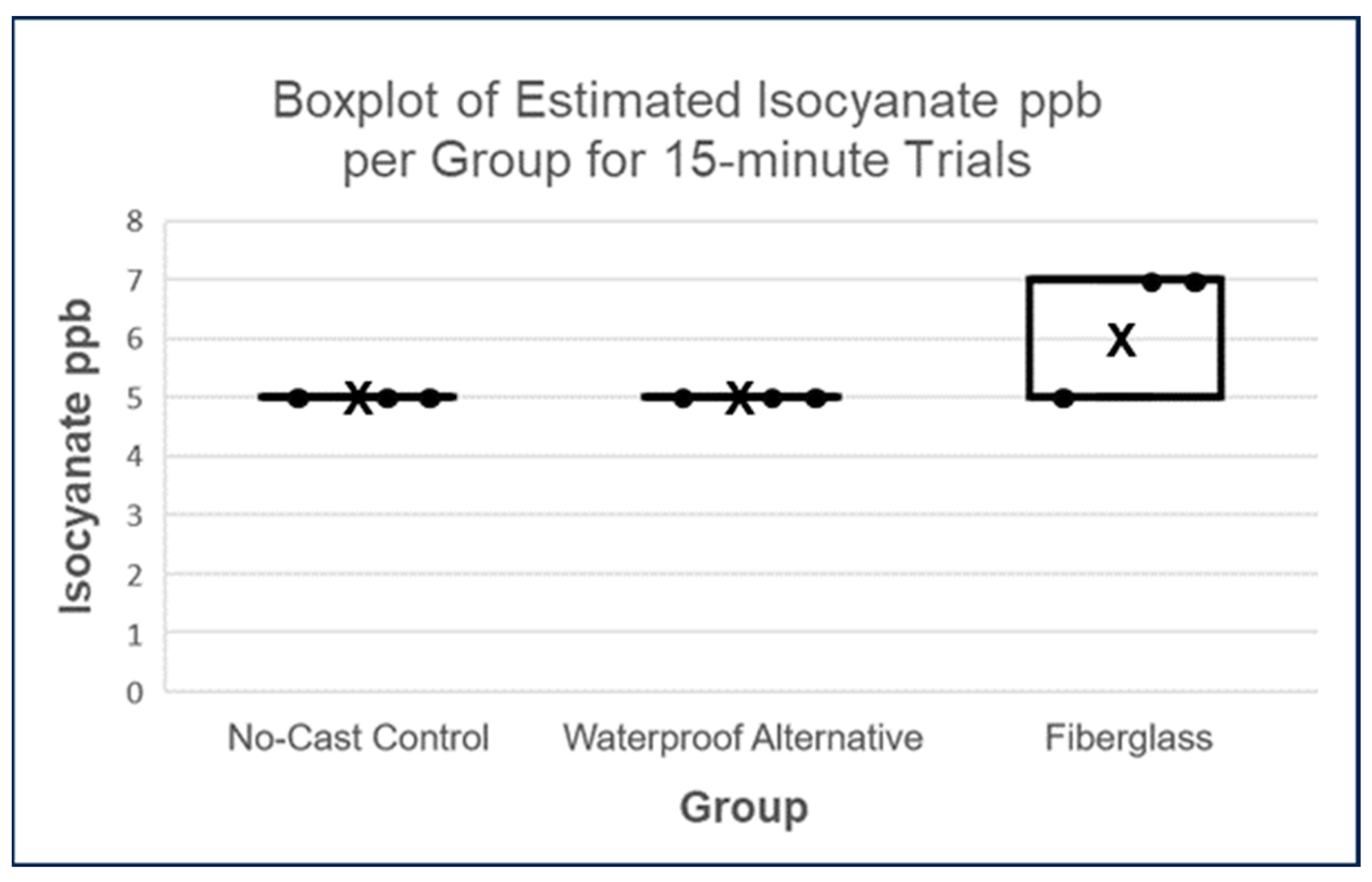
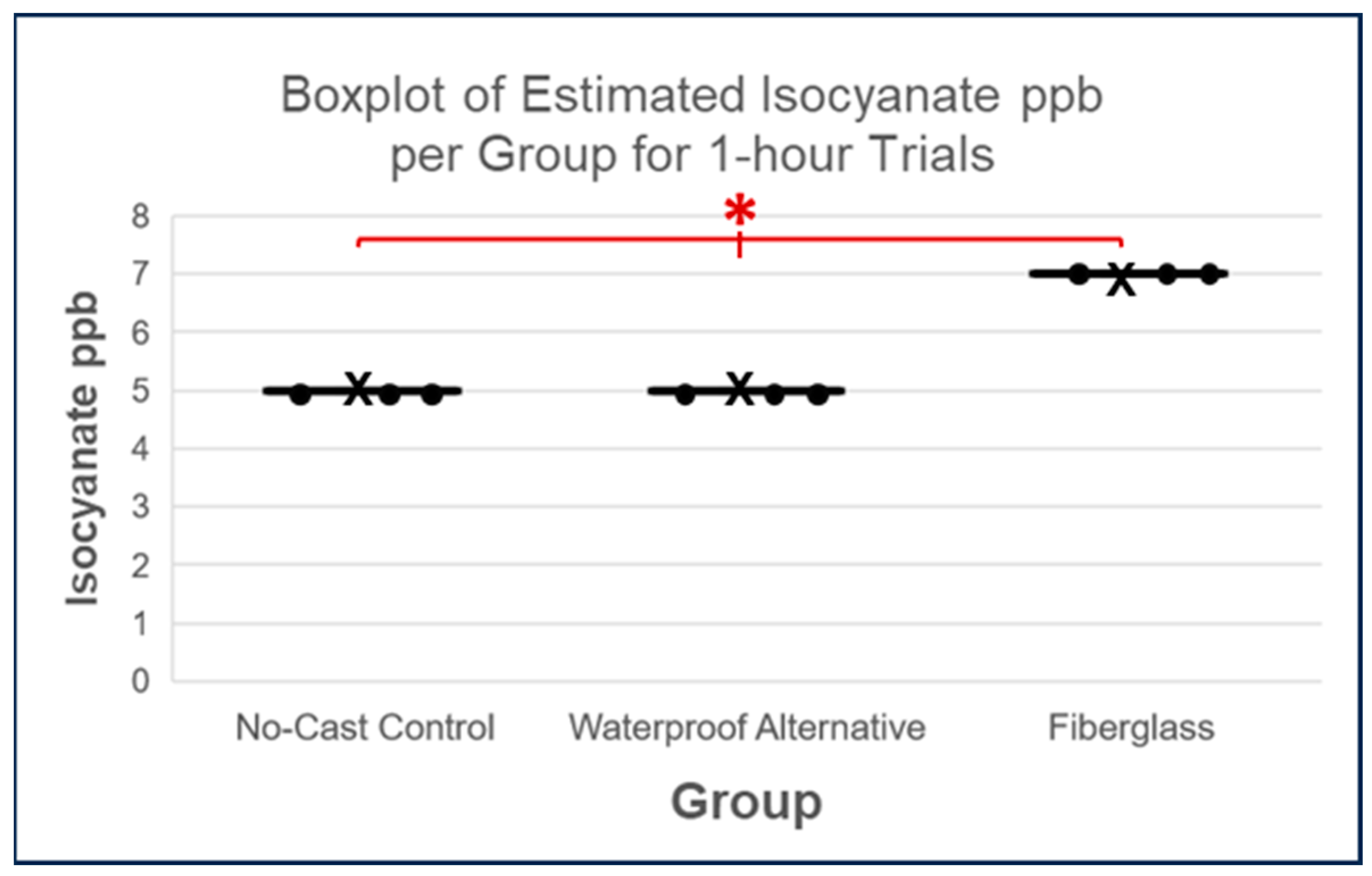
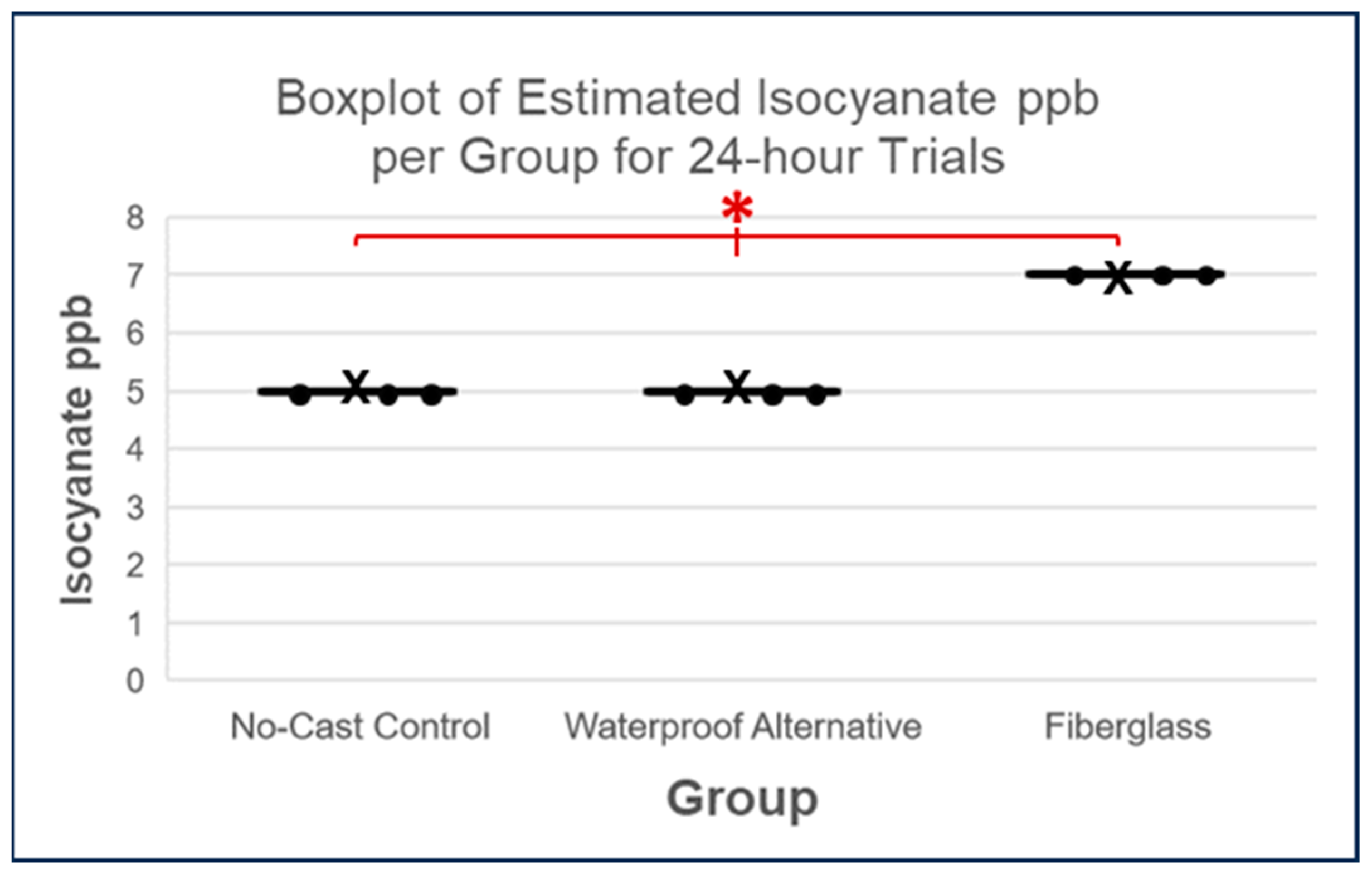
3.2. Estimated Isocyanate Release in PPB
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lockey, J.; Redlich, C.; Streicher, R.; Pfahles-Hutchens, A.; Hakkinen, P.; Ellison, G.; Harber, P.; Utell, M.; Holland, J.; Comai, A.; et al. Isocyanates and human health: Multi-stakeholder information needs and research priorities. Brain Lang. 2015, 57, 44–51. [Google Scholar] [CrossRef]
- Streicher, R.P.; Reh, C.M.; Key-Schwartz, R.; Schlecht, P.C.; Cassinelli, M.E. Determination of Airborne Isocyanate Exposure. NIOSH Man. Anal. Methods 1998, 115–140. [Google Scholar]
- Daniels, R.D. Occupational asthma risk from exposures to toluene diisocyanate: A review and risk assessment. Am. J. Ind. Med. 2018, 61, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Lenzi, V.; Crema, A.; Pyrlin, S.; Marques, L. Current State and Perspectives of Simulation and Modeling of Aliphatic Isocyanates and Polyisocyanates. Polymers 2022, 14, 1642. [Google Scholar] [CrossRef] [PubMed]
- Olivito, F.; Jagdale, P.; Oza, G. Synthesis and Biodegradation Test of a New Polyether Polyurethane Foam Produced from PEG 400, L-Lysine Ethyl Ester Diisocyanate (L-LDI) and Bis-hydroxymethyl Furan (BHMF). Toxics 2023, 11, 698. [Google Scholar] [CrossRef] [PubMed]
- Suojalehto, H.; Linström, I.; Henriks-Eckerman, M.L.; Jungewelter, S.; Suuronen, K. Occupational asthma related to low levels of airborne methylene diphenyl diisocyanate (MDI) in orthopedic casting work. Am. J. Ind. Med. 2011, 54, 906–910. [Google Scholar] [CrossRef] [PubMed]
- Pedata, P.; Corvino, A.R.; Lamberti, M.; Petrarca, C.; Di Giampaolo, L.; Sannolo, N.; Di Gioacchino, M. Non Pulmonary Effects of Isocyanates. In Current Topics in Environmental Health and Preventive Medicine: Allergy and Immunotoxicology in Occupational Health; Springer: Singapore, 2017; pp. 129–141. ISBN 978-981-10-0349-3. [Google Scholar]
- National Toxicology Program. Report on Carcinogens, Fifteenth Edition: Toluene Diisocyanates; U.S. Department of Health and Human Services, Public Health Service: Research Triangle Park, NC, USA, 2021. [Google Scholar] [CrossRef]
- Schupp, T.; Plehiers, P.M. Absorption, distribution, metabolism, and excretion of methylene diphenyl diisocyanate and toluene diisocyanate: Many similarities and few differences. Toxicol. Ind. Health 2022, 38, 500–528. [Google Scholar] [CrossRef]
- Pollaris, L.; Devos, F.; De Vooght, V.; Seys, S.; Nemery, B.; Hoet, P.H.M.; Vanoirbeek, J.A.J. Toluene diisocyanate and methylene diphenyl diisocyanate: Asthmatic response and cross-reactivity in a mouse model. Arch. Toxicol. 2016, 90, 1709–1717. [Google Scholar] [CrossRef] [PubMed]
- Matheson, J.M.; Lange, R.W.; Lemus, R.; Karol, M.H.; Luster, M.I. Importance of inflammatory and immune components in a mouse model of airway reactivity to toluene diisocyanate (TDI). Clin. Exp. Allergy 2001, 31, 1067–1076. [Google Scholar] [CrossRef]
- Zhuang, J.; Cui, H.; Zhuang, L.; Zhai, Z.; Yang, F.; Luo, G.; He, J.; Zhao, H.; Zhao, W.; He, Y.; et al. Bronchial epithelial pyroptosis promotes airway inflammation in a murine model of toluene diisocyanate-induced asthma. Biomed. Pharmacother. 2020, 125, 109925. [Google Scholar] [CrossRef]
- Yao, L.; Zhao, H.; Tang, H.; Song, J.; Dong, H.; Zou, F.; Cai, S. Phosphatidylinositol 3-kinase mediates β-catenin dysfunction of airway epithelium in a toluene diisocyanate-induced murine asthma model. Toxicol. Sci. 2015, 147, 168–177. [Google Scholar] [CrossRef]
- Peng, X.; Huang, M.; Zhao, W.; Lan, Z.; Wang, X.; Yuan, Y.; Li, B.; Yu, C.; Liu, L.; Dong, H.; et al. RAGE mediates airway inflammation via the HDAC1 pathway in a toluene diisocyanate-induced murine asthma model. BMC Pulm. Med. 2022, 22, 61. [Google Scholar] [CrossRef]
- Baur, X.; Fruhmann, G. Specific IgE antibodies in patients with isocyanate asthma. Chest 1981, 80, 73S–76S. [Google Scholar] [CrossRef] [PubMed]
- Tee, R.D.; Cullinan, P.; Welch, J.; Burge, P.S.; Newman-Taylor, A.J. Specific IgE to isocyanates: A useful diagnostic role in occupational asthma. J. Allergy Clin. Immunol. 1998, 101, 709–715. [Google Scholar] [CrossRef]
- Yucesoy, B.; Johnson, V.J.; Lummus, Z.L.; Kashon, M.L.; Rao, M.; Bannerman-Thompson, H.; Frye, B.; Wang, W.; Gautrin, D.; Cartier, A.; et al. Genetic variants in the major histocompatibility complex class i and class II genes are associated with diisocyanate-induced asthma. J. Occup. Environ. Med. 2014, 56, 382–387. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yucesoy, B.; Kashon, M.L.; Johnson, V.J.; Lummus, Z.L.; Fluharty, K.; Gautrin, D.; Cartier, A.; Boulet, L.P.; Sastre, J.; Quirce, S.; et al. Genetic variants in TNF, TGFB1, PTGS1 and PTGS2 genes are associated with diisocyanate-induced asthma. J. Immunotoxicol. 2016, 13, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Redlich, C.A.; Karol, M.H. Diisocyanate asthma: Clinical aspects and immunopathogenesis. Int. Immunopharmacol. 2002, 2, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Fisseler-Eckhoff, A.; Bartsch, H.; Zinsky, R.; Schirren, J. Environmental Isocyanate-Induced Asthma: Morphologic and Pathogenetic Aspects of an Increasing Occupational Disease. Int. J. Environ. Res. Public Health 2011, 8, 3672–3687. [Google Scholar] [CrossRef] [PubMed]
- Bello, D.; Herrick, C.A.; Smith, T.J.; Woskie, S.R.; Streicher, R.P.; Cullen, M.R.; Liu, Y.; Redlich, C.A. Skin exposure to isocyanates: Reasons for concern. Environ. Health Perspect. 2007, 115, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Coureau, E.; Fontana, L.; Lamouroux, C.; Carole, P.; Charbotel, B. Is Isocyanate Exposure and Occupational Asthma Still a Major Occupational Health Concern? Systematic Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 13181. [Google Scholar] [CrossRef] [PubMed]
- Redlich, C.A. Skin exposure and asthma is there a connection? Proc. Am. Thorac. Soc. 2010, 7, 134–137. [Google Scholar] [CrossRef]
- Collins, J.J.; Anteau, S.; Conner, P.R.; Cassidy, L.D.; Doney, B.; Wang, M.L.; Kurth, L.; Carson, M.; Molenaar, D.; Redlich, C.A.; et al. Incidence of Occupational Asthma and Exposure to Toluene Diisocyanate in the United States Toluene Diisocyanate Production Industry. J. Occup. Environ. Med. 2017, 59, S22–S27. [Google Scholar] [CrossRef]
- Clark, R.L.; Bugler, J.; Paddle, G.M.; Chamberlain, J.D.; Allport, D.C. A 17-year epidemiological study on changes in lung function in toluene diisocyanate foam workers. Int. Arch. Occup. Environ. Health 2003, 76, 295–301. [Google Scholar] [CrossRef]
- Gui, W.; Wisnewski, A.V.; Neamtiu, I.; Gurzau, E.; Sparer, J.A.; Stowe, M.H.; Liu, J.; Slade, M.D.; Rusu, O.A.; Redlich, C.A. Inception cohort study of workers exposed to toluene diisocyanate at a polyurethane foam factory: Initial one-year follow-up. Am. J. Ind. Med. 2014, 57, 1207–1215. [Google Scholar] [CrossRef] [PubMed]
- Lemiére, C.; Romeo, P.; Chaboillez, S.; Tremblay, C.; Malo, J.L. Airway inflammation and functional changes after exposure to different concentrations of isocyanates. J. Allergy Clin. Immunol. 2002, 110, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.E.; Burkert, A.L. Biomarkers of toluene diisocyanate exposure. Appl. Occup. Environ. Hyg. 2002, 17, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Sabbioni, G.; Gu, Q.; Vanimireddy, L.R. Determination of isocyanate specific albumin-adducts in workers exposed to toluene diisocyanates. Biomarkers 2012, 17, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Pearson, R.L.; Logan, P.W.; Kore, A.M.; Strom, C.M.; Brosseau, L.M.; Kingston, R.L. Isocyanate Exposure Assessment Combining Industrial Hygiene Methods with Biomonitoring for End Users of Orthopedic Casting Products. Ann. Occup. Hyg 2013, 57, 758–765. [Google Scholar] [CrossRef][Green Version]
- Tanaka, Y.; Satoh, F.; Komatsu, T.; Muto, H.; Akiyama, N.; Arai, Y.; Miyamoto, Y.; Sano, Y. A Case of Suspected Occupational Asthma in an Orthopedist, Due to Cast Materials Containing MDI. J. Jpn. Thorac. Soc. 1994, 32, 606–609. [Google Scholar]
- Sommer, B.G.; Sherson, D.L.; Kjøller, H.; Hansen, I.; Clausen, G.; Jepsen, J.R. Asthma forårsaget af methylen-diphenyl-diisocyanat-gips hos en sygeplejerske [Asthma caused by methylene-diphenyl-diisocyanate cast in a nurse]. Ugeskr Laeger 2000, 162, 505–506. [Google Scholar]
- Donnelly, R.; Buick, J.B.; Macmahon, J. Occupational asthma after exposure to plaster casts containing methylene diphenyl diisocyanate. Occup. Med. 2004, 53, 432–434. [Google Scholar] [CrossRef][Green Version]
- Rodham, P.; Giannoudis, P.V. Innovations in orthopaedic trauma: Top advancements of the past two decades and predictions for the next two. Injury 2022, 53, S2–S7. [Google Scholar] [CrossRef] [PubMed]
- Szostakowski, B.; Smitham, P.; Khan, W.S. Plaster of Paris–Short History of Casting and Injured Limb Immobilzation. Open Orthop. J. 2017, 11, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Davie, B.; Dooley, B. New Fibreglass Casting System in Orthopaedic Practice. Med. J. Aust. 1976, 1, 1010–1012. [Google Scholar] [CrossRef] [PubMed]
- Ekanayake, C.; Gamage, J.C.P.H.; Mendis, P.; Weerasinghe, P. Revolution in orthopedic immobilization materials: A comprehensive review. Heliyon 2023, 9, e13640. [Google Scholar] [CrossRef]
- Halanski, M.; Noonan, K.J. Cast and splint immobilization: Complications. J. Am. Acad. Orthop. Surg. 2008, 16, 30–40. [Google Scholar] [CrossRef]
- Ravi, M.; Fernandez Faith, E.; Whitaker, A.; Kaffenberger, J. Dermatologic complications of orthopedic casts in pediatric patients. Pediatr. Dermatol. 2022, 39, 5–11. [Google Scholar] [CrossRef]
- Lépine, M.; Sleno, L.; Lesage, J.; Gagné, S. A validated UPLC-MS/MS method for the determination of aliphatic and aromatic isocyanate exposure in human urine. Anal. Bioanal. Chem. 2020, 412, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.W.; French, J.E.; Robbins, Z.G.; Nylander-French, L.A. Epigenetic Markers Are Associated With Differences in Isocyanate Biomarker Levels in Exposed Spray-Painters. Front. Genet. 2021, 12, 700636. [Google Scholar] [CrossRef]
- Johnson, N.A.; Stirling, E.R.B.; Alexander, M.; Dias, J.J. The relationship between temperature and hip and wrist fracture incidence. Ann. R. Coll. Surg. Engl. 2020, 102, 348–354. [Google Scholar] [CrossRef]
- Chen, Y.-J.; Lin, H.; Zhang, X.; Huang, W.; Shi, L.; Wang, D. Application of 3D–printed and patient-specific cast for the treatment of distal radius fractures: Initial experience. 3D Print. Med. 2017, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Guebeli, A.; Thieringer, F.; Honigmann, P.; Keller, M. In-house 3D-printed custom splints for non-operative treatment of distal radial fractures: A randomized controlled trial. J. Hand Surg. Eur. Vol. 2023, 0, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Van Lieshout, E.M.M.; Verhofstad, M.H.J.; Beens, L.M.; Van Bekkum, J.J.J.; Willemsen, F.; Janzing, H.M.J.; Van Vledder, M.G. Personalized 3D-printed forearm braces as an alternative for a traditional plaster cast or splint: A systematic review. Injury 2022, 53, S47–S52. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparison | Adjusted p-Value |
|---|---|
| No-Cast Control vs. Waterproof Alternative | 0.1603 |
| No-Cast Control vs. Fiberglass | 0.0006 |
| Waterproof Alternative vs. Fiberglass | 0.0002 |
| Comparison | Adjusted p-Value |
|---|---|
| 15 min vs. 1 h | 0.0774 |
| 1 h vs. 24 h | 0.0003 |
| 15 min vs. 24 h | 0.0002 |
| Comparison | Adjusted p-Value |
|---|---|
| No-Cast Control vs. Waterproof Alternative | 1.0000 |
| No-Cast Control vs. Fiberglass | 0.0653 |
| Waterproof Alternative vs. Fiberglass | 0.0653 |
| Comparison | Adjusted p-Value |
|---|---|
| No-Cast Control vs. Waterproof Alternative | 1.0000 |
| No-Cast Control vs. Fiberglass | 0.0653 |
| Waterproof Alternative vs. Fiberglass | 0.0653 |
| Comparison | Adjusted p-Value |
|---|---|
| 0 vs. 15 min | 0.0252 |
| 0 vs. 1 h | 0.0342 |
| 1 h vs. 24 h | 0.0342 |
| 15 min vs. 1 h | 0.9564 |
| 1 h vs. 24 h | 0.9564 |
| 15 min vs. 24 h | 1.0000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanescu, K.; Timlin, C.L.; Moy, A.S.; Zapotoczny, G. Reduced Isocyanate Release Using a Waterproof, Resin-Based Cast Alternative Relative to Fiberglass Casts. Toxics 2023, 11, 1002. https://doi.org/10.3390/toxics11121002
Stefanescu K, Timlin CL, Moy AS, Zapotoczny G. Reduced Isocyanate Release Using a Waterproof, Resin-Based Cast Alternative Relative to Fiberglass Casts. Toxics. 2023; 11(12):1002. https://doi.org/10.3390/toxics11121002
Chicago/Turabian StyleStefanescu, Kristen, Claire L. Timlin, Ashley S. Moy, and Grzegorz Zapotoczny. 2023. "Reduced Isocyanate Release Using a Waterproof, Resin-Based Cast Alternative Relative to Fiberglass Casts" Toxics 11, no. 12: 1002. https://doi.org/10.3390/toxics11121002
APA StyleStefanescu, K., Timlin, C. L., Moy, A. S., & Zapotoczny, G. (2023). Reduced Isocyanate Release Using a Waterproof, Resin-Based Cast Alternative Relative to Fiberglass Casts. Toxics, 11(12), 1002. https://doi.org/10.3390/toxics11121002